
Abstract
Background:
Caring for persons with alcohol use disorder (AUD) significantly affects the quality of life (QoL) of caregivers. According to Lazarus and Folkman’s Stress and Coping Model (1984), the severity of alcohol consumption (SAC) is a major stressor for AUD caregivers. These stressors impact well-being, with QoL linked to caregivers’ coping resources, especially social support (SS) and family functioning (FF). The study aimed to investigate the mediating roles of SS and FF in the relationship between the SAC and caregivers’ QoL.
Material and Methods:
A cross-sectional study was conducted in two psychiatric hospitals in Amritsar city, Punjab. We used a purposive sampling technique to collect data from 128 family caregivers aged 18 and above who were caring for male patients with AUD aged between 20 and 65. The assessment tools used were the World Health Organization Quality of Life-Brief Version (WHOQOL-BREF), Alcohol Use Disorders Identification Test (AUDIT), Family Assessment Device (FAD), and PGI Social Support Questionnaire (PGI SSQ).
Results:
There is a significant and partial mediation of the association between SAC and QoL by both SS and FF (P < .001, 99% CI). Moreover, SAC (r = –0.519), FF (r = –0.603), and SS (r = 0.641) showed significant correlations with caregivers’ QoL (P < .001). The mean scores for SAC, SS, FF, and QoL were 22.66 (11.38), 50.88 (9.45), 127.18 (43.85), and 84.13 (18.70), respectively, suggesting moderate SAC in patients, moderate to high perceived SS levels, moderate perception of family dysfunction, and moderate to high QoL among the caregivers.
Conclusion:
SAC detrimentally impacts caregivers’ QoL both directly and indirectly through SS and FF, with the latter serving as mediators, partially mitigating SAC’s negative impact. Clinical implications underscore the importance of tailored interventions, emphasizing the strengthening of support systems and consideration of diverse FF domains for personalized approaches. The findings contribute valuable insights for developing targeted interventions customized to the specific needs of AUD caregivers to enhance their overall QoL.
The study highlights that the severity of alcohol consumption in patients with alcohol use disorder negatively impacts caregivers’ quality of life, both directly and through the mediating roles of social support and family functioning. Strengthening these support systems is crucial for improving caregivers’ overall well-being.Key Message:
Globally, most studies on caregiving have focused on those looking after the elderly with dementia 1 or chronic physical illnesses, 2 with less attention given to caregivers of persons with schizophrenia. 3 However, there is a lack of research on caregivers of individuals with alcohol use disorder (AUD), 4 which is widely recognized as a “family disease” and presents complex challenges in caregiving and managing the consequences of addiction. 5 The multifaceted role of families in caregiving and dealing with substance dependence significantly impacts caregivers’ well-being, making them more susceptible to mental health issues. 6 In India, 14.6% (16 crore) of individuals aged 10–75 use alcohol, with 2.9 crore being dependent users. Punjab ranks third with a prevalence exceeding 28%, 7 while the overall prevalence of AUD in India is 4.7%. 8 Studies show that caregivers of individuals with AUD experience high levels of stress and reduced well-being, 9 with 95% of caregivers reporting a significant burden. 10
Within the framework of Lazarus and Folkman’s transactional model of stress and coping, 11 the severity of alcohol consumption (SAC) emerges as a significant stressor for AUD caregivers. As suggested by the model, stressors are external events or conditions that pose a threat to an individual’s well-being, and their impact is contingent on the individual’s perception and appraisal of these stressors. In this model, the outcome of caregivers’ well-being, such as their quality of life (QoL), is intricately linked to the stressors they face and the coping resources at their disposal. Central to this framework are the roles of social support (SS) and family functioning (FF) as essential coping resources that significantly shape adaptive strategies. Earlier studies12,13 suggest that caregivers who find positive aspects in their caregiving role tend to report significant SS, which is further associated with improved psychological well-being and an enhanced sense of QoL. Moreover, caregivers who report lower FF exhibited higher levels of strain and burden 14 and lower levels of QoL. 15 Conversely, those with better FF reported lower burden.16,17
The level of SS and FF significantly affects caregivers’ ability to handle stress. This study focuses on caregivers of individuals with AUD. It seeks to investigate the mediating roles of SS and FF in association with the severity of the care recipient’s alcohol consumption and the caregivers’ QoL.
Based on theoretical considerations and existing literature, the following hypotheses were framed:
Patients’ SAC will significantly and negatively predict caregivers’ QoL. The caregiver’s perception of SS and FF will significantly mediate the relationship between patients’ SAC and caregivers’ QoL.
