
Abstract
The types of clinical rotation and organizational strategies are considered crucial for quality postgraduate training as they affect diverse clinical experiences and exposure, peer interaction, teacher–student interface, and the overall working environment. There is strong evidence that a planned clinical rotation, clear goal, organization functionality, and a psychologically safe learning environment help learners and teachers organize themselves better. 1
Like any other medical speciality, psychiatry training is known for its specific requisites. Comprehensive psychiatry care necessitates a multidisciplinary approach, detailed history taking, repeated mental state examinations, time-consuming psychotherapeutic interventions, and longitudinal engagement of the patients. Conventional psychiatry training centered around protracted observations and exhaustive documentation of patients during the era of mental hospitals (now better known as Institutes of Mental Health). General hospital psychiatry units (GHPUs) gradually became the primary site for postgraduate psychiatry training. In India, the transition still comes with challenges.2,3
One of the biggest challenges was meeting the demand for high-standard postgraduate psychiatry training despite limitations in infrastructure, workforces (primarily to provide psychosocial interventions), inpatient capacity, and public health interventions.3,4 Moreover, exposing postgraduates to diverse clinical and training experiences, having robust formative assessment strategies, and teaching the desired attitudes in a limited training period leaves no scope to waste precious training time.
Proportional and adequate exposure to crucial clinical areas, such as outpatient, inpatient, drug addiction, psychosexual medicine, community psychiatry, psychotherapy, consultation-liaisons psychiatry, and child and adolescent psychiatry, in three years postgraduation is a challenge that demands well-planned clinical rotation and careful utilization of limited resources in GHPUs.
GHPUs providing postgraduate psychiatry degree courses can be divided into two broad categories: one belonging to medical colleges under the National Medical Commission (NMC) and the other belonging to Institutes of National Importance (INIs). The former has an annual system; that is, postgraduate entries and final degree exams are conducted annually and follow a yearly curriculum system. The latter has a biannual system; that is, postgraduate entries and final degree exams occur every six months, and have adopted a semester system.
The traditional annual examination system is inherited from the British method of medical education; however, subsequent universities and INIs, including GHPUs, essentially adopted an alternative semester system for higher medical education promoted by the Bologna declaration. 5 It offers the advantages of frequent assessments, feedback, a better student–teacher interface, and a better learning trajectory.6–8
There are various strategies and approaches to overcome these training challenges. Unfortunately, we do not have sufficient literature to support or evaluate the effectiveness of any of these approaches. The biggest hurdle is the lack of uniformity and inconsistency in the functioning of psychiatry departments and training.9–11 Still, we attempt to understand two fundamentally distinct approaches commonly adopted in the GHPUs: a multiunit system with inter-unit clinical rotation and a nonunit system with time-based clinical rotation. Here, we evaluate the clinical rotation styles and unit and nonunit organizations in GHPUs.
Multiunit System and Unit-Wise Clinical Rotation
The multiunit system is widely used; the NMC also advocates it for broad clinical specialities with relaxation to small departments with day-care services. 12 In a typical multiunit system, a prescribed strength of faculty, trainees, staff, and teaching beds is grouped into units, which are also used as a yardstick for recognition of postgraduate seats specified by the NMC. Hence, depending on available resources, GHPUs in medical colleges that function under the NMC have a monounit or a multiunit system. Each unit has fixed days of outpatient and inpatient activities; the patient seen on a particular day by a unit shall be admitted under the name of the unit head, a senior most faculty in the unit, and the clinical care of the patients shared by the unit consultants. Similarly, the unit conducts its other clinical rounds on fixed days and times so that its activities do not clash with those of different units. In a classical multiunit system, the trainee undergoes periodic interunit clinical rotation for a significant proportion of the training period. This rotation is usually combined with peripheral postings in a time-based manner (Figure 1).
A Multi-Unit Organization with Interunit Clinical Rotation and its Merits and De-merits.
