
Abstract
Purpose of the Review:
Paraphilias, encompassing a diverse range of atypical sexual interests and behaviors, have been a subject of profound interest and scrutiny throughout history. These sexual interests are a matter of debate with the changing society and also with the changing world view. The rise in awareness about abnormal sexual interests also poses difficulty in adding to the existing list. This article aims to provide a comprehensive exploration of the historical underpinnings, current diagnostic criteria, legal considerations in India, and treatment approaches available for paraphilias.
Collection and Analysis of Data:
Electronic searches were done on PubMed, Science Direct, Web of Science, and Google Scholar. Search term included were “paraphilias,” “history,” “nosology,” “legislation,” “law,” “treatment guidelines,” and “treatment recommendations” in various combinations. An independent online search was also conducted for historical and legal aspects of India. The classification and understanding of paraphilias have evolved over time, with some being removed from criminalized groups and laws and legislation changing based on societal norms. ICD and DSM have become more structured, but need constant updating.
Conclusions:
India's laws need to be more specific and streamlined, and guidelines have not been assessed for effectiveness. Paraphilias has been treated as a foster child in psychiatry, raising concerns about treatment options.
Keywords
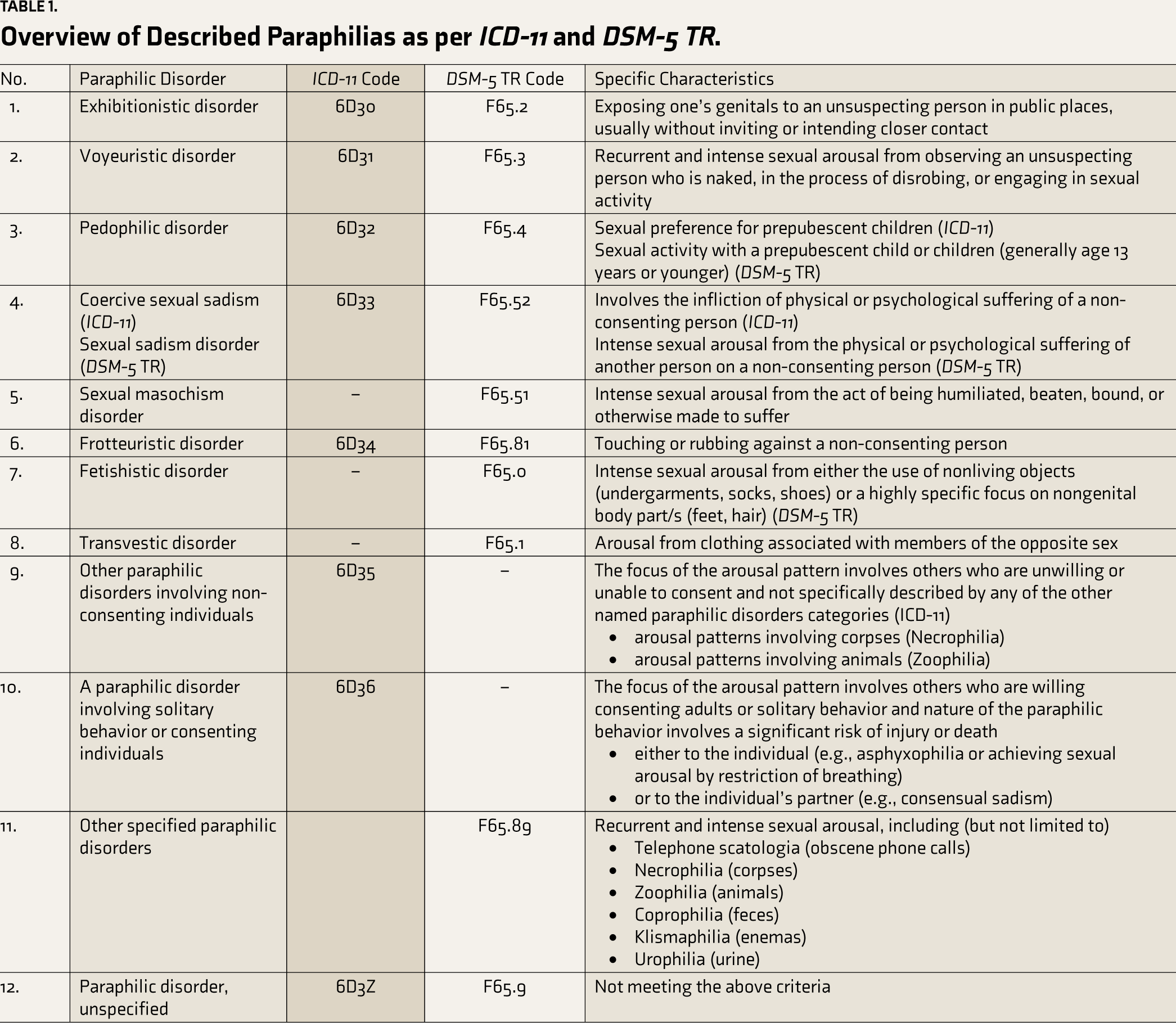
For a considerable amount of time, researchers, medical professionals, and the general public have been fascinated by paraphilias, a broad category of abnormal sexual behaviors and interests. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) defines “paraphilia” as “any intense and persistent sexual interest other than sexual interest in genital stimulation or preparatory fondling with phenotypically normal, physically mature, consenting human adult partners.” 1 Although not innately pathological, a paraphilic disorder can evolve if paraphilia invokes harm, distress, or functional impairment in the lives of the affected individual or others. The DSM-5 enlists eight different types of paraphilias, which include (in the order described in DSM-5 with codes): voyeuristic disorder (302.82), exhibitionistic disorder (302.4), frotteuristic disorder (302.89), sexual masochism disorder (302.83), sexual sadism disorder (302.84), pedophilic disorder (302.2), fetishistic disorder (302.81), and transvestic disorder (302.3). 1
Table 1 lists the essential characteristics of each major paraphilic disorder as listed in International Classification of Diseases-11 (ICD-11) and DSM-5 TR, along with the corresponding codes. This article explores the fascinating world of paraphilias and examines the progression of cultural perspectives, historical foundations, the current state of diagnosis, legal considerations, and available treatment options and guidelines with respect to India.
