
Abstract
Background:
Brief self-report measures of cognition are advantageous for flagging significant cognitive dysfunction without extensive neuropsychological assessments. The Cognitive Assessment Instrument for Obsessions and Compulsions (CAIOC-13) is a recently developed self-report that assesses everyday cognitive dysfunction in obsessive-compulsive disorder (OCD), for example, difficulties with reading, slowness, and decision-making. This study was undertaken to validate the CAIOC-13 in an Indian sample of OCD.
Methods:
75 subjects with OCD and 81 non-clinical controls completed CAIOC-13, Perceived Deficits Questionnaire (PDQ), and Dysfunctional Attitude Scale-Short Form (DAS-SF1). Convergent and divergent validity with PDQ and DAS-SF1 were established with Pearson’s correlation; the Receiver Operating Characteristic (ROC) curve was used to analyze discriminant validity; and factorial structure was evaluated using the principal component analysis (PCA).
Results:
CAIOC-13 scores showed a strong significant correlation (r = 0.56; p < .001) with PDQ and a moderate correlation with DAS-SF1 scores (r = 0.33; p = .003). CAIOC-13 could accurately discriminate between OCD and controls (area under curve = 0.92). PCA revealed strong loading on a single component.
Conclusion:
CAIOC-13 is a valid tool for briefly assessing OCD-related cognitive dysfunction in Indian samples. Future studies may examine the correlation of CAIOC-13 with standardized neuropsychological assessments.
CAIOC-13 is suitable as a brief self-report for OCD-specific everyday cognitive dysfunction in Indian samples. The instrument shows good convergent and divergent validity and discriminates accurately between OCD and non-clinical controls. The instrument may identify cognitive dysfunction without requiring extensive neuropsychological assessments.Key Messages:
Cognitive deficits are well established in obsessive-compulsive disorder (OCD) 1 and may precede the onset of OCD symptomatology, persist despite remission,2,3 and even predict poor treatment outcomes. 4 Mounting evidence in other disorders points to cognitive dysfunction as a significant contributor to poor clinical and functional outcomes, even when the severity of illness is controlled. 5 OCD is associated with significant academic and occupational dysfunction, 6 and treatments targeting cognition may enhance occupational functioning in OCD. 7 However, the relationship between cognitive and occupational dysfunction has received scant research attention. Cognitive difficulties in OCD are not routinely assessed in clinical settings, perhaps owing to the time- and labor-intensive nature of detailed neuropsychological assessments. Indeed, despite neuropsychological tests’ objectivity and rigorous psychometric properties, test performance may not always closely correspond to real-life functioning. 8
Moreover, research in OCD highlights significant heterogeneity and inconsistency in findings across studies, 9 and a recent review has suggested that methodological and psychometric issues inherent to neuropsychological testing, such as the utilization of different tests under the same neuropsychological domain, choice of outcome measures, etc., may contribute to such heterogeneity. 1 Also, discrepancies between objectively assessed neuropsychological performance and subjectively reported cognitive problems are well-known in many disorders.10,11 This indicates the critical need for brief and valid assessments of cognition from multiple perspectives, including self-rating, standardized neuropsychological assessment, and functional correlates. Existing scales to assess subjective reports of cognitive difficulties12,13 are not specific to the difficulties evinced by individuals with OCD.
In this context, the Cognitive Assessment Instrument of Obsessions and Compulsions (CAIOC-13) is a brief measure developed to assess everyday functional difficulties resulting from cognitive dysfunction specific to OCD (e.g., difficulties with reading, making choices, slowness, perfectionism, procrastination, etc.). The items in the scale have been selected from a more extensive set through pilot trials within an OCD population. 14 The scale is brief, uses simple language, and addresses key areas of expected impairment in individuals with OCD. The scale has demonstrated good test–retest reliability and discriminant validity in discriminating between OCD, depression, and healthy controls. 14 The present study aimed to validate the CAIOC-13 on an Indian sample of patients with OCD.
Method
Study Setting and Design
The study was carried out at the OCD clinic of a tertiary psychiatric institute in India between January and November 2021 and was approved by the Institute Ethics Committee. A cross-sectional design was adopted, and informed consent was obtained from all participants prior to participation.