Materials and Methods
Participants
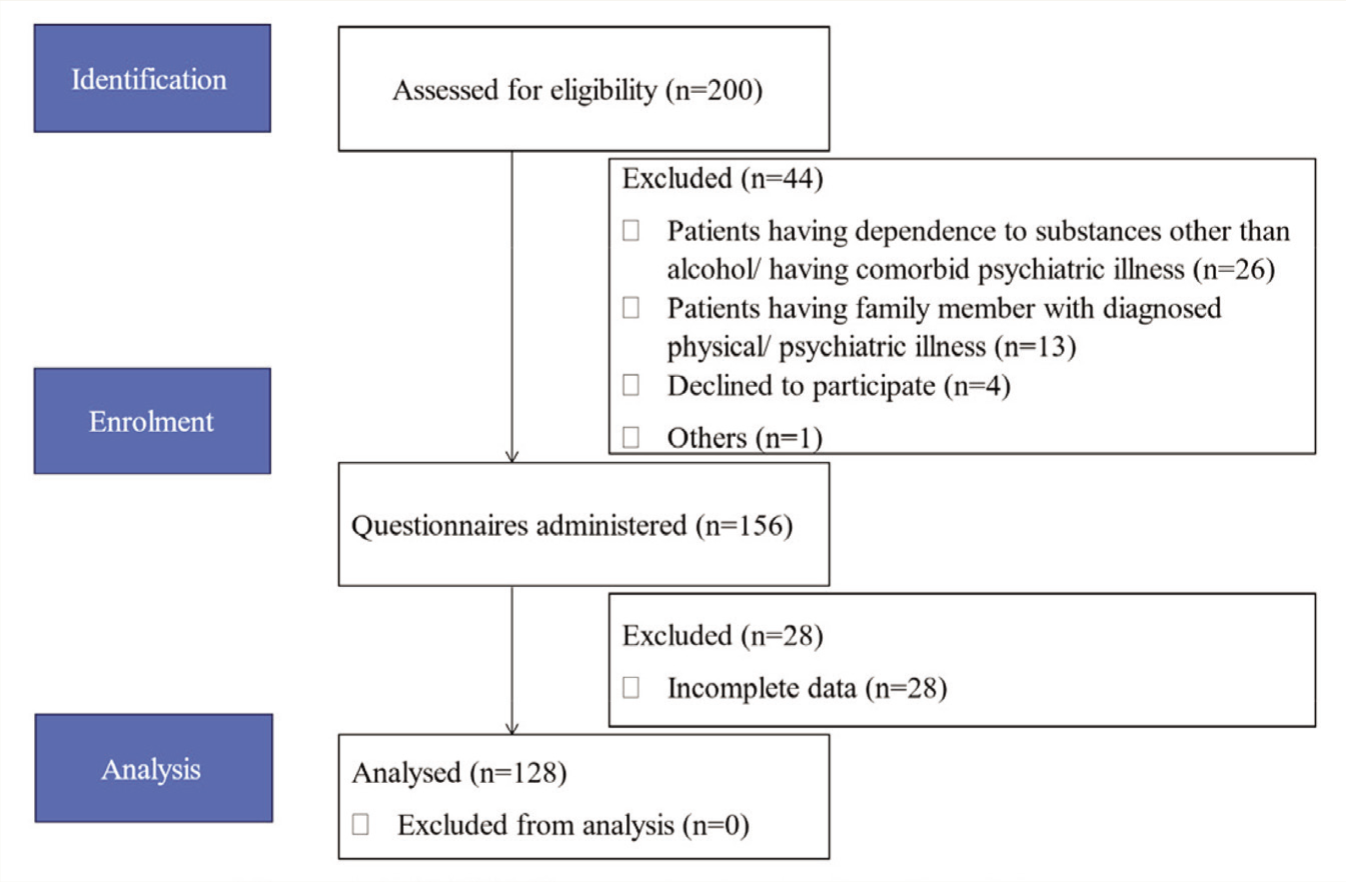
A cross-sectional study was conducted at two psychiatric hospitals in Amritsar, Punjab. The recruitment took place from August 2022 to January 2023, with approval from the University’s Institutional Ethics Committee. All participants provided written informed consent. A purposive sampling technique was used. The study involved 128 male patients with AUD along with their caregivers, including 18 male caregivers with a mean age of 44.94 years and 110 female caregivers with a mean age of 42.74 years. A priori power analysis was done to determine sample size using GPower 3.1 software. The parameters used for the calculation were an effect size (f²) of 0.1, alpha level of 0.05, power of 0.95, and three predictors (one-tailed) for linear multiple regression analysis. The software suggested a sample size of 110. However, to accommodate potential data loss, data was collected from an additional 18 samples. A total of 200 individuals with AUD were initially assessed for eligibility. Out of these, 44 were excluded for various reasons, including comorbidity (n = 26), having a family member with diagnosed physical or psychiatric illness (n = 14), and refusal to participate (n = 4). Following the identification stage, questionnaires were administered to 156 eligible participants. However, 28 individuals were subsequently excluded from further analysis due to incomplete data. Data from 128 participants were included in the final analysis. Figure 1 provides a comprehensive overview of the study’s participant recruitment, enrollment, and data analysis processes.
STROBE Diagram Showing the Flow of Participants.
Male patients aged 20–65 who met the ICD-11 criteria for AUD, along with their male or female caregivers aged 18 and above, were included in the study. Patients with dependence on substances other than alcohol (excluding nicotine) or any comorbid physical or psychiatric illness were excluded from the study. Additionally, patients with a family member diagnosed with a chronic physical illness or psychiatric disorder (excluding themselves) were also excluded from participation in the study.
A primary caregiver was defined as a person residing with the patient and actively involved in the patient’s care for at least 1 year. If more than one caregiver fulfilled the definition, preference was given to the person more actively engaged with the patient. In these instances, the extent of caregiving involvement was established according to the patient’s viewpoint. More specifically, the patient was asked to specify which family member was more actively engaged in their caregiving compared to other family members. Subsequently, data was gathered directly from the family member identified by the patient.