Overview of Described Paraphilias as per ICD-11 and DSM-5 TR.
Methods
In order to provide a comprehensive overview of the Indian aspect of paraphilias, electronic searches were carried out using databases such as PubMed, Science Direct, Web of Science, and Google Scholar for this review. The following search terms were entered into the electronic search engines as described above—“paraphilias,” “history,” “nosology,” “legislation,” “law,” “treatment guidelines,” and “treatment recommendations”—with various combinations such as “paraphilia/ paraphilic disorder” and/or “Indian history” and/or “epidemiology” and/or “nosology” and/or “assessment” and/or “diagnosis” and/or “treatment/guidelines.” An independent online search was also conducted for historical and legal aspects of India.
Historical Aspects
Descriptions of people experiencing repeatedly high levels of sexual desire in response to non-traditional (unconventional) stimuli date back long before the term “paraphilia” was coined. Sanctions and stigma against such acts and behaviors cause difficulty in ascertaining whether paraphilia exists and to what degree. Ancient Egyptian and Greek erotic art mentions some images of bestiality and large phalluses. However, a detailed description of how this artwork was understood is unavailable. The Greeks and Romans engaged in pedophilia and hebephilia as part of their relationship-building practices with their students, purportedly providing them with healthy guidance. 2 The Bible contains mentions of paraphilic behavior (voyeurism, bestiality, necrophilia, and exhibitionism) and labels them as socially unacceptable and forbidden. 3 Islamic texts mention sexual arousal due to various paraphilias such as offensive, makruh, prohibited, and haram. 4
In the modern era, examples of sexual masochism appeared in the late fifteenth century. Friedrich Solomon Krauss, an Austrian ethnologist, coined the term “paraphilia” in 1903 to refer to “abnormal erotic instinct.” 5 In 1925, J. S. van Teslaar translated Wilhelm Stekel’s “Peculiarities of Behaviour-II,” when the term “paraphilia” was first used in English. 6 John Money, who promoted the term “paraphilias” instead of perversions, has been credited with making it into the mainstream. 7
Overview in Indian Context
This part can be easily understood by looking at three different periods in Indian history: ancient or pre-colonial, colonial, and post-colonial.
Ancient or pre-colonial period: The Kama Sutra, the Koka Shastra, and the Ananga Ranga are among the ancient Indian texts that address biting, love marks left after intercourse, and love blows. The fact that the scriptures reference such deeds suggests that these methods aroused some people. Whether they were assimilated into people’s long-lasting sexual routines is unknown, however. 8 Indian mythology is replete with stories that involve gods, goddesses, and mythical beings engaging in behaviors that might be considered paraphilic by modern standards. For example, the tales of Shiva’s unconventional sexual practices or the androgynous nature of certain deities challenge conventional norms and reflect the fluidity of sexual expression in ancient India. 9 Rituals and ceremonies in ancient India often incorporated elements of sexuality and sensuality. Practices such as tantric rituals, which sought spiritual enlightenment through the union of opposites, involved the exploration of taboo subjects such as sexual energy and ecstasy. 10 Since Patanjali defines yoga as “Citta Vritti Nirodha,” or regulating the turbulent forces of the mind, sex has also been discussed in yoga practices. There are eight stages in all, and the stage of “Yama” includes the following five abstentions: ahimsa (non-violence), satya (truthfulness), asteya (not stealing or avoiding misappropriations in thought and action), brahmacharya (sexual abstinence, which some understand to mean controlled sexual activity), and aparigraha (non-acquisitiveness). 11
Throughout the past, as a result of several invasions, India has seen a gradual integration of other languages, religions, cultures, and civilizations, which has enriched Indian identity throughout the centuries and led to ultimate blending with the native people, and these practices of paraphilias and sexual practices have also been introduced to the Indians. 11
Colonial period: During the colonial period, India was introduced to Western medical concepts of mental illness and sexual deviance, leading to a more medicalized approach to understanding and addressing paraphilias. Mental illness and even paraphilias were viewed through the lens of Western psychiatric nosology and have been influenced by colonial attitudes. 12 There were no attempts to integrate the ancient Indian understandings with Western concepts.13,14
Post-colonial period: During the post-colonial era or modern times, there were no attempts to integrate Indian concepts and Western psychiatry as far as mental illness, which includes paraphilias, was considered. The lack of historical and cultural understanding in Indian psychiatry hinders the exploration of its unique conceptual issues and further challenges in eradicating this gap in Euro-American psychiatry.13,15 The issues mentioned above, which persisted during the colonial and post-colonial periods, have led us to follow the understanding and nosology of paraphilias as laid out in Western literature, which lacks the Indian touch.
Epidemiology
The prevalence rates of paraphilias are difficult to ascertain as the criteria change over time and between cultures. 16 Information about the epidemiology of paraphilia is quite scarce. According to several studies, the prevalence ranges from 1.7% to 62.4% of patients exhibiting at least some paraphilia-related patterns. 17
In a 2011 research conducted in Germany, 1,915 German males between the ages of 40 and 79 were tested, and 62.4% of them reported having at least one sexual arousal pattern linked to paraphilia; just 1.7% of these cases reported them as distressing. This study seems to indicate that the majority of people had paraphilic arousal, which is also not seen to be disturbing. 18 In contrast, 3.1% of participants in a 2006 Swedish National Population survey, which polled a sample of 2,450 people aged 18–60, reported at least one instance of being sexually aroused by flashing their genitalia to a stranger, and 8% acknowledged being sexually aroused by spying on others while they were having sex. 19 Concerns with inconsistency in validity are raised by the significant diversity in paraphilia prevalence rates in broad sampling. This might be because questionnaires are personal and private, which could reduce their validity. 20
Regarding more standardized studies, most data are based on criminal reports or studies using clinical populations referred for legal reasons rather than for self-help in the general population. An analysis of 166 sexual murderers conducted in 2006, for example, found that sexual sadism was more prevalent, coupled with other disorders and interests connected to paraphilia. However, prevalence rates are still difficult to report with any certainty, and the contentious nature of paraphilia definitions further underpins this. 21 A recent study conducted in 2018 examining paraphilic behaviors among 1,040 participants found that nearly half indicated an interest in paraphilic categories, with 15.9% reporting fetishism, frotteurism, voyeurism, and masochism. Both males and females showed interest in these behaviors, with voyeurism and fetishism being the most common. There was no discernible difference in the interest levels of males and females. 22
In a research carried out in southern India, paraphilias were also taken into account when examining the frequency and correlation of sexual disorders in 1,529 individuals. Results showed that no cases of paraphilias were found. 23 No specific study has been conducted in India, focusing only on paraphilias until this review was done.
