
Abstract
Background:
Electroconvulsive therapy (ECT) is a widely used treatment modality for mental disorders such as major depression, bipolar affective disorder (BPAD) and catatonia. However, it is considered as one of the most controversial and misunderstood procedures, especially among caregivers.
Methods:
An experimental pre-test, post-test design was adopted. Forty caregivers of persons with schizophrenia (n = 12), depression (n = 13), BPAD with mania (n = 8), and BPAD with depression (n = 7) were selected using convenience sampling. The caregiver’s knowledge and attitude toward ECT were assessed before and after the intervention with a single session video-assisted teaching on ECT. The data collection tool used to assess the caregiver’s knowledge and attitude was based on a pre-validated questionnaire.
Results:
The pre-test evaluation demonstrated poor knowledge among 12 (30%) and a moderate level of knowledge on the remaining 28 (70%) of the study subjects. The attitude scores revealed a neutral attitude among 47.5% and a conservative attitude among 10% of the subjects toward ECT. There was a significant improvement in both mean (±SD) knowledge (13.4 ± 4.7 vs 25.6 ± 2.9) and attitude (10.7 ± 3.5 vs 14.6 ± 3.9) scores following intervention with video-assisted teaching.
Conclusion:
A single session involving video-assisted teaching improves the knowledge and attitude toward ECT among caregivers by removing the myths and misconceptions about ECT.
CTRI reference number REF/2016/11/012581
Caregivers of patients with mental illnesses have a lack of knowledge and ambivalent attitudes toward ECT. Single session video-assisted teaching intervention improves the knowledge and acceptance of ECT among them.Key Messages:
Materials and Methods
An experimental, one group, pre-test, post-test design was used. The study was carried out in the Dept. of Psychiatry, Jawaharlal Institute of Post Graduate Medical Education and Research (JIPMER), Puducherry, Southern India. The study population comprised of caregivers of patients with major mental illness attending the inpatient and outpatient units of the Dept. of Psychiatry who were undergoing ECT. The sample size was informed by the previous study conducted by Kheiri et al. 11 In that study, the authors had observed a mean difference of 7.0 units, whereas we collectively decided that a mean difference of 2.5 units is clinically significant. We estimated that a sample size of 40 would have 90% power to detect this difference with an alpha error of 5%.
Forty caregivers of patients with schizophrenia (n = 12), depression (n = 13), bipolar affective disorder (BPAD) with mania (n = 8), and BPAD with depression (n = 7), of both sexes, aged above 18 years and who can read, speak, and understand either English or Tamil, were recruited by convenience sampling. In this study, the “caregiver” refers to a person/family member who assumes the responsibility of taking care of the patient without any wages (unpaid) and has been living with the patient for at least one year. Caregivers of clients with acute medical illness, those who had a mental illness and those who had received a similar type of ECT educational program in the past were excluded.
The research proposal was approved by the institutional ethics committee (IEC) for human studies. The study was prospectively registered under the Clinical Trials Registry-India (CTRI) with the reference number: REF/2016/11/012581. Data collection was done from October 2016 to November 2016. After explaining the study details, informed consent was signed by the participants. The outcome measure used was a standardized tool that has been used in many previous studies in the Indian population.7,12–14
The knowledge assessment questionnaire had 29 items and the scores ranged from 0 to 29. A score of one was given for every correct answer and the wrong response was scored as zero. The knowledge scores were categorized into three groups: those with scores 0–11 (less than 40% of total score) were considered as having poor knowledge; 12–20 (40%–70% of total sore) as moderate; and 21–29 (more than 70% of total score) as good.
The attitude assessment questionnaire consisted of 16 items: 9 items were negatively phrased and 7 were positively phrased. The total score ranges from 16 to 48. A higher score represents a positive attitude. Scores were categorized into three groups—positive attitude: 39–48, neutral: 28–38, and negative attitude: 16–27.