Participants
Considering the subject-to-item ratio method, 15 the sample required for validation would be 130 (13 items × 10 subjects per item). Based on power analysis (G-power), 16 the number of participants needed to achieve a significance level of 0.05 with 80% power using a medium effect size for an independent samples t-test was estimated to be 51 in each group, a total of 102 participants. Accordingly, using a conservative estimate accounting for both methods of sample calculation and considering 15%–30% attrition/incomplete data, 150 individuals (75 patients diagnosed with OCD on the Diagnostic and Statistical Manual-5 and 75 non-clinical controls (NC) scoring below the cut-off on the Kessler Psychological Distress Scale) aged 18–50 years with a working knowledge of English language were recruited for the study. For the OCD group, individuals were excluded if they had a history of other conditions that may exaggerate cognitive impairment, such as bipolar disorder, schizophrenia, substance dependence, central nervous system conditions (cerebrovascular accident, traumatic brain injury, epilepsy, and degenerative disorders), or developmental disorders (intellectual development or specific learning disability, autism, Asperger’s syndrome, and attention deficit hyperactivity disorder). The OCD sample was recruited from individuals seeking treatment at the tertiary center. The NC sample was recruited through an e-mail or a social media flyer.
Materials
Procedure
Given the COVID-19 pandemic and based on individual preferences, the scales were administered either in person or through an online link. Among the mentioned scales, YBOCS, HAM-A, and MADRS were used only on the OCD group, and the K-10 scale was used only for NC. Individuals in the NC group scoring more than 20 on K-10 were excluded from the analysis. All the other scales were administered to both groups.
Data Analysis
The data were analyzed using R version 4.2.0. Descriptive statistics of clinical and demographic variables such as means, standard deviations, frequency, and percentages were calculated. Validity of the test was established with the following methods—convergent validity through correlation with PDQ, divergent validity through correlation with DAS-SF1, discriminant validity through the significance of the difference between clinical and control samples using a t-test, and the receiver-operating characteristic (ROC) curve. The area under the ROC curve (AUC) was computed to measure how accurately the CAIOC-13 could discriminate between OCD and NC. The sensitivity and specificity at different cut-off scores were examined to determine the optimal cut-off value at which the instrument discriminates cases and controls. Factor analysis (PCA) was used to establish factorial validity. The YBOCS, HAMA, and MADRS were correlated with CAIOC-13 to understand the relationship between anxiety, depression, and severity of OCD with subjective reports of cognition.
Results
Sociodemographic and Clinical Characteristics
Of the 81 responses received from the NC group, 11 individuals scored greater than 20 on the K-10 scale, and hence, their data were excluded from further analysis.
The OCD and NC groups were comparable in age, gender, and demographic characteristics, except for significantly higher education in the non-clinical group (Table 1). The OCD group had a range of illness severity between moderate to severe (Table 2). Lifetime diagnosis of a major depressive disorder (12%) or any anxiety disorder (8%) was the most common comorbid illness in the OCD group.
Demographic Variables of the Groups.
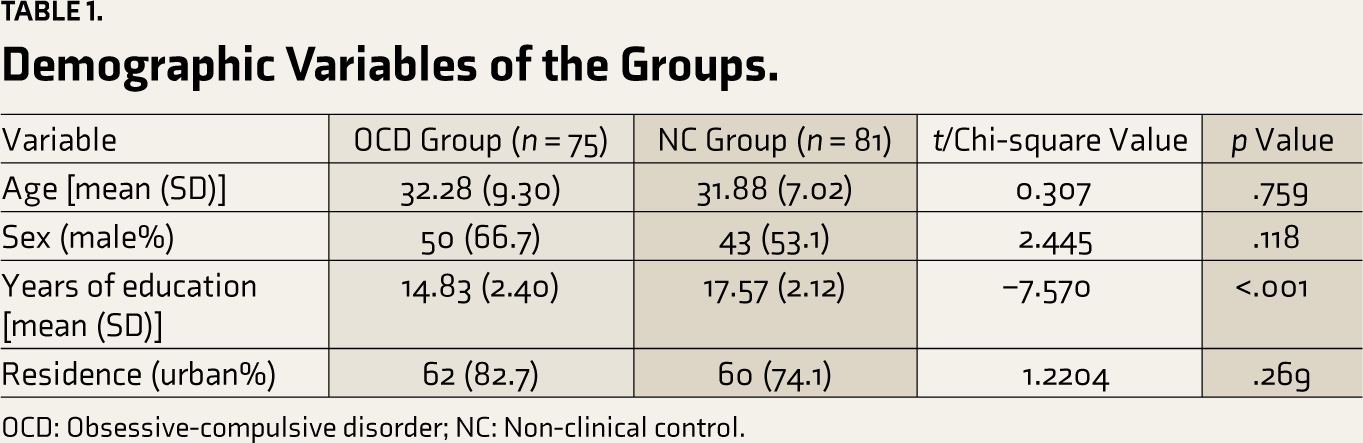
OCD: Obsessive-compulsive disorder; NC: Non-clinical control.