The Nosology of Paraphilic Disorders
Usually, two categories of paraphilias are identified: criminal and non-criminal. While the latter involves a willing partner, an inanimate object, or a consenting person, the former involves sexual behavior with a non-consenting person, a person who is incapable of giving consent (such as minors), or animals. This type of classification has not been strictly followed and has been challenged as there has been a change in culture. 37
DSM
In DSM-I (1952), five categories of sexual deviations, transvestism, homosexuality, fetishism, pedophilia, and sexual sadism, which are now known as paraphilias, were listed. Rape, assault, and mutilation were all included under sexual sadism but not sexual masochism. 24 These were known as “psychopathic personality with pathologic sexuality” even before DSM-I was published.
Further, in DSM-II (1968), sexual interests were characterized as bizarre and non-bizarre, though without any definition, and it was stated that persons suffering from the disorder were unable to substitute their bizarre with non-bizarre interests despite having distress with it. The list was extended to include eight more categories of deviations: voyeurism, exhibitionism, fetishism, pedophilia, transvestism, sadism, and masochism. Rape was removed from the list, and a separate category of other sexual deviations was added. 25
In DSM-III (1980), a separate diagnostic category for “paraphilias” was created for the first time in the DSM classification. Zoophilia was added to the list of paraphilias because animals cannot consent to sexual activity, and homosexuality was removed from the list. However, ego-dystonic homosexuality was retained as a mental disorder but not paraphilia. Also, whether the patient was distressed or not by paraphilia was not considered. 26 The patient needed to have either acted on those desires or experienced noticeable distress to apply the criteria in the updated DSM-III. A criminal paraphilia called frottérism was added to the list, along with episodic paraphilia. 27
“The fantasies, sexual urges, or behaviors cause clinically significant distress or impairment in social, occupational, or other important areas of functioning” was added to all paraphilic diagnostic criteria in DSM-IV (1994), and the list of disorders under the NOS for paraphilias remained unaltered. 28 However, DSM-IV had a significant change, which was though not distinct but did provide a difference between paraphilia and paraphilic disorders, which read as follows: “A paraphilia must be distinguished from the non-pathological use of sexual fantasies, behaviors, or objects as a stimulus for sexual excitement in individuals without a Paraphilia.” This remained unchanged in DSM-IV and was more distinct in DSM-5. 1
The criteria for criminal paraphilias, such as voyeurism, exhibitionism, frotteurism, and pedophilia, were changed in the DSM-IV TR (2000) to read: “The person has acted on these sexual urges, the sexual urges or fantasies cause marked distress or interpersonal difficulty.” However, the criteria for BDSM (bondage and discipline, dominance and submission, sadism, and masochism), which may have been adopted because of organizations that supported the traits, were amalgamated and read: “It is either with a non-consenting person or is causing marked distress or interpersonal difficulty. 29
In DSM-5 (2013), significant changes include the change in nomenclature from “paraphilia” to “paraphilic disorder.” In earlier DSM categories, the term “disorder” was not used. The distress and/or dysfunction is necessary for the patient to be suffering from the paraphilic disorder apart from obviously having a paraphilia. However, there is a catch in it. If a person, once labeled with a diagnosis, had sought help for distress that was short-lived, the person would remain in remission for the rest of their life. 1 Additionally, DSM-5 clarified the distinction between behavior and paraphilias and added specifier phrases such as “in remission.” The specifier is silent about changes in the presence of the paraphilic interest per se. The other course specifier, “in a controlled environment,” is included because an individual’s propensity to act on paraphilic urges may be more difficult to assess objectively when the individual has no opportunity to act on such urges. DSM-5 maintains the same standard for pedophilia as DSM-IV TR. It has been modified, meanwhile, for other paraphilias (which the nation’s legal system views as crimes), such as: “The individual has acted on these urges with a nonconsenting person.”
The DSM and ICD do not specifically define paraphilias as belonging to “criminal” or “non-criminal” categories. As an alternative, the DSM and ICD offer diagnostic standards for certain paraphilic diseases without classifying them as essentially criminal or non-criminal. Also, for pedophilia, the interest in children need not be greater than the individual’s homophilic interests, and even having any sexual interest in children can be a ground for diagnosis. 1 The list of disorders in the section of “other specified paraphilic disorder” was not changed except for partialism being included under fetichism. 1
DSM-5 TR (2022) has kept paraphilic disorder the same as that mentioned in DSM-5 with no further changes. 30
ICD
The first two editions of ICD (which listed the mental disorders), that is, ICD-6 (1948) and ICD-7 (1958), included the paraphilias as sexual deviations with “other pathological personality disorders.”31,32 Apart from the “other and unspecified categories,” these abnormalities were divided into eight subcategories in ICD-8 (1968). The eight categories were exhibitionism, voyeurism, fetishism, masochism, pedophilia, transvestism, and homosexuality. 33 Then, homosexuality was eliminated, and transsexualism, sexual dysfunctions, disorders of psychosexual identity (such as gender-role disorder), and ego-dystonic homosexuality were added to the list in ICD-9 (1979). The terms “other” and “unspecified psychosexual disorders” were nevertheless included. 34
In ICD-10 (1993), the list of paraphilias remained the same as before, with two changes, which were the merging of sexual sadism and sexual masochism into a single category and the addition of dual role transvestism in which there is cross-dressing without any permanent desire for transition or sexual arousal with fetishistic transvestism. It was kept under the rubric of disorder of sexual preference under disorders of adult personality and behavior. F65.6, a new diagnosis code, was added for various disorders of sexual preference. 35
A new diagnostic category for sexual health issues not classified as mental illnesses was included in the most recent version of ICD-11 (2022). Mentioned in these are sexual dysfunctions, sexual pain disorders, gender incongruence, etiological factors in sexual dysfunctions and pain disorders, and other specific and undefined problems with sexual health. Though they are still classified as mental diseases, paraphilias were thought to fit under this category by many authors. Under ICD-11, it is classified under “Paraphilic Disorders” rather than “Disorder of Sexual Preferences,” as it was done under ICD-10. 36
In total, eight categories of paraphilic disorders have been mentioned in ICD-11. These include disorders such as voyeuristic behavior, exhibitionistic disorder, pedophilia, coercive sexual sadism disorder, frotteuristic disorder, other paraphilic disorders involving non-consenting individuals, paraphilic disorders involving solitary behavior or consenting individuals, and unspecified paraphilic disorder. It has, nonetheless, included sexual behaviors that are linked to a high risk of harm or death; nonsexual activities that bear a similar risk are not included in a diagnostic category that is comparable. 36
Laws Related to Paraphilias in India
The concept of paraphilia about normal versus abnormal behavior is constantly up for debate. The second aspect of paraphilia is that, under some conditions, a person with a paraphilia diagnosis may be imprisoned, foreseeing future harm to society. 37 With time, there have been changes in the law, and in this view, a major change came when the Indian Supreme Court ruled that “Section 377” of the Indian Penal Code, 1860, which criminalized consensual sexual conduct between adults of the same sex, was unconstitutional. The court argued that discrimination based on sexual orientation violated rights to equality, privacy, and human dignity and that fundamental rights cannot be denied based on population size. 38 The MHCA 2017 was one of the major documents based on which the Indian Supreme Court ruled that Section 377 was unconstitutional because it violated the basic rights provided by the Indian Constitution and discriminated against members of the LGBTIQ community based on their sexual orientation.39,40 Distinct nations and cultures have distinct laws about sexuality. The following list includes the many IPC sections, 41 and penalties have been discussed in Table 2.
