
Abstract
Background:
Indian medical graduates are expected to be lifelong learners, and medical teachers need to find newer and more engaging ways to help them hone their lifelong learning skills. Online learning can be a stepping stone toward this goal.
Methods:
We conducted a pre-post design interventional study in which 22 phase two MBBS students rated their self-directedness in learning using the Self-Rating Scale of Self-directed Learning (SRSSDL) at two points in time—before and after completing a 10-week online basic psychopharmacology module. Participant feedback was obtained regarding various aspects of the online modular learning experience.
Results:
The participants’ mean SRSSDL scores before and after the intervention were 231.31 ± 26.64 and 227.31 ± 31.33. The difference is not significant. The students’ scores at both points in time placed them in the “high” range of level of self-directed learning, leaving less realistic scope for a large change in the given time frame. Participant feedback was encouraging, with 19 out of 22 reporting that the overall learning experience was a “positive” one.
Conclusions:
Second-year medical students’ self-reported self-directedness is high. Online modular learning may be a feasible addition to medical education, even though it may not increase self-directedness in the short term. A limited sample size can lead to type 2 errors.
Keywords
Phase two medical students rated themselves as highly self-directed. The online modular teaching intervention was engaging and aroused participants’ interest in psychopharmacology. More than half reported it helped them reach stated learning objectives, set their own goals, and allowed autonomy and flexibility. Although the self-directedness scores didn’t change significantly, these are key components of becoming self-directed and lifelong learners. A small sample size may lead to false negatives (type 2 error).Key Message
Malcolm Knowles defined self-directed learning (SDL) as “…a process in which individuals take the initiative, with or without the help of others, in diagnosing their own learning needs, formulating goals, identifying human and material resources for learning, choosing and implementing appropriate learning strategies, and evaluating learning outcomes.” Although the National Medical Commission (NMC) has increasingly emphasized SDL sessions in the new undergraduate curriculum, there needs to be more clarity and understanding regarding how SDL sessions must be carried out.
Self-directed learning ability involves a gradual transition from the teacher-led education that students are used to from school. The inculcation of SDL skills through scaffolding is extremely important, and we must facilitate the process as teachers. 1 SDL skills typically are promoted through various interactive teaching–learning methods such as group discussions, peer-to-peer teaching, seminars, debates, quizzes, and problem-based learning sessions.2,3 The coronavirus disease 2019 (COVID-19) pandemic forced a shift to online medical education with prolonged suspension of all interactive and small group sessions that normally foster SDL. Now, all stakeholders have become more comfortable with this altered educational atmosphere and have embraced online methods that are suitable for local needs in this post-COVID-19 time.
Asynchronous online learning offers to bridge the route from teacher-led to self-directed learning. It allows students flexibility with respect to time and place of study, autonomy in learning, and allows for multiple reviews, which are features that aid SDL.4,5 Well-designed and interactive modules make the experience even more engaging by opening up virtual discussions and assessments for feedback and grading. Utilizing easily available resources to develop simple online modules is a feasible teaching strategy for some knowledge competencies. Dedicated learning management systems (LMS) provide an excellent platform for more sophisticated teaching–learning experiences. Once created, online modules require little investment, mainly for updating information, engaging with learners, and reviewing assignments. This allows students to do the learning in a self-directed manner and frees the teachers to act as facilitators of deeper learning. Asynchronous teaching–learning also offers a realistic solution to the gaps created in medical education due to declining student attendance in real-time classroom teaching sessions.6,7
Despite the recent interest in SDL among medical students in India, most of the published work measures students’ perceptions regarding SDL or their estimates of their self-directedness.8,9 There needs to be more literature on how newer, technology-assisted teaching–learning methods can help facilitate self-directed learning skills. An Iranian study identified “prescription medications” among the top ten topics identified by faculty and students that could be included in MOOCs (massive open online courses) in undergraduate medical courses. 10 Pharmacology is a subject often perceived by students as difficult. They also have been reported to feel that traditional didactic methods need to be supplemented by other teaching–learning methods. 11 Students also report low levels of confidence in their knowledge and application of it.11–13 Others have also noted that such subjects/ topics are suitable to be taught via SDL. 3 Inspired by the MOOCs available on wide-ranging topics within medicine, we wanted to examine how online modular teaching–learning of psychopharmacology can foster SDL skills among students and their perceptions of this method.
