
Abstract
Background:
Alcohol use disorder (AUD) causes significant morbidity and mortality. Prescription of AUD pharmacotherapies remains low. Attitudes toward AUD pharmacotherapies influence their prescription rates. We conducted an online survey to assess how attitudes modulate the association between knowledge and prescription rates for four commonly used AUD medications among Indian clinicians.
Methods:
An online survey was sent nationwide to Indian physicians between February and April 2023 to assess knowledge, attitudes, and practices of various AUD medications. An a priori model was defined to indicate the relationship between study variables. Bootstrapped correlation analysis was conducted to determine confidence intervals of the correlation coefficients between knowledge, attitudes, and prescription practices. Additional subgroup analysis was conducted for faculty and private psychiatrists to assess if they prescribed differently.
Results:
A total of 387 physicians responded to the survey. Bootstrapped correlation analysis indicated that safety and acceptability played a moderated prescription rates for acamprosate and naltrexone while they mediating role among faculty. For Disulfiram, perceived efficacy had a mediating effect, especially among private psychiatrists. Among faculty, perceived safety negatively mediated Disulfiram prescriptions. There was no indirect effect of attitudes on the association between knowledge and prescription practices for Baclofen.
Conclusion:
The role of attitudes varied across medications. For acamprosate and naltrexone, perceived safety and acceptability significantly moderated prescription rates. For Disulfiram, perceived efficacy played a significant mediating effect. Attitudes did not influence Baclofen prescriptions as a whole, but acceptability significantly mediated prescriptions for private psychiatrists. This might indicate that physicians prescribe Baclofen as an ineluctable option.
Perceived attitudes significantly influence the association between knowledge and prescription rates for AUD pharmacotherapies. For acamprosate and naltrexone, safety and efficacy positively moderate prescription rates, while perceived efficacy mediates prescription rates for Disulfiram. However, there was no significant effect of any perceived attitudes on prescription rates for Baclofen.Key Message:
Alcohol use disorder (AUD) imposes a heavy health and economic burden. AUD was responsible for an estimated 5.3% of all deaths and 5.1% of all DALYs lost globally in 2016. 1 In India, the prevalence of AUD is estimated to be 29 million dependent users, resulting in a loss of 258 million life years between 2011 and 2050.2,3 Several pharmacological interventions are effective for AUD, but their prescribing rates have remained low.4,5 The poor uptake of AUD pharmacotherapies is present even in specialized addiction treatment programs. 6
The reasons for poor uptake of AUD pharmacotherapies have included structural barriers (licensing and personnel requirements, physician access, cost of treatment), provider-based barriers (e.g., lack of knowledge or confidence, reluctance to prescribe pharmacotherapy), and patient characteristics (e.g., no interest in pharmacotherapy, poor access to care, fear of side-effects or stigmatization). 7 Clinician-based barriers (knowledge gaps and unfavorable views toward the effectiveness of AUD medications) are also reasons for the low use of AUD pharmacotherapy.8,9 Addressing these barriers may help reduce the large treatment gap for AUD that prevails in the country and the world.2,10
The theory of planned behavior (TPB) has often been used to explain prescribing behaviors. In this framework, behavioral intention (i.e., physician’s decision to prescribe a drug) is predicted by attitude toward medications, subjective norms, and perceived behavioral control over prescribing. 11 Attitudes that impact prescriptions include familiarity, beliefs about efficacy, and beliefs about safety. Other factors influencing prescriptions include subjective norms (e.g., perceptions of the need for AUD pharmacotherapy) and the desire to conform (with colleagues’ prescribing behaviors). 12 Studies that have used TPB as a framework to explain physician prescription patterns for AUD pharmacotherapies concluded that physician prescriptions are impacted significantly by attitudes, which serve as a modulator of the relationship between knowledge and prescription rates.8,13
Cross-national differences in attitudes and pharmacotherapy use are common. A case in point is Disulfiram. 14 Relegated as a second-line drug in Western nations, it is particularly efficacious in the Indian context.15,16 The prescription of anticraving medications also significantly varies within India. 17 To the best of our knowledge, there is a lack of Indian studies on how attitudes drive prescription rates for AUD pharmacotherapies. This report is a continuation of a previous article in which we explored how clinician and caseload variables impact physician attitudes and diffusion of AUD pharmacotherapy. In this article, we explored how three attitudes (perceived efficacy, safety, and acceptability) impact the relationship between knowledge and prescription rates among Indian physicians. 18 We hypothesized that despite an adequate understanding of the medical model of substance use and the need for pharmacotherapy, the choice of pharmacotherapy is significantly driven by physician attitudes toward each medication. To enhance the quality of AUD treatment, barriers to AUD pharmacotherapy (specifically in the Indian context) need to be elucidated. Our study hoped to address these knowledge gaps.
