
Abstract
Purpose of the Review:
Accidental autoerotic death, more commonly known as “autoerotic asphyxia,” is an extreme paraphilic behavior wherein individuals induce cerebral hypoxia during self-stimulated sexual activities, often by constricting the neck or obstructing respiratory passages. Data on accidental deaths caused by autoerotic play is very low because of the non-disclosure of the mode/circumstances of death or non-paralleled forensic systems in many countries. There is a high likelihood of coexisting mental disorders with such behavior. This review identifies the association of any comorbid mental disorder with accidental autoerotic deaths.
Collection and Analysis of Data:
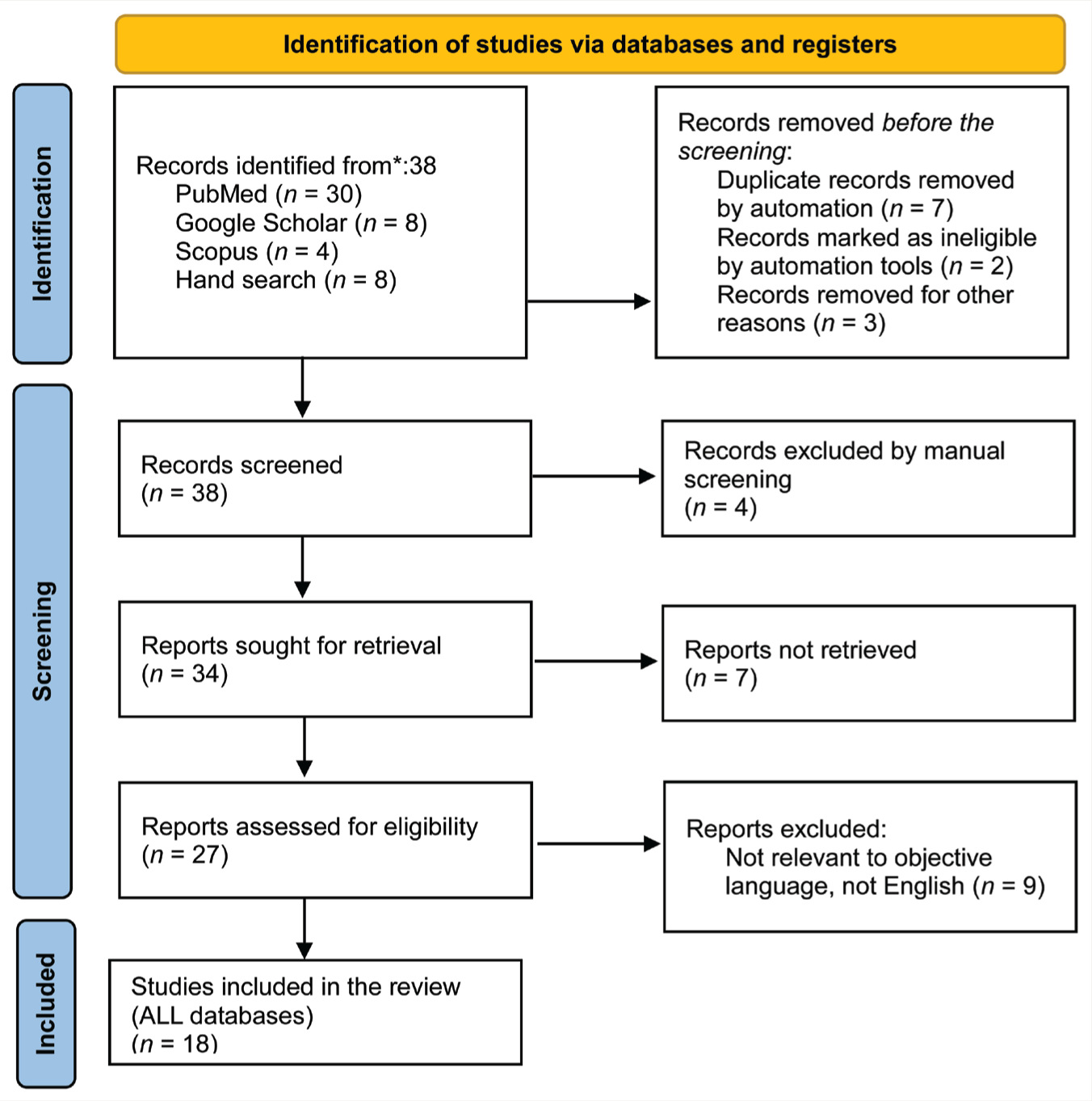
On August 23, 2023, a systematic literature search was carried out through Cochrane, PubMed, ScienceDirect, and SCOPUS, and studies identified in the English language were screened using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Review (PRISMA-ScR) guideline. Eighteen studies identified specific mental disorders with autoerotic deaths, including paraphilia, vaginismus, gender dysphoria, multiplex paraphilia, alcohol dependence, bipolar disorder, borderline personality disorder, and substance use disorder. Inhalant use like chloroform, toluene, and xylene was implicated during autoerotic fantasies.
