
Abstract
Background:
Women in India are often disadvantaged in accessing education, employment, health services, and decision-making within families. This inequality is particularly pronounced among women with severe mental illness, especially those from rural areas.
Methods:
The study explored the employment status, facilitators, and barriers to employment among women with severe mental illness availing a rural community-based rehabilitation (CBR) program in Jagaluru, South India. Interviews were conducted with 15 women, their family caregivers, the CBR program social worker, and a community program coordinator of a nongovernmental organization partner. The study used a qualitative research design. Thematic analysis was used to identify emerging themes.
Results:
Ten women were employed. Among five unemployed women, two independently took care of household responsibilities, and one assisted the family. Medication compliance and the desire to earn money for oneself were significant facilitators. Employment opportunities for some women were hindered by poor bus connectivity in interior villages, patriarchal familial attitudes, and challenges in availing loans for livelihood ventures.
Conclusion:
Rural families access treatment for severe mental illness when it is available at the nearest government health facility. With symptom improvement, many women could avail themselves of local employment opportunities without additional inputs from the CBR team.
Pragmatic interventions to facilitate the employment of women with severe mental illness in rural communities require free treatment to be offered locally, be mindful of local employment opportunities, and unique sociocultural factors of the family and community.Key Message:
Despite a strong desire to be gainfully employed, persons with mental illness have lower employment rates than persons with other physical disabilities and the general population. 1 Employment helps persons with severe mental illness improve their self-esteem, functioning, and societal reintegration.2,3
Published studies from urban tertiary care centers in India and high-income countries have identified the following facilitators for employment for persons with mental illness: medication adherence, societal factors (social support from employer, family, co-workers, and mental health services), and work-related skills (presence of desired skills, prior work experience, access to various programs and services, involvement in supported employment programs). Barriers include illness-related factors (poor adherence to medication, difficulty in concentrating, decreased motivation for work, symptoms, medication side effects, co-morbidities), work environment-related factors (unrealistic expectations from supervisors, discrimination, lack of services), and psychological factors (lack of confidence, perceived stigma, low self-esteem).4–15 Employment assistance for persons with mental illness is restricted to limited centers.9,16,17
Implementing evidence-based supported employment models developed in high-income countries in India is challenging due to resource constraints and different sociocultural contexts. The pervasive role of the Indian family in the care, treatment, and rehabilitation of persons with mental illness needs to be factored in Sivakumar and Thirthalli. 18
Employment opportunities differ between rural and urban areas. Urban areas offer work in offices, malls, and factories, which are available throughout the year. In contrast, rural areas rely primarily on agrarian work, which is seasonal by its very nature. For this reason, impoverished rural people need to work to meet their most basic needs. 19 Employment in rural areas is sought mainly through the informal kinship network, which is more accommodating than the impersonal norms of urban areas.16,19–22 Psychological and skill-related barriers are less problematic in rural areas, as agrarian work skills are quickly learned from one’s family, facilitating employment.19,21,22
In rural India, regular treatment makes a difference in the work functioning of persons with severe mental illness. 21 However, access to mental health services is a challenge in rural India. 23 When poor rural families spend from their pocket for treatment, they may prioritize the health of the family’s breadwinner (who is more likely to be a male in a patriarchal society) over other members to ensure continued income. In such a scenario, women may be at a disadvantage in accessing health services. 24 Families of untreated women with severe mental illness may seclude or restrain them at home due to stigma and protect them from possible sexual exploitation.25,26 However, some families may not pursue treatment for women with severe mental illness even when it is offered locally, free of cost. 27
There are limited studies on women with severe mental illness from rural areas. This qualitative study aimed to understand the employment status, facilitators, and barriers to employment among women with severe mental illness availing a rural community-based rehabilitation (CBR) program in a South Indian community.