Materials and Methods
A cross-sectional, observational study was designed with approval from the Institute’s Research Review Board and Ethics Committee. Data collection was conducted between January to March 2023. An online questionnaire-based survey was conducted among MBBS-qualified physicians, including psychiatrists with adequate experience in treating AUDs (self-reporting to having attended to at least 30 patients with AUD in the past 2 years) and working in government, semi-government, and private sectors. This nationally representative physicians’ sample across the country was contacted via email with the assistance of the Addiction Psychiatry Society of India (APSI). Participation in the survey was voluntary, and consent was obtained prior to participation. In case someone did not respond at the first instance, weekly reminders were sent for the next 2 weeks. Confidentiality of the information was maintained. No financial compensation was given for participation. After informed consent, participants meeting the inclusion criteria responded to a study-specific knowledge, attitudes, and practices questionnaire (KAP) developed based on existing literature. The completion of the survey required approximately 5–10 minutes. Since there is no centrally available database of practicing psychiatrists in India, we used the membership size of the Indian Psychiatric Society (IPS) as the best estimate of the number of psychiatrists in India. Using a confidence level of 95% with a margin of 5%, a sample size of 367 was determined to be adequate. Although we determined the sample size using the membership of the IPS, we used the assistance of the APSI as their members would be more representative of psychiatrists who are more likely to attend to persons suffering from AUD. Most members of the APSI are also members of the IPS (internal communication). The sample size after adding the entire membership of the IPS and the APSI using the same parameters was determined to be 370.
The demographic variables included were gender, age, education, designation, current practice environment, years of experience in treating AUD, locality of practice, estimated annual caseload, and knowledge regarding AUD pharmacotherapy. The knowledge questionnaire was formulated based on the literature review, where the responses may depend on the value of their agreement on several treatment approaches on a 7-point Likert scale. A composite score is determined by participants’ responses to two items from the questionnaire reflecting participants’ overall valuation and knowledge of pharmacotherapy. 19 The composite score reflects participants’ overall valuation of adjunctive pharmacotherapy and avoids any biases for a particular pharmacotherapeutic mechanism. Other variables assessed were attitudes (perceived acceptability, safety, and efficacy) and practices toward AUD pharmacotherapy. The respondents were asked to rate their perceived effectiveness, acceptability, or safety for each medication included in the study, namely Acamprosate, Disulfiram, Naltrexone, and Baclofen, on a 10-point Likert scale. The physicians were also given an option of responding “do not know” if they felt they could not assess for an attitude toward a medication. Participants were asked to rate the approximate percentage of their prescriptions for AUD for each of the above medications. The percentages were to be selected from one of seven ranges (with a total range covering 0% to 100%). An additional item allowed the participant to indicate that they had never been prescribed the medication. The percentage range was then converted into a rank variable with a higher rank indicating a greater percentage of prescriptions.
Statistical Analysis
All data were tabulated and analyzed using SPSS 25.0 statistical software (IBM Inc.). The continuous variables were presented as means and standard deviations and analyzed using independent samples t-tests. The categorical variables were presented as percentages and analyzed with chi-square tests. Univariate associations between measures were assessed using Spearman correlations.
Mediational Analysis
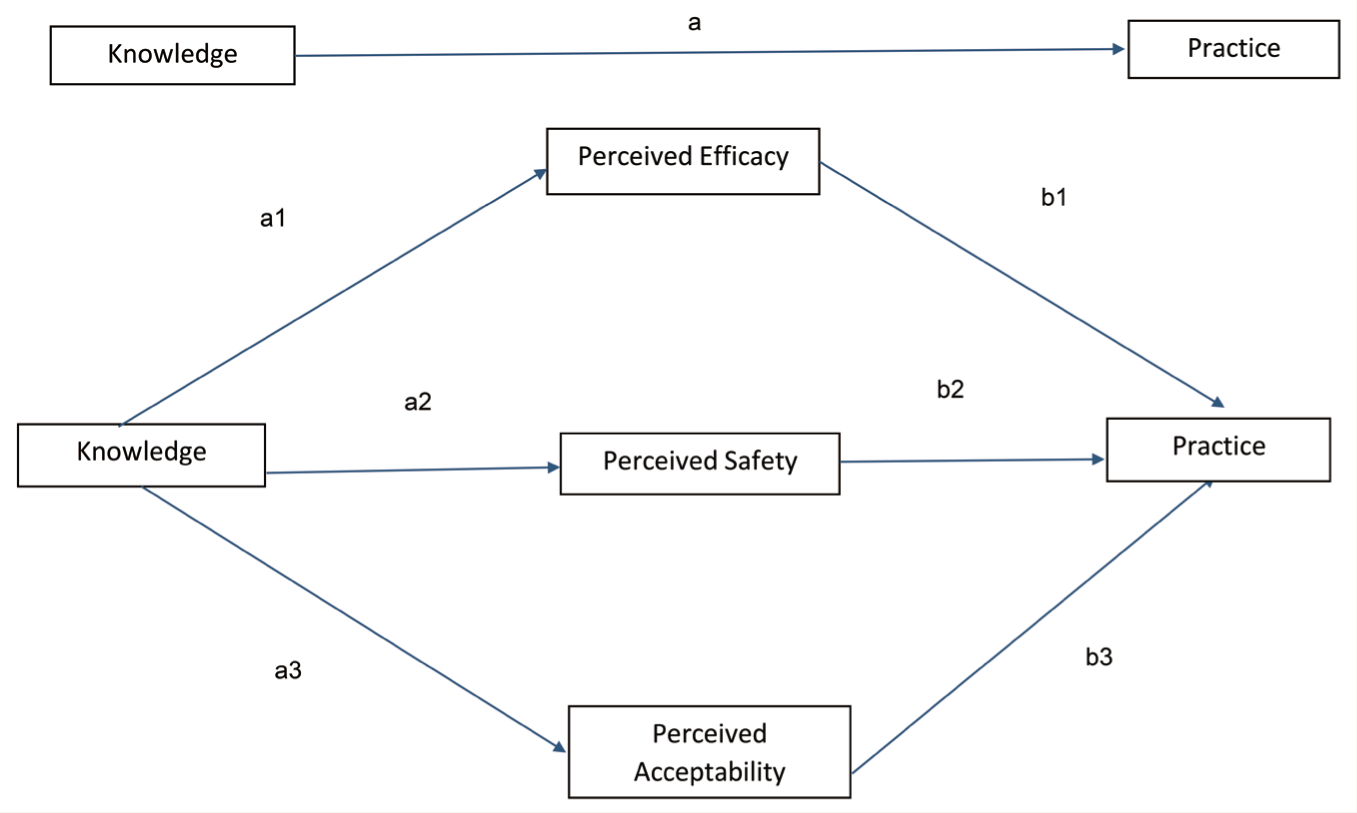
Mediational analysis is a statistical method that identifies the role of an intermediary variable (also known as the mediator variable or intervening variable) in determining the relationship between an independent variable (IV) and a dependent variable (DV). In our study, knowledge is the IV, practice is the DV, and attitudes (perceived efficacy, safety, and acceptability) are the intermediary variables. To determine the impact of attitudes, a mediation model was hypothesized a priori, postulating the relationships between these variables (Figure 1).