Laws Related to Various Paraphilias in India.
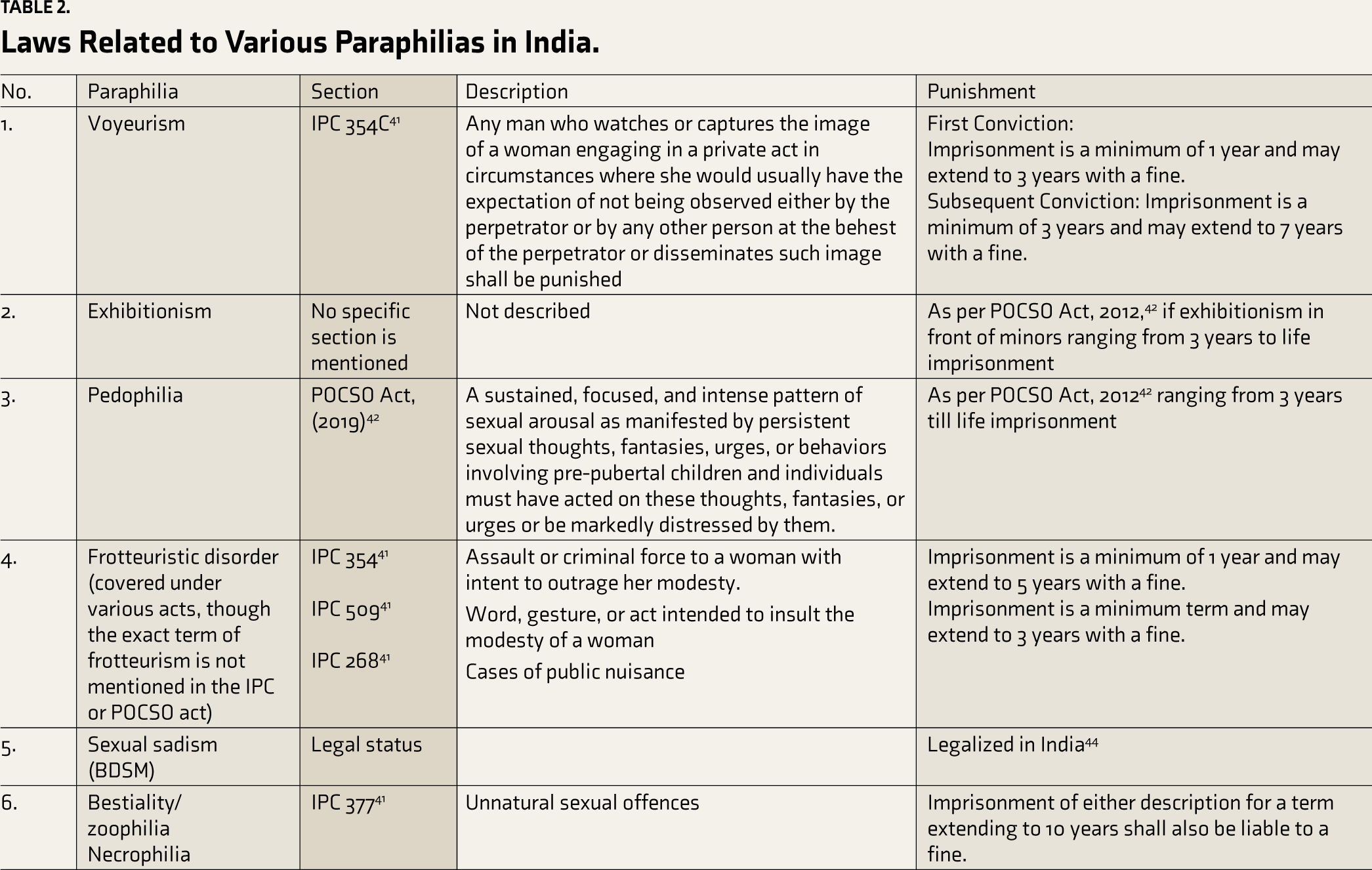
The POCSO Act, 2012, 42 and the JJ Act, 2015, 43 deal with all cases of children (less than 18 years); however, as shown in Table 2, some clear-cut laws are missing in Indian law.
WFSBP Algorithm of Pharmacological Treatment of Paraphilic Disorders.