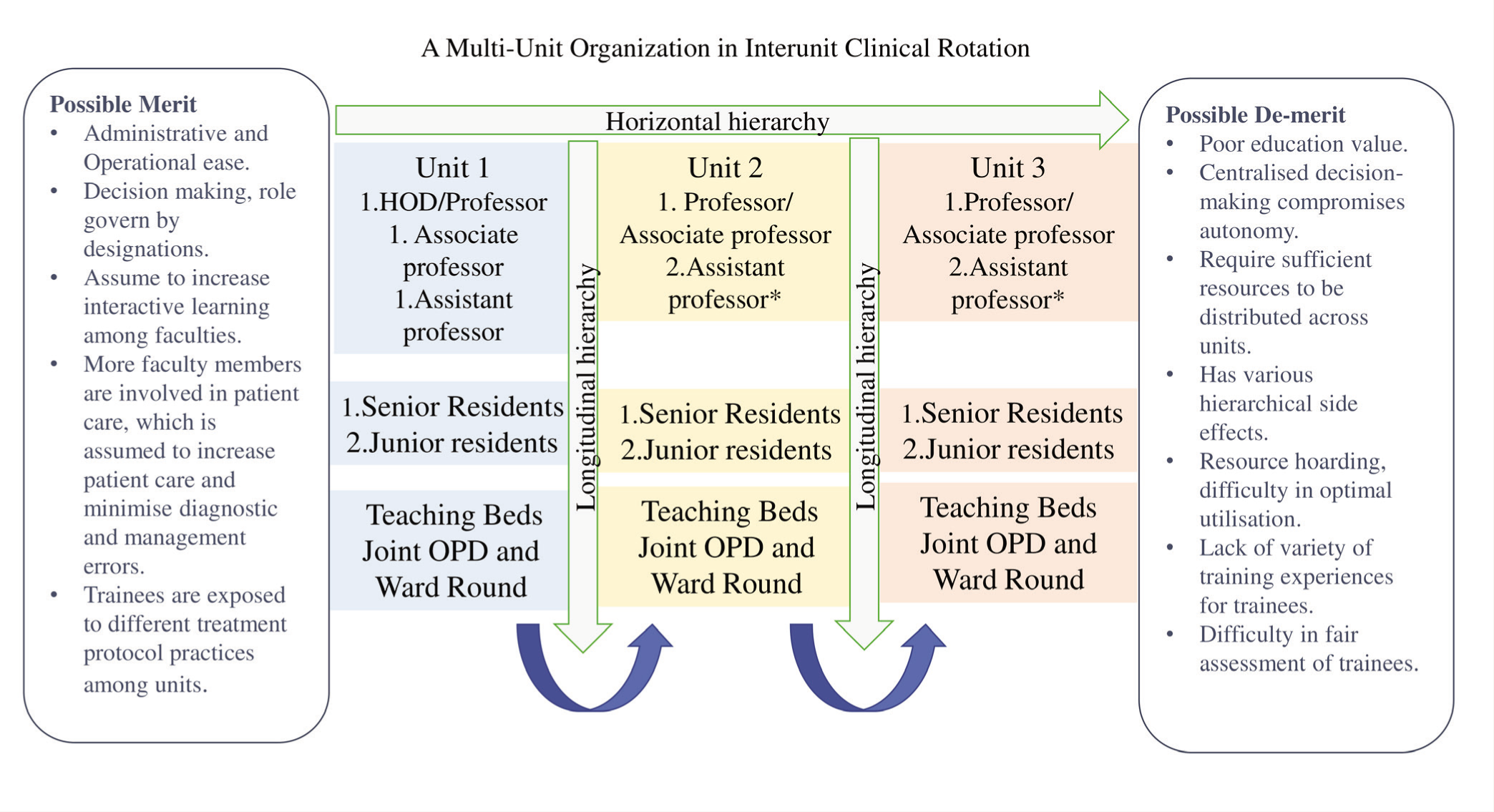
A multiunit approach can have merits and demits regarding the training environment training and assessments system. Classically, a unit represents a hierarchical organization where faculties are placed longitudinally and horizontally based on their seniority status. The unit system has apparent advantages regarding operational and administrative ease; the roles, responsibilities, and decision-making based on seniority statuses possibly allay interpersonal conflicts and facilitate interactive learning among unit members. 13 It may also preferred in larger clinical departments that involve frequent high-stakes decisions, such as critical medicine and surgical specialties, to slacken diagnostic and management-related errors. It helps expose trainees to various treatment protocols followed between the units.