Assessment Tools
World Health Organization Quality of Life-Brief version (WHOQOL-BREF):18,19 The caregivers’ QoL was assessed using the English version of WHOQOL-BREF, an abbreviated 26-item version of the WHOQOL-100 that measures four domains: physical capacity (seven items, score range 7–35), psychological well-being (six items, score range 6–30), social relationships (three items, score range 3–15), and environmental health (eight items, score range 8–40). The scale has a five-point Likert-type rating ranging from 1 to 5, with higher scores indicating a better perception of QoL. The Split-Half Reliability of the WHOQOL-BREF revealed a Spearman-Brown coefficient of 0.935, indicating excellent internal consistency.
Alcohol Use Disorders Identification Test (AUDIT):20,21 The SAC in the patients was assessed using the English version of the AUDIT. The AUDIT, developed by the World Health Organization, is a 10-item scale designed to identify unhealthy alcohol use. It covers three domains: Alcohol consumption, Alcohol dependence symptoms, and Harmful alcohol use. Each of the 10 questions is scored on a scale from 0 to 4, contributing to a total score ranging from 0 to 40. A score of 1 to 7 indicates low-risk alcohol consumption, 8 to 14 indicates hazardous alcohol consumption and 15 or higher indicates the possibility of alcohol dependence. The Split-Half Reliability of the AUDIT yielded a Spearman-Brown coefficient of 0.854, suggesting strong internal consistency.
PGI Social Support Questionnaire (PGI SSQ): 22 The perception of SS in caregivers was assessed using the PGI SSQ, a self-report measure adapted from the Pollack and Harris scale (1983) 23 and customized for use in Indian psychiatric patients. Translated into Hindi by Nehra and Kulhara (1987), 22 this questionnaire consists of 18 items, each offering four response options ranging from fully agreed to not agreed. Positively worded items (e.g., items 2, 4, 8, 9, 11, 12, and 18) are scored positively, reflecting their framing. Conversely, negative items (e.g., items 1, 3, 5, 6, 7, 10, 13, 14, 15, 16, and 17) require reverse scoring to capture the intended responses accurately. The cumulative total score obtained from the questionnaire serves as an indicator of the individual’s perceived level of SS, with higher scores indicating greater perceived support. The Spearman-Brown coefficient for the split-half reliability of the PGI SSQ was calculated to be 0.743, indicating satisfactory internal consistency.
Family Assessment Device (FAD):24,25 The caregivers’ perception of FF was evaluated using the English version of FAD, a standardized measure designed to assess perceived functioning and dysfunction within family dynamics. The FAD, developed by Epstein (1983), 26 is based on the McMaster model of Family Functioning 27 and consists of 60 self-report items. Each item is scored on a 4-point scale, with a cut-off score of 2 or more indicating poorer FF. The FAD provides a total score and seven subscale scores, each representing a different dimension of FF. These dimensions include problem-solving (six items), communication (nine items), roles (11 items), affective responsiveness (six items), affective involvement (seven items), behavioral control (nine items), and general functioning (12 items). In this study, the total FAD score was used to comprehensively assess family dynamics. The FAD’s split-half reliability was assessed, resulting in a Spearman-Brown coefficient of 0.967, indicating excellent internal consistency. It has been used in several studies in India. It has been found to be a valid instrument for assessing a wide range of families in psychiatric, nonclinical, and other medical samples.28,29
Procedure
Before collecting data, participants were given clear instructions. The initial steps involved building rapport, and participants were thoroughly briefed on the study details. Those who understood the study were asked to provide written consent, and confidentiality was assured. Participants were free to withdraw from the study at any time without facing consequences. Participants were given clear instructions for each test based on the test’s respective manuals. Assessments were carried out individually, with the AUDIT administered to patients, while the remaining scales were administered to caregivers.
Statistical Analysis
The data distribution was assessed, with skewness and kurtosis both falling within the range of ±2, meeting the parametric limits. Descriptive statistics were computed using IBM SPSS Statistics software, version 21 (released in 2012, based in Armonk, New York). A Pearson product-moment correlation matrix was calculated to provide an overview of the association between study variables, with a significance level set at P < .001. The SPSS PROCESS Macro (developed by Andrew F. Hayes) 30 was used to examine the mediation effect of SS and FF on the association between SAC as the predictor variable and QoL as the criterion variable. Standardized indirect effects were calculated for each of the 5000 bootstrapped samples, and the 99% confidence interval (CI) was determined. A mediation effect was considered significant if the CIs did not include 0, with a P value of .001 indicating the level of significance. A more conservative alpha level was chosen for priori sample size calculation to ensure adequate power to detect effects. In contrast, a stricter alpha level was used during data analysis to reduce the likelihood of false positives.