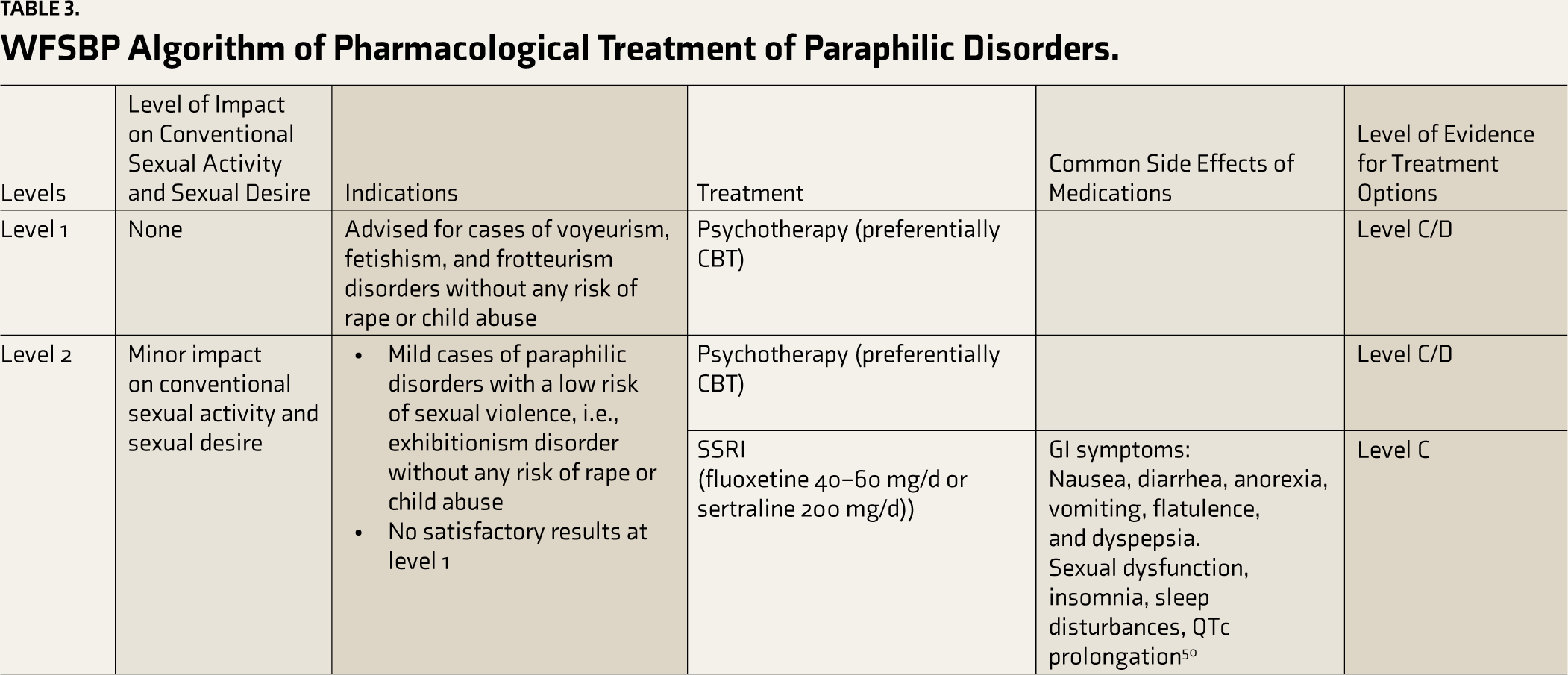
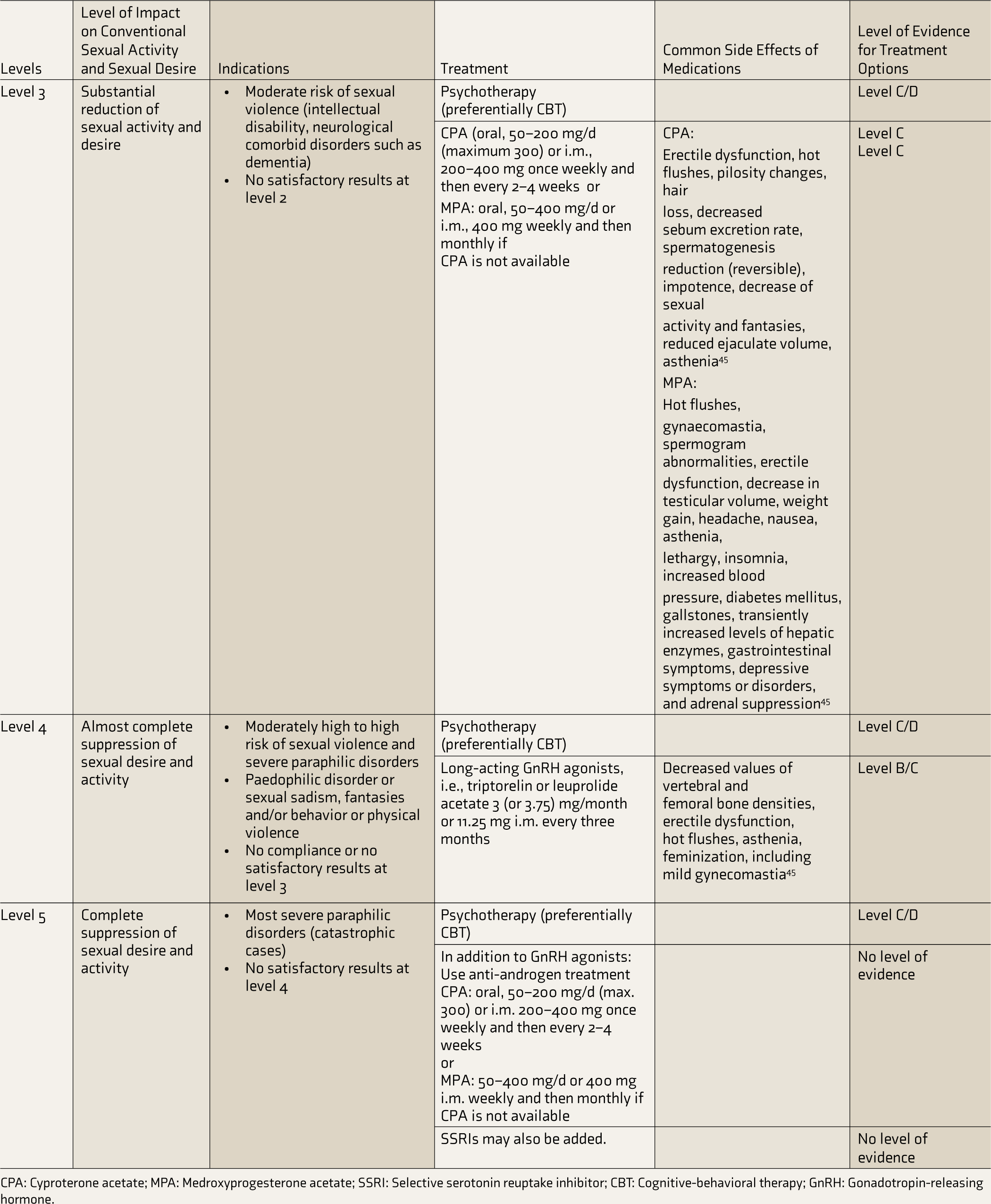
CPA: Cyproterone acetate; MPA: Medroxyprogesterone acetate; SSRI: Selective serotonin reuptake inhibitor; CBT: Cognitive-behavioral therapy; GnRH: Gonadotropin-releasing hormone.
