
Abstract
Background:
The pathogenesis of depression remains elusive and uncertain. The literature suggests that low-grade systemic inflammation might contribute to the etiology of depression. Other markers that are studied are serum magnesium and serum cortisol. The association between these factors might help understand the etiology.
Methods:
This was a cross-sectional study conducted on a sample of 40 participants. Socio-demographic data was noted, and the Hamilton depression rating scale was applied to rate the severity of depression. Blood samples were drawn at 8 a.m. to record a complete blood picture (to derive the neutrophil–lymphocyte ratio (NLR)), C-reactive protein, serum magnesium, and serum cortisol.
Results:
In this study, conducted on a sample size of 40, inflammatory markers such as C-reactive protein (CRP: mg/dl) and NLR were significantly increased to 15.52 ± 13.10 and 6.46 ± 2.92, respectively, showing an underlying inflammatory pathology. Serum cortisol (µg/dl) was also raised to 22.30 ± 5.46, and there was a fall in serum magnesium. Also, it is noteworthy that all these markers were significantly associated with the severity of depression, as the Pearson correlation between the Hamilton depression rating scale-21 item (HAM-D-21) score and CRP, NLR, and serum cortisol was positive and statistically significant (r = 0.55, p < .01; r = 0.51, p = .01; r = 0.46, p = .002). The Pearson correlation between the HAM-D score and serum magnesium was negative and statistically significant (r = -0.82, p < .01)
Conclusion:
There is a state of systemic inflammation, hypercortisolemia, and hypomagnesemia in depressive disorders.
Inflammation plays a significant role in the etiology of depression and other psychiatric disorders. Understanding this role helps in managing depressed patients and preventing the specific effects of inflammation on the brain.Key Messages:
Depression is a widespread mental illness, and the World Health Organization has recognized that depression is a notable cause leading to disability worldwide. 1 It has also been predicted that by 2030, depression will surpass all other health conditions and become a prime cause of the global burden of diseases. Depression is becoming a global epidemic, with over 350 million people affected. 2 The prevalence of depressive disorders in India is 2.7%, as per the National Mental Health Survey. 3 Suicide is another significant concern, along with depression, and ranks fourth among the various causes of death in 15- to 29-year-olds, as more than 700,000 people lose their lives to suicide. 4
However, the etiopathogenesis of depression remains elusive and uncertain. Many hypotheses aim to explain the etiopathogenesis of depression. The monoaminergic pathway hypothesis is one of the most widely known and discussed. However, recent research shows that there is a swift growth in the biological groundwork of depression, and it is demonstrated in other pathways, such as the inflammatory and neurodegenerative pathways, 5 dysregulations of the hypothalamus–pituitary–adrenal axis (HPA), 6 DNA injury due to oxidative stress, 7 epigenetic mechanisms, 8 and the neurodevelopmental theory. 9
Among the numerous hypotheses proposed to elucidate the etiology of depression, the inflammatory hypothesis has been studied extensively. Inflammation usually indicates cell damage caused by infections, physical injury, or the tissue response to an antibody challenge. However, with research, it has become evident that an inflammatory response can be precipitated by psychological stress, thereby linking inflammation to both physical and mental ill health. Literature suggests enhanced inflammation has been reported in depression as reflected by increased concentrations of inflammatory markers—C-reactive protein (CRP) and interleukins (IL-3, IL-6, IL-12, IL-18, and sIL-2R).10–12 A normal individual’s CRP values are generally below 3 mg/L. 13 Apart from the markers discussed above, white blood cells and their subtypes, such as neutrophils and leukocytes, are also predictors of inflammation. The neutrophil–lymphocyte ratio (NLR), which can be easily derived from the white blood cell count, is an inexpensive test, and normal levels of NLR range between 0.78 and 3.53. 14 It is probed as a neoteric biomarker for systemic inflammatory response. While elevated neutrophil counts indicate inflammation, low lymphocyte counts indicate physiologic stress. 15