Results
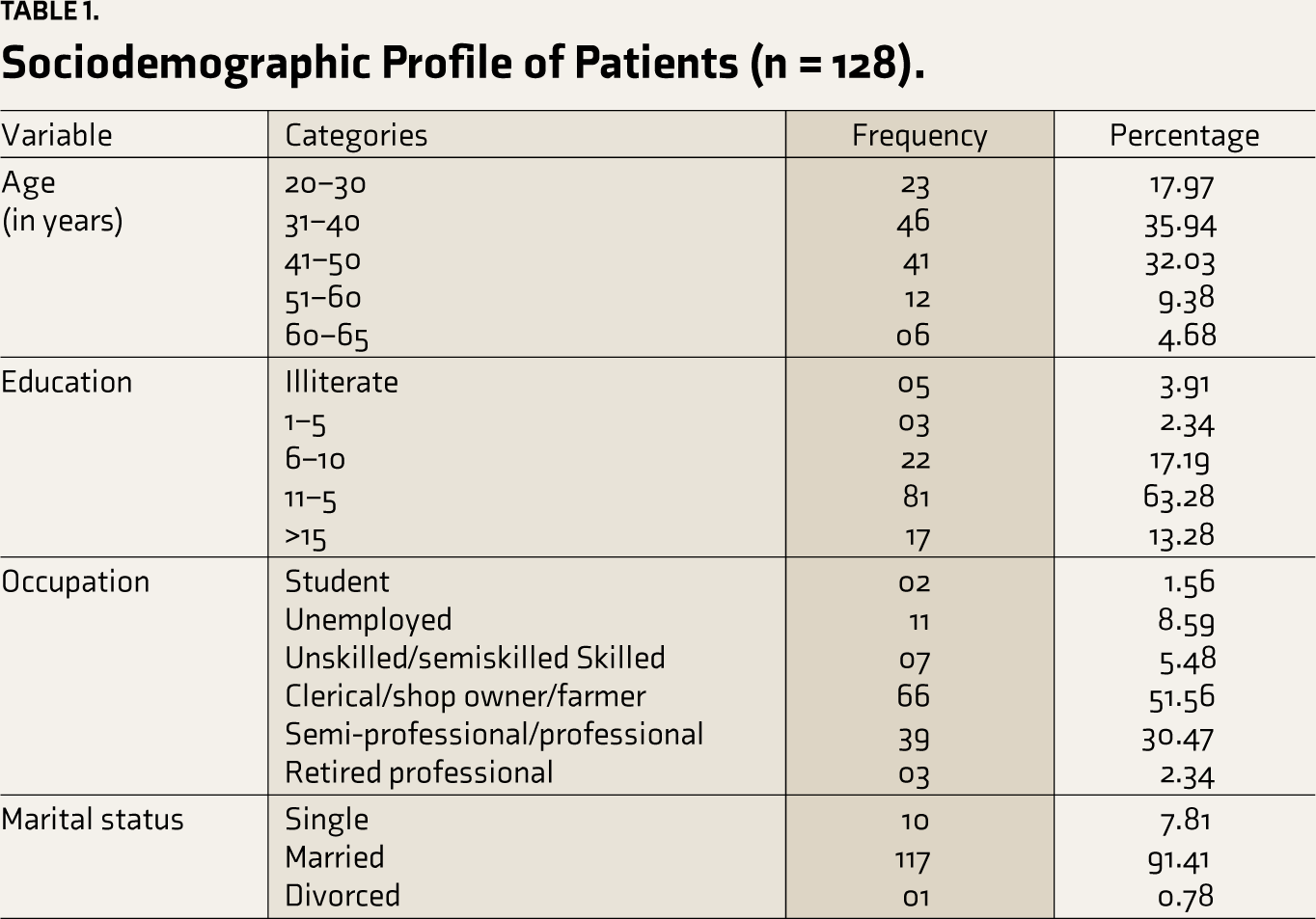
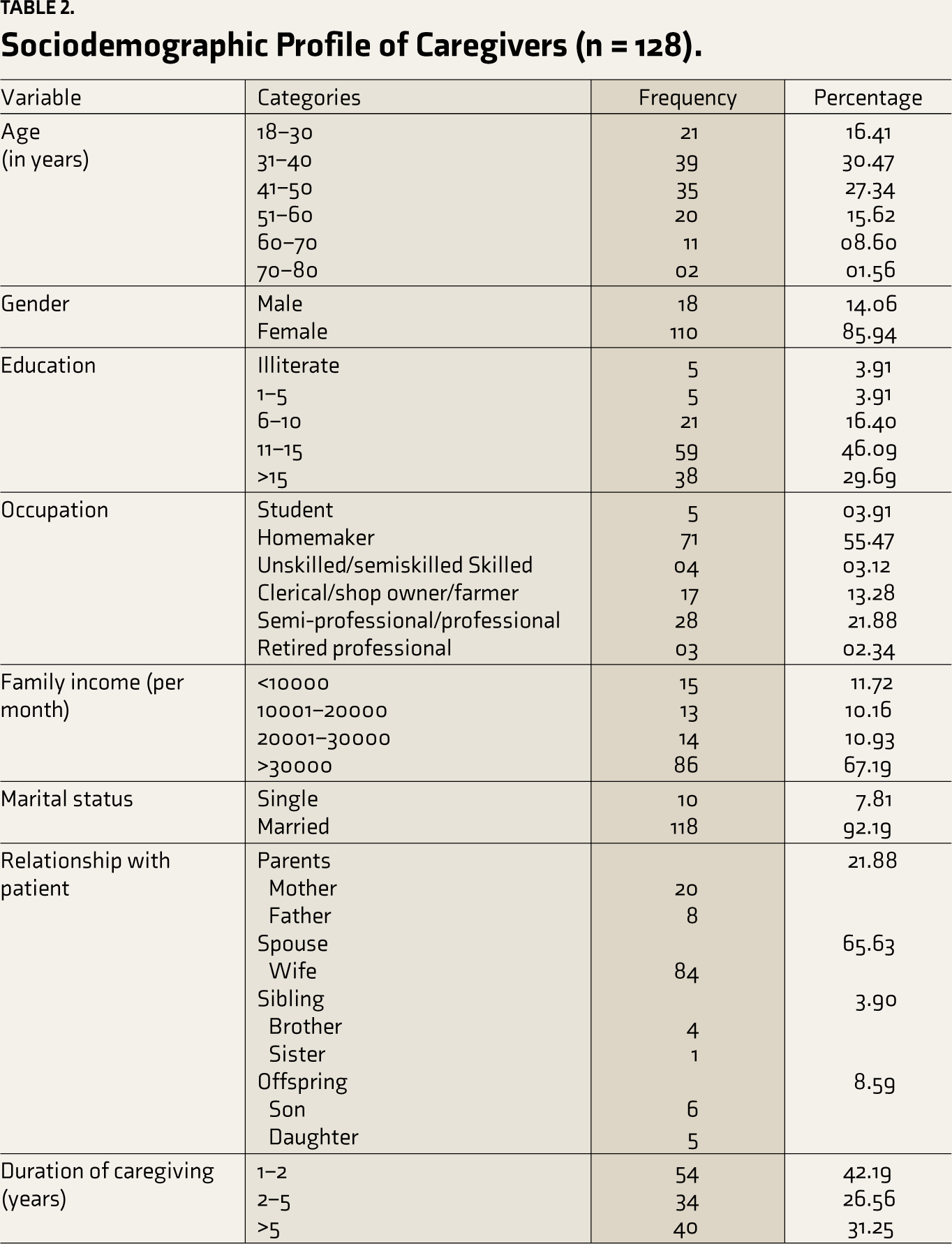
The demographic information for both patients and caregivers is outlined in Tables 1 and 2, respectively. Among the patients, ages ranged from 20 to 65 years, with the highest proportion falling within the 31–40-year bracket (35.94%). Similarly, caregivers’ ages ranged from 18 to 80 years, with the most common age group being 31–40 years (30.47%). The average age of patients was 41 years, while caregivers had a slightly higher average age of 43.05 years. Patients and caregivers had varying levels of education, with a significant portion having completed 11–15 years of schooling, comprising 63.28% and 46.09%, respectively. Occupationally, patients and caregivers were from diverse sectors. A significant portion of patients were engaged in clerical/shop