However, a hierarchical approach is criticized for centralizing decision-making, compromising the autonomy of junior faculties, hindering their growth, creating communication barriers promoting an “Us or “Them” work culture, and delaying patient management.14–17 Moreover, resource distribution is often unequal and biased based on seniority; hoarding resources leads to imbalance and can compromise patient care.15–17, 19 Grouping consultants may curb individual freedom of time management, affecting appointment handling, hindering the establishment of longitudinal therapeutic relationships, interfering with expressing personal style and originality, and decreasing initiatives and work satisfaction.15,18
The involvement of multiple consultants in case management can result in contradicting or haphazard instructions and produce moral dilemmas for the trainees. 19 The bureaucratic nature of the unit can directly or indirectly affect the trainees, as they are the ones who observe the faculty and their dynamism. The imprinting of hierarchical culture reflects a penchant to push responsibilities down the hierarchy; legitimizes mistreatment and harassment, a tendency to cajole senior faculty, subjected to a “hidden curriculum” causes moral distress; enhances stress, fatigue, and burnout; and lowers training satisfaction among trainees.19–22
The functioning and nature of work in all the units are grossly similar; therefore, interunit rotation is criticized for needing more diversity in training experience and a justified utilization of training time. Sometimes, additional services or special clinics can run under a unit, adding a layer of intraunit clinical rotation within the unit rotation. However, we should remember that clinical rotations should be simple and conducive to standard formative assessment strategies.
The authenticity of formative assessments relies on multiple unbiased assessments by various assessors in different settings and meaningful feedback that requires a much more equitable environment. Contemporary evidence-based medical education discredits the educational value of a hierarchical framework.20–22,23,24
A Nonunit System and Time-Based Clinical Rotation
A non-unit approach is fandamentaly distinct from the multi-unit system and is commonly followed in clinical departments, super specialities, and GHPUs belonging to INIs. In contrast to a multi-unit organization, a non-unit approach does not have group consultants based on seniority and does not have an inter-unit clinical rotation either. The individual faculty are authorized to admit, discharge, and sign hospial indents related to the patients under their care, entrusted as a treating consultant.
The department is divided into distinct functional domains based on the nature of work, clinical care, type of service, and specific training requirements, for example, out-patient department (OPD), in-patient department (ward), psychotherapy, consultation-liaison service, community psychiatry, drug-de-addiction service, neuromodulation, child and adolescent, and marital psychosexual services etc. Each domain has a specific standard operating procedure (SOP) for its operation under the supervision of nominated faculty. The senior and junior residents are given time-based clinical rotations in these domains, with specific learning objectives (SLOs) assigned with responsibilities as needed for service and training.
The approach may have been innovated and adopted in clinical departments of INIs, including GHPUs, for specific reasons for postgraduate training. The presence of a semester system, as students enter every six months, results in a higher student–faculty ratio, biannual degree exams, and increased academic and training load requiring higher faculty supervision. A nonunit system and time-based clinical rotation provided a much simpler, feasible approach with optimal utilization of limited resources.
The nonunit approach with a time-based clinical rotation has several training advantages. It fundamentally provides a functional approach, disengaging the usual hierarchical network from clinical care and training, cutting down bureaucratic hindrances in routine functioning, clinical care, training and assessment, resulting in quicker decision-making, better communication, and better clinical and training outcomes.17,18,22,24 Hierarchy is restricted for administrative purposes while flattening down to bring the individual consultant to the forefront to take up more responsibilities, boosting productivity and utilizing resources more effectively. 25
Clinical, training, and administrative responsibilities are distributed based on choice, interest, expertise, and faculty experience in their respective areas. A better communication interface between the faculty and clear roles and responsibilities help cultivate an environment of coexistence, mutual respect, and understanding. Moreover, exposure to administrative, clinical, and training skills during an early professional period helps faculty members harness their best potential, inculcate leadership quality, prevent sudden leadership crises, and may even stabilize the system with mutable and rotational headship. 24
Resource allocation is carried out according to the area’s requirements based on the condition rather than an obligation to divide it among units or seniority status, which enables better resource utilization and enables one to devise some crucial clinical training areas that are often neglected, such as psychotherapy training, 26 marital and psychosexual, consultation-liaison, 27 and psychology rotation in GHPUs (Figure 2). The approach has the flexibility to allocate resources to more needy areas. For example, GHPUs usually require a robust outpatient service due to limited inpatient bed capacity; much of the acute management and close follow-ups for chronic illness need to be done on an outpatient basis. This invokes better bed economic strategies and diverts resorces and more residents into the out-patient clinical rotation.