Conclusions:
Prospective clinical screening and comprehensive multicentric psychological autopsy studies are needed to clarify the prevalence of accidental autoerotic death and related mental health conditions in the future. Given the possibility of accidental death, it remains to be seen whether paraphilia involving a single harmful event could be classified as a specifier within the impulsive-compulsive-reward spectrum, similar to how newer diagnostic systems address substance use disorders.
Keywords
Autoerotic play, particularly involving masochism, is categorized as paraphilia, where individuals derive sexual pleasure from physical pain and/or humiliation. One extreme form of this spectrum is known as “autoerotic asphyxia,” a phenomenon wherein individuals induce cerebral hypoxia during self-stimulated sexual activities, often by constricting the neck or obstructing respiratory passages. The deprivation of oxygen to the central nervous system triggers a rapid disturbance in central inhibition mechanisms, heightening sexual sensitivity and potentially inducing erotic hallucinations. 1 This behavior, also known as “Asphyxiophilia,” tends to be a repetitive and secretive behavior, often intertwined with other paraphilias and substances like alcohol or drugs to enhance pleasure. Masturbation is the most common method of autoeroticism to get sexual gratification and is considered as harmless. A few similar practices involving heightened sexual pleasure include erotic fantasy, the use of sex toys, erotic literature or media, and fetishistic and other paraphilias. However, certain autoerotic practices can lead to accidental mishaps such as erotic asphyxiation, sensory play, and self-bondage. 2 Among these, asphyxiophilia is known to be more dangerous than consensual Edge play or BDSM (bondage and discipline, dominance and submission, sadism, and masochism).2,3 It is evident from the research that asphyxiophilia starts early in adolescence and develops strong behavior patterns driven by strong euphoriant effects and often tends to be comorbid with psychological problems. 3 However, its closeness to mental health problems is controversial when compared with consensual BDSM. Typical methods of oxygen deprivation may include hanging, ligature, or the use of gaseous substances. Fatal masochistic asphyxia, though rare, can occur due to apparatus malfunction, with hanging being the most common cause of autoerotic death. Despite most deaths being accidental, potential suicidal or homicidal motives and the presence of mental disorders should be uncovered through psychological autopsy findings. 4
The prevalence of autoerotic play as sexual fantasy suggests that 85%–95% of men and women are involved in masturbatory practices, while 50%–60% use sex toys for fantasy. However, only 5%–10% are involved in asphyxiophilia or breathplay. 5 Approximately 250 deaths per year in the United States are attributed to the dangerous act of autoerotic sexual play and asphyxia. 3 According to an autopsy report, nearly 10.3% of autoerotic deaths are caused by atypical methods of autoeroticism, and isolated asphyxiophilia accounts for 2.9% of such deaths. 6 It is known that some forms of autoerotic plays could lead to accidental death due to failure of self-rescue mechanisms and possible poor judgment associated with mental morbidity, which becomes difficult to comment upon in autopsy findings. 3 The risk factors for mortality during such acts include intoxication with substances, secretive and solitary activity by locking room, and untrained autoerotic play that could be potentially lethal, for example, inability to rescue from the tight and difficult knot of ropes around the neck, inability to open the bag/mask in time, inability to reach the metal chains/locks/cuffs/belts, failure of straight jackets and helmet with rods compressing throat, chest, and abdomen.
Data on accidental deaths caused by autoerotic play is very low because of the non-disclosure of the mode/circumstances of death or non-paralleled forensic systems in developing countries such as India. Reported cases from India have not been able to verify the mental disorder associated with accidental autoerotic death due to limited coordination within the legal and medical system, non-uniform reporting quality, and infrequent utilization of psychological autopsy.4–6 Most studies on auto-erotic deaths have been done by forensic medicine experts and have been done from the point of view of the mechanism of deaths and to rule out suicide and other foul play. But the important question that remains unanswered is whether the choice of involving in such an act is just another way of voluntary sexual gratification or whether it involves diagnosable mental disorders that could mediate the phenomenon of accidental death. It is, therefore, essential to review the existing literature on this topic.