owner/farmer roles (51.56%), while caregivers predominantly identified as homemakers (55.47%). The majority of patients and caregivers were married, comprising 91.41% and 92.19%, respectively. Additionally, the majority of caregivers were spouses (65.63%), highlighting the integral role of spousal caregiving within the familial context. The duration of caregiving varied among participants, with a considerable portion (42.19%) providing care for 1–2 years.
Sociodemographic Profile of Patients (n = 128).
Sociodemographic Profile of Caregivers (n = 128).
The results shown in Table 3 provide an overview of the correlations among the key variables in the study.
Showing Pearsons’ Product-moment Correlations of Quality of Life, Family Functioning, Social Support, and Severity of Alcohol Consumption.
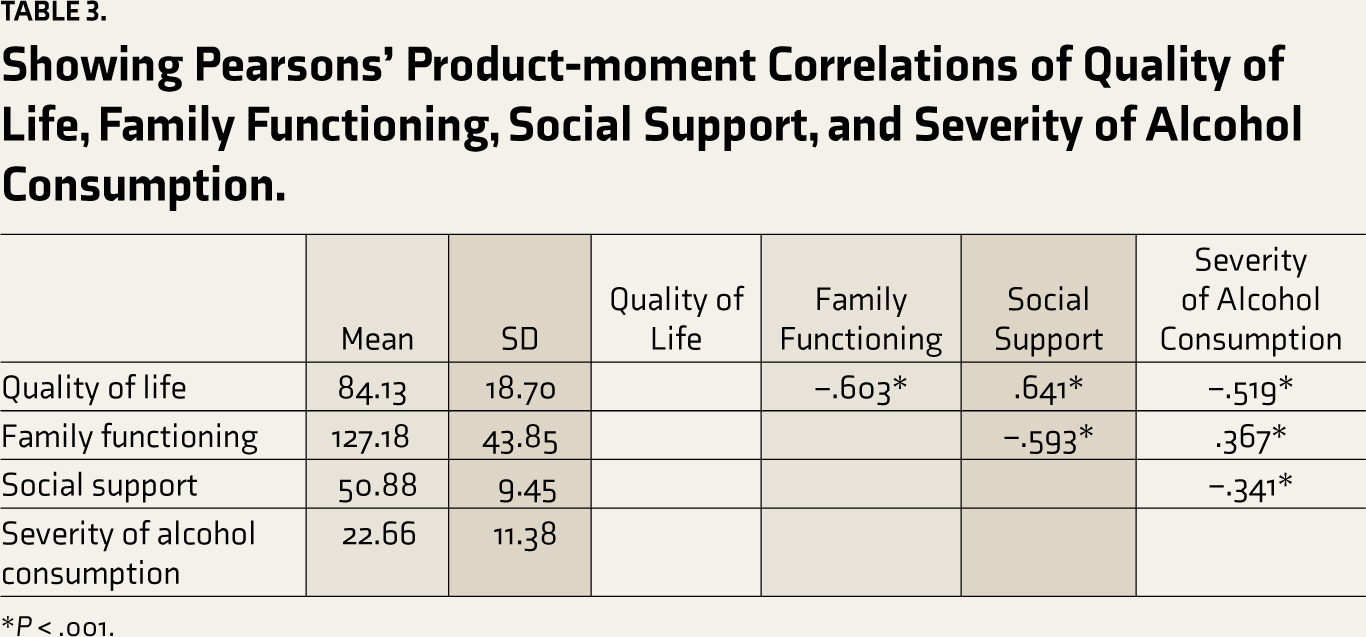
*P < .001.