Path Letters and the Proposed Relationship Between Knowledge, Attitudes, and Practices in our a Priori Model.
Bootstrapped correlation analysis allowed us to test for the mediation or moderation effect of the attitudes in the association between the knowledge and practices. This analytic strategy has been used before and allowed us to overcome the limitations of using regression for ordinal variables. 20
Path a describes the total association between knowledge and practice. Paths a1, a2, and a3 described the association between knowledge and perceived efficacy, safety, and acceptability, respectively, while paths b1, b2, and b3 described the association between practice and perceived efficacy, safety, and acceptability, respectively. If the association between knowledge and practice is not significant, but if any of the indirect paths, including an attitude (path a1* b1 or path a2*b2 or path a3*b3), is significant, it indicates that there is a significant mediating effect of that attitude between knowledge and practice. Suppose both the direct association between knowledge and practice (path a) is significant and any of the indirect paths are significant. In that case, it indicates a moderating role of that attitude between knowledge and practice.
Bootstrapping
A bias-corrected (BC) bootstrapped correlation analysis (with n = 1000 bootstrap samples) was done to determine the confidence intervals of the correlation coefficient. Bootstrapping is a nonparametric procedure that is used to test mediation effects and provides a way of circumventing power deficiencies of normal theory tests typically introduced by the non-normality in the sampling. The procedure involves treating the sample as a population and replacing a new sample of size n (where n = original sample size) from the available data, sampling with the replacement, and computing the indirect effect (i.e., path a × b) for each sample. This process is repeated over a total of k times, and the distribution of the k values of a × b serves as an empirical, nonparametric approximation of the sampling distribution of ab. The mean of the k estimates of ab is used as a point estimate of the indirect (i.e., mediation) effect, and the standard deviation functions as the standard error of the sampling distribution of ab.21,22 Once completed, the bootstrapped sampling distribution is used to generate CIs around point estimates in the mediation model. Bootstrapping was conducted to correlate knowledge, attitudes, and practices among all respondents (Table 1), faculty (Table 2), and independent private psychiatrists (Table 3).
Bootstrapped Correlation Analysis of Knowledge, Attitudes, and Practices for AUD Pharmacotherapies for all Respondents.
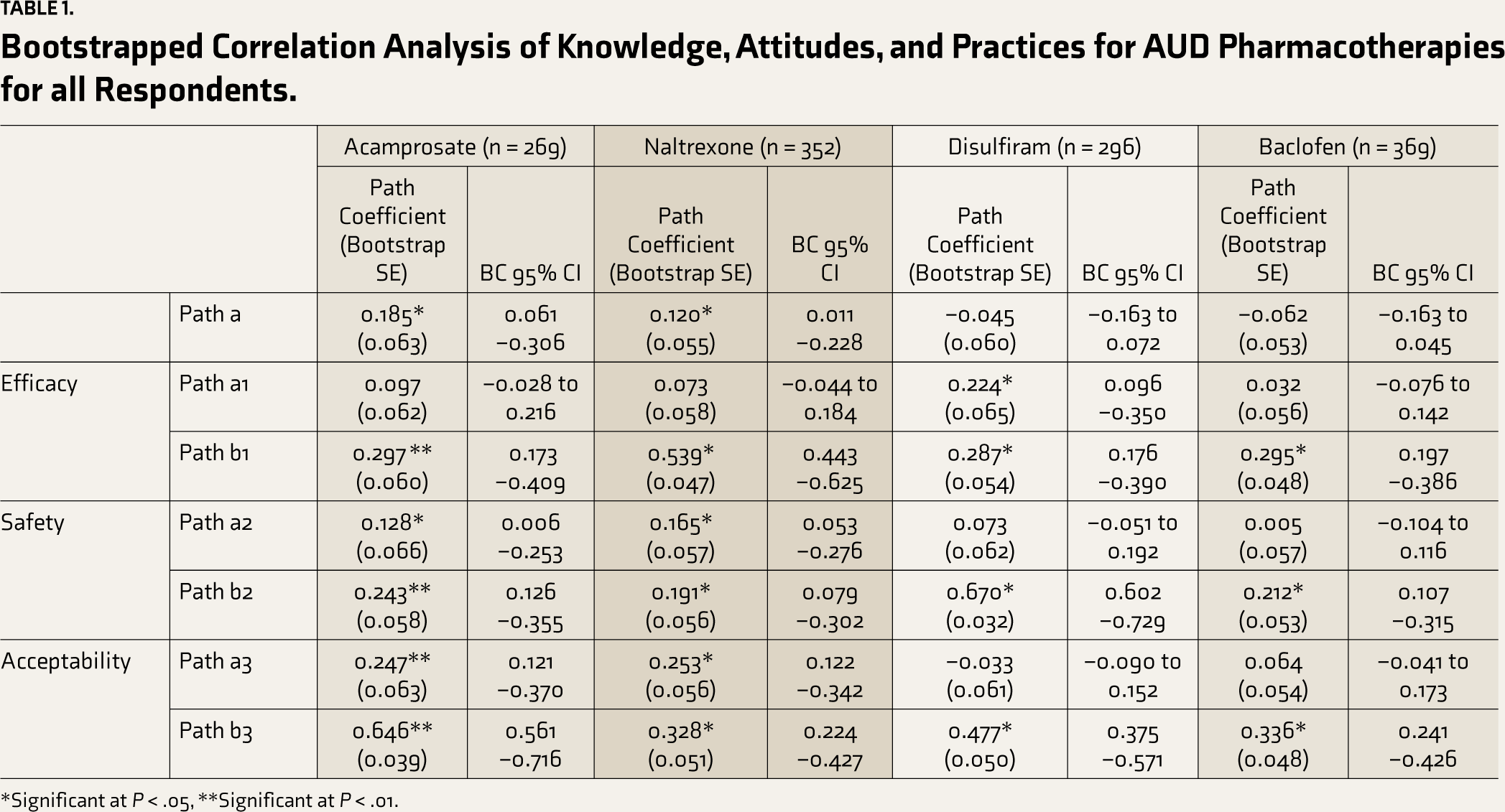
*Significant at P < .05, **Significant at P < .01.
Bootstrapped Correlation Analysis of Knowledge, Attitudes, and Practices for AUD Pharmacotherapies for Faculty.
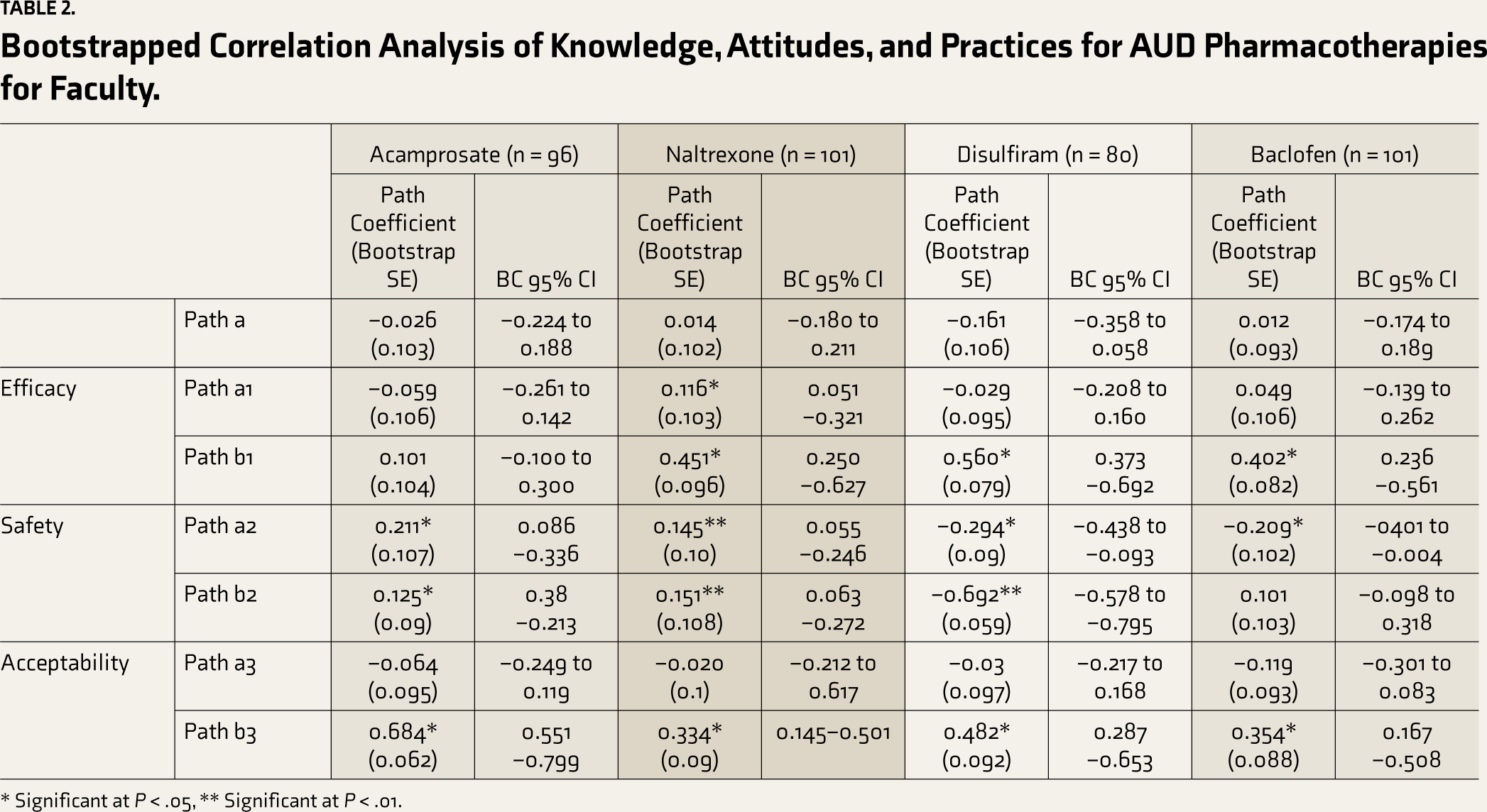
* Significant at P < .05, ** Significant at P < .01.