Method
This was a single-group pre-post-design interventional study conducted at a medical college after approval from the Institutional Ethics Committee. The teaching intervention and data collection began on July 10, 2021, and ended in October 2021. Students from the second phase of MBBS were invited to participate. We aimed to examine the effect of an online modular teaching intervention on self-reported self-directed learning among phase two MBBS students.
Objectives
We conducted this pilot study to expand our understanding of how online learning affects SDL. Our objectives were 1. to measure SDL scores among the students before and after the teaching intervention and 2. to examine the association between SDL scores and specific socio-demographic variables.
We selected the pharmacology competency to describe mechanisms of action, therapeutic doses, adverse effects, indications, and contraindications of medications used in the treatment of common mental illnesses (competency “PH 1.19” of the CBME) [Medical Council of India, Competency-based Undergraduate curriculum for the Indian Medical Graduate, 2018. Vol. 1; p. 110]. The psychopharmacology module was created accordingly by the first author, and three faculty from the Department of Psychiatry examined it for content validity.
We used Google Classroom (GC) as we had a subscription to Google Workspace. The module contained six units (details in supplement provided):
Each unit consisted of:
Specific learning objectives A clinical case scenario for set induction in the form of cartoon strips /short write-ups Video lecture(s) Additional web-based reference materials A self-assessment quiz with answer keys for feedback List of recommended textbooks/ learning resources
One unit was uploaded to GC each week, and the module remained available for another four weeks after the last to allow the participants time to use it, given they had their routine classes, activities, and assessments going on during the study. We encouraged participants to utilize the “stream” feature as a discussion forum. The GC landing page for a classroom is typically the stream page, which facilitates teachers’ and students’ posting of messages and updates.
Tools Used for Data Collection