Clinical Measures for the Two Groups.
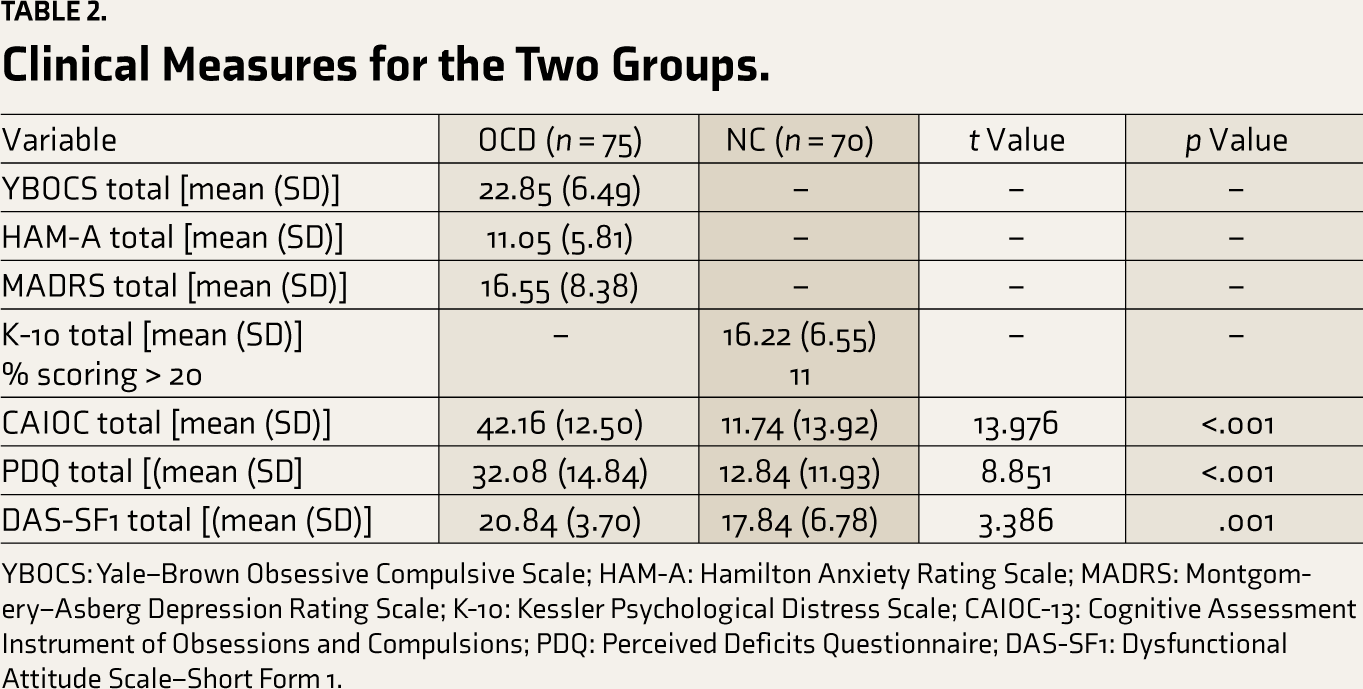
YBOCS: Yale–Brown Obsessive Compulsive Scale; HAM-A: Hamilton Anxiety Rating Scale; MADRS: Montgomery–Asberg Depression Rating Scale; K-10: Kessler Psychological Distress Scale; CAIOC-13: Cognitive Assessment Instrument of Obsessions and Compulsions; PDQ: Perceived Deficits Questionnaire; DAS-SF1: Dysfunctional Attitude Scale–Short Form 1.
