
Abstract
Background:
Adolescents are susceptible to using tobacco because of early exposure to tobacco through family members, easy access, or peer pressure. School-based educational programs are crucial for raising awareness of the harms of tobacco, thus preventing its uptake among adolescents. Studies conducted recently have recognized the need to bring change and reinforce ongoing school-based anti-tobacco education programs. Our study protocol aims to evaluate the effectiveness of a revised school-based anti-tobacco education on susceptibility to tobacco use among school-going adolescents.
Method:
Project TEACH (Tobacco Education and Awareness for Creating Healthier Adolescents) is an educational intervention that will comprise an animated video on the effects of tobacco on physical and mental health, along with dispelling myths about tobacco, which will be delivered along with a standard education program. The control group will only receive the standard school-based anti-tobacco education program. It will be conducted among students between 6th to 10th grade, with a sample size of 3,310 students.
Results:
Bivariate relations between the main socio-demographic characteristics and susceptibility to tobacco use will be tested using Pearson or Spearman’s correlation coefficients. For multivariable analyses, the binary logistic regression analysis is used to establish a risk model to correlate the socio-demographic factors with susceptibility to tobacco use and awareness of the harms of tobacco.
Conclusion:
Project TEACH aims to provide a sustainable school-based anti-tobacco education intervention. It will help test the effectiveness of the revised intervention, which could be incorporated into the current school education program being conducted in the district.
School education programs are critical for the primordial prevention of preventable risk factors. Project TEACH is an educational intervention developed to offer new insights into prevention strategies and strengthen the existing school-based anti-tobacco education program. This study focuses on curbing students' intention to experiment with tobacco products, which is often the pathway to actual tobacco use.Key Messages:
Tobacco use is associated with over 8 million deaths globally. 1 The noxious effects of tobacco are not limited to physical health alone and extend to the economy,2,3 environment,4,5 and overall growth of a country. Studies show a decline in the prevalence of smokers globally; however, they are still high in many regions of the world, including South-east Asian countries. 6 In India, the prevalence of current tobacco users among children aged 13–15 years stands at 8.5%. 7
The use of tobacco by family members and friends, easy availability, and novel marketing gimmicks are some of the ways through which children get exposed to tobacco products early in life. 8 The use of tobacco among children is a growing public health concern in India as the median age for initiation of cigarette, bidi smoking, and smokeless tobacco were reported to be 11.5 years, 10.5 years, and 9.9 years, respectively. 7 Children even trying a few cigarettes have a higher probability of being smokers in both early and late adulthood years of life. 9 Consumption of smoking and smokeless tobacco leads to various physical health issues such as impaired lung growth, reduced lung functioning, asthma, and early abdominal aortic atherosclerosis. 10 Exposure to tobacco smoke, in both direct and indirect forms, is known to lead to behavioral issues and emotional difficulties among children.11–13
Studies have reported that susceptibility to smoking is 11.8%, 14 while the incident smoking rate stands at 1.1% 15 among adolescents in a district in southern India. Susceptibility is defined as the lack of a firm decision not to use tobacco among never users. 16 Studies have highlighted susceptibility and often predicted tobacco use.17–19 A longitudinal study highlighted that those adolescents who were never smokers but were susceptible to smoking were four times more likely to have experimented with smoking. 20 Thus, showing that susceptibility is an important factor that needs to be targeted.
