
Abstract
Background:
The current sensory assessment measures for autism spectrum disorder (ASD) have issues related to cultural and clinical applicability, which makes them difficult to apply in the Indian context consistently. The current study aimed to explore locally relevant themes for sensory reactivity in children with ASD.
Methods:
This exploratory phenomenological qualitative study was carried out on 15 parents of children with ASD visiting the child guidance clinic. An in-depth interview (IDI) guide was prepared on the conceptual framework based on Dunn, as well as, Miller’s models, which was then further refined based upon the inputs from the experts (psychiatrists, child psychologists, speech-language pathologists, and occupational therapists) working with children with ASD. IDIs were conducted with parents of children with ASD. The data was recorded in audio and video format. It was transcribed and translated from Hindi to English. Coding was done manually, and themes were extracted.
Results:
The findings identified four superordinate themes: sensory hyperreactivity, sensory hyporeactivity, sensory seeking, and socio-emotional response.
Conclusion:
The lived experience of parents aids in identifying and describing dimensions of sensory reactivity in children with ASD. It will help further in developing a valid and reliable instrument for the assessment of sensory reactivity in children with ASD.
Keywords
This study tried to depict and understand the lived experience of parents of children with ASD for sensory reactivity through in-depth interviews. The exploratory phenomenological analysis was carried out to extract the themes of sensory reactivity in children with ASD. Themes: sensory hyperreactivity, sensory hyporeactivity, sensory seeking, and socio-emotional response.Key Messages:
Autism spectrum disorder (ASD) is a neuro-developmental disorder characterized by social interaction, communication difficulties, recurrent repetitive behavior (RRB), and interests or activities. 1 Joint attention problems, poor eye contact, a lack of social connection for communication, poor social imitative play, an obsession with sensory inputs, repetitive and stereotypical behavior patterns, and activities are some of the early indicators of ASD. Complex interactions between genetically driven and environmental epigenetic factors lead to ASD. 2 In India, 59 out of 100 children are diagnosed with ASD. 3 The global rate ranges from 0.60% to 1.0%. The ratio of men to women is 4.2:1. 4 Various reasons, such as modifications to the diagnostic criteria and heightened awareness of the condition, can account for the rise in prevalence. 5
Sensory abnormalities are a common trait that is frequently missed in children with ASD. In children with ASD, rates of sensory processing dysfunction have been reported to be as high as 90%,6-9 while in the general population, they are estimated to be 5%–16%.10,11 The DSM-5 now lists sensory disturbance as a symptom within the repetitive behavior domain of ASD. The DSM-5 criteria define this type of symptomatology as either an extraordinary interest in sensory parts of the environment or an enhanced or diminished responsiveness to sensory input. 1 In several prospective studies, atypical sensory reactivity has been found in infants and toddlers who were later diagnosed with ASD, suggesting a potential precursor to an ASD diagnosis. 12