Conceptual Framework
We aimed to understand and describe the experience of women with severe mental illness in a rural community. We viewed this with a lens of intersectionality 28 in which different factors, such as being a woman in a patriarchal society, in a rural area, with a diagnosis of a severe mental illness, and poverty, intertwine with each other to create an experience. We recognized that women with severe mental illness (referred to as “women” from hereon) do not live in a vacuum and are part of a social fabric that determines access to care and recovery options, including employment when facing systemic barriers. This approach has been used by other Indian studies that have looked at disability contextually rather than viewing it as the only factor that influences experience. 29
Setting
This study was conducted in Jagaluru (rural block) in Davanagere. The Jagaluru CBR program is a partnership between the NIMHANS, the Government of Karnataka and a nongovernmental organization (NGO), The Association of People with Disability (APD). Jagaluru is predominantly rural area with low literacy. Most of the population belongs to scheduled caste tribes and backward classes. The agrarian Taluk depends on rain and is regularly declared “drought-affected.” People rely on farming either in their fields or on others. Some rear chickens, sheep, or buffaloes if they have the resources to do so. Agrarian work is seasonal by its very nature and tends to be centered around the times of sowing and harvesting. At other times, some people migrate for work on coffee plantations or for construction work in nearby cities. Interior villages have limited transport facilities, and people travel in their own or neighbor’s vehicles if they have to travel to the Taluk.
Before the CBR program, persons with mental illness traveled 50–250 km to access treatment from private or government hospitals. Since the inception of the CBR program, they have had access to free treatment from outreach camps organized at the nearest government health facility, including primary health care center (PHC), sub-centers, and Taluk Hospital. This program also involves Accredited Social Health Activists (ASHAs),3,30 a social worker, and a volunteer coordinating the CBR program, reminding families and participants of scheduled consultations, visiting their homes, and guiding them about disability certificate application and welfare benefits. In addition, the family federation for persons with mental illness has been formed at the Taluk, and families meet monthly at the Taluk Hospital for advocacy. Families of persons with mental illness without access to bank loans or local self-help groups (SHGs) (SHG primarily cater to women) can avail of revolving funds from the family federation for livelihood initiatives.
Participants
For this study, we approached women older than 18 years of age who had been diagnosed with a severe mental illness—schizophrenia, schizoaffective disorder, or bipolar affective disorder, and who were accessing support and treatment from the CBR program. All women with severe mental illness were from lower socioeconomic status. Those with intellectual and developmental disability (IDD), which could have interfered with understanding the concepts or the interview process, were excluded. A “family caregiver” was defined as a family member above 18 years of age living with any participant under the same roof for at least one year and taking responsibility for their care. All women included in the study were diagnosed and treated by the psychiatrist in charge of the CBR program (TS).
Method
The present paper is part of a PhD thesis (of MJ) on developing a framework for addressing the rehabilitation needs of women with severe mental illness in rural areas. The focus of this paper is to understand the employment status, facilitators, and barriers to employment among rural women with severe mental illness accessing the Jagaluru CBR Program. For this study, employment was operationalized as self-employment (working in one’s field, tending to livestock) and wage employment (working in others’ fields, doing construction work, working in small establishments such as shops and hotels, and livelihood based on Mahatma Gandhi National Rural Employment Act [MNREGA]). We did not consider “household chores” as wage employment.
Given the nature of the study and a desire to understand women’s and caregiver’s subjective experiences related to employment in the face of a severe mental illness, a qualitative research design with an exploratory approach has been used.
A detailed interview guide was prepared after a literature search and discussion with mental health professionals with experience in rural CBR. The interview guide was then validated for content, breadth, and depth by five mental health professionals (three psychiatrists, one clinical psychologist, and one psychiatric social worker). Women were asked to describe any employment they may have had, including the nature of their work, their experiences, their feelings about why employment was essential, available opportunities, and any challenges they faced in securing employment. If they were unemployed, they were asked how that made them feel, the possible reasons for not being employed, and any other challenges in employment.
While the interview guide was designed to elicit rich narratives from the women, we found that the responses needed longer in the pilot interviews with five women despite being given enough time and space to express their concerns. This could be due to the presence of impairment due to a chronic severe mental illness or related to sociocultural reasons, such as not being encouraged to speak openly about one’s feelings and experiences. After considering various options to promote the expression of feelings, we decided to use the photo-elicitation method to enable the women to express themselves more freely and openly. This method has been used among vulnerable populations and the community to increase participant engagement and provide rich data.31,32 The photo-elicitation method (researcher-driven), where pictorial cards were designed to aid richer conversations, was added along with the interview. Fifteen pictorial cards that depicted women and various rehabilitation needs (including employment) were prepared. Two psychiatrists validated the content of the cards.