The QoL scores had a mean of 84.13 (SD = 18.70). QoL had significant negative correlations with SAC (r = –0.519) and FF (r = –0.603) and a positive association with SS (r = 0.641). This indicates that higher levels of alcohol consumption and perceived family dysfunction were associated with lower QoL, while higher levels of perceived SS were related to better QoL. The FF had a mean score of 127.18 (SD = 43.85) and showed a significant negative correlation with SS (r = –0.593) and a positive correlation with SAC (r = 0.367), suggesting that lower SS and increased SAC are linked to higher perception of family dysfunction. The SS had a mean of 50.88 (SD = 9.45) and exhibited a significant negative correlation with SAC (r = –0.341). These findings emphasize the intricate relationship between QoL, SAC, SS, and FF in the context of caring for individuals with AUD.
Additionally, Table 4 presents the results of path analysis using the mediation model framework.
Path Analysis Results on Mediation Model.
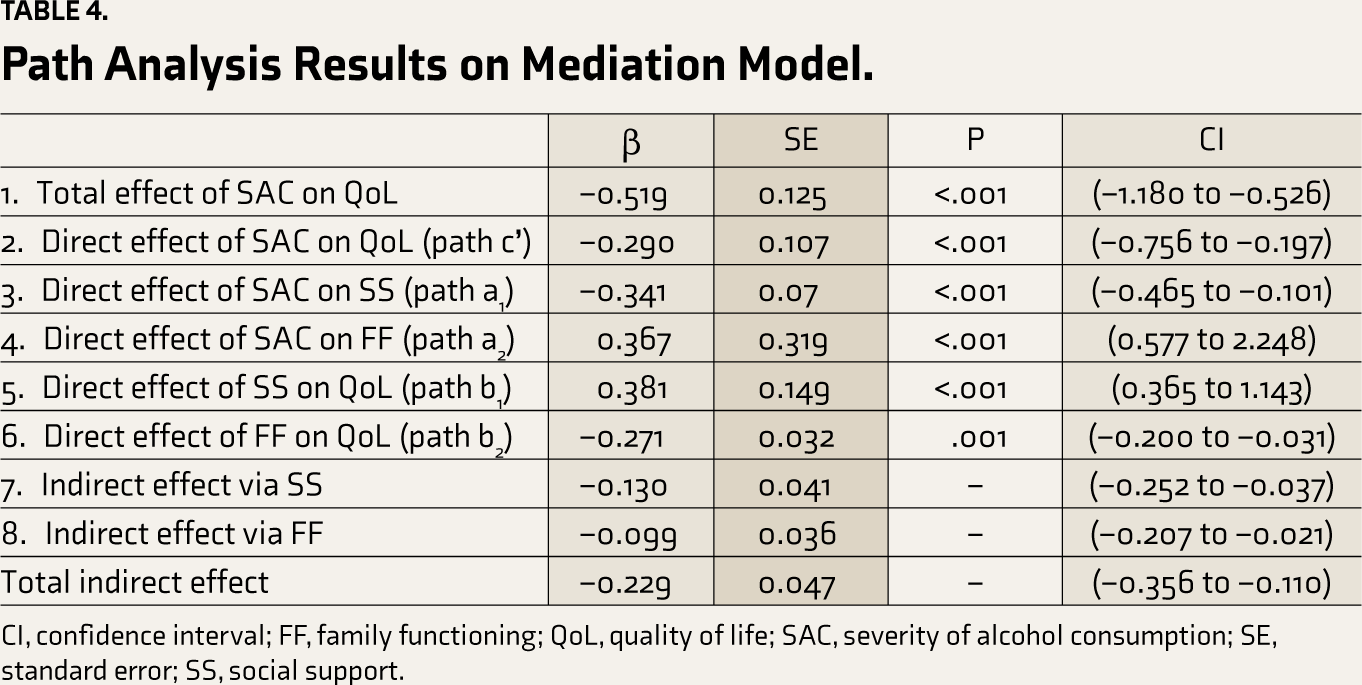
CI, confidence interval; FF, family functioning; QoL, quality of life; SAC, severity of alcohol consumption; SE, standard error; SS, social support.
The mediation model’s results provide a detailed understanding of the connections between SAC, SS, FF, and QoL. The overall impact of SAC on QoL is significantly negative (β = –0.519), indicating a substantial influence. Additionally, the direct effect of SAC on QoL, without considering mediation through SS and FF, is also negative and statistically significant (β = –0.290), suggesting that SAC independently influences QoL negatively. Thus, Hypothesis 1 is accepted.