The HPA axis dysregulation in response to stress is also implied in depressive pathophysiology. Under stress, the adrenal gland secretes cortisol (17-hydroxyl-11-dehydrocorticosterone). The plasma cortisol level ranges between 5 µg/dl around midnight and 23 µg/dl in the morning. 16 The impairments in the functioning of the HPA axis can be noticed in patients diagnosed with depression, along with variations in serum cortisol levels. On the other hand, the elevated level of serum cortisol is also associated with depressive symptoms and, therefore, is recommended as a biomarker of depressive disorders. 17
Micronutrient deficiencies may play a part in the etiology of depression. Magnesium has been studied most commonly. The normal serum Mg is about 1.6–2.5 mg/dl. 18 It plays a significant role in many biochemical and physiological processes. Its deficiency has been linked with impairments in the central nervous system functions, specifically in the regions that significantly contribute to the etiopathogenesis of depression—glutamatergic transmission in the limbic system and cerebral cortex. Magnesium decreases adrenocorticotrophic hormone (ACTH) release and prevents hyperactivation of the HPA axis. Therefore, if HPA axis dysfunction has a significant role in the etiopathogenesis of depression, magnesium deficiency perhaps can be a risk factor by making individuals susceptible to chronically elevated cortisol and its neurodegeneration. 19
This study aimed to determine the association between inflammatory markers, serum cortisol, serum magnesium levels, and the severity of depression. The objectives included assessing CRP, NLR, serum magnesium, and serum cortisol and the association between the markers and the severity of depression.
Methods
The Institutional Ethics Committee, Gandhi Medical College, Secunderabad, Telangana, India, approved the study proposal (Ref No. IEC/GMC/2023/07/17). This cross-sectional study was conducted from May 2023 to July 2023 on 40 treatment-naive inpatients of the Department of Psychiatry, Gandhi Hospital, Secunderabad, who were diagnosed as having a depressive disorder(International Classification of Diseases, 10th revision). 20 Those with metabolic syndrome, acute infection or injuries, chronic medical illnesses, dementia, delirium, substance use, pregnancy, lactation, and currently having menstruation were excluded.
Written informed consent was obtained from the participants for study participation and blood sample drawing. A semi-structured intake proforma was used to gather details, such as socio-demographic data. The Hamilton Depression Rating Scale-21 item (HAM-D-21) 21 was used to rate the severity of depression on the day of presentation. The blood sample was drawn the next day after overnight fasting, at 08:00 a.m., to conduct a complete blood picture, serum cortisol, and serum magnesium.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) software v. 22 was utilized for data analysis. Continuous variables’ means and standard deviations were computed depending on the distribution. Pearson correlation was done to find out the correlation between variables such as depression severity and biological markers. A p value less than .05 was considered statistically significant.
Results
The total study sample was 40, with a mean age of 25 ± 6.37 (range: 19–32 years), with male predominance (60%, n = 24). Table 1 depicts various biological markers studied, including markers of inflammation, such as CRP and NLR, and other parameters, such as serum cortisol and serum magnesium. Both the inflammatory markers were increased, and the mean CRP was raised (15.52 ± 13.10), followed by the NLR, which was also enhanced. Other markers, such as serum cortisol, were also raised, and serum magnesium was decreased. Table 2 depicts the Hamilton Depression Rating Scale score. Table 3 shows various severity levels of depression and associated mean serum cortisol levels. With the increasing severity of depression, there is an increase in the mean serum cortisol value.
Mean and Standard Deviations of Biological Markers in the Study Population.