Bootstrapped Correlation Analysis of Knowledge, Attitudes, and Practices for AUD Pharmacotherapies for Independent Private Psychiatrists.
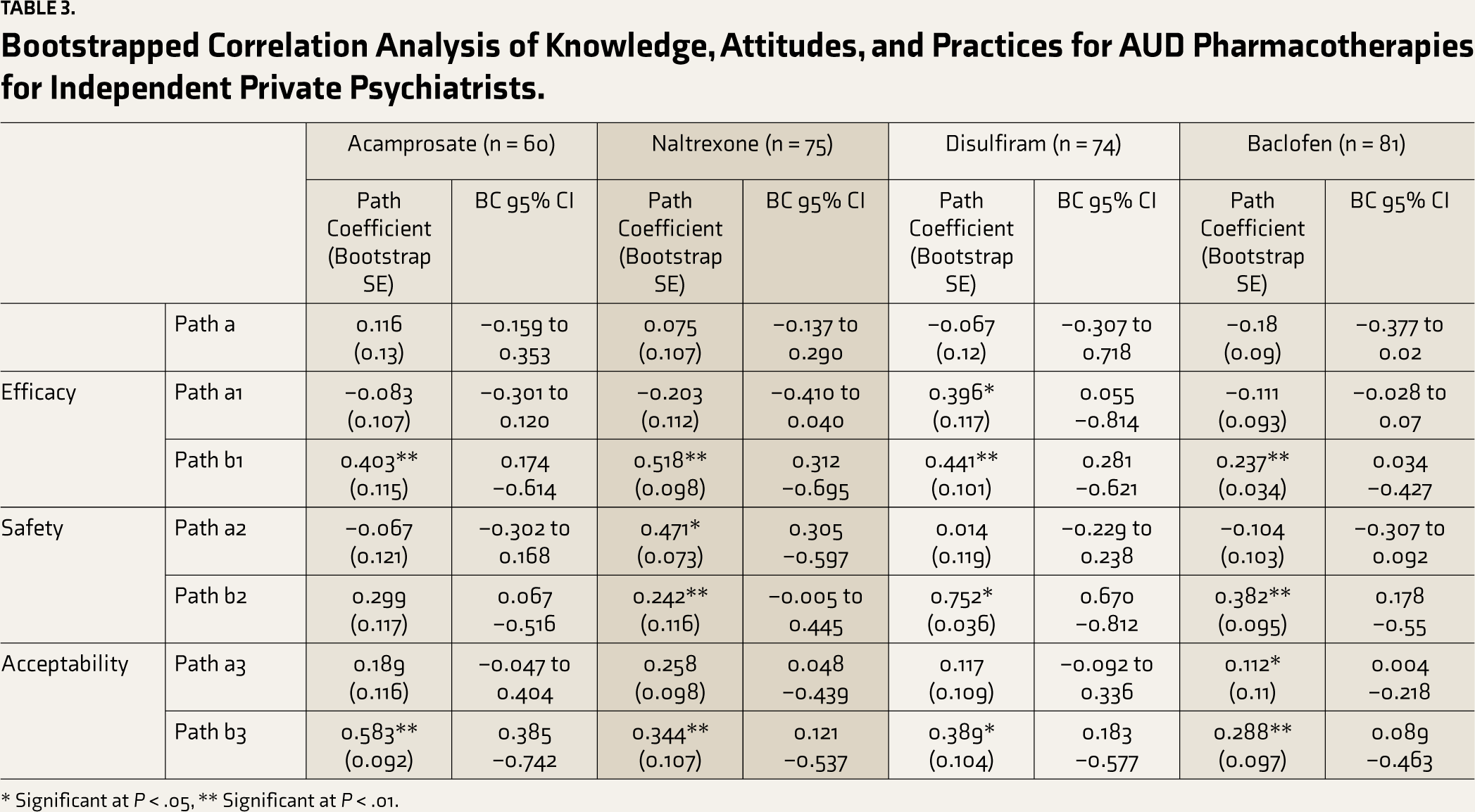
* Significant at P < .05, ** Significant at P < .01.