The closest disorder linked to asphyxiophilia is paraphilic disorder, which is included under mental disorder as defined by Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) and International Classification of Diseases-11 (ICD-11). The term asphyxiophilia in DSM-5 TR is classified under the chapter “Paraphilic Disorders” as “Sexual masochism disorder” with asphyxiophilia being one of its specifiers. In the ICD-11, the former is placed in the same chapter but in the category of “Paraphilic disorder involving solitary behavior or consenting individuals.” Therefore, underdiagnosis of paraphilic disorder potentially carries a small amount of risk of accidental death among unidentified individuals with such practices.7,8 Besides these, it is valuable to estimate the associated other mental disorders such as mood disorder, psychosis, and substance use disorder that could lead to poor judgment and make an individual involved in autoerotic practices vulnerable to accidental death. Most of the literature in the world has studied the cause of death retrospectively through psychological autopsy findings. 9 The existing literature offers a limited understanding of the co-occurrence of mental disorders in autoerotic practices. Particularly, there is a notable dearth of studies examining individuals actively engaging in these behaviors, such as self-asphyxiation during masturbation. 10 Understanding the potential interplay between autoerotic behaviors and mental disorders could address this knowledge gap, inform medical and legal systems about this interplay, and contribute toward studies on targeted interventions. This review is an attempt to systematically identify the word data in the English language on the co-occurrence of any mental disorder with accidental autoerotic death.
Methods
A systematic search of the literature was carried out on August 23, 2023, by using the scoping review guideline. 11 The objective of the review was to explore the association of mental health conditions with accidental autoerotic deaths.
Eligibility Criteria
We included all the types of original studies published in the English language till August 8, 2023, including case-control, cohort, comparative studies, randomized controlled trials (RCTs), case reports, and case series focusing on accidental autoerotic deaths and mental disorders. We excluded reviews of all types. Our data included participants of any age, sex, and any type or severity of autoerotic play who have been reported to have mental health conditions before death or identified after autopsy.
Search Strategy
Two independent authors (RS and AA) conducted a systematic literature search of the following databases on August 8, 2023: Cochrane, PubMed, ScienceDirect, and SCOPUS. In addition, the reference lists of the pertinent literature were screened for relevant studies.
Search Keywords
The literature was searched using keywords: (“death”[MeSH Terms] OR “death” [All Fields] OR “deaths”[All Fields]) AND (“autoerotic”[All Fields] OR “autoerotism”[All Fields]) AND (“mental disorders”[MeSH Terms] OR (“mental”[All Fields] AND “disorders”[All Fields]) OR “mental disorders”[All Fields] OR (“mental”[All Fields] AND “disorder”[All Fields]) OR “mental disorder”[All Fields]) AND (“autopsied”[All Fields] OR “autopsy”[MeSH Terms] OR “autopsy” [All Fields] OR “autopsies”[All Fields]). Additional MeSh Terms searched included Accidents, Adult, Asphyxia/pathology, etiology, Forensic Pathology, Humans, Neck Injuries/pathology*, Paraphilic Disorders/psychology, Time Factors, Unconsciousness / Videotape Recording
Data Collection and Analysis
Two investigators (RS and AA) independently evaluated the studies and extracted the data in a predesigned proforma as per inclusion criteria. The details included were study ID, authors, year, country, inclusion criteria, sample size in each group, age, sex, cause of death, description of the circumstances of autoerotic play just before the time of death, including object used around the body part, mental health condition described in the report, substance use, and other important autopsy findings.
Data Extraction and Management
Two authors (AA, RS) independently extracted data from the selected studies using a standardized coding form prepared in Microsoft Excel 2010. They discussed any differences in the data extraction until a third author (DB) resolved the conflict. The study results were tabulated to mention the characteristic findings of each study.