We used a semi-structured questionnaire to obtain demographic information. Self-directed learning was rated using the self-rating scale of self-directed learning (SRSSDL)—a valid and reliable self-administered tool to estimate one’s self-directedness in learning. 14 The tool provides information across five domains of SDL—awareness, learning strategies, learning activities, evaluation, and interpersonal skills. There are 12 items in each domain rated using a 5-point Likert scale. Scores range from 60–140, 141–220, and 221–300 (interpreted as “low,” “moderate,” and “high” self-directedness in learning, respectively). Permission to use this tool was obtained from the author. SRSSDL was applied before and after completing the module. Student feedback was obtained using a semi-structured questionnaire.
Our sampling strategy was convenient and voluntary. The sample size was estimated assuming an increase in self-directedness scores by 30 ± 20 after teaching intervention using the formula below:
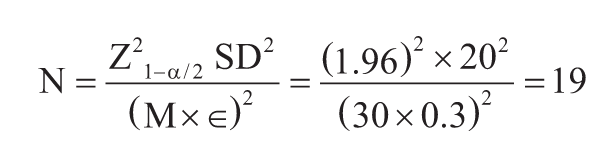
(where M is the mean change in SRSSDL score, where Z is the statistic for a 95% level of confidence, SD is the assumed standard deviation, and ϵ is precision = 0.3 or 30%) Assuming an attrition of 10%, we arrive at a final sample size of 19 + 2 = 21.
All documentation was completed online using Google Forms and Google Classroom.
Statistical analysis included descriptive statistics and t-tests (paired and unpaired). We used the STROBE guidelines for reporting. 15
Results
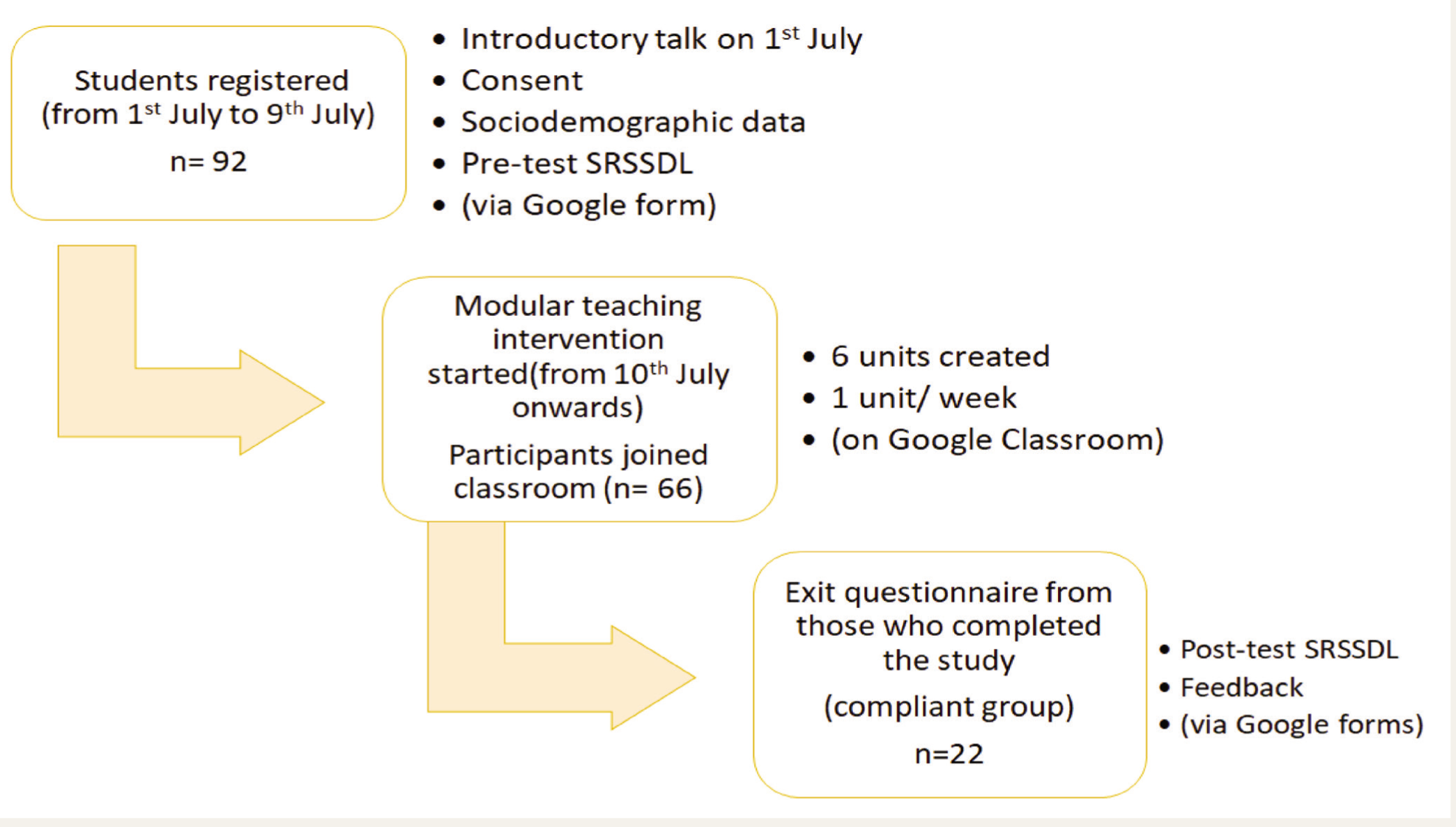
Ninety-two second-year MBBS students consented to participate at the outset, out of which 66 joined the Google Classroom. At the end of the study period, 22 students had completed the module and filled out the postintervention SRSSDL and feedback form. Data from these 22 students were used for analysis (refer to Figure 1).
Brief Flow of the Study.
Participant characteristics are tabulated in Table 1. The mean SRSSDL score of 70 participants who initially filled out the entry forms but did not complete the postintervention SRSSDL assessment and feedback (noncompliant group) was 233.61 ± 25.78, which puts them in the “high” self-directedness range. This is similar to the entry SRSSDL scores of the 22 participants who completed the modular intervention-compliant group (231.31± 26.64).
Participant Characteristics (n = 22).
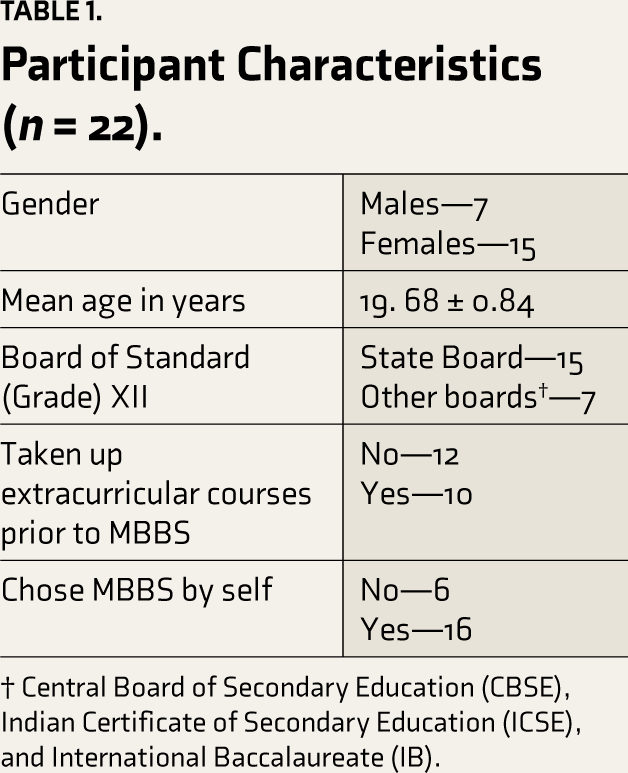
† Central Board of Secondary Education (CBSE), Indian Certificate of Secondary Education (ICSE), and International Baccalaureate (IB).