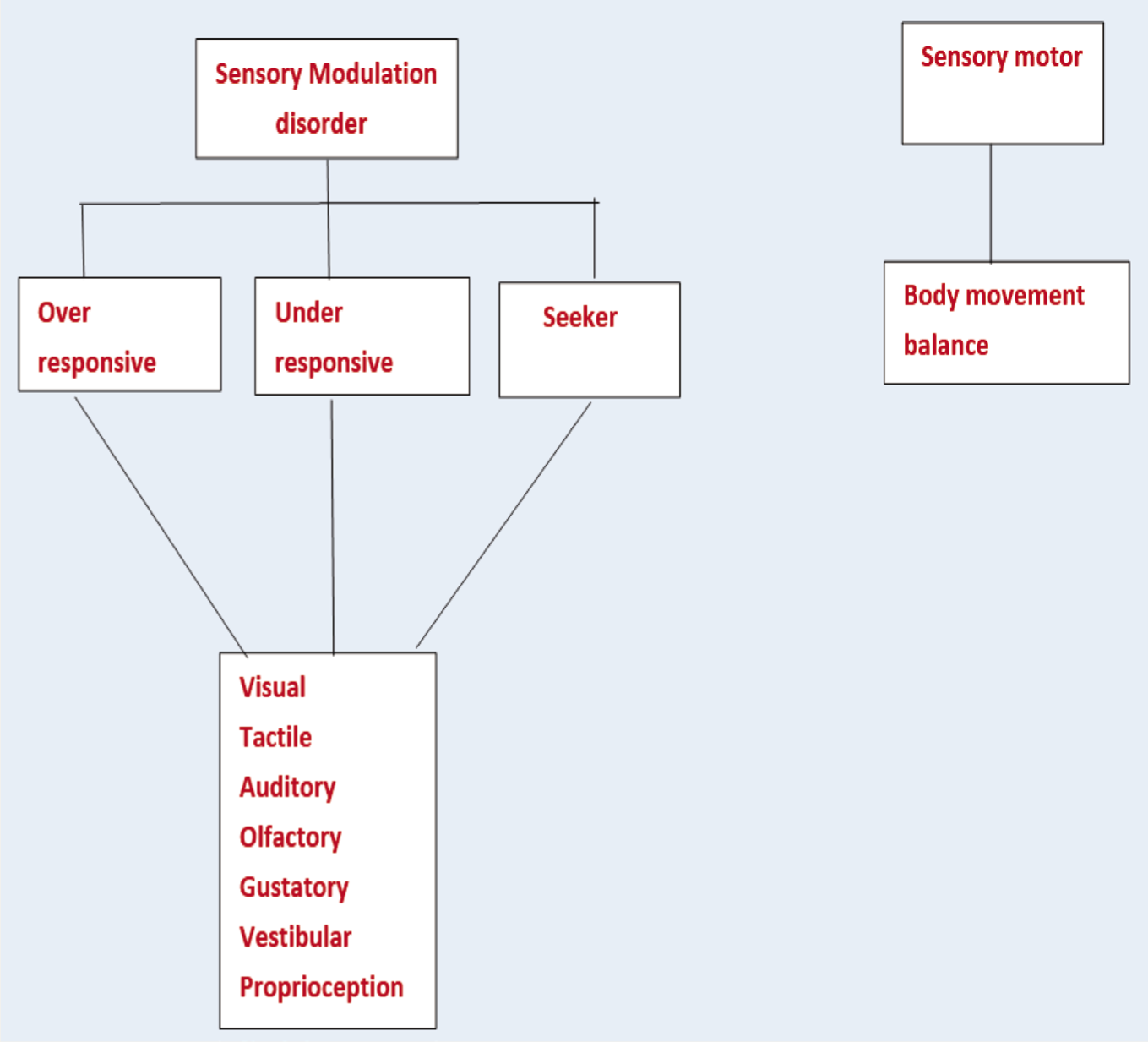
Different authors have proposed various models of sensory reactivity. Ayers was guided by the principle that “intersensory integration is foundational to function since problems with sensory integration can impede learning, development, and emotional control”. 13 Dunn described four primary forms of sensory modulation dysfunction based on an individual’s threshold and responding techniques. 14 The domains proposed were low registration, sensory seeking, sensory sensitivity, and sensory avoidance. According to Miller, sensory processing deficits are of three types: processing issues that impact modulation (sensory modulation disorders), motor planning (sensory-based motor disorders), and sensory discrimination (sensory discrimination disorders). 15 Poor motor planning or postural instability caused by inefficient processing of sensory information are classified as sensory-based motor disorders, which can manifest as disorganized or immature movement patterns. 9 The failure to comprehend differences and similarities between information gathered through the senses is referred to as sensory discrimination disorder. A group of illnesses known as sensory modulation disorders are defined by alterations in the consistency and kind of behavior in response to sensory input. 15 It has been proposed that sensory over-responsivity, sensory under-responsivity, and sensory seeking are three subgroups of sensory modulation disorder.16,17 While Ayers’s theory focuses on a child’s ability to process and internally integrate sensory information from the internal and external environments, which is a basic and generalized view of the sensory reactivity of a child. In contrast, Dunn emphasizes the child’s response to a threshold of stimulus. Therefore, it only included only sensory modulation. The Miller model is more comprehensive and includes most of the dimensions of sensory processing (sensory modulation, sensory discrimination, and sensory-motor). Hence, we utilized both models for our conceptual framework, which included thresholds of stimulus (Dunn’s model) as well as dimensions of sensory processing (Miller’s model), excluding sensory discrimination, which is minimally observed in ASD.
There are tools developed for sensory reactivity assessment based on these models. Some of them are short sensory profile, sensory profile, Glassgow sensory questionnaire, and Sensory Over-Responsivity Scales (SenSOR). Items developed in these scales are showing difficulty in application in the Indian context, and the language of the items is quite unrelatable to Indian parents. Most of the tools used are so extensive, take too much time to administer, and lack precision. There are also gaps in the understanding of the parent’s perspective in relation to sensory issues in children with ASD. To address this issue, we are attempting to explore the sensory reactivity in children with ASD through parent’s narratives, which will be further helpful in developing a sensory assessment tool that will better suit the Indian context with comprehensive and precise themes that can fit all aspects of sensory reactivity in children with ASD.