Results
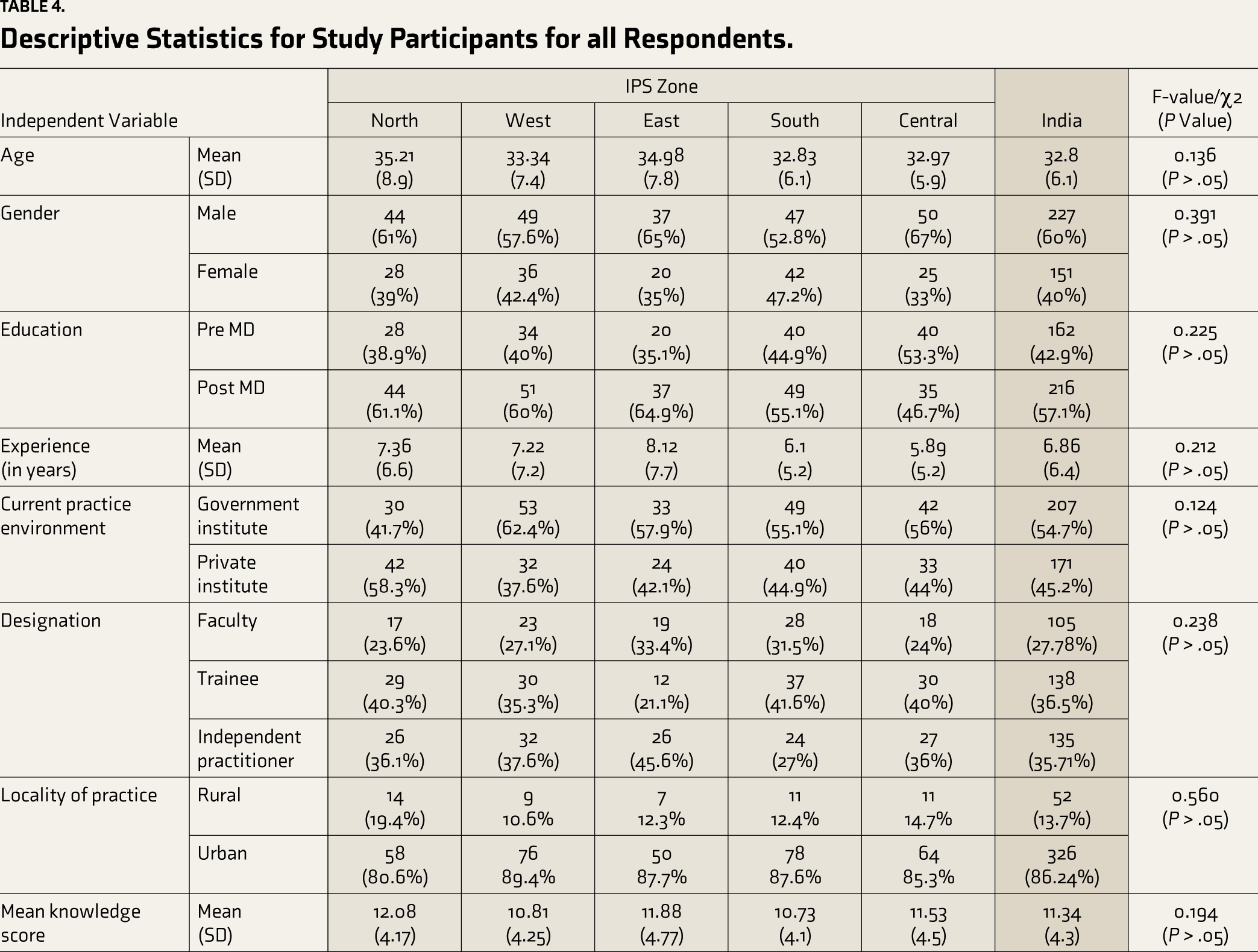
A total of 387 physicians responded to the survey. The response rate was 15%. Twelve responses were removed because their responses were incomplete or duplicated. Descriptive statistics for study participants are presented in Table 4 separately for the various zones of the Indian Psychiatric Society. Analyses revealed no significant differences in age, gender, education, experience, current practice environment, designation, locality of practice, and mean knowledge score between the respondents from the various zones. Across all zones, participants had a higher knowledge score compared to previous studies (reflecting a higher valuation of the role of pharmacotherapy).23,24
Descriptive Statistics for Study Participants for all Respondents.
Role of Attitudes Between Knowledge and Practice for Acamprosate
As shown in Table 1, the bootstrapped correlation analysis revealed that there was a significant correlation between Knowledge and Practice for Acamprosate (path a: r = 0.185, P < .05), indicating a direct relationship between them. There was a significant correlation between knowledge and perceived safety (path a2: r = 0.128, P < .05) as well as between knowledge and perceived acceptability (path a3: r = 0.247, P < .01). Similarly, there was a significant correlation between practice and all three attitudes (path b1: r = 0.297, P < .01; path b2: r = 0.243, P < .01 and path b3: r = 0.646, P < .01). The combination of the paths reveals that perceived safety and perceived acceptability played a moderating role in the association between knowledge and practice. Among faculty, there was a significant correlation between knowledge and perceived safety (path a2: r = 0.211, P < .05) and between perceived safety and practice (path b2: r = 0.125, P < .05). Therefore, perceived safety was a significant mediator between knowledge and prescription rates. Among private psychiatrists, although there was a significant correlation between perceived efficacy and practices (path b1: r = 0.403, P < .01) and between perceived acceptability and practices (path b3: r = 0.583, P < .01), the correlation between knowledge and these attitudes was not significant. Therefore, any mediational role of these attitudes could not be ascertained.