Results
Studies not mentioning accidental death during autoerotic play, cases of controversial suicide in the absence of evidence, and not detailing mental health conditions were excluded.12,13,9,14–19
Results
The findings reveal a diverse dataset across 18 studies spanning multiple countries, with Germany, the USA, Australia, Italy, Japan, and Canada contributing significantly, having a maximum of five studies from Germany (shown in Figure 1). Of the total studies, three were case series, while 15 were individual case reports demonstrating both individual instances and broader trends, with the total sample size of the review being 47 individuals. No RCTs, case-control, cohort, and comparative studies were found in the literature review. Sample sizes varied from as small as one to as large as 17. Male outnumbered (n = 41) female cases (Six) across all the reports. The mean age of the sample was 39.88 years, and the age range was between 26–35 years (8 cases), followed by 36–45 years (5 cases) and 46–55 years (4 cases), as shown in Table 1.
PRISMA Flow Diagram.
Characteristics of Included Studies on Accidental Autoerotic Deaths and Mental Disorders.
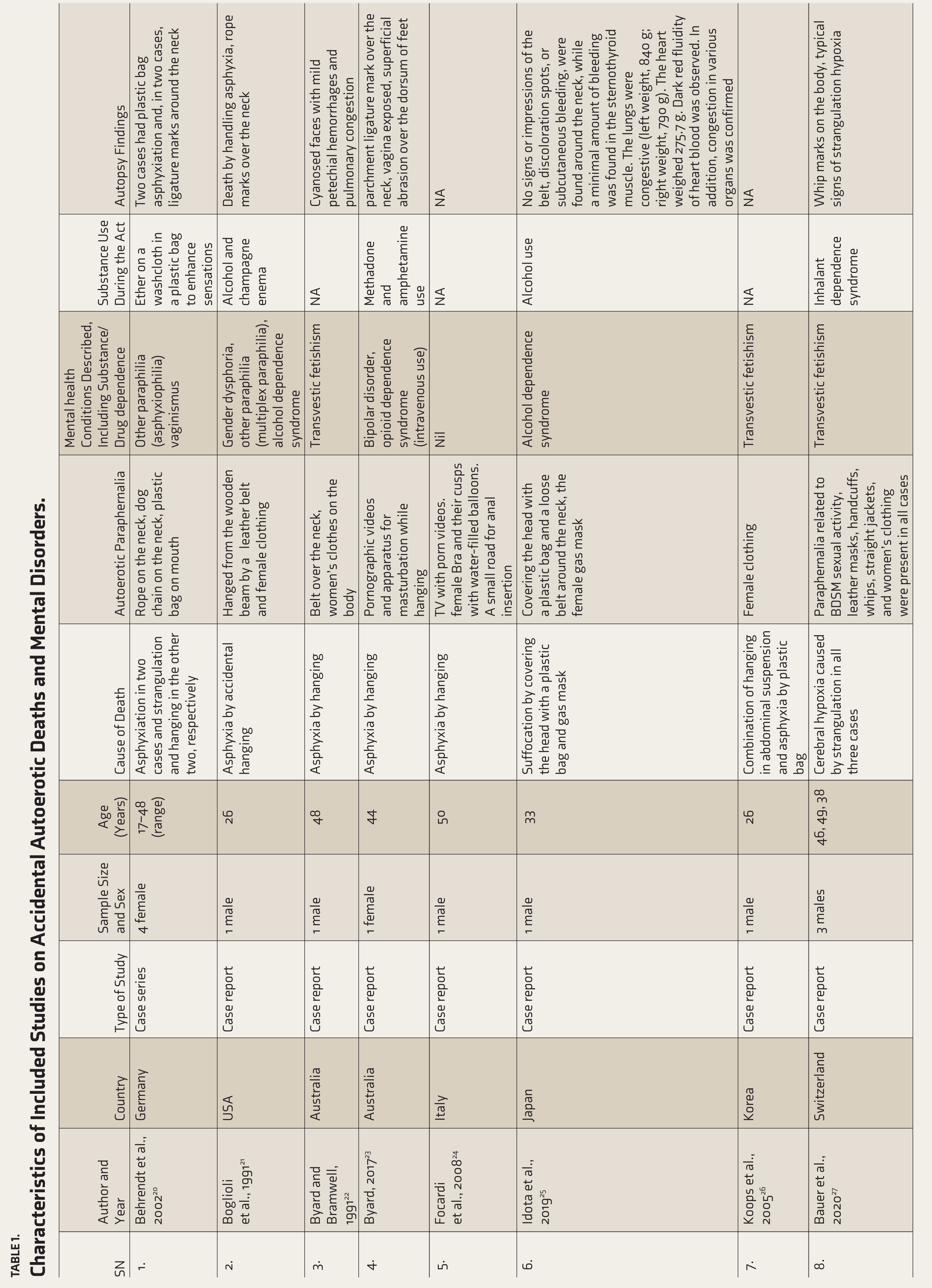
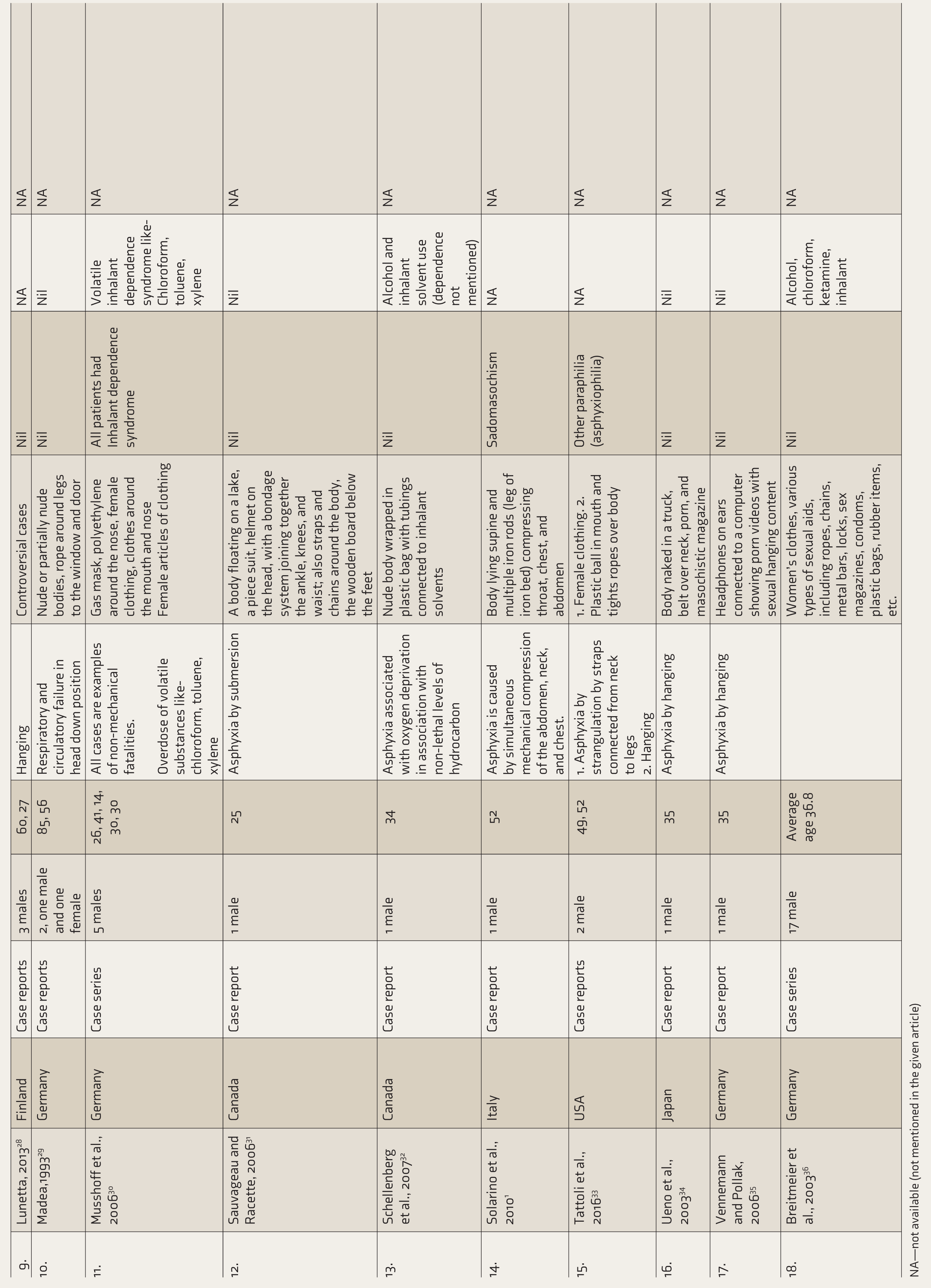
NA—not available (not mentioned in the given article)
The cause of death in the provided cases varied, but all of them share common features of asphyxiation or oxygen deprivation leading to fatal outcomes. Several cases involved asphyxiation by hanging, mostly accidental, with instances of individuals succumbing to strangulation, hanging, or a combination of both. In some cases, the asphyxiation was exacerbated by additional factors such as covering the head with a plastic bag and gas mask or utilizing volatile substances like chloroform, toluene, and xylene, leading to suffocation. Additionally, some fatalities resulted from a combination of mechanical compression to the abdomen, neck, and chest, exacerbating the asphyxiation process.1,24,29,31 Notably, all cases presented are examples of non-mechanical fatalities, highlighting the diverse but interconnected nature of asphyxiation-related deaths and the critical importance of understanding and addressing the underlying factors contributing to such tragedies.1,3,20–35