Educational programs in schools play an important role in generating awareness and preventing engagement in health-risk behaviors like alcohol use, tobacco use, illicit drug use, and antisocial behaviour.21,22 Over the years, various school-based interventions aimed at preventing tobacco use among children have been developed.23–25 Multi-component interventions like providing Information, Education, and Communication (IEC) packages, classroom activities, posters, and focus group discussions have been most commonly employed in schools and have been found effective in reducing tobacco use in children.23,26 Awareness about the harms of tobacco was also given as a part of a comprehensive health education program, which also included aspects like hygiene, bullying, mental health, substance use, diet, and physical activity.27–29 Peer-led interventions have also been utilized to prevent tobacco uptake among school-going adolescents.23,30 However, studies in the recent past highlighted the need for bringing a change in the anti-tobacco education currently delivered to students31,32 and recommended strengthening the ongoing school awareness sessions to influence behavior change at a younger age. 33
The current school-based anti-tobacco education program covers a wide range of topics like the ill effects of tobacco use and provisions of various statutes by the government. 34 Although school programs have been successful in raising knowledge of the long-term health risks associated with tobacco, they still reject the knowledge received because they cannot connect it to their experiences. 35 There is a need to educate on the immediate as well as long-term consequences stemming from tobacco use36,37 and using appropriate modalities for disseminating information.37,38 Thus, recommendations from various research studies have highlighted the importance of targeting efforts at school-going adolescents, with the prevention of initiation of tobacco at its forefront.
Project TEACH (Tobacco Education and Awareness for Creating Healthier Adolescents) is developed to strengthen the ongoing school-based anti-tobacco education program with the help of a short, animated video, along with a session on dispelling myths about tobacco use, which has yet to be systematically evaluated. Thus, our study aims to evaluate the effectiveness of this revised component to reduce the susceptibility to tobacco use among the school going adolescents. The proposed intervention trial is timely and important as it gives the opportunity to target susceptible school-going adolescents and augment the existing intervention.
Objective
Primary Objective
To evaluate the effectiveness of a revised school-based anti-tobacco education comprising of a digital story and dispelling myths about tobacco use on susceptibility to tobacco use among school-going adolescents compared to standard anti-tobacco education intervention.
Secondary Objective
To evaluate the effectiveness of a revised school-based anti-tobacco education comprising of a digital story and dispelling myths about tobacco use on awareness of the harms of tobacco among school-going adolescents compared to standard anti-tobacco education intervention.
Hypothesis
The null hypothesis for the study is as follows:
The revised education intervention will not lead to any change in susceptibility to tobacco use among school-going adolescents compared to standard anti-tobacco education intervention. The revised education intervention will not lead to any change in awareness of the harms of tobacco among school-going adolescents compared to standard anti-tobacco education intervention.
Trial Design
A two-arm cluster randomized control trial will be conducted across schools planned for visits in the academic year 2024–25 across a southern Indian district with schools as clusters. The schools will be stratified by type, that is, government, private, and aided. The protocol is reported according to the SPIRIT Guidelines. 39
Methods
Study Setting
The study will be conducted in schools that will receive school-based anti-tobacco education in a southern Indian district.
Eligibility Criteria
The study will include students (between 6th and 10th grade; age 11 to 15 years) who will receive the school-based anti-tobacco education program by the District Tobacco Control Cell in a southern Indian district. We will include schools with a strength above 25 students.
Students in school with special education and college students will be excluded from the study.
Intervention
The experimental group will receive a revised school-based anti-tobacco education, which will comprise standard school-based anti-tobacco education, an animated video on the effects of tobacco on physical and mental health, and dispelling myths about tobacco use. The revised education has been prepared based on the findings of our systematic review (unpublished data) and a qualitative study (unpublished data) carried out among teachers and students to explore ways to strengthen the current school-based anti-tobacco education program. The researcher will administer this session.
The control group will receive the standard school-based anti-tobacco education module, which focuses on the harms of tobacco, withdrawal symptoms, ways to quit, and tobacco control laws. 40
The education intervention for both groups shall be delivered in either English or Kannada, depending on the schools’ requirements. If the intervention provided to the experimental group is found to be effective, it will also be delivered to the control group after the study.
Outcomes
Primary outcome: Changes in susceptibility to tobacco use
Secondary outcome: Changes in awareness of the harms of tobacco
Outcome Measures
The primary outcome, susceptibility to tobacco use, will be assessed using four questions: Do you think you will try smoking soon? Would you try it if offered by your best friend next year or in college? Answering ‘no’ marks the student as non-susceptible to tobacco use. The secondary outcome, awareness of the harms of tobacco, will be assessed using a questionnaire adapted from previous research studies.