Convergent Validity
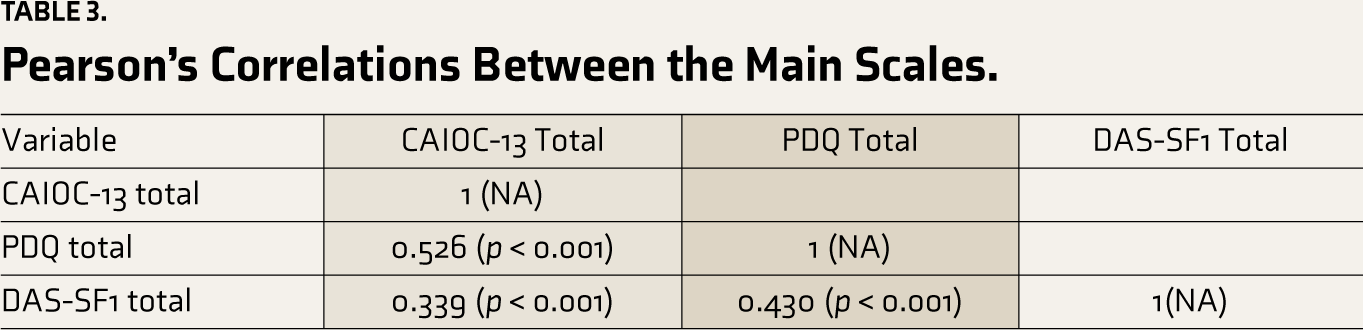
Using Pearson’s correlational analysis, the total scores on CAIOC-13 in the OCD group correlated strongly with the total scores on PDQ (0.526, p < .001) (Table 3).
Pearson’s Correlations Between the Main Scales.
Divergent Validity
Using Pearson’s correlational analysis, the total scores on CAIOC-13 in the OCD group showed a moderately significant correlation with the total scores on the DAS-SF1 (0.339; p = .003).
Correlations of CAIOC-13 were also obtained with YBOCS, HAM-A, and MADRS. The scale showed a low nonsignificant correlation with YBOCS (0.110, p = .345), a low but significant correlation with HAM-A (0.237, p = .040), and a moderately significant correlation with MADRS (0.404, p ≤ .001) (Table 3).
Discriminant Validity
The ROC analysis provided a cut-score of 28.5, which indicates the optimal combination of sensitivity (accurately identifying true case positives: OCD) and specificity (accurately identifying true case negatives: NC) (Figure 1). The AUC value was found to be 0.92 (an AUC value of 0.50 reflects the identification of cases at the chance level, and 1.0 indicates a perfect diagnostic tool). Even after adjustment for years of education between the two groups, the AUC value was found to be 0.85 (95% CI: 0.798–0.920). However, the item relating to compulsions in the CAIOC scale may confound this analysis, as controls without OCD are very unlikely to endorse this item. Hence, the ROC analysis was repeated after excluding the item “Compulsions” from the CAIOC total score. The AUC was still found to be 0.91 (95% CI: 0.87–0.96) for the unadjusted score and 0.84 (95% CI 0.78–0.90) when adjusted for years of education.