A time-based clinical rotation offers several training advantages. It is more structured and “learner-centred” (Figure 1). It reduces unpredictability, multiple instructions, and shuffling between different duties. It enables trainees to focus on the task, prioritize work, and develop time management skills, providing better opportunities for harnessing trainees’ potential and reducing work stress, burnout, and depression.1,28
As most trainees start with the core clinical rotations that are inpatient or outpatient service areas, they get an opportunity to interact with all consultants as they are required to discuss cases with respective consultants, unlike the multiunit system, when one set of trainees is exposed to one set of consultants at a time. The clinical rounds are conducted by individual consultants, with the senior and junior residents posted in the inpatient department (IPD) discussing cases under their care, allowing surplus time to have in-depth discussions and attention on each patient due to the lesser number of cases being discussed at a time.
The time-based clinical rotation also provides flexibility in arranging sequence and time duration, with varying levels of difficulties, nature of work, and competencies, allowing strategic controlled exposure to the trainee and consistency in the training framework (unlike multiunit system where inconsistency is observed between the units) (Figure 2). The academic load, on-call, or night duties are also moderated, keeping the nature of clinical rotation in mind; trainees posted in clinical areas demanding close patient care (e.g., ward and consultation liaison rotation) can be exempted from other duties so that patient care is not compromised.
A Non-Unit Organization with Time-based Clinical Rotation and Its Utility in Postgraduate Psychiatry Training in GHPUs.
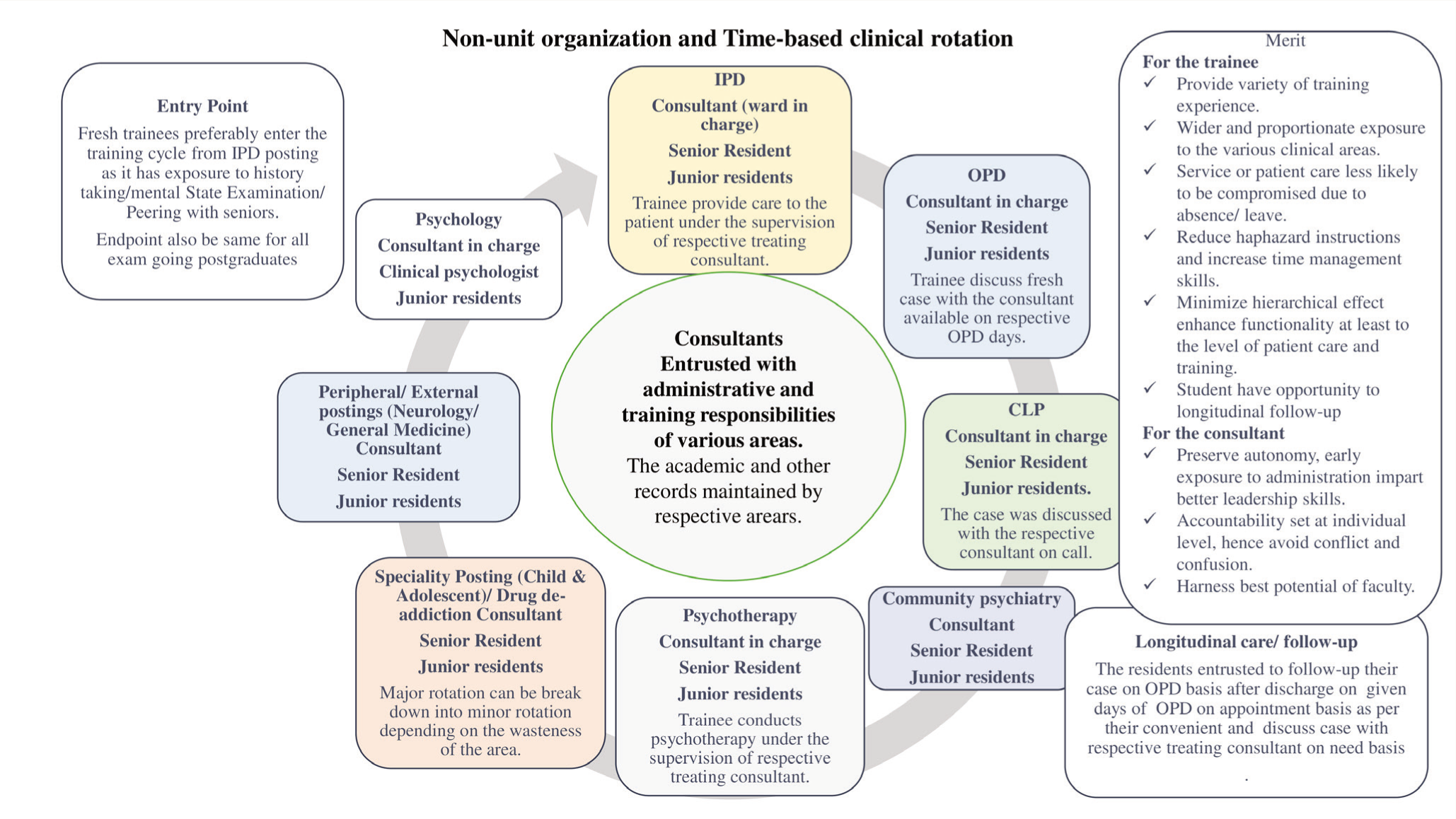
The nonunit approach and time-based clinical rotation offer more diversity and depth in training experiences. Well-defined role responsibilities and duties factored by time and clinical area make it simple to keep track of training and performance and are also conducive to work-based assessment 29 ; it is relatively more conducive to routine formative assessments free from bureaucratic barriers, provides more authentic feedback, and allows students to self-assess their strengths and weaknesses.1,30