The findings from the cases depict a range of objects used around various body parts, highlighting the diverse circumstances surrounding each incident. Instances included the presence of ropes, dog chains, plastic bags, belts, and women’s clothing wrapped around body parts, such as the neck or mouth. In some cases, the use of paraphernalia associated with BDSM sexual activity, including leather masks, handcuffs, whips, and straitjackets, was noted alongside women’s clothing, suggesting a potential connection to such practices.3,20–26 Controversial cases involved nude or partially nude bodies with unique configurations, such as ropes around legs tied to windows and doors, gas masks, polyethylene coverings, bondage systems, various sexual aids, and joining ankles, knees, and waists. Additionally, the presence of headphones connected to computers displaying pornographic content with sexual hanging themes, as well as the discovery of magazines in trucks, further underscored the complexity and sensitive nature of these cases. These findings highlight the importance of thorough investigation and understanding of the contexts surrounding each incident to accurately determine cause and motive.
The findings regarding mental health conditions provide insight into the complexities of psychological factors potentially influencing the cases examined. Conditions such as paraphilia, vaginismus, gender dysphoria, and multiplex paraphilia were noted, indicating a range of sexual disorders and identity concerns.1,31–35 Additionally, instances of alcohol dependence, bipolar disorder, and opioid dependence syndrome (intravenous use) recognize the importance of screening for substance-related issues and mood disorders within the population studied. Moreover, the mention of masochism practice undergoing psychotherapy in few studies suggests a treatment seeking for mental health in individuals involved in autoerotic play and accidental death. Interestingly, some cases reported no apparent mental disorders, suggesting a need for further exploration into other contributing factors such as personality types, coping skills, attachment, and relationship styles.