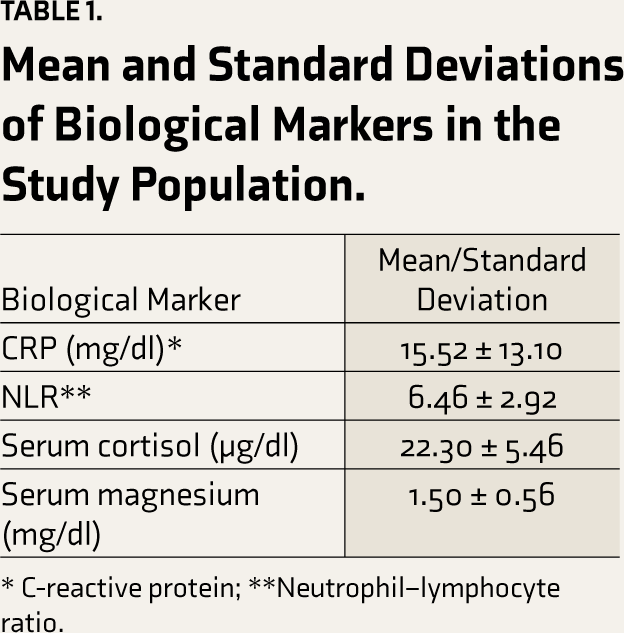
* C-reactive protein; **Neutrophil–lymphocyte ratio.
Frequency Based on Depression Severity.
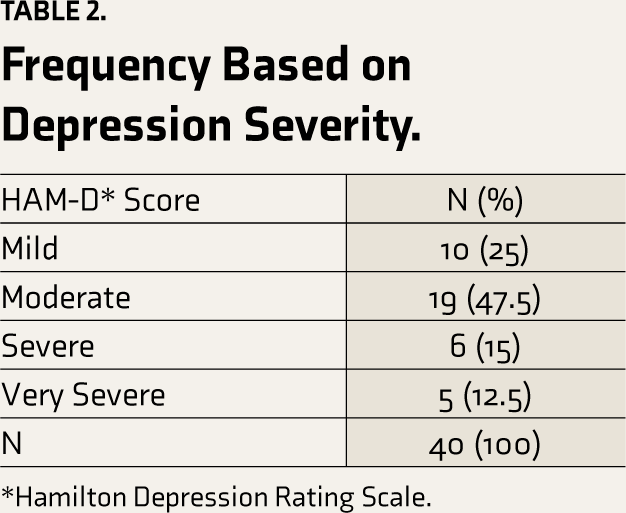
*Hamilton Depression Rating Scale.
Comparison of Mean Depression Severity Scores (HAM-D) and Mean Serum Cortisol Levels.
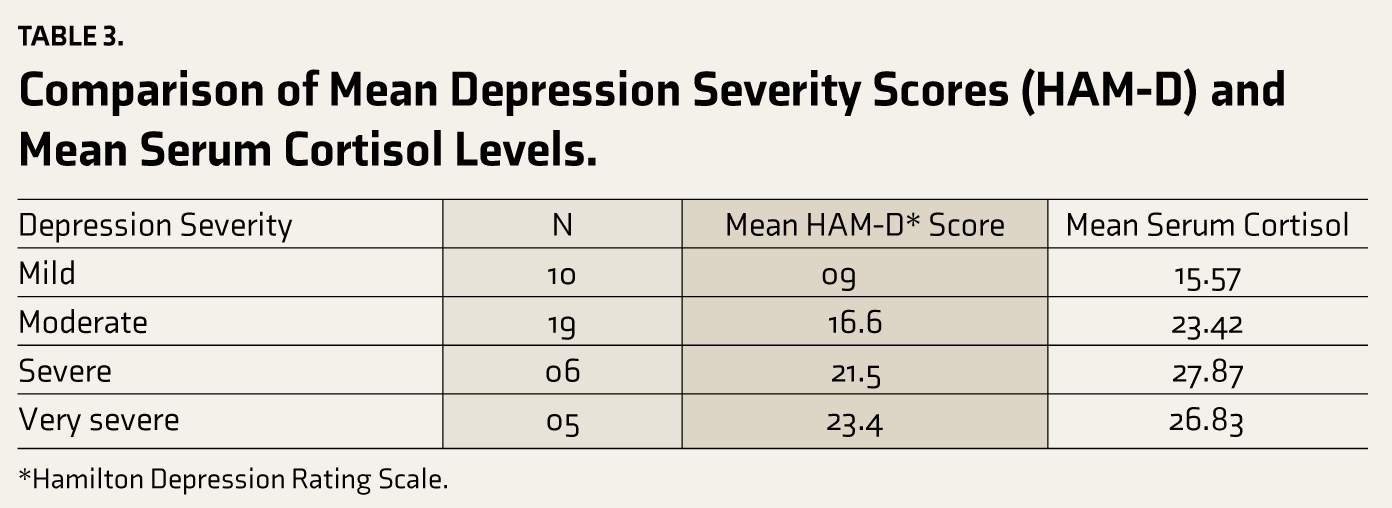
*Hamilton Depression Rating Scale.