Women and family caregivers were encouraged to speak as much as possible using the interview guide and probes. The interview usually lasted for 30–45 minutes. Data saturation occurred at the 12th interview, but supersaturation was achieved by interviewing three more women.
Data Collection
Familiarization and Training
Before starting the study, MJ attended several extension/ outreach/ satellite clinics conducted as part of the Jagaluru CBR program (November 2018 onwards) to become familiar with the community and better understand the context in which women live and work. The CBR team introduced MJ to women and their family caregivers. Their consent was sought to visit their houses for an interview. Using convenience sampling, participants were recruited over one year (October 2021–October 2022). The CBR social worker accompanied MJ to the women’s homes.
All participants and caregivers were interviewed in the Kannada language, which MJ was fluent in. Field notes and observations were recorded as memos and incorporated later in the results and discussion. Most interviews were conducted at women’s homes. Privacy was challenging in some homes (5 out of 15) where families insisted on being present. One family did not allow MJ to enter the house due to caste-related issues, and the interview was conducted on a veranda outside the home.
In addition to the women, other stakeholders (including family caregivers, CBR program social worker (1 No), and community program coordinator of NGO partner of Jagaluru CBR program) were also interviewed for data triangulation and to gain a more in-depth understanding. All interviews were audio recorded. (The interview guide relevant to employment for all stakeholders has been enclosed as a supplementary file.)
Ethical Considerations
The NIMHANS Institute ethical committee (NIMH/DO/BEH. Sc. Div./2021-22) approved the study. Women were explained in detail about the nature of the study, and their doubts or concerns were addressed. Written consent was obtained from both the woman and the caregiver. The voluntary nature of participation was emphasized. The women and caregivers were reassured about confidentiality and continuity of treatment, even if they refused consent for the study. The need for audio recording was also explained. One woman withdrew consent during the data collection process, and her data was removed from the study. All data was pseudonymized and stored using codes in a password-protected device. After completing the research, data will be retained for three years before being securely erased.
Data Analysis