The direct effects of SAC on SS and FF show distinct patterns. SAC has a negative influence on SS (β = –0.341), meaning that increased alcohol consumption in patients is associated with lower perceived SS among their caregivers. On the other hand, SAC has a positive direct effect on FF (β = 0.367), indicating that more severe alcohol consumption is linked to perceived deterioration in FF. Both SS (β = 0.381) and FF (β = –0.271) have direct impacts on QoL. Higher levels of SS positively predict QoL, while perceived family dysfunction negatively predicts QoL.
The indirect effects of SAC on QoL through SS (β = –0.130) and FF (β = –0.099) are also negative and statistically significant. This suggests that SS and FF partially mediate the relationship between SAC and QoL. Although the direct impact of SAC on QoL remains, the mediation through SS and FF contributes to the overall negative impact observed in the total effect. These nuanced findings emphasize the complexity of the interplay between SAC, SS, FF, and QoL, highlighting both direct and mediated pathways. Overall, Hypothesis 2 is also accepted.
Discussion
The main aim of this study was to understand the complex relationship between SAC, SS, FF, and QoL among caregivers of patients with AUD. Using mediation analysis, we aimed to identify both the direct and mediated pathways through which SAC affects QoL, focusing on the potential mediating roles of SS and FF. The analysis of these pathways in the mediation model provides a detailed understanding of how SAC influences the QoL of AUD caregivers. Importantly, examining the total effects, including both direct and mediated influences through SS and FF, offers a comprehensive perspective on the overall impact of SAC on QoL. The analysis of direct and indirect effects reveals that SS and FF partially mediate the relationship between SAC and QoL.
Interpreting SAC as a key stressor in the caregiving experience for AUD, our study is consistent with Lazarus and Folkman’s framework, 11 highlighting FF and SS as crucial coping resources. As Figure 2 illustrates, the direct effect (path c’) emphasizes SAC’s role as a stressor, exerting a considerable negative influence on caregivers’ QoL. Paths a1 and a2 shed light on SAC’s impact on SS and FF, respectively. SAC negatively influences SS (path a1) while positively affecting FF (path a2), reinforcing its role in shaping available coping resources. Paths b1 and b2 delve into the relationships between SS, FF, and QoL. Higher SS correlates with better QoL, supporting the framework’s assertion that SS is a vital coping resource.
Mediation Model With Standardized Coefficients, Illustrating the relationships Between Severity of Alcohol Consumption in Patients (Independent Variable), Caregivers’ Quality of Life (Dependent Variable), and mediators, Social Support Perception, and Family Functioning Perception Among Caregivers.
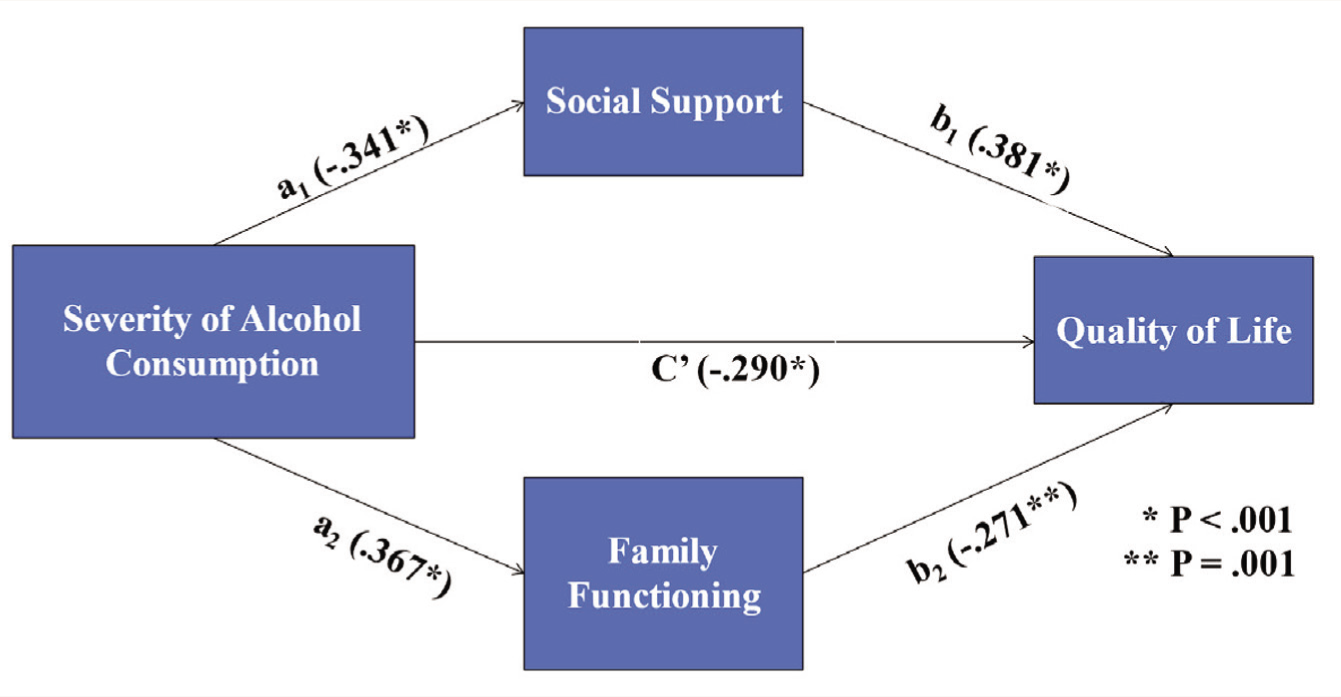
Conversely, higher perceived family dysfunction is linked to lower QoL, underscoring the importance of effective FF in caregiver well-being. The indirect effects via SS and FF align with the framework, illustrating that higher levels of these coping resources contribute to better caregiver QoL. The total indirect effects highlight the combined impact of SS and FF in mitigating the negative effects of SAC on QoL.