Scores on SRSSDL before and after the modular teaching–learning intervention were examined, and results are tabulated (Table 2). We did not find any significant change in self-rated self-directedness before and after the intervention.
SRSSDL Scores Before and After Online Modular Teaching Intervention (n = 22).
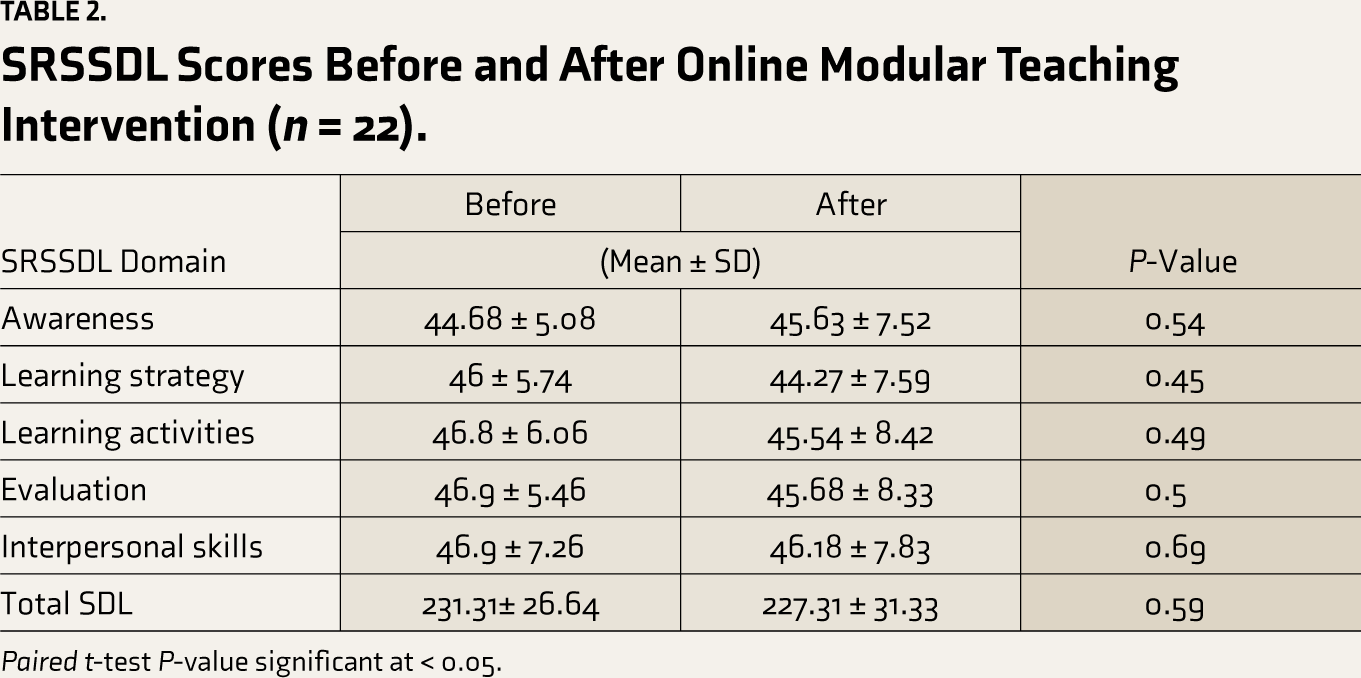
Paired t-test P-value significant at < 0.05.