Material and Methods
Participants and Setting
The present study had an exploratory phenomenological qualitative study design. It was conducted from June 2022 to November 2023. Institute ethics committee approval was obtained before including the subjects in the study. The sample for the present study consisted of parents (n = 15) of children with ASD who were clinically diagnosed as per DSM-5 criteria (aged between 2 and 6 years), attending the child guidance clinic in a tertiary care center. No assent was obtained from children with ASD as they were below 7 years of age; parent written informed consent was obtained for the in-depth interview (IDI). The parents were interviewed individually for about 45 minutes to an hour. The standards for phenomenological research were taken into consideration for the study. Parents of children with autism who came to the child psychiatry consultation clinic willing to participate in the study and who were able to give adequate information about their child clearly were selected for an IDI.
Instrument
The interview guide was developed on a conceptual framework based on Dunn as well as Miller models14-15 (Figure 1). Further, Sensory Profile 2, which is based on the Dunn model, was taken into consideration for the development of the interview guide. It is a caregiver questionnaire consisting of 86 items under four quadrants of seeking, avoiding, sensitivity, and registration; scored on five point Likert scale for assessing the levels of severity: (1-almost never (10% or less), 2-occassionally (25%), 3-half the time (50%), 4-frequently (75%), and 5-almost always (90% or more). 18 A sample questionnaire was developed, which was then refined based on the inputs from the experts (early interventionists- psychiatrists, child psychologists, speech-language pathologists, and occupational therapists) working on children with ASD. A final interview guide was prepared (e.g., genital play, peripheral vision, toe walking, food pocketing, fascination with shiny objects, holding objects with heavy pressure), which was then used to conduct an IDI. The interview was kept open as well as close-ended, and if some new theme emerged during the interview, it required more in-depth exploration. Open questions for IDI started with likes and dislikes of the child, odd behaviors noted, behaviors different from other children, the child’s reaction in different situations, and related to activities of daily living. Closed questions were related to sensory reactivities in different sensory systems like visual, auditory, gustatory, olfactory, tactile, vestibular, and proprioceptive sensations and related to the emotional domain. Finally, closing questions were asked of parents to get any information left out.
Proposed Conceptual Framework/Model for Exploration of Sensory Reactivity in Children with ASD.
Procedure
The Institutional Ethics Committee, AIIMS, Patna, India, provided ethics approval (Ref. AIIMS/ Pat/ IEC/PGTh/July 21/38). The socio-demographic details of the children were recorded with semi-structured proforma. The interview was conducted at our child guidance clinic, which consisted of one psychiatrist, a clinical psychologist, and a postgraduate trainee (note taker). This process was followed by transcription of the interview, followed by translation from Hindi to English, after which themes were identified and extracted accordingly. The interview was video and audio recorded after obtaining consent from the participants. Each interview was conducted in the language (Hindi) in which the parents were comfortable. Data were collected until saturation was achieved. The coding was done manually.