Role of Attitudes Between Knowledge and Practice for Naltrexone
The bootstrapped correlation analysis revealed a significant correlation between Knowledge and Practice for Naltrexone (r = 0.120, P < .05), indicating a direct relationship between them. Correlation analysis between knowledge and attitudes revealed a significant correlation between perceived safety and perceived acceptability (path a2: r = 0.165, P < .05 and path a3: r = 0.253, P < .05). Similarly, the correlation between practice and attitudes revealed that the correlation was significant for all three attitudes (path b1: r = 0.539, P < .05; path b2: r = 0.191, P < .05 and path b3: r = 0.328, P < .05). Taken together, it implies that, like Acamprosate, perceived safety and perceived acceptability played a moderating role (and an indirect effect) in the association between knowledge and practices for naltrexone. Among faculty, there was a significant correlation between knowledge and perceived efficacy (path a1: r = 0.116, P < .05) and between perceived efficacy and practice (path b1: r = 0.451, P < .01). Therefore, perceived efficacy was a significant mediator between knowledge and prescription rates for faculty. Similarly, perceived safety was also a significant mediator between knowledge and prescription rates. Correlations between knowledge and perceived safety (path a2: r = 0.145, P < .01) and between perceived safety and practices (path b2: r = 0.151, P < .01) were also significant. Among private psychiatrists, perceived safety was found to have a mediating effect (path a2: r = 0.471, P < .05 and path b2: r = 0.242, P < .01).
Role of Attitudes Between Knowledge and Practice for Disulfiram
There was no significant correlation between Knowledge and Practice for Disulfiram (path a: r = –0.045, p>0.05). The correlation analysis between knowledge and attitudes revealed that the correlation was significant for perceived efficacy (path a1: r = 0.224, P < .05). Similarly, the correlation was significant between practice and all three attitudes (path b1: r = 0.287, P < .05; path b2: r = 0.670, P < .05 and path b3: r = 0.477, P < .05). Therefore, perceived efficacy played a mediating effect in the association between knowledge and practices. Those who perceive Disulfiram as more efficacious are more likely to prescribe Disulfiram. Among faculty, there was a significant negative correlation between knowledge and perceived safety (path a2: r = –0.294, P < .05) and a similar negative correlation between perceived safety and practices (path b2: r = –0.692, P < .1). This seemed to suggest that perceived safety seemed to play a significant negative mediating effect for Disulfiram prescriptions among faculty. Among independent psychiatrists, there was a significant correlation between knowledge and perceived efficacy (path a1: r = 0.396, P < .05) and between perceived efficacy and practices (path b2: r = 0.441, P < .01). This is indicative of the fact that perceived efficacy seemed to have a positive impact on private psychiatrists’ prescriptions of Disulfiram.
Role of Attitudes between Knowledge and Practice for Baclofen
The bootstrapped correlation analysis lacked a significant correlation between Knowledge and Practice for Baclofen (path a: r = –0.062, P > .05), suggesting no direct relationship, as shown in Table 1. The correlation analysis between knowledge and attitudes revealed no significant relationship either for perceived efficacy, safety, or acceptability. Similarly, the correlation between practice and attitudes revealed that the correlation was significant for all three attitudes (path b1: r = 0.295, P < .05; path b2: r = 0.212, P < .05 and path b3: r = 0.336, P < .05). However, taken together, the results indicate that none of the attitudes had an indirect effect (mediation or moderation) on the association between knowledge and practices. Among private psychiatrists, there was a significant correlation between knowledge and perceived acceptability (path a3: r = 0.112, P < .05) and between perceived acceptability and practice (path b3: r = 0.288, P < .01). This suggests that perceived acceptability was a significant attitudinal factor driving Balcofen prescriptions among private psychiatrists.
Discussion
This investigation focused on the role of physicians’ perception of AUD pharmacotherapy in modulating the relationship between their overall valuation of pharmacotherapy and actual prescription rates for four commonly prescribed medications. A previous analysis indicated that the four pharmacotherapies selected in this study had the highest diffusion rates among Indian physicians. 25 The survey was conducted among approximately 400 physicians providing treatment services for AUD across the country. These physicians represent the vanguard of medically supervised AUD treatment in the country. Therefore, assessing factors determining prescription rates of AUD medications will help develop approaches to enhance the use of these medications. As shown in our previous publication, the diffusion of these AUD medications is varied and is determined by factors extending beyond evidence of their efficacy.
Results demonstrated that the role of attitudes in determining prescription rates varies with medication. For acamprosate and naltrexone, a higher valuation of pharmacotherapy (knowledge) correlated (albeit weakly) with greater prescription rates. Perceived safety and efficacy played a moderating role in determining these prescription rates, with physicians who perceived these medications as safe and efficacious prescribing these medications more often, especially among faculty, perceived safety and efficacy significantly mediated prescriptions for naltrexone, while only perceived safety significantly mediated prescriptions for naltrexone. For Disulfiram, physicians’ valuation of pharmacotherapy did not correlate significantly with prescription rates. Instead, perceived efficacy played a significant mediating effect. This implies that physicians who perceived Disulfiram as particularly effective were the ones who prescribed it more often. However, additional analysis among faculty and independent practitioners seemed to suggest that these groups seemed to behave differently when prescribing Disulfiram. Among faculty, perceived safety played a major negative mediating role in determining Disulfiram prescriptions among private psychiatrists, and perceived efficacy played a significant positive mediating effect. For Baclofen, there was no significant correlation between knowledge and prescription rates. Neither did any of the perceived attitudes play a mediating factor between knowledge and prescription rates when analyzed together. However, among private psychiatrists, perceived acceptability has a mediating effect on knowledge and prescription practices. This finding stands at odds with our previous finding that Baclofen is the most commonly prescribed AUD pharmacotherapy in India. 18 This finding may reflect that physicians may be prescribing Baclofen as an ineluctable option as they did not perceive the other medications to be safe, acceptable, or efficacious.