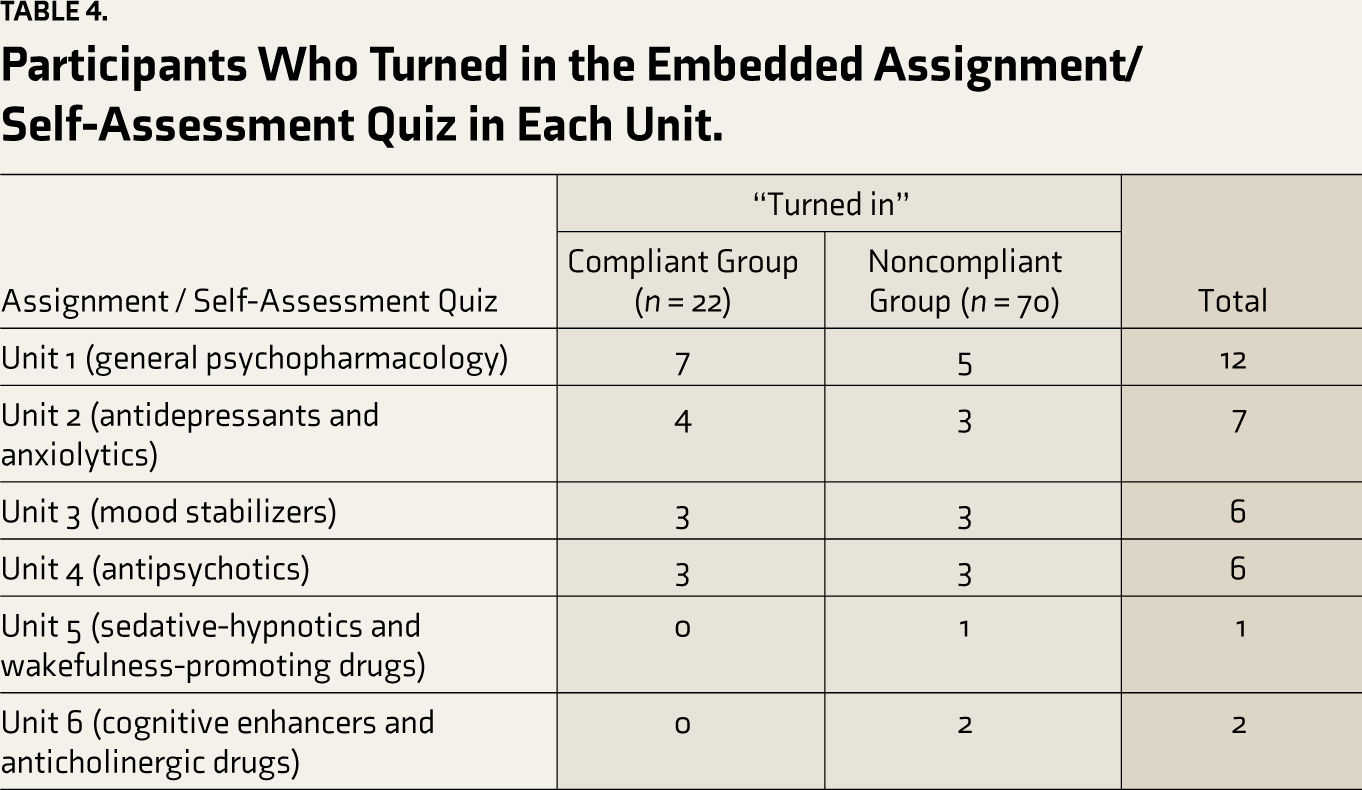
Students who had completed standard XII from state boards rated themselves lower in all domains of the SRSSDL compared with students from other boards (CBSE, ICSE, IB). The difference was significant for total SDL score and awareness, learning strategies, learning activities, and interpersonal skills domains before the modular learning intervention. All these became statistically insignificant after the intervention. The participants from the state boards rated themselves as more or less similar at both periods, while those from other boards rated themselves as lower after the intervention (Table 3). Differences in SRSSDL scores before and after intervention on the basis of choice of studying MBBS and prior experience with undertaking extracurricular courses were not significant. Table 4 shows the number of participants who turned in the embedded assignment/ self-assessment quiz in each unit.
SRSSDL Score Differences Between State and Other Board-Educated Students for Standard (Grade) XII.