Operational Definition
Susceptibility to tobacco use is defined as the intention to use tobacco among new users in the future.
Standard school-based anti-tobacco education contains aspects like the harms of tobacco, withdrawal symptoms, ways to quit, and tobacco control laws.
Participant Timeline
The school principal will first be contacted to obtain permission to conduct the study. This will be followed by a session with the students to brief them regarding the study and distribute the participant information sheet and opt-out consent forms to seek parents’ approval for the study.
A second visit with the students will be scheduled after 7–10 days. During this visit, written informed assent will be taken from the students who have not returned the opt-out consent forms. A pre-test questionnaire will then be administered, followed by the delivery of the intervention.
Details of the Intervention Being Provided in the Experimental and Control Groups.
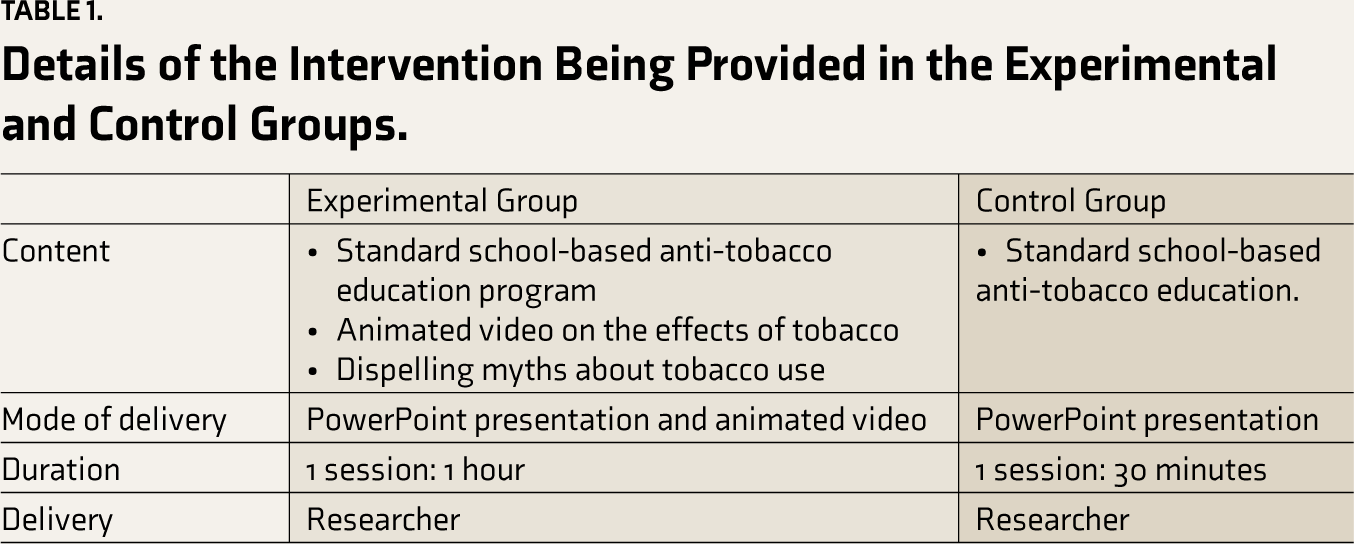
Project TEACH is primarily an educational intervention with two objectives: to reduce susceptibility to tobacco use and to generate greater awareness of tobacco’s harms among school-going adolescents. An outcome assessment after 7–14 days post-intervention will help assess short-term retention of concepts.
Sample Size
Considering the reduction in intention to tobacco use to be 1.2% more in the experimental group as compared to the control group in the previous study 23 with a 95% CI, 90% power, and 10% non-response rate along with a design effect of 1.5, the sample size estimated for the study is 3,310. There are five educational blocks in this district, with schools divided into government, aided, and private, along with the classification of rural and urban. Hence, for feasibility of executing the study, design effect of 1.5 was chosen. The authors estimated schools with a minimum of 25 students for the study. Schools will be approached till the desired sample size is attained.