The findings related to substance use shed light on the diverse methods and substances that might be used for heightening sexual arousal involved in the cases examined. Instances included the use of ether-soaked washcloths in plastic bags to heighten sensations, as well as unconventional practices like alcohol and champagne enemas, highlighting the extreme lengths some individuals may go to in pursuit of altered states. Additionally, methadone and amphetamine use were noted, underscoring the prevalence of illicit drug consumption among these subgroups. Alcohol and inhalant use emerged as recurring themes, with volatile substances like chloroform, toluene, and xylene implicated in some instances.3,20–28 Notably, findings also indicated cases with high blood alcohol levels, ranging from 0.1 to 2.5 per thousand, and the presence of substances such as chloroform, ketamine, and propane-butane gas mixtures, suggesting a complex interplay between various intoxicating agents and autoerotic play leading to accidental death.
Instances of death by hanging caused by asphyxia, indicated by rope marks around the neck, have been observed. Cyanosed faces with mild petechial hemorrhages and pulmonary congestion were frequently observed post-mortem. Additionally, parchment ligature marks over the neck were noted, often accompanied by exposed vaginas and superficial abrasions on the dorsum of feet, indicative of elaborate masturbation rituals involving strangulation. In some cases, no visible signs or impressions of belts were found, with minimal bleeding detected in the sternothyroid muscle. Congestion in various organs, particularly the lungs, was a common finding, along with dark red fluidity of heart blood. Notably, whip marks on the body were observed alongside typical signs of strangulation hypoxia, underscoring the complex and potentially dangerous nature of autoerotic behaviors.