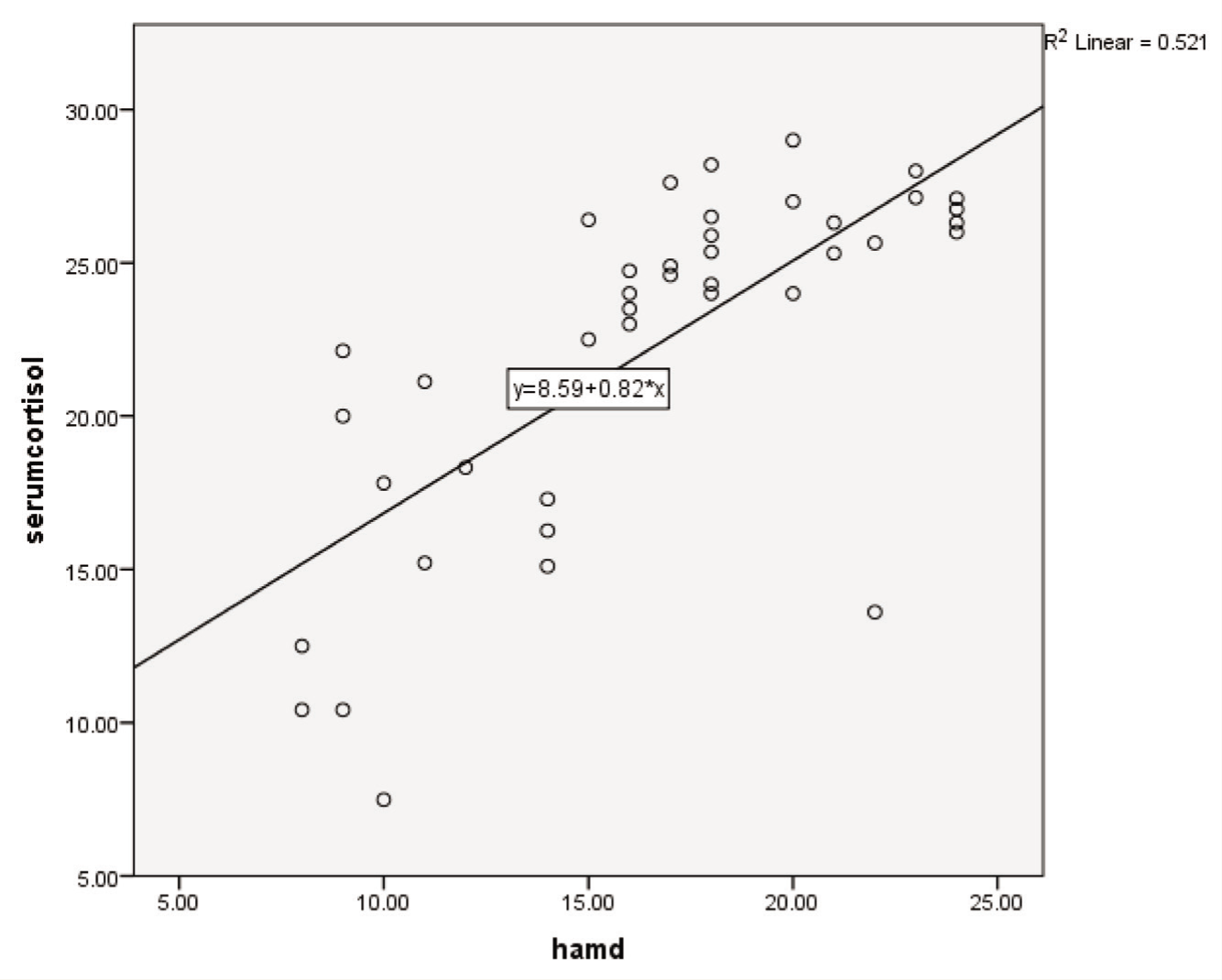
The correlation between biological markers and the severity of depression was done using the Pearson correlation test (Table 4). The HAM-D scores and CRP levels showed a positive correlation (r = 0.558), which indicates that with increasing severity of depression, there is an increase in CRP levels. This correlation was statistically significant (p < .001). Likewise, NLR and HAM-D had a positive correlation with r = 0. 515, which was also statistically significant. Other biological markers, such as serum cortisol and HAM-D, also showed