After the pre-test, on the same day, a video-assisted teaching session was administered to a group of 3–5 caregivers. After an extensive literature review and consultation with the experts, a video was prepared regarding the procedure and information about ECT. The video was prepared in an actual clinical setting. The main purpose of this video was to understand and see the real clinical scenario of ECT administration to a subject. We made the video like a film enacted by simulated patients. Simultaneously, a narration of the contents was provided, followed by discussion. The total duration of the video session was 20 minutes. The quality check of the video was done by two experts (qualified psychiatrists) from the Dept. of Psychiatry, JIPMER.
Handouts were distributed to reinforce the knowledge at the end of the session. The video-assisted teaching covered of the following aspects of ECT: myths and misconceptions, informed consent, indications, pre-, intra-, and post-procedural care, and the side effects. A post-test was conducted one week after the intervention with the same questionnaire used for the pre-test.
Data Analysis
The number of study participants and the number of responses were mentioned as frequency (percentage). The knowledge and attitude scores were mentioned as mean ± SD. The number of responses for each knowledge questionnaire item was analyzed using the McNemar test with Bonferroni correction, and the number of responses for each attitude questionnaire item was analyzed using the Wilcoxon signed-rank test with Bonferroni correction. The paired t-test was used for comparing the pre-test and post-test knowledge and attitude scores. Chi-square test was used to assess the association of knowledge scores with demographic variables. Data analysis was done using Statistical Package for the Social Sciences (SPSS 16.0). P < 0.05 was considered statistically significant for all comparisons except for the item-wise analysis of knowledge and attitude scales between groups, where Bonferroni correction was applied for multiple comparisons. Accordingly, P < 0.0017 was considered statistically significant for knowledge analysis and, P < 0.0031 was considered statistically significant for attitude analysis.
Results
A total of 40 caregivers participated. The distribution of their demographic variables is shown in
Knowledge Assessment Before and After the Intervention
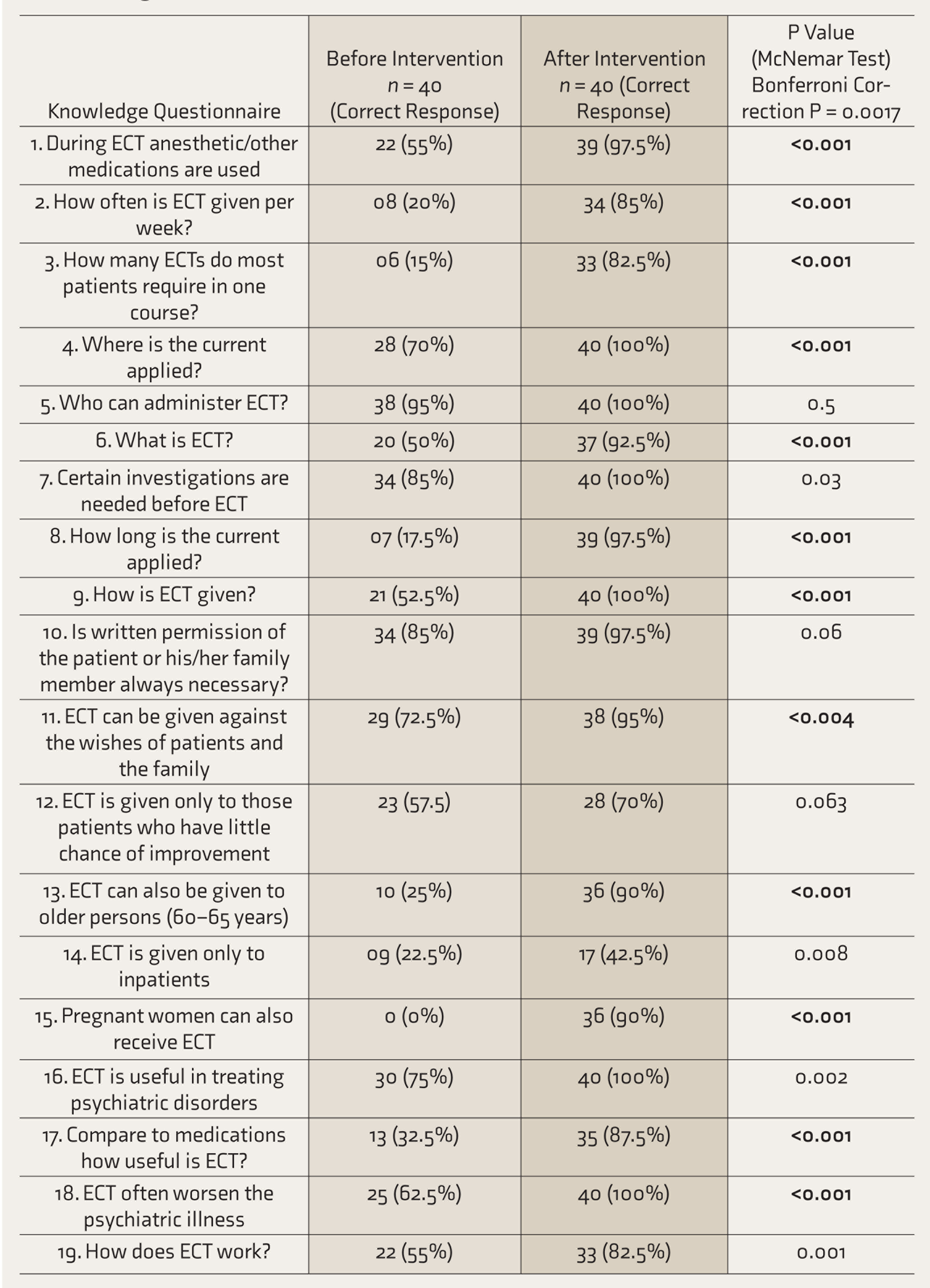
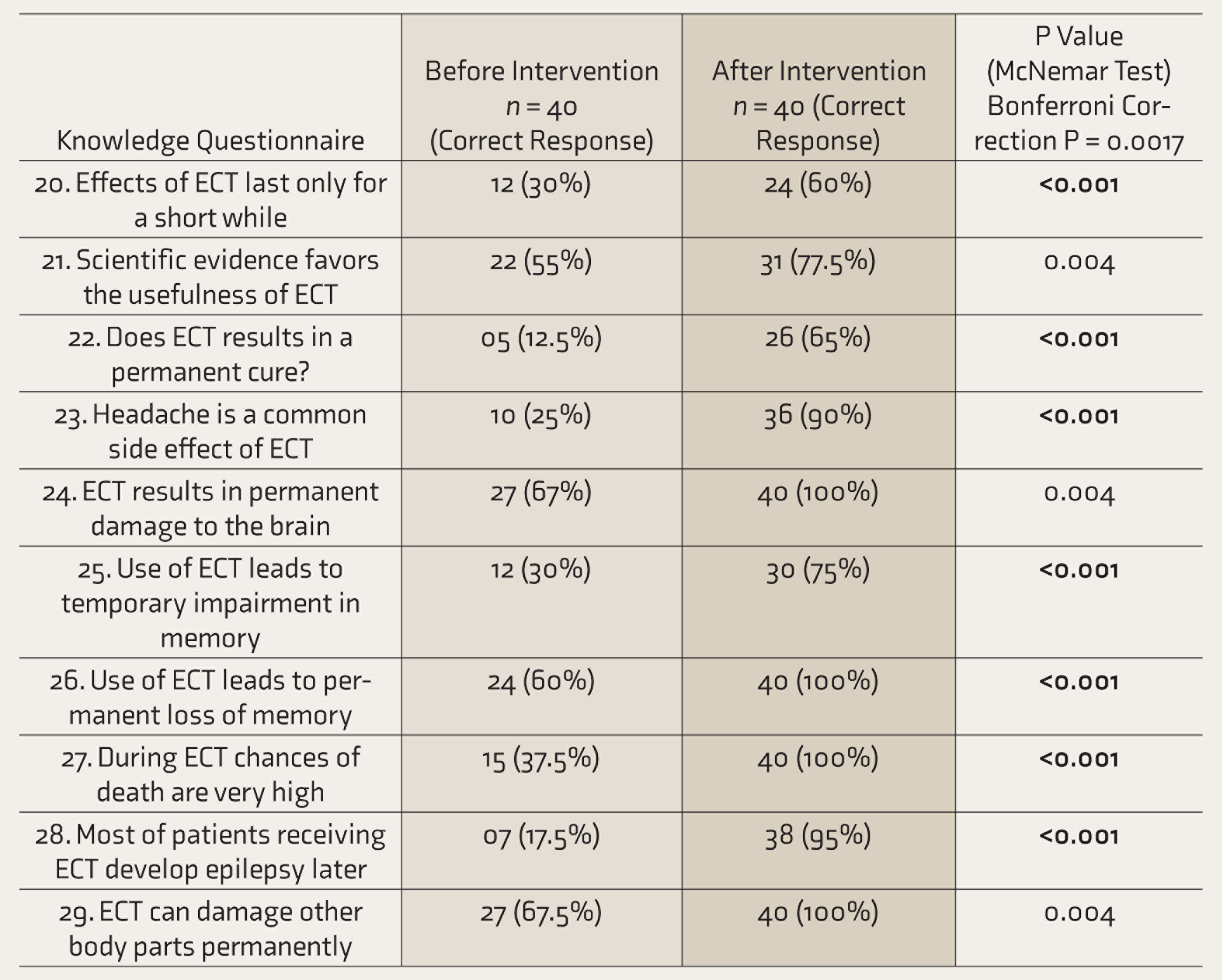
Statistically significant at P = 0.0017.