Discussion
Identifying mental disorders in individuals who have died from autoerotic activities can inform forensic psychiatrists for the assessment of the risk related to such behaviors. Although there is no strong, established evidence of the association of mental disorders with accidental autoerotic deaths, having understood the co-occurrence of mental disorders in autoerotic deaths from this review calls for dedicated efforts in risk assessments, disclosure techniques, screening, and safeguarding such individuals during clinical practice. Sexual experimentation could be common during adolescence, and sexual acts may occur impulsively, even among adults with autoerotic fantasies rather than having a recurrent pattern of sexual arousal. 8 More reports from Germany elucidate further behavioral norms, thresholds of abnormality, and attitudes regarding autoerotic plays that vary across cultures.7,8 The diverse sexual behaviors involving atypical patterns of sexual arousal that do not involve marked distress or significant risk of injury or death are generally not considered to be paraphilic disorders. They sometimes may be transient and occur concerning substance use or intoxication. 8 However, it becomes difficult to understand how these behaviors could be lethal in the absence of a diagnosable disorder. Further paraphilic disorders frequently co-occur with several other mental disorders, including mood disorders, anxiety disorders, personality disorders, and disorders due to substance use disorders. It is also common for an individual to meet the diagnostic requirements for more than one paraphilic disorder. For example, one of the studies highlighted a fatal outcome in shibari, a double-hanging sexual asphyxia practice, examining the psychiatric evaluation of the surviving participant revealed a history of borderline personality disorder, childhood sexual abuse, substance use, self-harm, and sexual dysregulation, prompting concerns about safety measures in masochistic practices in individuals with mental disorders. 37 In another case–control study, sexual masochism disorder was found to be 10 times higher in women with borderline personality disorder. 38 Among borderline personality disorder, those with masochism reported more prevalence of child sexual abuse, more hostile/dismissing attachments, higher sensation seeking, and more frequently exploratory/impersonal sexual fantasies. 38 Therefore, identifying borderline personality disorders among those practicing autoerotic play or vice a versa becomes a preventive health aspect for mental health professionals as well as forensic clinician. Screening of depression, psychosis, borderline personality disorders, and substance use disorders could be of paramount importance in preventing accidental consequences among autoerotic practitioners, as highlighted in the review.
From a psychoanalytical point of view, Freud’s conceptualization of masochism as a partial instinct within the pleasure principle elucidates its relationship to the life and death drives. 39 It can be broadly understood as thriving for happiness beyond life and death. Symbolically, the traumatic aspects of the primary relationship with the object could be stored as fantasies in the body, which later would represent masochistic fantasies of being beaten, and the pleasure of pain would lie in the attempt to “dream” the trauma not only in the imagination but also, “aesthetically,” in the body. 40 One study revealed that among individuals with paraphilic practices, there is a notable prevalence of childhood experiences such as sexual and physical assault, neglect, early sexual exposure, and a family history of deviant sexual behaviors. 38 Therefore, individuals with autoerotic practice must be aware of overcoming such experiences of childhood through healthy coping mechanisms and risk-benefit associated with the heightened stimulation involved in autoerotic plays. Psychodynamic psychotherapy, 40 and cognitive behavioral therapy (CBT), 39 could address the compulsive nature of these conditions, while relapse prevention, 40 and harm reduction therapy, 40 could focus on retraining inappropriate sexual interests. Pharmacotherapy options for paraphilias could be selective serotonin reuptake inhibitors, steroidal antiandrogens, and gonadotropin-releasing hormone (GnRH) analogs; the discussion, however, is beyond the scope of this review. 42
Notably, the presence of inhalant use among individuals with autoerotic practices highlights the possibility of forgetting past traumatic experiences within this subgroup of the population, which requires further research. 42 Though paraphilia and paraphilic disorders are differentiated in recent classifications, the concern of masochistic disorder requiring the inclusion of asphyxiophilia as a specifier for the disorder of sexual preference in recent diagnostic classifications can be examined further. These considerations, being sensitive, stigmatizing, and low in prevalence, make it a topic of future research.
There is no valid data on the proportion of individuals engaging in potentially lethal autoerotic practices who seek help from psychiatry or psychology clinics, making these cases often emerge only after a fatality. While online and offline communities exist for support, effective interventions are needed. Although pharmacological options are limited, psychodynamic therapies, behavioral therapies, and the teaching of safe techniques can be beneficial for these individuals. Therapeutic interventions can also focus on these practices along with primary mental health concerns. The complex grief process involved in families and friends of such persons could be better handled by psychologically informed social health workers and caregivers through psychological support and counseling about the processing of the unusual circumstances surrounding the death. This is also important for larger populations in identifying the risk involved in autoerotic practices and raising awareness among mentally ill patients who might have impaired judgment in limiting autoerotic practices. For a forensic investigation, it could be possible to routinely assist through the assessment of paraphilia, severe mental illnesses, and substance use disorders during psychological autopsy and differentiate from suicide or unnatural deaths. These findings emphasize the importance of comprehensive mental health assessments and tailored interventions to address the diverse needs of individuals experiencing mental health challenges within the context of autoerotic plays. Also, it becomes important to recognize and understand the unique characteristics and potential risks associated with autoerotic activities to prevent tragic accidental deaths. Further exploration of comprehensive personality domains involved, paraphilic behavior, extent of autoerotic plays, and substance abuse require detailed inquiry through psychological autopsy studies in forensic contexts and prospective cohort studies from a psychiatrist’s viewpoint.