Besides the above-mentioned organization, a mixed approach is followed in some GHPUs, which have an annual and semester system. A multiunit system with interunit clinical rotation is constituted while admitting patients under individual consultants within the unit, unlike under the head of the unit. Two variations are found to be followed: first, an adaptation similar to the classical multi-unit system, i.e., the clinical rounds are conducted jointly by the consultants of the unit, and the unit consultants share patient details and clinical decisions. Therefore, It shares similar merits and demerits as a classical multi-unit system. It shares more or less similar merits and demerits as a classical multiunit system. Second, it allows the individual consultant to have their separate clinical rounds, preserving the clinical autonomy of the treating consultant. Here, the rounds need to be conducted in different time frames by individual consultants of the same unit depending on the number of faculty in a unit and the number of non-outpatient department (OPD) days given to that unit.
Knowing each system’s training advantages and disadvantages is essential since the number of GHPUs has increased exponentially. More than two dozen new GHPUs under INIs, that is, All India Institutes of Medical Sciences (AIIMS), have been initialized in the last few years, recruiting faculty from different training backgrounds. It is essential to be mindful of setting up an organization that keeps clinical care and training in its core values. The clinical rotation should be strategically structured to guide trainees through challenges and a specific set of competencies. Nevertheless, the organization should be simple, feasible, and conducive to the fair assessment of trainees and faculty using appropriate resources.
Nevertheless, our discussion may have limitations as it is primarily based on the authors’ opinions and experiences from different GHPUs regarding the organisational and type of clinical rotation adopted. The inability to use a structured, systematic evaluation and a statistically valid method may leave scope for ambiguity and debate on several points. Moreover, no on-site observation was performed to validate their experiences. In the future, a statistically appropriate evaluation can provide substantial inferences.
Conclusion
Organizational approaches and clinical rotational styles can have a robust impact on the training and learning environment, faculty involvement and initiatives, clinical care, teacher–student interface, interpersonal communication pattern, diverse training experience, and authenticity of assessments. Setting up a framework and clinical rotation requires considerable deliberation to make it a rich learning environment with optimal resource utilization for high-quality training so that many benefits do not bleed away.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The authors shared their experiences regarding the strategies adopted officially by the department. Hence, the institutional ethics committee waived off the need for consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.