The clinical profile of patients suggested that among 40 patients, 52.5% were aged 31–45 years, 30% were 18–30 years, and 17.5% were aged ≥45 years. The main reason for ECT administration was suicidal risk in half of the patients, inadequate treatment response/resistance and refusal to take food in 22.5%, and catatonia in 5%. Duration of illness was less than one year for 45% of the patients and more than two years in 17.5%; 80% of the patients had been hospitalized 2–5 times and have had 2–5 episodes of illness, while 10%, each had ≥ 5 episodes and ≤ 2 past episodes.
Before the intervention, the mean knowledge score was 13.4 ± 4.7 and the mean attitude score was 10.7 ± 3.0. Twelve (30%) subjects had poor knowledge, 28 (70%) had a moderate level of knowledge, and none of the subjects had adequate knowledge. Attitude scores suggested that 17 (42.5%) had a positive attitude, 19 (47.5%) had a neutral attitude, and 4 (10%) had a negative attitude toward ECT.
The effect of video-assisted teaching was analyzed using the paired t-test. After the intervention, the mean knowledge score increased to 25.3 ± 2.9 from the baseline score of 13.4 ± 4.7. Similarly, the attitude score increased to 14.6 ± 1.43 from the baseline score of 10.7 ± 3.05 and both were found to be statistically significant (P < 0.001). Chi-square test revealed that none of the demographic variables were associated with knowledge or attitude scores at baseline.