Clinical Implications
Identification of mental disorders in cases of autoerotic play has clinical implications before the occurrence of accidental injuries. These accidental injuries raise alarm for clinicians in terms of risk assessment, treatment planning, psychological support for families, education, and associated forensic considerations after death. Integrating mental health assessment and intervention into clinical practice can help mitigate risks and improve outcomes for individuals with mental disorders who may be vulnerable by engaging in high-risk behaviors. Clinicians may recognize certain mental health conditions as potential risk factors for engaging in high-risk behaviors, including autoerotic practices, by conducting surveys or screening for such behaviors in suspected individuals. This recognition can prompt targeted interventions aimed at reducing the likelihood of similar incidents in at-risk individuals.
Paraphilias often involves recurrent, persistent, and intrusive sexual thoughts or fantasies that individuals find difficult to control, feeling compelled to act on these urges—similar to how those with obsessive-compulsive disorder (OCD) feel driven to perform rituals or behaviors to relieve anxiety. Both conditions share irrational or distorted thought patterns, fixated on specific fears (in OCD) or sexual themes (in paraphilias). However, distinguishing between cravings for paraphilic behaviors and reward dependence is challenging, as both may lie on an impulsive-compulsive-reward spectrum. The subjective sense of increasing tolerance to behavioral rewards can be explained within this framework.
Further, perhaps the inclusion of paraphilia with a single harmful event as a specifier could be reexamined from the dimensional viewpoint of diagnostic systems for impulsive-compulsive-reward spectrum disorders. What if a single episode of harmful use and harmful pattern of use could be identified as a specifier in the future?
Limitations
Small numbers may not be representative of the broader population, the reliance on the limited retrospective data from case reports, inherent limitations associated with post-mortem examinations and forensic investigations related to the accuracy and completeness of the data, absence of controls to establish causality or temporality between mental disorder, substance use, and autoerotic behaviors makes it difficult to generalize the findings and makes it more complex construct to study scientifically. All the sexual fantasies may not amount to paraphilias, as the review excluded studies not mentioning accidental death during autoerotic play. This could also imply the existence of autoerotic acts in the absence of paraphilia, and such practices could be common in the general population.
Conclusion
In this review, we found that 11 out of 18 case reports/series (62%) have clearly one or other diagnosable psychiatric disorders. The most common are paraphilias (specifically transvestic fetishism followed by asphyxiophilia), substance use disorders, and mood disorders. Impulsivity is an important trait that is potentially found in most cases. The absence of prospective studies, combined with the secretive nature of autoerotic behaviors, the unintentional omission of paraphilias during negative case histories, and the lack of specific data on causative associations of mental disorder with accidental autoerotic play, renders the finding of this scoping review inconclusive but intriguing. This review provides a scientific inquiry into the complexities surrounding autoerotic accidental deaths and mental health, thus emphasizing the need for further research in this area. The inclusion of paraphilia with a single harmful event as a specifier, rather than categorizing it as a full disorder, could be reconsidered within the impulsive-compulsive-reward spectrum, much like how newer diagnostic systems address single versus harmful patterns of use in substance disorders. The task force of ICD-11, DSM-5, and other research agencies could find the relevance of this review in conducting further studies on paraphilic disorders, substance use disorders, and borderline personality disorders, which are found to be commonly associated with such acts. Inhalant use, such as chloroform, toluene, and xylene, was implicated in some instances of autoerotic deaths. It should be carefully questioned among individuals with autoerotic fantasies, and suspected individuals may be informed regarding the associated risk of accidental deaths. Furthermore, given the scarcity of data, comprehensive approaches in multicentric psychological autopsy studies or prospective screening for transvestic fetishism, sadomasochism, asphyxiophilia, and multiplex paraphilia across the countries could give us a clear picturization of the prevalence of accidental autoerotic death and associated mental health conditions in the future.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Nil.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement on Prior Presentation
Authors declare that this article has not been presented in meeting or conference. The article has not been submitted to any other journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.