Recruitment
School
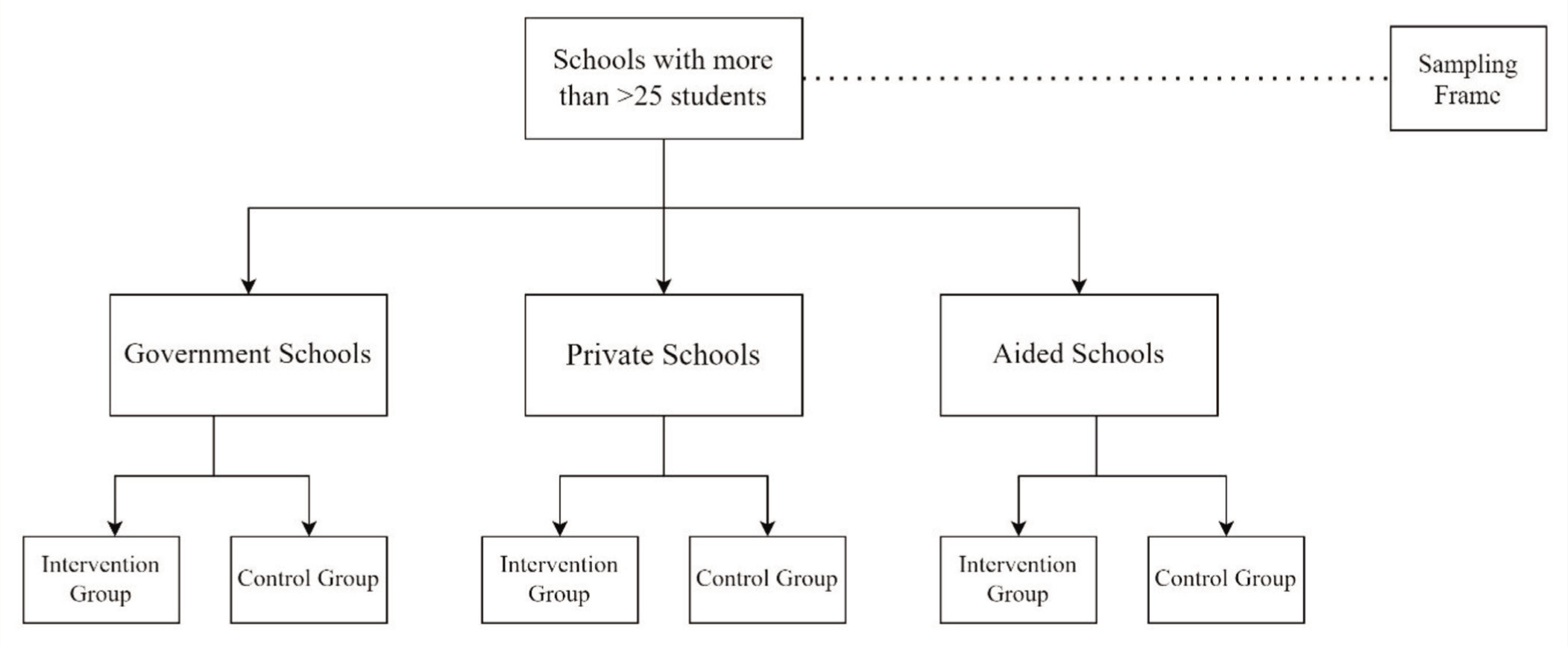
Every year, schools are selected to deliver school-based anti-tobacco education provided by the District Tobacco Control Cell (DTCC) under the National Tobacco Control Program (NTCP). From the above list, schools will be selected for the study. There are almost 700 government schools, 250 aided, and 200 private schools in this district, which brings the stratification to the ratio of 6:2:2, respectively. Figure 1 provides a pictorial representation of the sampling procedure. Randomization of schools into experimental and control groups will be done on the basis of block randomization, using a block size of four each.
Flowchart Depicting the Sampling Procedure.