Assessment and Formulation of a Treatment Plan for Paraphilic Disorders
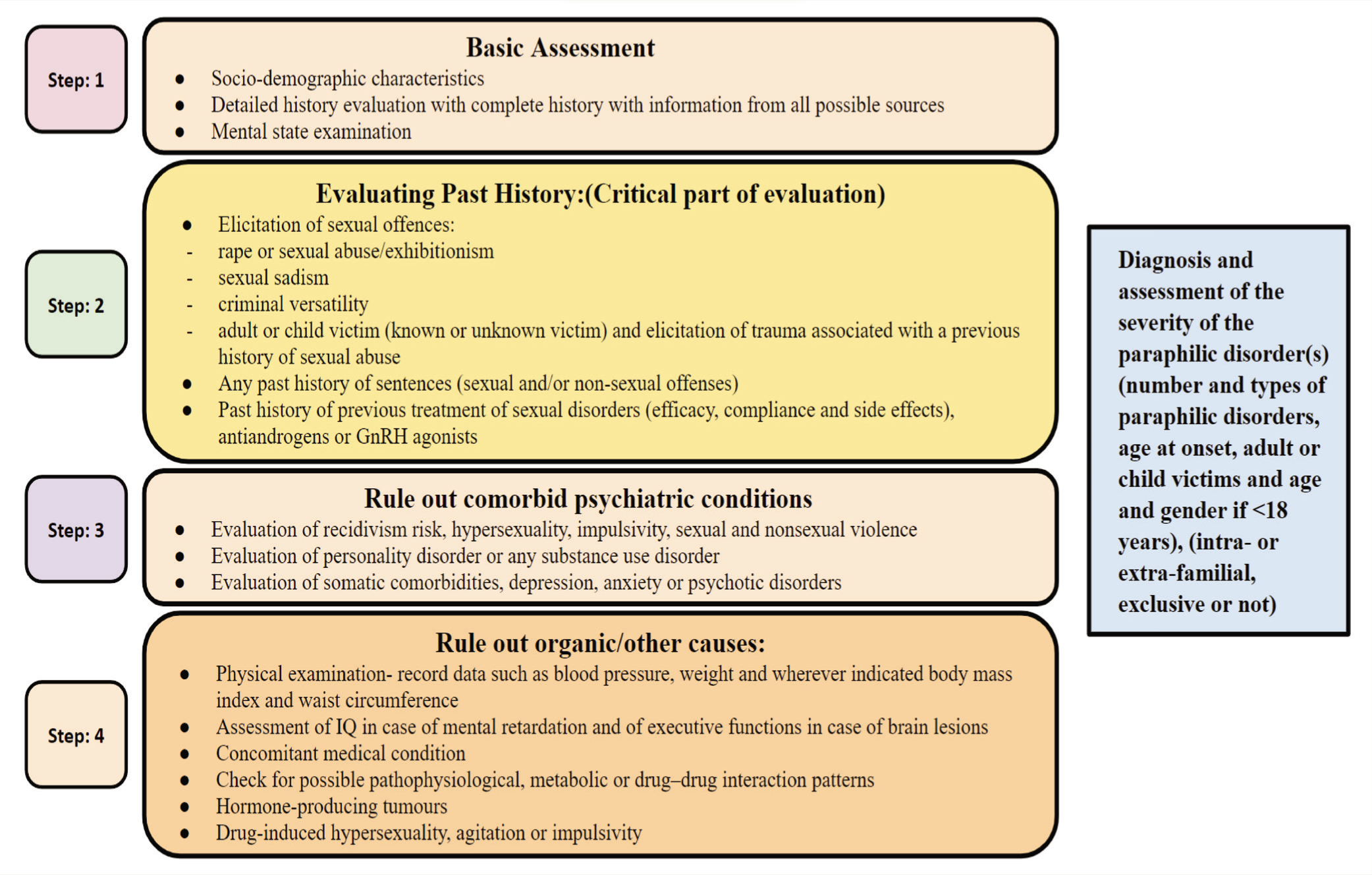
Evaluation of a person with paraphilic disorder needs special focus because of a very heterogeneous group of patient profiles. The aims of the baseline evaluation can be divided into four headings as follows:
44
Basic assessment: involving a detailed history evaluation with complete history with information from all possible sources and mental status examination Evaluating history: The most critical part of evaluation as it forms the basis to evaluate various underlying psychological causes and/or any past sexual abuse or any sexual offenses Ruling out comorbid psychiatric disorders Ruling out organic/other medical causes
Formulating a diagnosis based on the above four steps
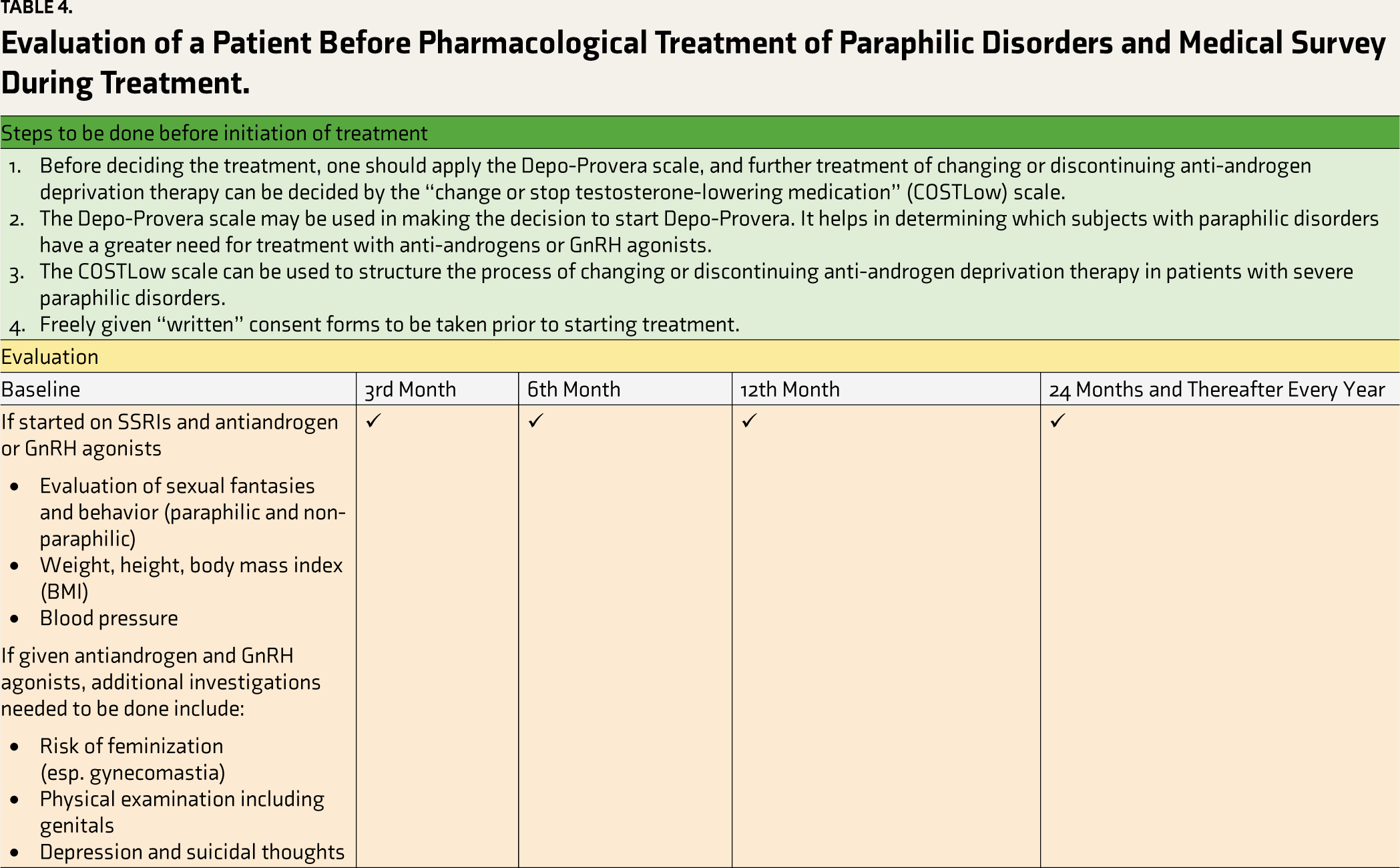
Finally, freely given “written” informed consent (with the help of their legal guardian if applicable) must be obtained from the subject if anti- androgen or GnRH agonist treatment is necessary. Numerous scales have been proposed to help in treatment decisions. A Depo-Provera scale may be used to start Depo-Provera.45,46 It has 13 items and helps in determining which subjects with paraphilic disorders have a greater need for treatment with anti-androgens or GnRH agonists, particularly those