Each questionnaire items of pre- and post-test knowledge and attitude score assessment are listed in
Attitude Score Before and After the Intervention
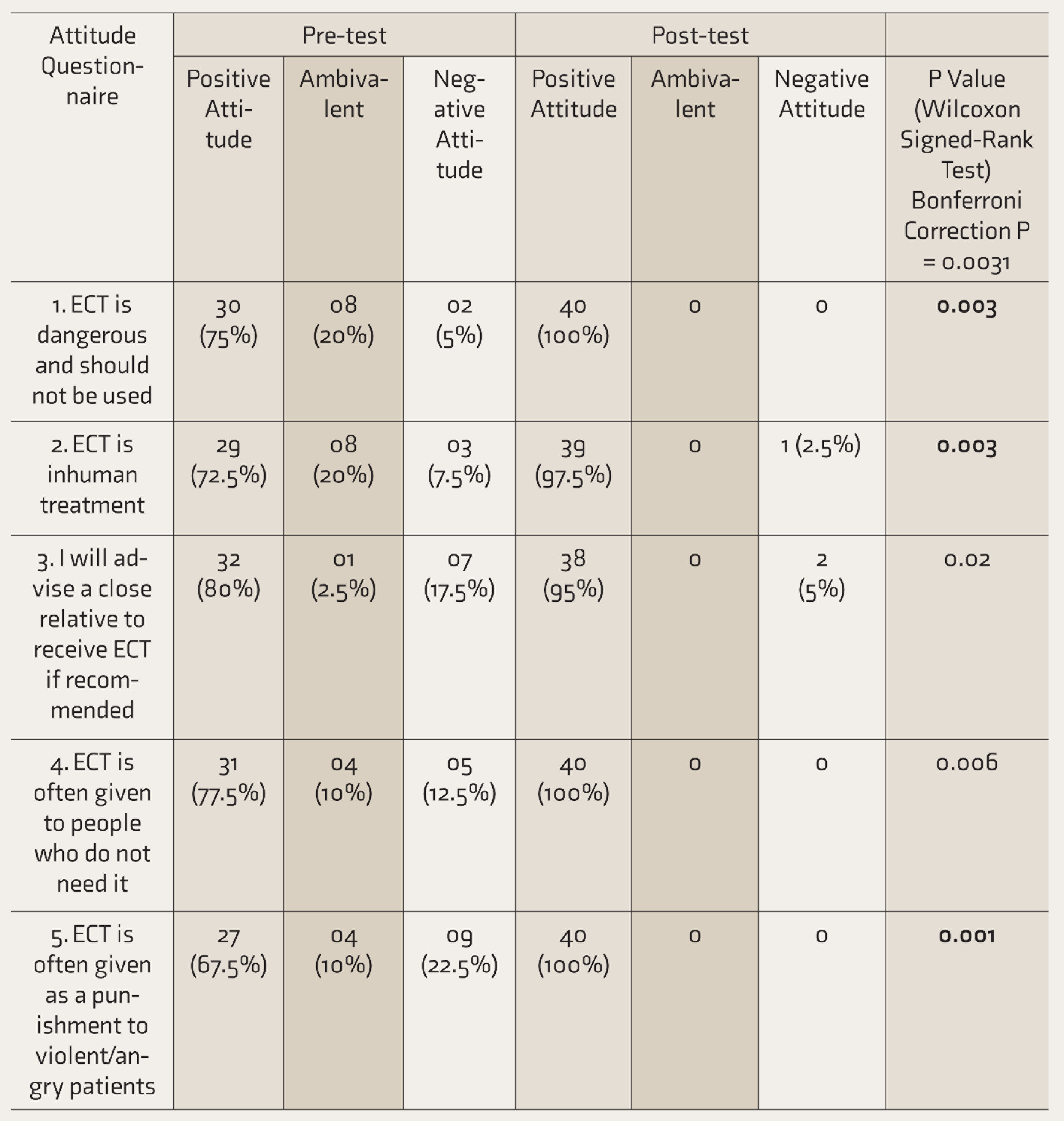
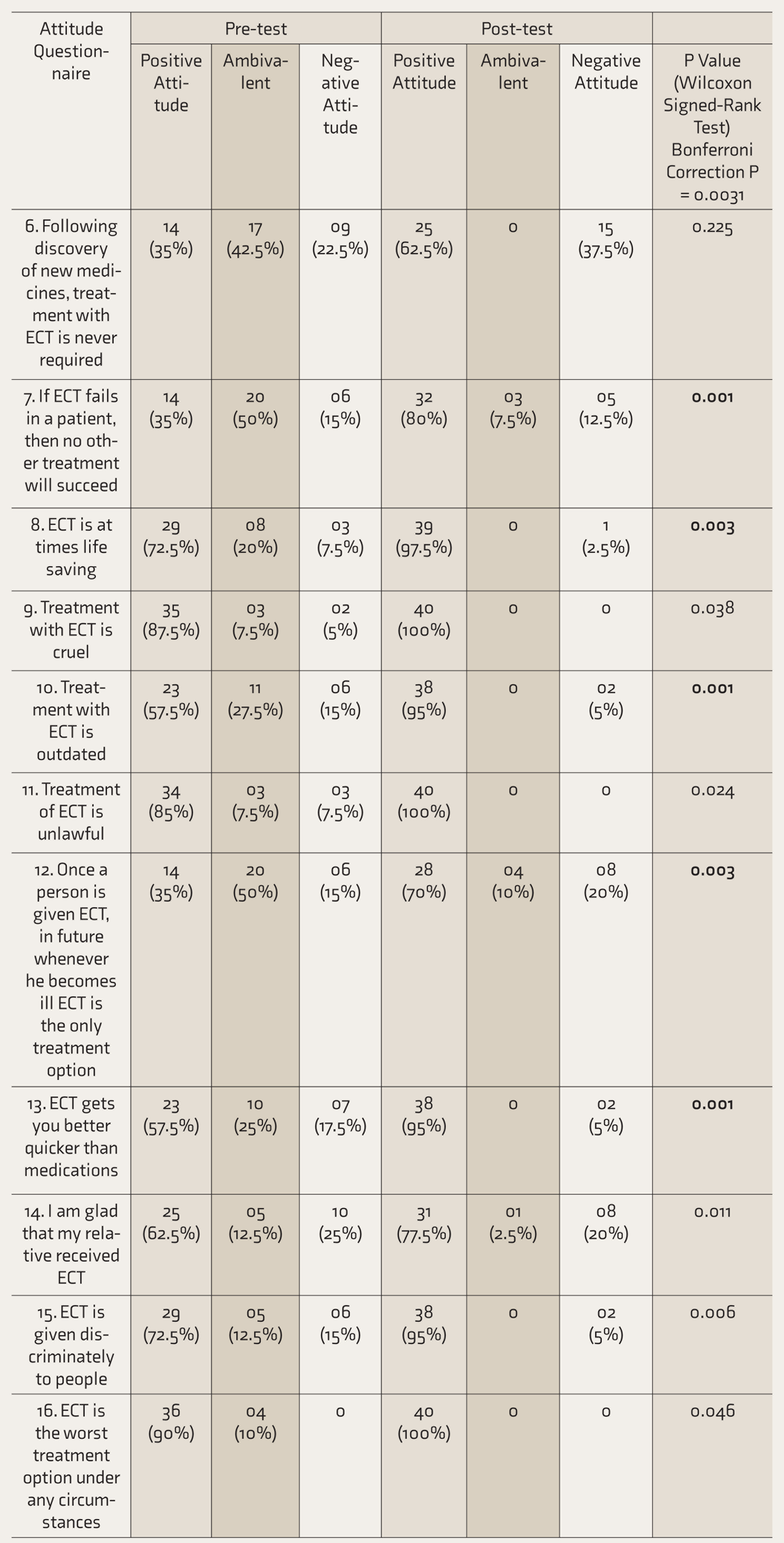
Statistically significant at P = 0.0031.