The interviews were translated into English and manually transcribed using a word processor. First, MJ listened to the interviews, read the transcripts multiple times to become familiar with the data and understand concepts, and then adopted open coding manually. A six-step method for thematic analysis based on Braun and Clarke was used for data analysis. 33 Similar codes were grouped into themes. One hundred forty-nine codes were identified, of which similar codes were merged, and insignificant ones were deleted. MJ and TS reviewed the codes and reached a consensus after discussing discrepancies. Nine themes and 22 subthemes were identified. Only employment-related themes (4) and subthemes (7) are presented in this article.
Results
The socio-demographic details are mentioned in Table 1.
Socio-demographic Details of the Women with Severe Mental Illness (n = 15).
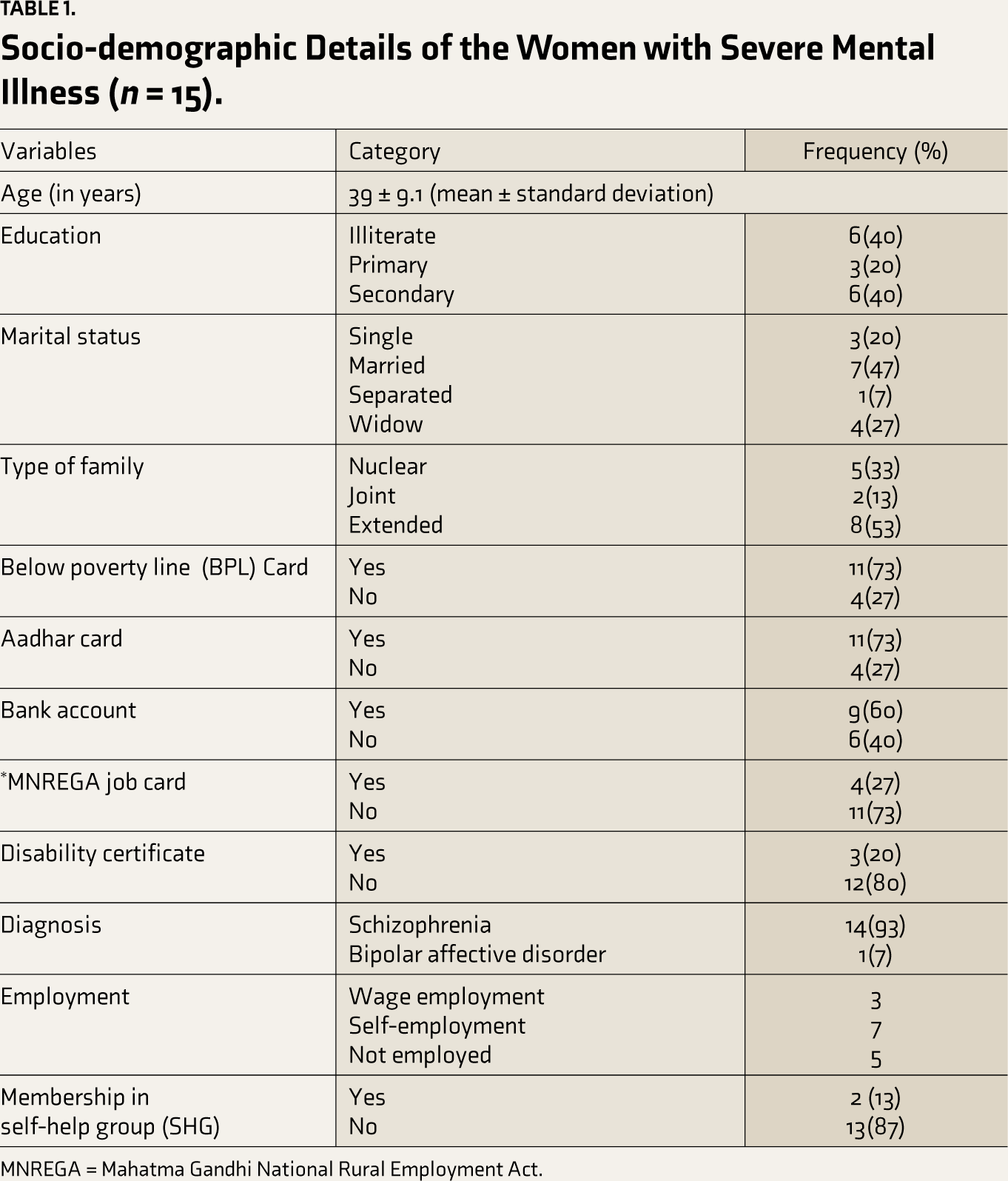
MNREGA = Mahatma Gandhi National Rural Employment Act.
Only 13 caregivers were interviewed; one woman stayed alone in the community, and the other caregiver was never available for the interview as he was working. The mean age was 49 years. Seven caregivers were male, and the remaining six were female. Five male caregivers (four husbands, two sons, and one uncle’s son) were involved in agriculture. The rest included a retired government servant and a private-sector employee. Among six female caregivers (four mothers, one daughter, and one sister), all except one (student: daughter) were involved in agriculture work.
Seven women were married and stayed with the family of procreation. Among the rest, three had never been married, one was separated (the family attributed this to the husband’s alcohol abuse), and four were widowed. One widowed woman stayed alone in a temporary shelter and was occasionally visited by her father. Another widowed woman lived with her mother while her in-laws raised her children. The remaining women stayed with their families of origin (four with parents and one with siblings) and one extended family.
Four of the 15 women interviewed received treatment at the inception of the CBR program. Three had previously sought treatment (two from the government and one from a private hospital) but had discontinued due to financial constraints and logistical issues. When the CBR program started treatment, these seven women were gainfully employed or involved in household chores. The remaining eight were on regular treatment from private or government hospitals and had then switched to the CBR program.
All four women who were never treated before the CBR program were symptomatic when Aadhaar enrollment was done in their village; hence, they did not have Aadhaar cards, nor were their names included in the below the poverty line (BPL) cards.