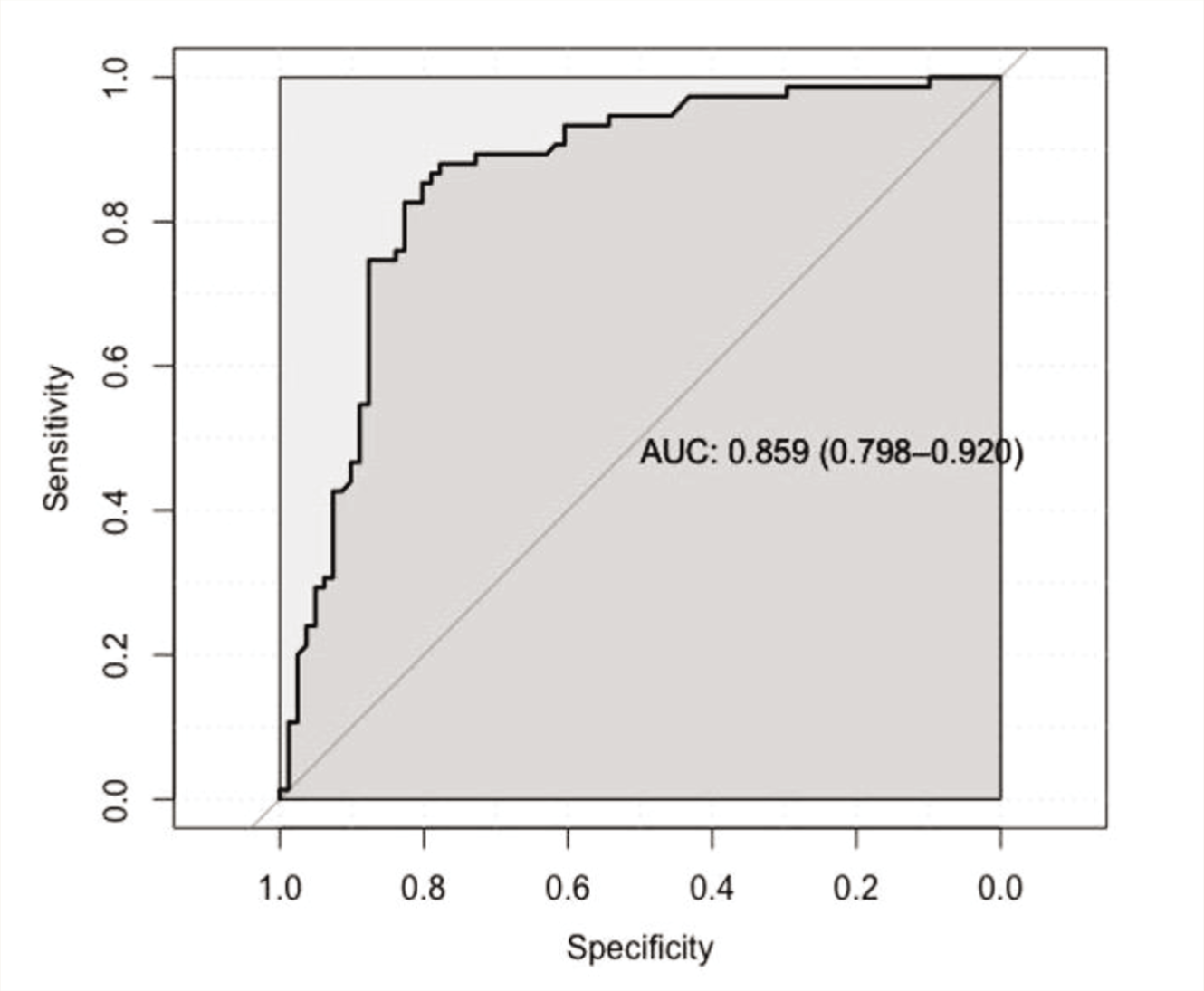
The diagonal line indicates chance level. AUC: Area under the curve.