Discussion
ECT is the oldest and most controversial treatment in the field of psychiatry. 15 It has been used for nearly 80 years and has been demonstrated to produce tremendous improvements in patients with mental illness. Even today, a mental illness that is non-responsive to drugs can respond to ECT, and it is mostly indicated in catatonia, and pre- and post-partum affective and psychotic states. ECT may even be lifesaving in these patients. 15 The negative media portrayal of ECT and the use of the word “electricity” may have contributed to its negative public perceptions. This negative attitude may lead to the fear and avoidance of ECT, which acts as an obstacle to psychiatric patients’ right to an effective treatment. Hence, the authors made an effort to educate the caregivers of patients with mental illness regarding ECT through video-assisted teaching.
Previous studies that employed different methods of educational interventions are summarized in
In addition, Shamsaei et al. demonstrated that the family pre-ECT teaching intervention and counseling decreased the depression, anxiety, and stress level of family caregivers of patients with mental disorders receiving ECT. Their results suggested that even a short-term educational intervention for family members can improve the emotional outcomes of treatment in the family. 13 Drawing from this available literature, we designed a simulated video with a voice-over providing the narration and a subsequent short discussion that aimed to address the frequently asked questions regarding the procedure.
Many researchers from India had explored the knowledge and views of patients and their relatives toward ECT and found that the knowledge and acceptance of ECT were poor.26–28
The pre-assessment knowledge scores of the present study indicated that many subjects were unaware of the ECT procedure and the related facts. The fear of anesthesia, brain damage, and memory loss and the stigma associated with the treatment were reported by other researchers as the main issues raised by the patients and caregivers.8,9 In contradiction, Chavan et al. highlighted that most of the patients and their relatives were well informed about ECT, and its effects and drawbacks. However, majority of them did not consider ECT as a safe treatment during pregnancy or old age. 29 The findings of the current study were almost similar and are supported by other studies, which revealed that the caregivers had lack of knowledge regarding ECT and that a substantial number of subjects had positive attitude toward ECT.7,12,24
Virit et al. 30 assessed the attitude of BPAD patients and their caregivers toward ECT, and they concluded that patients and relatives were satisfied with the treatment, found it beneficial, and maintained a positive attitude toward its use. Mccall et al. 31 found that among patients with major depression, the patient’s quality of life and function improved as early as two weeks after the completion of ECT. Although ECT was generally viewed as beneficial, effective, and safe, memory impairment was its most commonly reported adverse effect.14,32
The present study showed a significant difference in knowledge and attitude scores after video-assisted teaching program (P < 0.001). These findings are corroborated by several other studies that assessed the effect of educational intervention using the video among various groups such as caregivers, health care professionals, and the general public.11,31,14
Review of literature suggested that educational videos and pamphlets increased the knowledge and promoted a favorable and neutral attitude toward ECT. 18 The present study also got similar findings by using video-assisted teaching combined with handouts.
Our results indicated that the intervention was effective in improving knowledge and attitudes. Therefore, the intervention may be useful in those with moderate as well as poorer levels of knowledge about ECT.
Limitations
Non-probability sampling technique, tertiary care setting, limited sample size, non-randomized design, and the absence of a control group are the major limitations. Long-term effect of the intervention was not assessed. Therefore, the persistence of educational effect on knowledge and attitude scores of the caregivers after a certain time could not be commented on.
Conclusion
The knowledge possessed by caregivers was moderate and most of the caregivers had a neutral attitude toward ECT. Video-assisted teaching helps in increasing knowledge and attitude toward ECT. Our findings may indirectly indicate better acceptance of ECT as a lifesaving intervention among caregivers of patients with major mental illness following the intervention. More educational interventions are needed to reduce the stigma associated with ECT and to improve the acceptance of ECT among the general public, patients, health professionals, and significant others.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Effect of a Video-Assisted Teaching Program About ECT on Knowledge and Attitude of Caregivers of Patients with Major Mental Illness by Padmavathi Nagarajan, Gomathi Balachandar, Vikas Menon, Balachandar Saravanan in Indian Journal of Psychological Medicine
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.