Among three women who pursued wage employment, two had family-owned fields; however, they preferred to work only in other fields to earn remuneration. Among seven categorized as “self-employed,” five worked in their fields (two tended to work in the field and took care of sheep and buffalo), one only cared for poultry, and the other was a tailor. All ten employed women fulfilled employment responsibilities satisfactorily, socialized with neighbors, did expected household chores, and cared for family members and themselves.
Three of five unemployed women performed household chores. Two managed household chores independently, and one assisted her mother/sister. All three had adequate self-care. The two women who could manage household chores independently also socialized with neighbors and cared for their families and themselves. The woman who assisted her family had adequate self-care but would not initiate conversations; she would reply to questions.
The remaining two unemployed women did not socialize with neighbors and needed prompts for self-care and household chores (sweeping the floor and cleaning the cattle shed). They were not on regular medications and were doing better when they were adherent.
Two married women (who were on regular treatment even before the CBR program) were involved in women’s SHG even before the onset of mental illness and continue to do so; their families paid the weekly/ monthly due amount when they were symptomatic. Five women (including two already involved in their local SHG) aspired to join the family federation to avail of loans for livelihood initiatives. Eventually, only the two women with prior local SHG involvement availed of the family federation loans as they were skilled, had family support, and could travel independently. The three new aspirants could not avail of it for the following reasons: expectation of a bigger loan amount from family, a lack of space to rear the livestock, and challenges in attending regular monthly meetings from their villages.
The following section describes the various themes and subthemes related to employment.
Theme 1: Illness and Treatment-related Factors
Medication, Treatment, and Employment
Both the women and their caregivers reported that taking the medications as prescribed helped them recover, get enough sleep, eat food, manage their hygiene, and engage in meaningful work. The following narratives confirm this observation:
After starting her on medication, she is fine. If she leaves medication, she will become sick and does not do anything, does not even go to work nor does household chores. —Pt 6’s mother I cannot miss the medication, not even for a day; if I miss, I will not be able to do anything. I feel tired; I get a headache and cannot even go to work. So, I do not miss medication, not even on a single day. I am ready to take the medication till my death. —Pt 9
Some women reported that medication side effects (weight gain, fatigue, drowsiness, decreased activity levels, and uprolling of eyes) interfered with their employment. Some side effects of the medications (such as uprolling of eyes, tremors, and drowsiness) could be easily addressed, while others, like weight gain, could not be addressed with medications alone. As weight gain led to difficulties bending for agricultural work, one woman confined herself to household chores.
I am not sending my daughter to work since she is slow in her activities after starting the injection. If I send her, people will ask why you bring such people to work.
—Pt 7’s Mother
I could not go for SHG meetings regularly because, with medications, I was drowsy throughout the day. Then I stopped going.
—Pt 15
Two women were irregular in taking medications. One believed that medications would damage her kidney, despite the treating psychiatrist and family’s efforts to convince her otherwise.
She does not take tablets on time. She sleeps at 2 or 3 in the night. If we tell her, she will ask, “Do you want me to take medicine and die of kidney failure?” She does not do anything, not even household chores. Sometimes, she sweeps and cleans, that is all. We tell her to go out and work in the field, but she does not.
—Pt 1’s Son.
Theme 2: Social Factors
Support from Family and Villagers in Employment
The entire village knew about the mental illness of women whose treatment was started at the CBR program. When the woman improved symptomatically with treatment, her family involved her in their field, livestock rearing, or household chores based on their assessment of what she could do. Other villagers supported and accommodated the woman (especially when her social support was poor) when she faced difficulties.
What happens to her is if she is actively engaged in work, she will be fine. If she does not do any work, then she becomes sick. So, we encourage her to do household work and go to the field.
—Pt 10’s Husband
Full village knows that since I was not well earlier, I must take medication. They tell them she is not well; whatever she can do, let her do it. They help me while doing work.
—Pt 9
Familial Attitudes and Practices as a Barrier to Employment
In many Jagaluru taluk households, the male head of the family is expected to make the decisions. Three women wanted to work in other agricultural fields for wages but were discouraged by their families.
My husband and son said that we are earning, and that is enough. You can be at home and care for the cattle.
—Pt 9
One woman mentioned that her family, as per their tradition, never sent females out alone.