Data Analysis
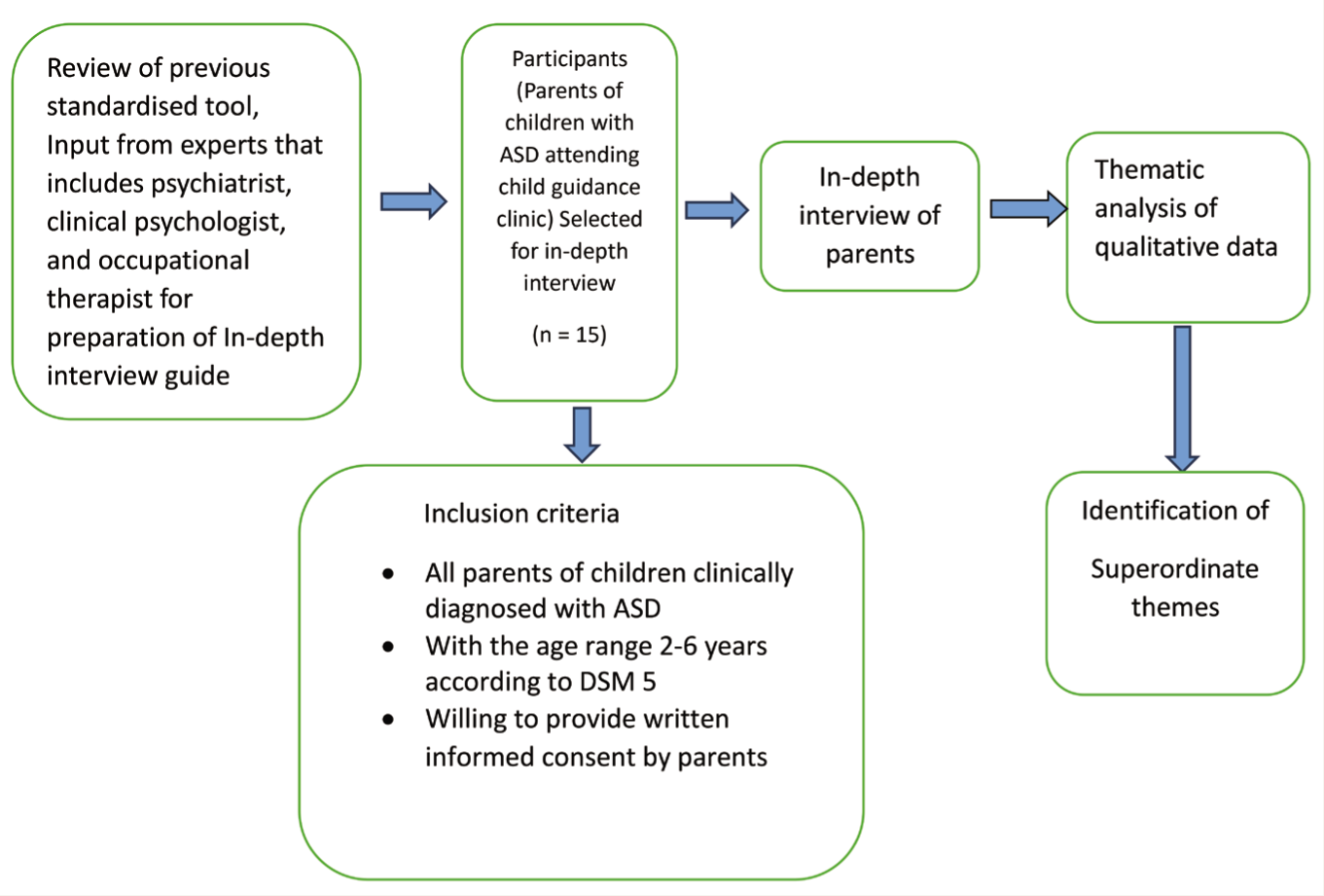
Thematic analysis was used to analyse the data (Figure 2). We followed the guidelines for translation about qualitative research. The recorded audio-video interview was transcribed after listening to it again and again. The interview transcript was then translated from Hindi to English, and all researchers checked it. 19 The transcribed data for each interview was read and re-read to ensure consistency with the raw data. During this process of familiarization, the newly developed codes were highlighted by all researchers (psychiatrists, clinical psychologists, and postgraduate trainees). The codes emerging were compared with each other, and themes were identified. We used linear steps to identify the subthemes and, finally, superordinate themes, which we had done open, axial, and selective coding, which is described below. 20 The categories were noted on the left side, and common themes that came out were noted on the right side. This was done many times to make sure to include all themes. It was cross-checked again by another researcher (psychiatrist). Then, similarities between categories were looked for, and emerging themes were noted (focused and deductive coding). The themes were analysed along with the supporting data (quotes) to fit together in a meaningful way. We considered all the data obtained and analysed it without any biases. We had ordered the questions in our interview guide in such a way that general questions were asked before moving on to specific questions. We recorded our interview session, which helped us to capture the emotional tone, pauses, and non-verbal cues of parents with ASD. Analytical rigor was ensured via internal review by all researchers.
Flow Chart Showing Thematic Approach of Qualitative Data Analysis.
The analysis of the data was done using the methods of phenomenological psychology, 21 which were used to interpret the important meanings of the lived experiences of parents of children with autism. Our study followed five steps of phenomenological research. We reviewed the recorded transcription several times to get a sense of the whole construct of sensory reactivity as a first step. Overall, we tried to reduce a particular region of meaning to suit our frame of reference for sensory reactivity. We went through the recorded material, and we segregated the transcript into smaller meaningful parts to allow for closer and more detailed focused themes for the next step. We extended the analysis of the initial meaning unit (everyday parental experiences) into several levels of elaboration, with individual variation among researchers. Finally, these phenomenologically elaborated parts of variant structures formed the basis of the sensory reactivity construct.