Factorial Validity
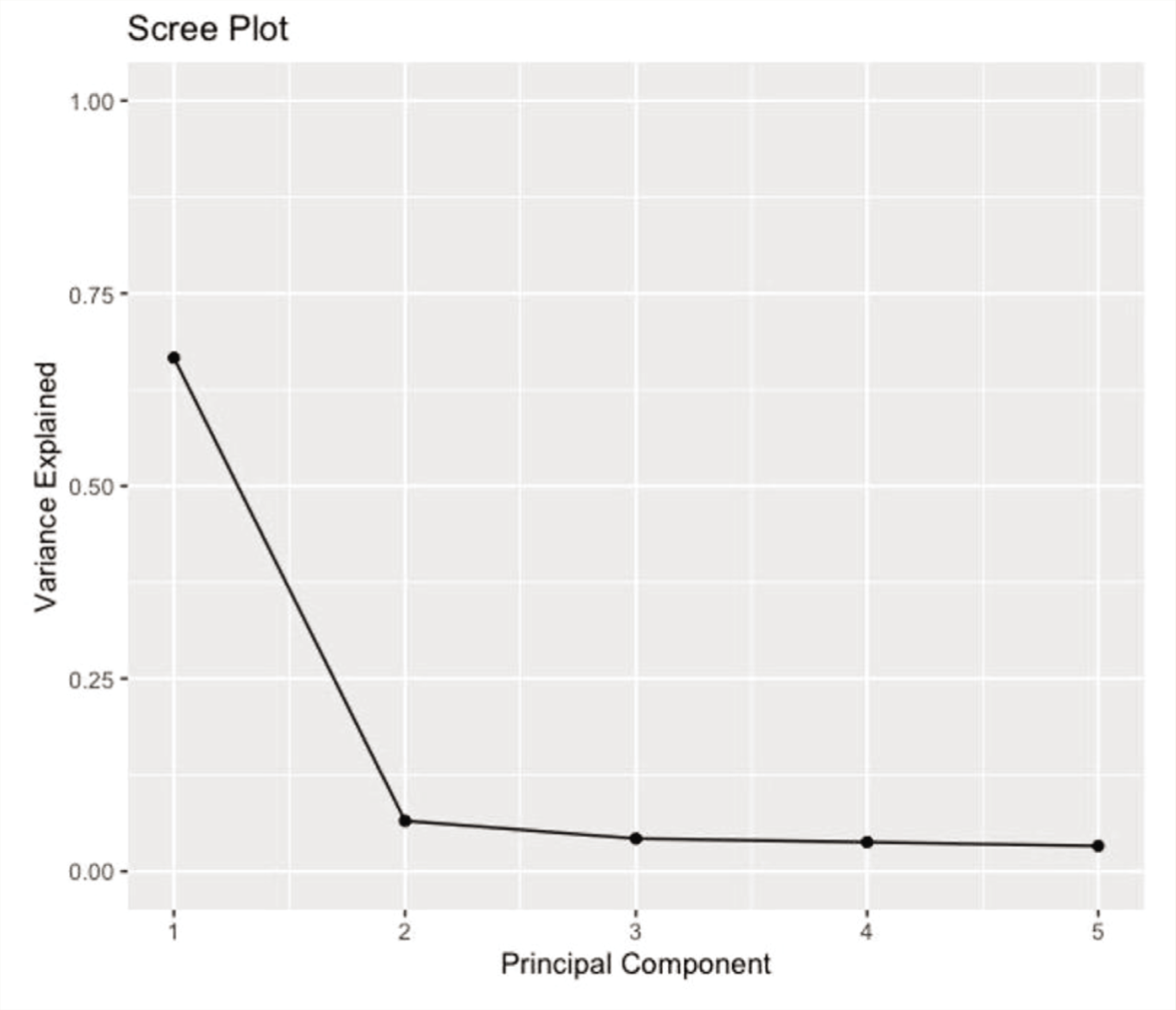
Using PCA, the CAIOC-13 item scale’s dimensionality in the OCD group was examined (Figure 2). The number of factors to retain was decided using the scree test and the interpretability of the factor solution. The scree plot indicated a one-factor solution. Factor 1 accounted for 67% (eigenvalue = 8.86) of the variance. Further examination of the component matrix revealed that all items were loaded significantly on a single factor; hence, the unrotated one-factor solution was selected.
Scree Plot Showing the Variance Explained by the Components.
Discussion
This study was undertaken to establish the validity of the CAIOC-13 scale on an Indian sample of patients with OCD. The scale was self-rated, acceptable to patients, and easy to apply. Importantly, it was sufficiently brief to be used in a clinical setting.