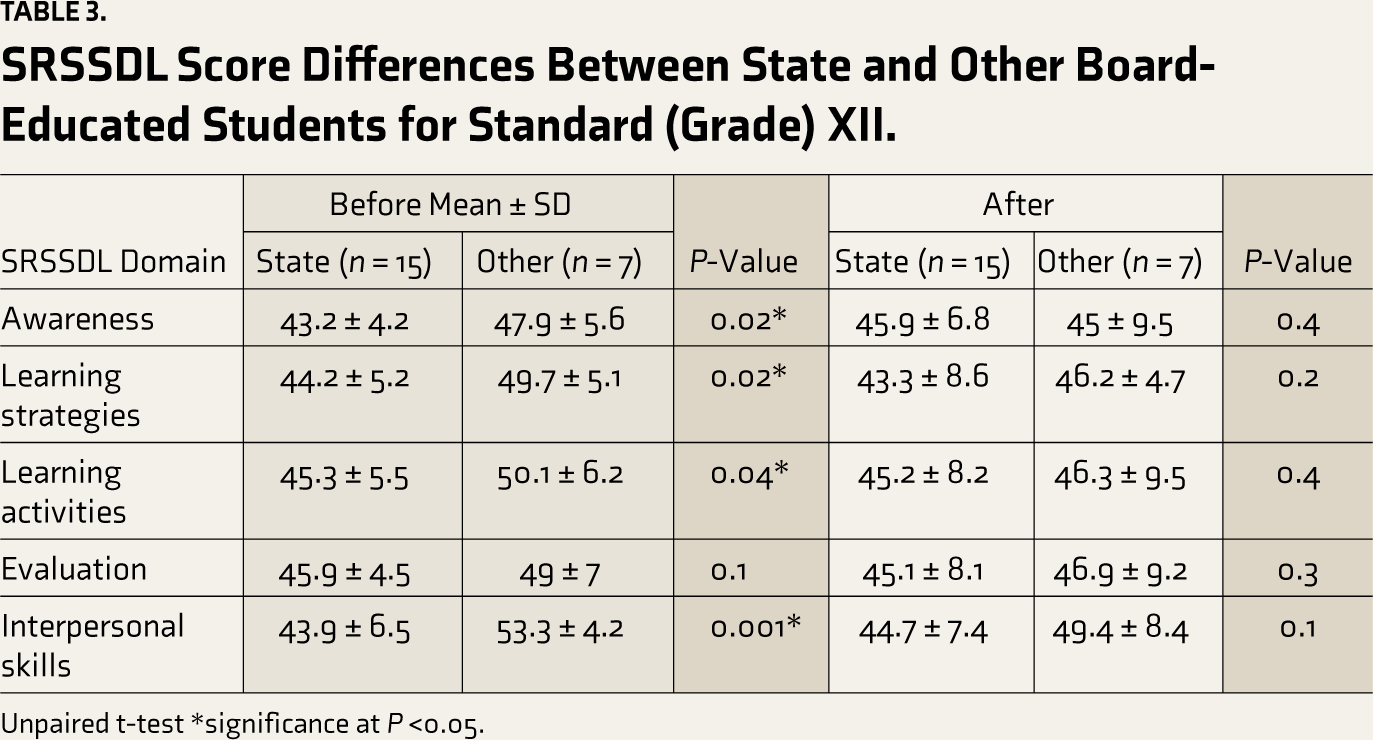
Unpaired t-test *significance at P <0.05.
Participants Who Turned in the Embedded Assignment/ Self-Assessment Quiz in Each Unit.
Discussion
Previous studies on MBBS students using the SDL Instrument (SDLI) reported that the participants rated themselves quite high on self-directedness.16,17 An interesting cross-sectional study of SDL readiness (SDLR) among undergraduate medical students in different years of training, performed at Christian Medical College, Vellore reported that self-rated SDLR scores progressively reduced from first year to internship, and the difference in the mean scores was significant. 8 Students in the early first year had a mean SDLR score in the above-average category, while interns’ mean score was close to below-average (228.21 and 202.11, respectively). Our study participants also rated themselves as highly self-directed in learning at entry, and the rating did not change significantly at the end of the study. There are studies where self-directedness has been found to reduce progressively during graduate study, irrespective of the course and curriculum followed.9,18 While it is established that SDL occurs when the learner aims for deep learning, the vast curriculum and limited time forces students to adopt surface and strategic learning approaches extensively. This may explain why overall self-directedness decreases throughout medical training. Additionally, SDL is affected by multiple factors such as personal interest, learning culture, age, curriculum, and individual characteristics. 8 Low self-efficacy and anxiety hinder self-directedness. 19 We believe that rating themselves in the high SDL range at the beginning of the study itself reduces the scope for a realistic significant increase in scores, especially after brief interventions like ours. Indeed, the scaffolding approach to teaching self-directedness requires long periods. 16 Interestingly, participants from grade XII boards, other than state boards, rated themselves higher on the SRSSDL across all the domains.