Results
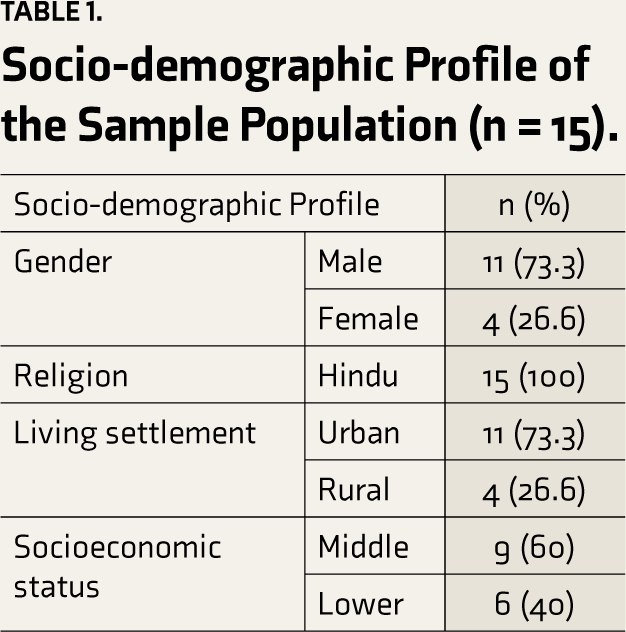
Fifteen parents of children with ASD were interviewed in our study. The majority of them were males (73.3%). Most of them were from urban backgrounds (73.3%) and belonged to middle socioeconomic status (73.3%). All were Hindus. The socio-demographic profile of the sample population is represented in Table 1. Table 2 shows a thematic analysis with various themes and subthemes. Table S1 describes an exploratory phenomenological analysis showing the superordinate themes, subthemes, and quotes of parents of children with ASD.
Socio-demographic Profile of the Sample Population (n = 15).
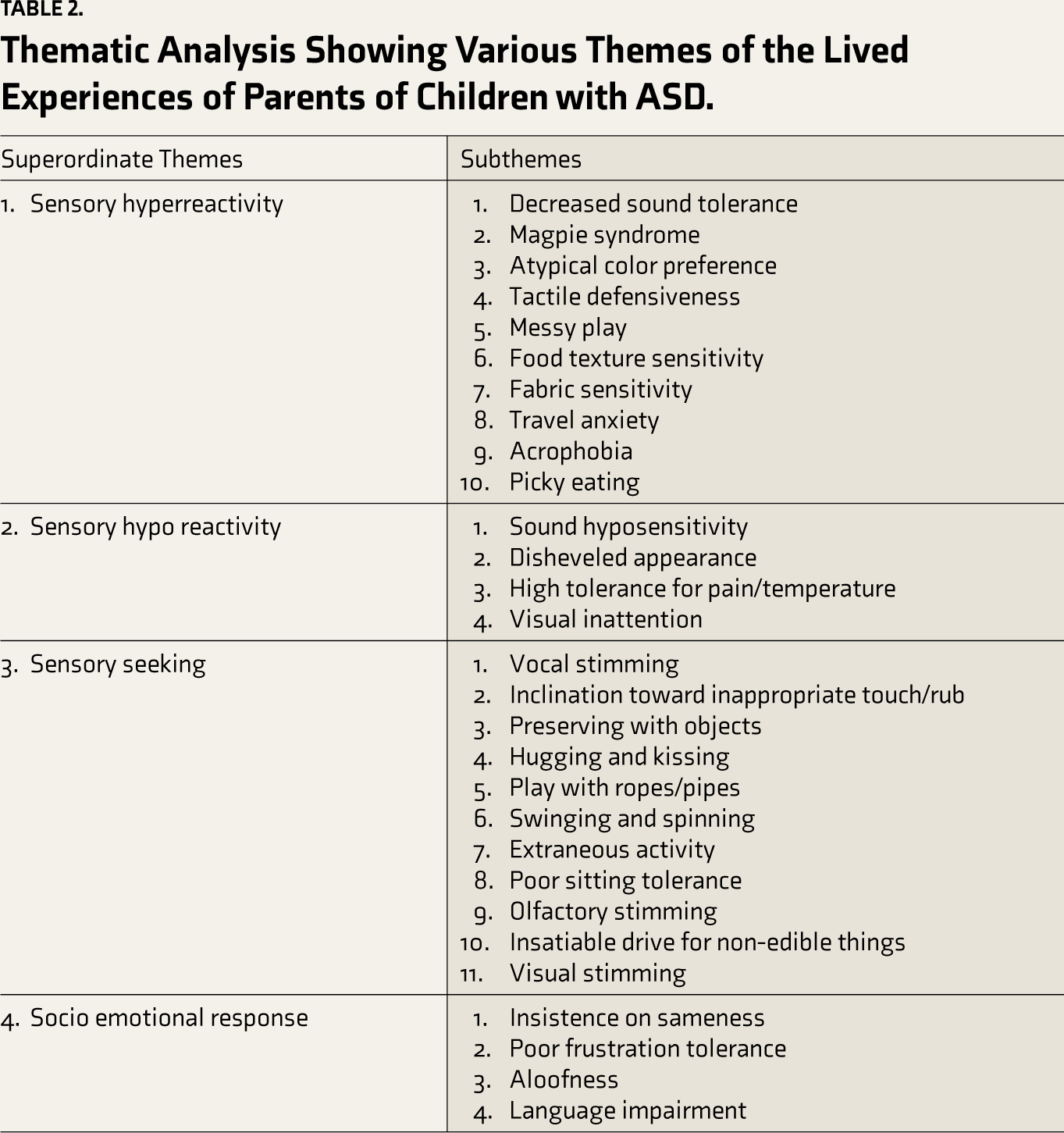
Thematic Analysis Showing Various Themes of the Lived Experiences of Parents of Children with ASD.
Superordinate Theme 1: Sensory Hyper-reactivity
This superordinate theme had 10 subthemes. The first subtheme was decreased sound tolerance, where the child could not tolerate even normal sounds in his surroundings and was afraid of it. The second subtheme was magpie syndrome, where the child gets attracted to and likes shiny things. The third subtheme was an atypical color preference, where the child likes and insists on a particular color. The fourth subtheme was tactile defensiveness, where the child reacts excessively to touch and is irritated by that. The fifth subtheme was messy play, where the child liked to play with sticky, messy objects. The sixth subtheme was food texture sensitivity, where the child feels the texture to decide whether to eat or not. The seventh subtheme was fabric sensitivity, where the child likes and dislikes particular textured clothes. The eighth subtheme was travel anxiety, where the child is scared of traveling by bike. The ninth subtheme was acrophobia, where the child is afraid of being at heights. The tenth subtheme was picky eating, where the child likes and dislikes particular food types.
Superordinate Theme 2: Sensory Hypo-reactivity
This superordinate theme had four subthemes. The first subtheme was sound hyposensitivity, where the child does not respond to normal sounds, like a poor response to name-calling. The second subtheme was the disheveled appearance, where the child is not responding to dirt and roaming untidily. The third subtheme was high tolerance to pain and temperature, where the child responds less to pain and temperature sensations. The fourth subtheme was visual inattention, where the child is not making eye contact and paying poor attention to things moving around him.