The study aimed to establish four types of validity for the CAIOC-13 scale: convergent, divergent, discriminant, and factorial validity. The original validation research for the CAIOC-13 scale 14 was done on a sample of individuals from the United Kingdom. There are some significant differences between both studies. The original study established concurrent validity using the Clinical Global Impressions Scale—a clinician rating of OCD severity—and the Sheehan Disability Scale—a self-report of socio-occupational disability. The study also used secondary correlations with YBOCS and MADRS for concurrent validity. However, no other measure of cognitive deficits was used. Concurrent validity indicates whether a test designed to measure a particular construct correlates with other tests of the same or similar constructs. 24 In the present study, we used PDQ, a self-rated tool for everyday cognitive dysfunction validated in multiple sclerosis and depression. PDQ assesses cognitive difficulties in various domains, including attention, retrospective memory, prospective memory, and planning and organization. Although CAIOC-13 and PDQ are both self-report measures of cognitive dysfunction in everyday life, the PDQ’s focus on prospective and retrospective memory deficits may make it less relevant to OCD since the literature has established that everyday memory in OCD is intact,25,26 along with subjective confidence in one’s memory.27-29 Our findings demonstrate a significant positive correlation (r = 0.526) between CAIOC-13 and PDQ, considered moderately strong in medical research. 30 In addition, our findings also show that individuals with higher severity of depression and anxiety report more significant cognitive dysfunction on the CAIOC.
The original study did not establish divergent validity of CAIOC-13 with any other scale. Divergent validity requires that the scale show a weak correlation with dissimilar measures. 24 Accordingly, CAIOC-13 shows a moderate correlation (0.339) with the DAS-SF1 in our study. The DAS-SF1 assesses dysfunctional attitudes and cognitive biases in psychiatric populations. 23 It was primarily developed for assessing dysfunctional cognitions in depression, subtyped into categories of dependency, self-control, and achievement. A modest correlation with DAS-SF1 suggests that the CAIOC-13 distinctively measures the construct of subjectively perceived cognitive difficulties rather than dysfunctional attitudes and cognitive biases. However, it is to be underscored that for divergent validity, correlations may be either negative or small but positive, indicating some overlap, 31 as seen in this case, since both PDQ and DAS-SF1 have a small number of similar items—for example, DAS—“If I do not set the highest standards for myself, I am likely to end up a second-rate person”; CAIOC—perfectionism—“Do you feel the need to have things perfect?”).
The ROC analysis was used to establish the discriminant validity of the CAIOC-13 scale. 32 The ROC graph was used to visualize and choose classifiers, that is, to assess the test’s capacity to appropriately categorize participants into clinically relevant subgroups based on performance. 32 In the present study, findings from the ROC analyses suggest that the CAIOC-13 could be an effective measure for discriminating between patients with OCD and NC. The optimal cut-off score, which yielded high sensitivity and specificity, was 28.5, 10 points lower than the original study. 14 This suggests that in Indian samples, 28.5 is the optimum score to reliably discriminate between OCD-related cognitive dysfunction and other generalized, non-clinical dysfunction. One reason for this difference may be the fact that the original study discriminated among three groups: OCD, depression, and healthy controls. Another reason might have been the broader range of OCD severity in the original sample (YBOCS score between 5 and 36) compared to the present sample (YBOCS range: 19–35). The CAIOC also includes an item on compulsions, which may confound cognition measurement. However, the AUC after removing the item on compulsions remained high.
Studies across different disorders have demonstrated that greater self-reported cognitive complaints may be linked to higher levels of anxiety and depression.33,34 Hence, it has been recommended that research on the validity of self-report measures should include non-cognitive measures, such as mood, personality, and health, to explain the variance in subjective reports. 35 Therefore, the correlations of CAIOC with symptom severity measures were investigated in the current study, and subjective reports of cognitive complaints showed small to moderate correlations with depression and anxiety.
Our study’s lack of correlation between YBOCS and CAIOC may suggest that the CAIOC measures something slightly different from the YBOCS. Examining the 13 items of the CAIOC reveals that they focus on difficulty reading, doubt, lassitude, slowness, indecisiveness, perfectionism, circadian rhythms, anxiety, procrastination, flexibility, executive function, worrying about the future, and compulsions. While many of these items are related to the clinical presentation of OCD, they are not strictly the same as what is assessed on the YBOCS (time spent, interference, distress, resistance, degree of control). Thus, despite some similarities, the YBOCS and CAIOC may assess different aspects of the dysfunction caused by OCD, with the CAIOC focused on functional impairments related to cognition. Nevertheless, the lack of correlation with YBOCS is interesting since CAIOC showed significant solid correlations in the original study. 14 It has been suggested that self-report of cognition may be more accurate in individuals with higher education. 35
Similarly, it is also possible that, in individuals with higher education, self-reported cognitive difficulties (CAIOC) may more closely corroborate with clinician-assessed severity of illness (YBOCS). This aspect is challenging to compare between the current and original studies 14 since the latter reports IQ but not education, and the reverse is true of the current study. The possibility of cross-cultural differences in subjective reports of cognition has also been highlighted. 35 It may also be essential to examine the relationships between self-report of cognition and objective assessments. However, studies in different disorders have often shown this relationship to be variable or discrepant.36-39
Factorial validity aids in examining the putative underlying structure of the scale and establishing its dimensionality. The current study’s factor analysis results indicated that all CAIOC-13 items loaded significantly on a single factor of cognitive dysfunction, indicating that the scale is unidimensional and has a factor structure aggregated to produce a single construct.