with a history of sexual offense or those at a high risk of sexual offense. A score more than or equal to 6 (maximum 17) on this scale of 13 items or the presence of three factors or two or more factors marked with ana could indicate hormonal treatment.
A change of stopping testosterone-lowering medication (Costlow) scale can be used to structure the process of changing or discontinuing anti-androgen deprivation therapy in patients with severe paraphilic disorders. It is a three-point ordinal rating scale with two points for “definitely present,” one for “possibly or partially present,” and zero for “absent,” which is used to score each factor of the COSTLow-Scale. A cumulative score and an overall assessment are generated by adding scores. The total assessment, which allows for considering changing or stopping testosterone-lowering medicine (TLM), is better supported by a higher sum score. There is no cut-off score. The limitation of the algorithm is that no prospective study on its effectiveness has been conducted.47-49
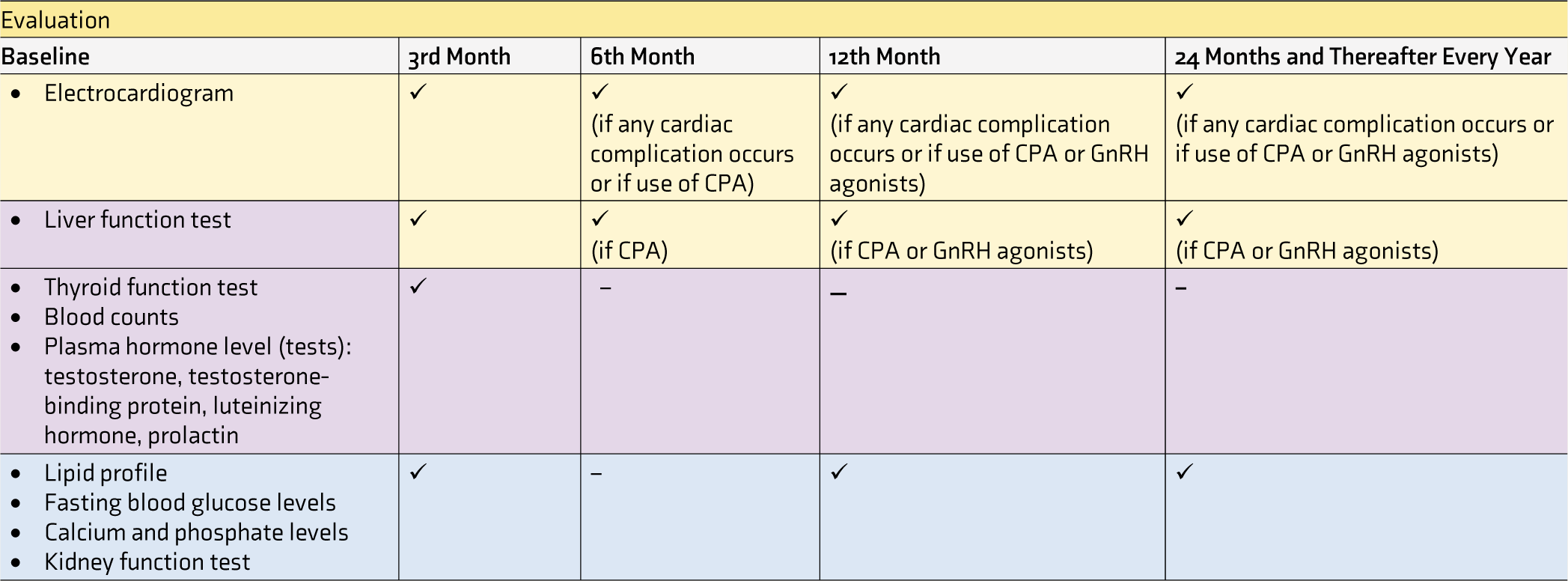
A basic evaluation of a patient before pharmacological treatment of paraphilic disorders and a medical survey during treatment should be done prior to starting any treatment, which includes investigations and scales. It has been summarized in Table 4.