Superordinate Theme 3: Sensory Seeking
This superordinate theme had 11 subthemes. The first subtheme was vocal stimming, where the child would make sounds and enjoy hearing them. The second subtheme was an inclination toward inappropriate touch/rub, where the child keeps touching and rubbing things. The third subtheme was perseverating with objects, where the child always wanted to hold something in his hand. The fourth subtheme was hugging and kissing, where the child likes hugging and kissing people tightly. The fifth subtheme was playing with ropes/pipes, where the child likes the texture of ropes and pipes and prefers play with those rather than toys. The sixth subtheme was swinging and spinning, where the child preferred swinging games and kept spinning on his own and around people. The seventh subtheme was extraneous activity, where the child kept jumping and engaging in self-injurious behavior like head banging. The eighth subtheme was poor sitting tolerance, where the child found difficulty in sitting in a place and kept moving here and there. The ninth subtheme was olfactory stimming, where the child likes to smell things. The tenth subtheme was an insatiable drive for non-edible things, where the child-like is keeping non-edible things in the mouth. The eleventh subtheme was visual stimming, where the child keeps staring at a particular place or thing.
Superordinate Theme 4: Socio-emotional Response
This superordinate theme had four subthemes. The first subtheme was the insistence on sameness, where the child faces difficulty and gets irritated if there is a slight deviation in his routine. They prefer to follow the same routine. The second subtheme was poor frustration tolerance, where the child gets easily irritable when something is not going according to his wishes. The third subtheme was an aloofness, where the child remains alone on his own and shows very poor interaction with the external world. The fourth subtheme was language impairment, where the child has poor language development.