Overall, this Indian psychometric study indicates that CAIOC-13 is a valid tool for screening functional cognitive difficulties in OCD. Such a tool could streamline the use of time-, labor-, and cost-intensive neuropsychological batteries. Cognitive dysfunction is prominent, persistent, and predictive of clinical outcomes in OCD3,4, 36 and hence needs to be assessed in busy clinical settings. The CAIOC-13 scale permits a brief measure of such deficits impacting functionality and is suitable for non-Western cultures.
Limitations
The current study has several drawbacks. The study sample was limited to a primarily urban, English-speaking group, which may not accurately reflect the bulk of the Indian population and hence may impact the generalizability of the findings. Even though the sample size was considered adequate for a medium effect size, a larger sample from a broader geographic area in India with a more comprehensive age range may contribute to the scale’s psychometric properties. Despite removing the item on compulsions, the AUC value remained high; nevertheless, we cannot establish that it was cognitive functioning alone that differentiated the OCD and NC groups. The results can be strengthened by comparing with other groups of psychiatric diagnoses and demonstrating the scale’s level of specificity.
Further, the validity of CAIOC with objective measures of cognition remains to be established. It may also be helpful to investigate the contributions of mood and anxiety symptoms to the discriminant validity of the tool, as well as convergent validity with objective measures of cognition. The above may be particularly important since this may help clarify nuances between overlapping terms such as “cognitive dysfunction” and “functional impairments,” which are often used interchangeably, including in the original study. 14 Finally, because the scale was a self-report and data for NC were obtained entirely online, the possibility of response bias cannot be completely ruled out. Additionally, for the same reason, two clinician-administered scales (HAM-A and MADRS) could not be administered on NC and hence not used for further analysis (e.g., ROC analysis controlling for symptom severity).
Future Directions
The CAIOC-13 aids in comprehensively analyzing the day-to-day cognitive challenges experienced by patients suffering from OCD, which are not routinely examined by currently available tools. Over a variety of categories, most patients had moderate impairment. This is the first study administering the English-language CAIOC-13 scale in Indian adults; therefore, future studies are needed to assess the replicability of these findings. Future research will be needed to correlate CAIOC-13 with standardized neuropsychological tests known to be impacted in OCD, such as domains of response inhibition, set-shifting, and non-verbal memory. More extensive sample studies may also potentially distinguish cognitive difficulties in distinct OCD symptom dimensions. The scale’s sensitivity to detect longitudinal changes in functional impairment and in response to intervention (such as cognitive training) is another important aspect to examine in the future. Furthermore, to apply the scale effectively in Indian samples, it must be translated into major Indian languages.
Conclusion
The current study has systematically established the convergent, divergent, and discriminant validity and factorial structure of the CAIOC-13 in an Indian sample. Cognitive dysfunction in OCD may contribute significantly to functional impairments but may often be overlooked in busy clinical settings. Thus, the CAIOC-13 is particularly relevant to resource-constrained settings such as India.
Footnotes
Acknowledgements
We would like to thank all the participants in this study, and the staff including the residents and the consultants of OCD Clinic, NIMHANS, for referring participants for the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study involving human participants was carried out in accordance with guidelines of the NIMHANS Ethics Committee (Behavior Sciences Division).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MB is funded by the Accelerator Program for Discovery in Brain Disorders Using Stem Cells (ADBS), Department of Biotechnology, Ministry of Science & Technology, Government of India (BT/PR17316/MED/31/326/2015).
Informed Consent
Informed consent was obtained from all participants prior to participation.