A Korean study surveyed self-directed learning skills/behaviors among medical students undergoing synchronous and asynchronous (through online meeting platforms and recorded video lectures, respectively) online classes during the COVID-19 pandemic. 20 The study reported high SDL skills scores among its participants and concluded that online learning environments must create opportunities that foster SDL skills, such as goal-setting. Our module provided clearly stated learning objectives, induction case scenarios, video lectures, and reference materials, including links to websites for a deeper understanding of topics, and self-assessment quizzes. Subjective SDL information can be supplemented by direct observation of student behaviors. Some LMS such as Coursera, Edx, Moodle, and Canvas, provide useful analytics like time spent on module contents, number of page views and clicks, forum engagement, etc., which can be valuable indirect indicators of SDL-features that GC lacked. Administrative issues, skills deficits, learner motivation, time constraints, cost and access to the Internet, lack of social interaction, and technical problems have all been reported as potential barriers to online learning.21–23
Ninety-two students initially consented to participate in our study, out of which 66 joined the GC, and 22 completed it within the stipulated time frame. Going by the definition of SDL, where the learners must set their own learning goals and objectives and proceed, it is impossible to replicate this in its entirety early in training. Teachers must take the lead and set the objectives. In fact, students have reported the need for help in finding correct learning resources, too. 16 Students and faculty participants of a study defined SDL in such a way that “..the emphasis of SDL was only in how and where the learning occurs—not on what”. 9 Students expected the “what” to be provided by the faculty, which is what we did. In that sense, we were facilitating self-paced learning through the module. The reader must recognize that SDL skills are not acquired en masse but through smaller steps, including self-paced and self-regulated learning experiences. 1 A lack of experience with online learning and the felt need to undertake a study of psychopharmacology at the time of the study may explain the attrition following initial consenting. Twenty-six of the 92 participants initially reported having had at least one prior experience with online/ blended learning. Of these, eight participants were in the compliant group.
Twenty compliant participants felt that the clinical case scenarios in each unit improved their learning experience. The number of assignments/ quizzes turned in by the end of the study period was quite small. The assignments were designed to be formative, emphasizing feedback to the students, and were ungraded, which may have affected their motivation to complete them. Some students may have utilized the assignments as tools for self-evaluation without actually submitting them. Indeed, 21 participants reported that the assignments helped them review their learning progress. Some assignments were also turned in by students who were in the “non-compliant” group, which shows the utilization of materials extended beyond the 22 compliant participants. Fifteen participants reported utilizing most of the reference materials given in each unit. Our findings replicate those of Lew and colleagues, who found that despite an expressed preference to learn asynchronously online, student utilization of online resources provided was quite poor. 4