Discussion
The study of sensory and motor issues in autism is a relatively new frontier for research in ASD. It is, therefore, imperative to understand the sensory issues faced by children with ASD that are relevant to the Indian context. The main objective of the study was to explore, describe, and characterize the sensory reactivity in children with ASD as per the lived experience of parents of children with ASD. This study helped in coherently understanding the underlying sensory processing deficits explaining various symptom presentations in children with autism by categorizing them into superordinate and subthemes.
In the DSM-5 criteria, sensory processing deficits have been newly included in the criteria for ASD, as it is more prevalent among children with autism. Previous literature has called for more in-depth cultural research on sensory reactivity issues in children with autism for a better understanding of the phenomenology of sensory processing issues in children with ASD. We decided to conduct a study to obtain local descriptions for symptoms of sensory processing issues by interviewing the parents of children with ASD attending our child guidance clinic. Our study adopted a robust methodology to understand the phenomenology of sensory issues. Our study utilized a comprehensive conceptual framework to understand the themes of sensory reactivity in children with ASD. Many studies have raised the question of whether sensory processing deficit forms a core feature or an associated feature of autism. From our study, it has been understood that sensory processing deficit could be considered a core feature of autism in the future as it contributes to all symptom presentation of autism, affects the social and communication skills of children with ASD, and makes their lives more challenging.
Easily Affected with Sensory Input (Sensory Hyper-reactivity)
Excessive sensitivity and reactivity to normal stimuli from the surroundings make the child attracted to particular things or get excessively irritable toward particular things, which makes them feel uncomfortable about their surroundings and makes it difficult for them to adapt to their surroundings. In our study, the parents described that their children are attracted to light and shining objects and keep staring at them. It was difficult for family members to distract them from that and to make him focus on some other activities. They like particular types of textured cloth and eat food only if they like the texture and smell of the food. They like to play with messy things like paint, glue, soil, and water and enjoy playing with them. In our interviews, irritability toward a particular stimulus by the child was explained in different ways by the parents. The children are not able to tolerate normal sounds, which makes them plug their ears, run to a calm place, and get irritable. Parents found it more difficult to make their child’s hair and nails cut as the patient would not be able to tolerate the touch, and they would start crying and screaming until it got done. They get easily irritated by simple touches and hugging them, and they try to remove people’s hands immediately if they touch them. This behavior does not allow them to be in cordial relationships with other people. They get easily irritated by tags on new clothes and try removing them as soon as possible. They are not able to tolerate the clothes becoming dirty and want to change clothes immediately. As they get attracted to one particular thing, they miss the opportunity to explore several other things, which would affect their further social and intellectual development. As they get irritable toward a particular stimulus, they face difficulty in managing their day-to-day activities, and parents find difficulty managing their behaviors.
The themes of “auditory filtering” in study 22 and “auditory filtering-hypersensitivity” in another study 23 are supported by our theme of “decreased sound tolerance.” The themes of “more tactile sensitivity” in study 22 and “hyperresponsiveness to tactile stimuli” in another study 24 are supported by our theme of “tactile defensiveness” in our study. The theme of “more taste sensitivity” in study 22 is supported by our theme of “picky eating.” The domain of “sensory over- responsivity” proposed in Lucy Miller’s model 15 and the domain of “sensor” and “avoider” in Dunn’s model 25 is supported by our superordinate theme of “Sensory Hyper-reactivity.”
Dream Toddlers (Sensory Hypo-reactivity)
Low responsiveness to sensory stimuli from the surroundings makes the child remain unbothered or unconcerned about his surroundings and not respond to the extent expected, which could also explain his lack of communication skills and lack of emotional reciprocity. In our study, parents described their children’s lack of responsiveness as affecting their lives. They will not respond if their name calls them. They remain indifferent to the loud sounds of mixers, trains, etc. Some parents felt that it was due to hearing loss. They understood unresponsiveness when autism was diagnosed, and they also found that their children do not respond if someone touches or hugs them and do not show any warmth toward them while hugging, which is not letting the child feel the emotions of others and hence lacking emotional reciprocity. If they get hurt, either they do not feel the pain at all or feel pain at a very low intensity and fail to report this to their parents. They also noticed that their children do not bother if they get dirty or wet and remain on that cloth for a long time till it gets changed by their parents. As the children remain under-responsive to environmental stimuli, their perception and expression of their thoughts to others have been hampered, which could explain their impaired social skills.