Participant
Students (between 6th and 10th standard, aged 11–15 years) from schools participating in school-based anti-tobacco education will be invited to take part in the study. A prior visit will be scheduled to seek the parents’ consent through the opt-out consent process. After the parents’ consent, written informed assent will be obtained on the day the intervention is provided to students.
Data Collection Methods
Data collection will be based on a structured questionnaire, which will be adapted from the Prevention of Smoking Uptake Study, 15 Global Youth Tobacco Survey (GYTS), 7 and HRIDAY’s Mobilizing Youth for Tobacco-Related Initiatives. 26 This will be piloted before finalizing and will have questions that will assess socio-demographic status, exposure to tobacco use, awareness about the harms of tobacco, and susceptibility to tobacco use. The researcher will administer it. This will be administered before giving the intervention. Post-test assessment using the questionnaire will be done 7–14 days after the intervention is provided.
Data Management
The data will be collected through a paper-based questionnaire and entered by the study researcher. Furthermore, it will be stored in Microsoft Excel Sheets. These will be password-protected and accessed only by the research team members, ethics committee members, or any other regulatory bodies. Each participant’s data will be coded using a code (educational block number and section-roll number) that will help link the pre-and post-intervention questionnaire.
Statistical Methods
Data will be entered into a Microsoft Excel sheet and exported to SPSS Version 26.0 for further analysis. Frequency and percentage will be calculated from descriptive variables. Summary statistics will be presented for all outcome measures, with the relevant adjusted effect measures with 95% confidence intervals and p-values (at less than 0.05) from two-sided tests. Bivariate relations between the main socio-demographic characteristics and susceptibility to tobacco use will be represented using Chi-square tests or Fisher exact test for categorical variables and Pearson or Spearman’s correlation coefficients for continuous variables. For multivariable analyses, the binary logistic regression analysis is used to establish a risk model to correlate the socio-demographic factors with susceptibility to tobacco use and awareness of the harms of tobacco. Explanatory variables that were found to be significantly associated with outcome variables on univariate analysis (p<0.2) will be evaluated by multivariate logistic regression analysis. We will consider estimates to be statistically significant if the p-value from a two-tailed test is less than 0.05. As measures of association, the odds ratios (ORs), relative risks (RR), and 95% confidence intervals (CIs) will be calculated.
Monitoring
The data collected through the questionnaire will be made accessible to the institutional ethics committee (IEC) for verification during the bi-annual meetings. There is a minor increase over minimal risk in the study as it involves providing education awareness to a vulnerable population, namely children. No additional expense is to be borne by the child or the family for taking part in the study.
Confidentiality
Information and results from this study may be presented at meetings or published in journals without including the child’s name and personal identification. They will be completely anonymized in oral or written reports, thus preventing identification of study participants.
Data Availability
Information from the study records, including the child’s name, address, other details, and study results, will be kept confidential and will be reviewed only by authorized personnel from the sponsor or their representative, the ethics committee, or regulatory bodies. The data will only be made available to another individual if specifically permitted in writing. Upon considerable request, the anonymized data will be shared after the results are published in relevant journals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Dissemination Policy
The findings of the study will be presented at the district and state level Government meetings for tobacco control. The findings of the study will be disseminated to the scientific committee through publication in good-quality, peer-reviewed journals. Policy briefs will be made, and state government authorities will be requested to utilize the educational module in the ongoing school-based anti-tobacco education provided by the National Tobacco Control Program, thus keeping the outcomes of the study sustainable after the completion of the project.
Ethics Approval
The study received approval from the Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee (IEC 1: 298/2022) and was prospectively registered in CTRI (CTRI/ 2022/12/048098).
Informed Consent
The opt-out consent forms will be used to obtain prior consent from parents. Assent will be obtained from students whose parents do not exercise the opt-out consent on the day of delivering the school-based anti-tobacco education program before administering the pre-test questionnaire, which will be administered by a student researcher.
Protocol Amendments
In the event of any protocol amendment, the principal investigator will inform the Institutional Ethics Committee, which is responsible for approving the trial protocol amendments. The governing authorities will also be informed.