The obtained results prompt exploration into potential explanatory mechanisms. The multifaceted nature of SS serves as a significant mediator between SAC and QoL among AUD caregivers. Emotional support, characterized by care and understanding, mitigates the emotional toll of SAC, enhancing emotional well-being. 31 Instrumental support, providing tangible assistance, alleviates caregiving burdens, positively influencing QoL. Informational support, guiding caregivers on AUD-related challenges, empowers them with knowledge, potentially improving their ability to navigate complexities and enhancing perceived QoL. Appraisal support, offering affirmations and validation, boosts caregivers’ confidence, positively influencing their appraisal of the caregiving situation and contributing to an improved sense of QoL. SS thus emerges as a crucial mediator, addressing various dimensions of SAC-related stressors and promoting resilience among AUD caregivers.
Further, FF acts as a mediator in the SAC-QoL relationship among AUD caregivers, operating through various domains outlined by the McMaster model. 27 Effective FF in problem-solving may provide caregivers with strategies to cope with AUD-related challenges, reducing stress and enhancing QoL. Communication may facilitate open dialogue, allowing caregivers to express concerns and potentially alleviate the emotional burden associated with SAC. Clear roles and responsibilities may contribute to a supportive environment, aiding caregivers in managing the stress of SAC and positively impacting QoL. Affective involvement and responsiveness may serve as a buffer against the negative emotional impact of SAC. These FF domains collectively mediate the SAC-QoL relationship, addressing different facets of AUD caregivers.
In addition to exploring the direct and mediated effects observed in the current study, it is essential to consider the broader implications within the context of co-dependency dynamics and the cultural influences shaping caregiving experiences. Improved overall FF mediated by interventions or support systems promotes healthier family interactions and boundaries, which may further reduce enabling behaviors that contribute to continued alcohol use. 5 Additionally, cultural factors such as values inherent in collectivistic societies may result in familial cohesion, contributing to a supportive family environment. 32 Furthermore, cultural attitudes toward alcohol use and mental health issues may influence caregivers’ willingness to seek support and engage in help-seeking behaviors. 33
The findings of our study are consistent with previous research34–37 in various caregiving contexts, reinforcing specific patterns in the relationships between SAC, SS, FF, and QoL relationship. While previous studies have explored these dynamics in chronic illness,38,39 mental health,36,40 and general caregiving contexts,34,37,41 our research focuses on caregivers of individuals with AUD, providing a unique contribution. This contextual specificity enhances existing knowledge and emphasizes the need for interventions tailored to the specific needs of AUD caregivers. The study highlights the complex interplay of SAC, SS, FF, and QoL within the specific caregiving context of AUD, enhancing our understanding of these relationships.
The study has a few limitations that should be considered when interpreting the findings. First, the sample size is relatively small, and the study was conducted in a specific geographic region, which may limit the generalizability of results to broader populations. Additionally, the cross-sectional nature of the sample provides a snapshot of the relationships at a specific point in time, and long-term dynamics or changes over time may still need to be fully captured. To address these limitations, future research could benefit from a larger and more diverse sample, along with the implementation of a longitudinal study design to explore the dynamic interactions among SAC, SS, FF, and QoL over an extended period.
Conclusion
Our study highlights the complex relationship between SAC, FF SS, and QoL of family caregivers of individuals with AUD. SAC significantly impacts caregivers’ QoL, both directly and indirectly, through its effects on SS and FF. SS and FF act as mediators, partially alleviating SAC’s adverse effects. These findings underscore the need for tailored interventions for caregivers, prioritizing the enhancement of SS, addressing SAC as a major stressor, and ultimately targeting FF domains to improve their QoL. 42 Tailored support programs should be implemented to alleviate the burden on caregivers and promote their overall well-being.
Footnotes
Acknowledgements
We extend our sincere appreciation to Professor N. S. Tung (Retd.) for his invaluable assistance in statistical analysis and thought-provoking inputs, which significantly contributed to the rigor and accuracy of our research. Additionally, we express our gratitude to Bhatia Neuropsychiatric Hospital and Deaddiction Center, Amritsar, and Government Medical College, Amritsar, for generously allowing data collection. Their support was crucial to the successful completion of our study, and we sincerely thank them.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study received approval from the Institutional Ethics Committee of the Guru Nanak Dev University, Amritsar, Punjab. Approval number: 1088/HG.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
As per requirements, informed written consent was obtained from all the participants, before initiation of data collection.