In spite of deficiencies, online learning is almost as good as offline learning, and it is becoming more acceptable among medical students.24,25 Regular use of asynchronous online learning during undergraduate years can make learners more comfortable determining their learning needs, finding, and appropriately utilizing resources such as MOOCs or scientific texts, and managing their time to achieve their goals.
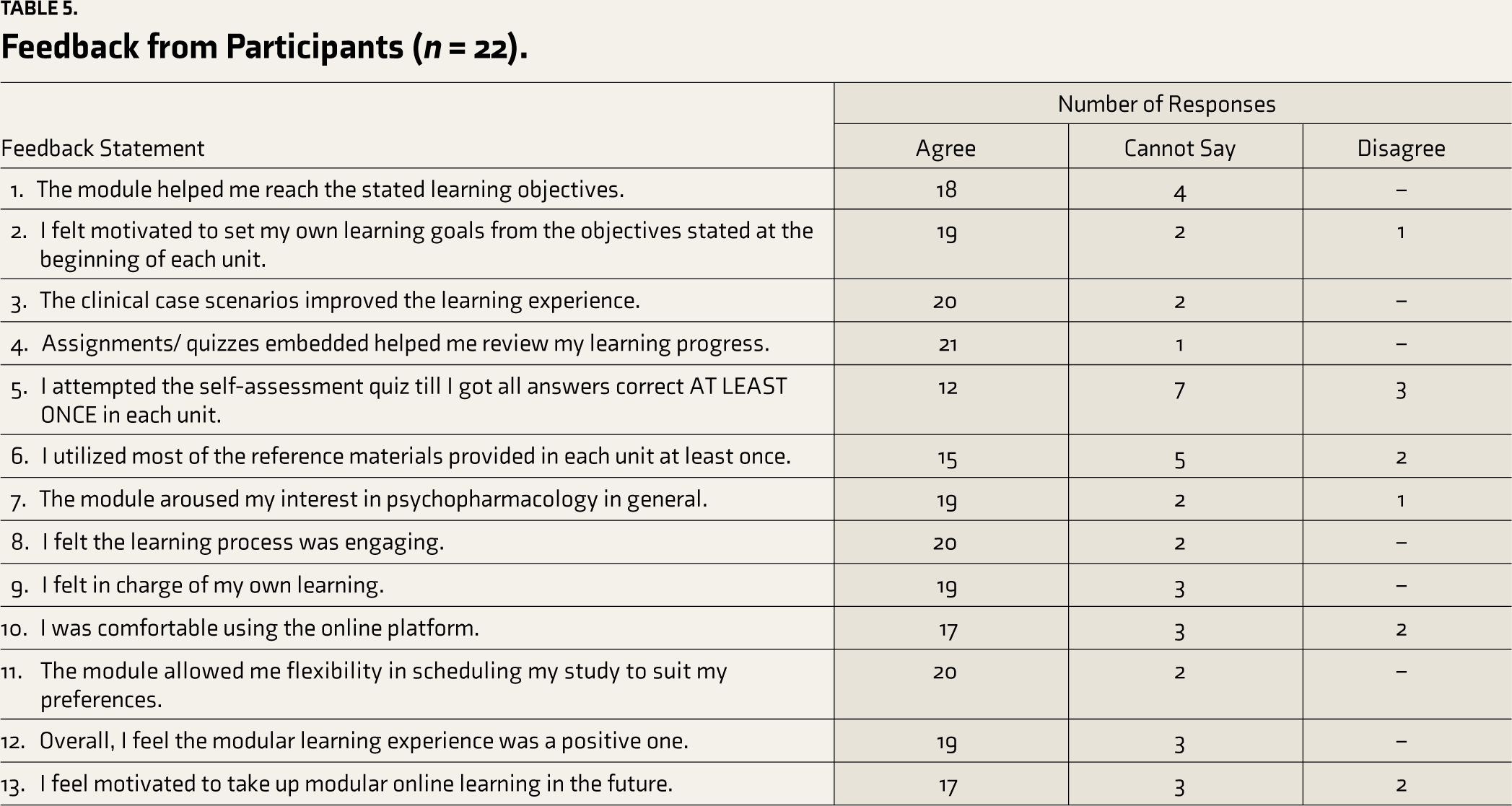
Feedback obtained from our participants was encouraging. The feedback obtained has been tabulated (Table 5). There was more than 50% agreement between them that the module helped them reach stated learning objectives and set their own goals; clinical case scenarios and quiz assignments were helpful; the module was engaging and aroused interest in psychopharmacology; and it allowed autonomy and flexibility. Overall, 19 students felt that this learning experience was a positive one, and 17 reported feeling motivated to take up similar online learning opportunities in the future. Seventeen students reported feeling comfortable using the online platform.
Feedback from Participants (n = 22).
Limitations
Despite frequent attempts to engage the participants in discussions, there was only one such interaction with a student during the entire study period. The module was developed by faculty from the Department of Psychiatry, which is a clinical subject in the final year of MBBS. This may have created a hesitation among the students to interact. A few warm-up meetings with the faculty, weekly group discussion sessions, and involvement from faculty in pharmacology could have resulted in greater student engagement. The challenges of fitting everything in the hectic post-COVID-19 year affected interdisciplinary coordination. Ongoing events such as scheduled assessments, central nervous system topics in pharmacology not being scheduled in the timetable at the time of this study, and other commitments likely hindered the prioritization of the module and did not create the felt need at the time. These are challenges that real-world medical students and teachers have to face. Due to the post-pandemic staggered return to campus, we were unable to include any small-group discussions, which might have better-facilitated student engagement.
Conclusion
The study has set the stage for phase two students and teachers to become comfortable with online learning, beginning with a simple platform such as Google Classroom. By providing a framework for self-directed study, we have created the necessary scaffold to facilitate SDL and know that students have a better understanding of how to proceed with self-directed study should they feel motivated to utilize various online learning opportunities as a result. We also recognize that SDL scores would change over a much longer period and with multiple learning opportunities throughout medical training. With the experience from this pilot study, we have modified the modules for students of subsequent batches to utilize.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received the Indian Teachers of Psychiatry (IToP) MUST ENRICH Research Grant from Minds United For Health Sciences and Humanity Trust, Mysore, India for conducting this study.
Institutional Ethical Committee Approval
Number – Original Article (protocol number: 222/ 2020-2021; IEC Certificate: KIMSDU/ IEC/ 05/ 2021 dated 8-6-2021).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.