The theme of “auditory filtering-hyposensitivity” in a study 23 is supported by our theme of “sound hyposensitivity.” The theme of “hyporesponsiveness to tactile stimuli” in a recent study 24 is supported by our theme of “high tolerance to touch/pain and temperature.” The domain of “sensory under-responsivity” proposed in Lucy Miller’s model 15 and the domain of “register (low registration)” in Dunn’s model 14 is supported by our superordinate theme of “sensory hypo-reactivity.”
Gratifying to Senses (Sensory Seeking)
The habit of a tendency to stimulate their own senses develops in some children who are hyporesponsive to their surrounding stimulus as they have the intense urge to self-stimulate their various sensory systems, which are not able to be stimulated naturally, which helps the children to keep their senses active. In our study, parents described how their children are trying to stimulate their senses in different ways. Their children prefer always holding something in their hands, hugging and kissing tightly, and touching and rubbing surfaces to stimulate their tactile senses and control their urges. They stimulate themselves by spinning around people, spinning around themselves, and prefer to play in swings in parks rather than other play games. Stimulate their auditory system by making sounds and listening to them. They stimulate their gustatory sense by keeping non-edible things in their mouths and licking and biting objects, which may lead to the destruction of objects. They like to go near objects and people who apply strong perfumes and oil over the forehead and smell it, which gives them pleasure. They would smell the food before eating, and he would keep jumping and banging his forehead to get pleasure. The domain of “sensory seeking” proposed in Lucy Miller’s model 15 and the domain of “seeker” in Dunn’s model 19 is supported by our superordinate theme of “sensory seeking.”
Socio-emotional Reciprocity (Socio-emotional Response)
Children are not able to successfully fulfill their expected social roles and face difficulty controlling their emotions due to the sensory issues they face. This was described in our study by the parents, as their child is less reactive to their surrounding stimulus; they remain aloof most of the time, and they are not as interactive as other children of his age. They noticed they were always playing alone and not making eye-to-eye contact with others, even if they would interact. As they do not interact much, most of the children in our study showed a delay in their language development, and children are using sign language or gestures if they need something, which was found to be the first symptom noticed by most of the parents, which made them consult a doctor. As their children show selective responsiveness (hyper or hyporeactivity) to a particular stimulus, they stick to one type of routine. They are not able to tolerate, adjust, or flex to the changes. They go into tantrums and start harming others and property if their routine gets slightly changed or disturbed, and it is difficult for their parents to handle such situations. They remain more sensitive emotionally as they are disturbed by their differential reactivity to surrounding stimuli, always in the background, and get irritated and annoyed easily if something is not going according to their wish. As the socio-emotional response of the children gets affected due to both hyper or hypo-reactivity to the stimulus or sometimes both, we have classified this as a separate superordinate theme. Socio-emotional responses are a separate domain of sensory processing deficit as a widely used sensory profile tool that supports this theme of ours.
Our study has a few limitations. We have included a few children who were also undergoing therapy; hence, during the interview, it was difficult for parents to recall those sensory issues that were present earlier before the commencement of the therapy. For a few children, we could not interview both parents due to logistical reasons, which could have affected the data enrichment. Also, we included children between the ages of 2–6 years. Children belonging to other age groups were left out, which might not completely reflect the sensory reactivity of children with ASD. We conducted our study in a single tertiary care referral hospital in east India, which might affect its applicability in other parts of India. The identified themes in our study were based on the pre-determined conceptual framework. It precluded us from exploring other themes. There might have been an opportunity to explore more dimensions and items if we had not based our study on a pre-determined framework.
To conclude, our study results captured various possible clinical presentations of sensory processing issues in children with ASD through parental experiences. Insights from parents helped us explore and identify various dimensions of the sensory reactivity construct of ASD children. Key findings from our study will help in framing an interview guide for identifying sensory issues of children with ASD. Our study findings will help further develop a valid and reliable tool for sensory reactivity in children with ASD. After identification, further, it would help therapists to work on it, which would facilitate in improving sensory issues for better social adaptability of the child with ASD. The items generated may help in discovering new therapeutic techniques in occupational therapy to mitigate the repetitive undesired behavior arising from sensory issues.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the use of Generative AI
No AI tools were implemented to collect or analyse the data or to produce images or graphs and write the manuscript.
Ethical Approval
An ethical approval was taken from Institute Ethics Committee Approval Number AIIMS/ Pat/ IEC/PGTh/ July21/38.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was taken from parents for use of information for reporting this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.