a positive correlation, with r = 0.468, and this was statistically significant with p = .002 (Figure 1). Unlike other markers, serum magnesium had a negative correlation with the HAM-D scores (r = –0.826), indicating that with increasing severity of depression, there was a drop in serum magnesium levels; this was statistically significant with p < .001.
Pearson Correlation Between Various Biological Markers and Severity of Depression.
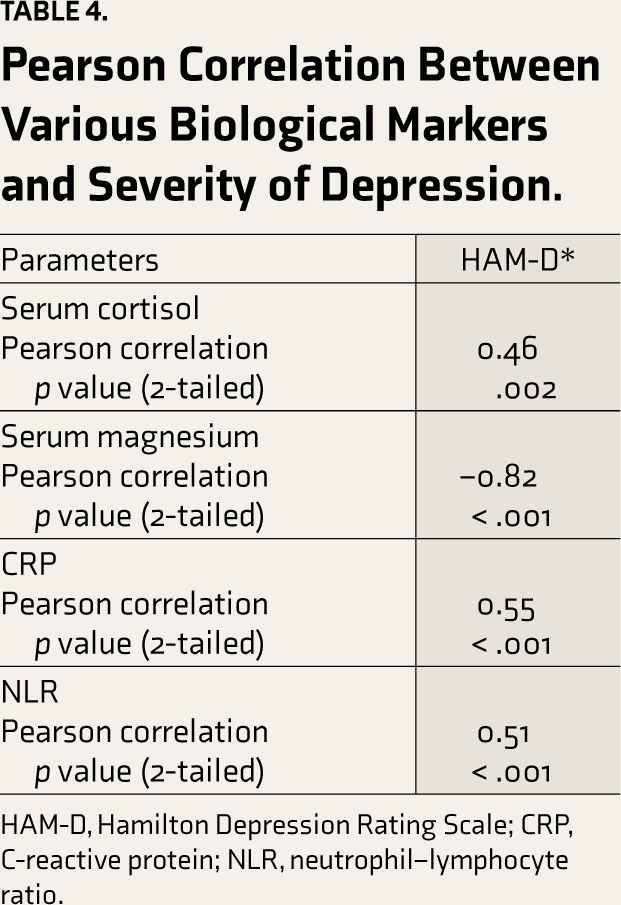
HAM-D, Hamilton Depression Rating Scale; CRP, C-reactive protein; NLR, neutrophil–lymphocyte ratio.