Assessment of Paraphilic Disorders.
Evaluation of a Patient Before Pharmacological Treatment of Paraphilic Disorders and Medical Survey During Treatment.
Treatment of Paraphilias
An algorithmic approach was given by the World Federation of Societies of Biological Psychiatry (WFSBP) in 2010, 20 which was later updated in 2020. 45
The treatment choice for paraphilic disorders will primarily depend on the following factors:
A patient’s previous medical and psychiatric history A patient’s compliance The intensity of paraphilic sexual fantasies The risk of sexual violence
Treatment for paraphilic disorders atte-mpts to achieve either of the following:
To manage paraphilic sexual urges To prevent paraphilic fantasies and behaviors that might increase the likelihood of a sexual offense To help lessen the degree of suffering experienced by those who have a paraphilic disorder To promote sexual behaviors and interests that are not considered paraphilic
The WFSBP focuses its treatment strategy on two important aspects: the degree of impairment and the risk for harm. The program has five stages, each with increasing levels of intervention. Treatment ranges from SSRIs to synthetic steroidal analogs and gonadotropin-releasing hormones. Psychotherapy has also been recommended, but other than cognitive behavior therapy (CBT), no other type of psychotherapy is effective (Table 3). Written informed consent is mandatory for the initiation of treatment.
The hierarchy of treatment recommendations (concerning the stated degree of evidence) was determined using the following four categories:
Level A: The recommendation is well-supported by research. The proof was gathered from at least three reasonably sizable, positive, randomized, controlled, double-blind trials (RCTs), with at least one of the three investigations having to be a skillfully executed, placebo-controlled research. Level B: The recommendation is well-supported by research. Data were gathered from a minimum of two large, positive, randomized, double-blind trials or from one large, positive, randomized, double-blind study, as well as from one perspective, moderately large (with a sample size of at least 50 participants), open-label, naturalistic study. Level C: Minimal research-based evidence to support this recommendation. Evidence was gathered from a minimum of two prospective open-label studies/case series (with a sample size of at least 10 participants) or one randomized, double-blind study with a comparator treatment and one prospective open-label study/ case series (with a sample size of at least 10 participants) demonstrating efficacy. Level D: Expert views from authors and WFSBP Task Force members were used to gather evidence backed up by at least one prospective, open-label research or a case series with a sample size of at least 10 individuals.
Duration of Treatment
In cases with a moderate paraphilic disorder, the course of therapy should be continued for at least two years; if required, it should be prolonged for at least five years (if there is a significant risk of sexual violence). 45
Treatment Cessation
Treatment is to be stopped under two conditions:
45
If no change in sexual orientation or paraphilia is consistent with the treatment If 90% of cases of sexual violence and violent sexual fantasies return months or years after treatment withdrawal for a given paraphilia
Future Directions
This review also points out certain areas where Indian research is lacking, and those lacunae need to be filled in to understand the situation about paraphilias in the Indian context properly. First, there is a dire need for studies looking at the prevalence of paraphilias in India as more awareness and legal considerations have been at the forefront in recent times. An approximate number will help us reach out to the population needs to address the issues. Second, treatment guidelines have been formulated and need to be followed along with long-term follow-up studies to focus on the efficacy of the treatment guidelines. Third, the development of an Indian classification system is needed akin to the Chinese Classification of Mental Disorders (CCMD), Korean, and Japanese systems that have incorporated indigenous concepts with the contemporary classification system that would facilitate comprehension of cultural and religious beliefs based on rich ancient literature. It will not be a boon in classification only. It would also aid in diagnosing such an important concept with a high variability based on cultural and regional variations by Indian values, unlike the modern classification, which is not included. Fourth, studies on paraphilias and crime, such as those carried out in other nations, have to be carried out because sexual crimes may have underlying causes that indicate a higher prevalence of sexual sadism in addition to other diseases and interests associated with paraphilia. This has to be investigated from India’s viewpoint.
Limitations
There are certain limitations to this review, as some aspects were out of the scope of the review. This review does not describe the various historical facts prevalent in other parts of the world. It does not discuss how various interventions used in the treatment of paraphilias came into the mainstream. There is also no comparison of Indian laws with laws and legislations in the West in this review.
Conclusion
A gradual shift is noted in the description and classification of various paraphilias, which has been a matter of debate with an evolving civilization. Some of the paraphilias were removed from criminalized groups to non-criminal, and the laws and legislation are also making gradual shifts based on current societal norms. ICD and DSM have become more structured in the domain of paraphilic disorder and have been scrutinized based on current world norms, but this needs constant updating as the understanding is still evolving. The laws in India need to be more specific and streamlined, as multiple sections pose difficulty and raise legal noise in the common people’s minds. Guidelines have been stated, but their effectiveness and long-term follow-up studies have yet to be assessed, which raises concerns about the present range of treatment options. This review summarizes the current understanding of paraphilias, recent laws, and treatment and poses a question about it. Paraphilias has been treated as a foster child in psychiatry, as this has never been in the mainstream discussion from the treatment aspect. This review would add to the literature summarizing Indian issues in both legal and therapeutic aspects.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.