It should be noted that our analysis did not include participants’ endorsement of standard psychosocial interventions (e.g., reducing denial, identifying triggers for drinking, and developing drink refusal skills). These approaches have had greater valuation and acceptance than pharmacotherapy in previously conducted studies. 23 Some studies indicate that preference for psychosocial interventions may reduce the use of AUD pharmacotherapies. 26
The findings of our study have important implications for training of physicians in the use of AUD pharmacotherapies in India. Common approaches used for increasing prescription rates for any pharmacotherapy have included educational programs in some form, that is, dissemination of educational materials, education, and facilitation conferences, academic detailing, and EHR decision-support interventions. However, results have also shown that, at least for AUD pharmacotherapies, efforts to increase knowledge and awareness have only been marginally effective.27–29 It has been postulated that physician attitudes may partially explain the low prescribing rates seen in these interventions. As in Western studies, in our study, too positive attitudes toward AUD pharmacotherapies led to greater prescription rates. However, for Disulfiram, perceived safety (or rather the lack of it) significantly impacted prescriptions among faculty. Differences among groups in Disulfiram prescription rates have been observed previously and may reflect a particularly cautious risk/benefit assessment or predominant focus on psychosocial treatment. 14
It has to be noted that the governing attitude may be different for different medications. The findings of our study indicate that knowledge-based training alone might not be sufficient to increase pharmacotherapy prescription rates, and interventions may also be required to cause an attitudinal shift. One previous study has suggested that training focusing on attitude can cause increased receptivity for opioid use medications, and the same should be applicable to AUD pharmacotherapy. 30 Although the present study focused only on members of psychiatric societies, psychiatrists are not the only ones who provide pharmacotherapy for AUD. Other allied professions, like emergency care physicians and hepatologists, who also have opportunities to provide AUD pharmacotherapy, have also been shown to have similar concerns. 31 Studies have also shown that, at least in some countries, patients’ experiences and attitudes also determine the use of pharmacotherapy. Therefore, the need of the hour is to develop interventions that address the perceived attitudes toward AUD pharmacotherapies for multiple segments of healthcare stakeholders.
Limitations
As the study was conducted exclusively online, some limitations and biases associated with online surveys remained. 32 Additionally, it was the convenience of online studies that made such a study possible. However, a mixed-methods approach could be used in future studies. Such a study may provide valuable insight into details around knowledge and attitudes that were difficult to capture in a survey. In addition, one limit to the generalizability of the study findings is that often, the prescription of medications is determined not only by the physician’s perception but also by the availability of the medication with the hospital. Since we did not collect information about the availability of the medications at the place of practice, we could not control for this variable. Additionally, we did not collect data about non-responders and hence were unable to determine if there was any selection bias. The analytic strategy used also had its limitations, as the results indicate the correlation between two variables rather than identifying one variable as the dependent variable. This single-item ordinal nature of the attitude variables led us to use this analytic process. Regardless, the survey results indicate important factors that determine prescription practices of AUD in India—a topic that has not been previously explored before. The results also indicate the need to address attitudinal concerns in specific pharmacotherapies.
Conclusions
Different attitudes play different roles in moderating/mediating physicians’ choice of medication for AUD. The role of attitudes also varies across subgroups of clinicians. Safety and acceptability are prime considerations for increasing the number of prescriptions for acamprosate and naltrexone. For Disulfiram, efficacy is the most important consideration. Additionally, a perceived lack of safety reduces Disulfiram prescriptions in certain groups. The study indicates that training addressing specific attitudes toward specific medicines may be required to optimize AUD pharmacotherapy in India.
Footnotes
Acknowledgements
We thank the Addiction Psychiatry Society of India and its secretary general, Dr. Atul Ambekar, for facilitating its members’ responses to this study.
Author Statement
The article has not been previously published or simultaneously submitted for publication in any other journal. The article has been read and approved by all the listed authors and each author believes that the manuscript represents honest work. The authorship guidelines have been met. The authors believe that to the best of their knowledge, the manuscript does not infringe upon any copyright or property right of any third party.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of the manuscript, and no parts of the manuscript were generated using any artificial intelligence tool.
Ethical Approval
An ethical approval was taken from Institutional Human Ethics Committee, 3rd Floor Academic Block, Department of Psychiatry, All India Institute of Medical Sciences, Saket Nagar, Bhopal, Madhya Pradesh, India.
Approval Number: IHEC-LOP/2023/IL055
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior Presentation
There has been one previous paper that has been published in your journal using a different set of data gathered during the same study. We believe that this paper serves as a useful addition to the published paper and builds a comprehensive picture of the topic being investigated.