Relationship Between Serum Cortisol and Illness Severity HAM-D (Hamilton Depression Rating Scale) Score.
Discussion
The current study assessed the association between inflammatory markers, serum cortisol, and serum magnesium levels and the severity of depression. The CRP levels were found to be increased. The US Centers for Disease Control and Prevention and the American Heart Association have given the cut-off CRP levels as less than 1 mg/L with a low risk of cardiovascular impairment or systemic inflammation; 1–2.9 mg/L has an average risk of cardiovascular impairment or systemic inflammation; 3–10 mg/mL has a high risk of cardiovascular impairment or systemic inflammation; and > 10 mg/L has acute risk.22,23 In our study, the striking finding was that the mean CRP levels were increased (15.52 ± 13.10), indicating an underlying inflammatory pathology. This finding is analogous to previous research works, which have also found an elevated level of CRP in depressive patients.24–26 The Pearson correlation (
Another inflammatory marker studied was NLR, which was also significantly raised to 6.46 ± 2.92. Our findings denoted that NLR is also linked with the severity of depression, as the Pearson correlation between NLR and HAMD score was positive (0.538), which is statistically significant (p = .003). This would strengthen the significance of inflammation in the etiology of depression and indicate NLR as a state marker to detect the presence and severity of depression. A meta-analysis 27 also reported the findings that depression is associated with inflammation and NLR may be an indicator of depression. This finding was supported by many other studies where high NLR was significantly linked with an increased risk of depression.28,29 Hence, depression can be considered as a pro-inflammatory stage.
We found that in patients with depressive disorder, serum cortisol levels were significantly raised (22.30 ± 5.46). With increasing severity of depression (mean HAM-D scores), there was an increase in mean serum cortisol values (
Another marker that is not routinely evaluated but establishes and strengthens the role of inflammation in depression is serum magnesium, which was decreased in our study (1.50 ± 0.56), and its relationship with the severity of depression showed that the Pearson correlation was negative (–0.789) and statistically significant (p < .001). This indicates that a higher severity of depression is associated with lower serum magnesium levels. In animal and human studies, depression severity and magnesium deficiency were documented to have a positive association. Magnesium-deficient diets administered to mice had shown behavioral deficits akin to depression.34,35 Similarly, in cross-sectional studies,36,37, a reciprocal relationship was reported between symptoms of depression, magnesium levels, and magnesium intake. Magnesium ions within the central nervous system are significant neuromodulators and signaling molecules as they are endogenous NMDA receptor antagonists and interact with monoaminergic, immune, and endocrine systems. Magnesium blocks the inflammatory cytokine cascade and decreases CRP concentrations dose-dependently, while magnesium deficiency increases inflammatory markers accompanied by hypercortisolemia. Magnesium deficiency leads to the release of corticotropin-releasing hormone, which subsequently increases adrenocorticotropin hormone (ACTH) and cortisol levels. 38
The strength of the current study is that there is a paucity of published literature where all three pathways have been researched in a single study. However, the limitations include a small sample size; also, the confounders, such as age, gender, and socioeconomic status, which could alter the biological markers, were not accounted for. Hence, the results cannot be generalized. Being a cross-sectional study, we could assess only association, not causation. Also, we did not follow up with the patients to study the effect of pharmacotherapy on these biomarkers.
Conclusion
This study provides support for the hypothesis linking systemic inflammation with hypercortisolemia and hypomagnesemia in depression. There is a need for further research with a larger sample size and a follow-up design. It is pertinent to assess prospectively whether treatment with antidepressants and supplementation with magnesium leads to improvement in depression.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding Generative AI
We did not use AI tools to collect or analyse data, produce images or graphs, or write this article. We assume full responsibility for the entire content of the manuscript.
Ethical Approval
Th study was approved by the The Institutional Ethics Committee, Gandhi Medical College, Secunderabad.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the participants for study participation and blood sample drawing