From my family, they will not send me; see, last time I got angry and came alone for camp. I wanted to work and earn money, but my family will not allow it. Here, females do not go out and work.
—Pt 2
Lack of Women’s Empowerment as a Barrier
One woman wanted to learn tailoring, which required her to travel to a nearby city (50 km to Davanagere). Another woman who had studied until the tenth standard aspired to data entry work, which was available only in the cities. As they had never traveled alone, the family was uncomfortable sending them outside the village, fearing they might get lost or taken advantage of.
I had gone for agricultural work for some days. Then stopped. I occasionally go to my field since I handle the household chores. I have never traveled outside my village! So, if there is anything nearby, I am willing to go.
—Pt 4
See, this area is an orthodox area. They will not send women out. Even if they want to work, they have to go for daily wage jobs. They will not send them to jobs outside. The family will be afraid because of her mental illness and then because she is a woman.
—CBR Program Social Worker
Theme 3: Financial Factors
Money as Motivation
Two women felt they were not paid when they worked in their fields or cared for their livestock. So, they preferred working in others’ fields for wages. They spent the money earned on their needs (e.g., ornaments, dresses), family (e.g., groceries), or children (e.g., books and eatables).
She does not even miss a single day. She does not come to our field because she is not paid here, right? She goes to other fields and works. She cooks and prepares before us and goes regularly to work.
—Pt 6’s Sister
I want to work outside of my agricultural field. So that I will get money.
—Pt 10
Since she (the woman with severe mental illness) is getting a disability pension, she feels that she is also earning money and contributing to the family. So, she is happy about it.
—Pt 15’s daughter
Theme 4: Systemic Factors
Lack of Public Transport as a Hindrance
Several women and the CBR program Social Worker reported that the lack of public transport in interior villages hampered employment opportunities.
Public transport is less here. They have difficulty going and coming. If the employer is their family member or someone close, they will be sent to far-off places. That is all. So, they prefer daily wages in these fields.
—CBR Program Social Worker
For a widowed woman, the Family federation monthly meeting was the only possible source of seed funds for livestock rearing. She had never traveled alone, and there were no direct buses from her village to the Taluk headquarters. When the fellow villager (another woman on treatment) who accompanied her to the nearest PHC for treatment was not interested in the Family federation monthly meeting, she dropped the plan.
I would want to attend the monthly group meeting, but I have never traveled alone, and there are no direct buses. I have to depend on someone to accompany them on a bike to Jagaluru, which I do not want to do. If S (referring to another patient who stays near her home) comes, then I can come with her.
—Pt 8
Despite poverty, the extended family of another woman took care of all her needs. She was willing to take medications. However, they could not periodically bring her to the nearest PHC for consultation and medication refill due to logistical issues.
She cannot walk and come, and my father, who was bringing her, is also aged now. Furthermore, I go to work outside the village. It is almost 4 km from here to the PHC. The bus is also not there, and she does not sit on the bike.
—Pt 13’s uncle’s son
Difficulty in Getting Loans for Livelihood
Livestock rearing is a sustainable livelihood option at Jagaluru Taluk. However, some families needed more funds to pursue it. Due to previous loan defaults, they could not procure fresh loans from the formal banking sector, and the high interest rates charged by local money lenders needed to be revised.
Previously, around 30 people were trained in animal husbandry in a training institute for our patients and caregivers. They also gave certificates, and a few applied for bank loans. Still, some did not get them due to lack of proper documents or previous default in loan repayment.
––Community Program Coordinator (NGO)
Discussion
Financial gain is a crucial motivation for impoverished families. The same was true for the women interviewed for this study. Most of the women interviewed were functioning well: Two women whose families had fields refused to work there as they would not be paid. They worked in other fields. There were two other women whose families also owned fields and wished to work elsewhere for the wages. As their family disapproved of it, they continued working in their fields. However, five other women were employed (in fields and upkeep of livestock) but did not desire any wage. Each family may have its way of acknowledging or rewarding ‘invisible unpaid work’ by women. The aspiration and empowerment of women also play a role. The complex interplay of these factors needs to be explored further. One woman who was unemployed but independently handling household responsibilities felt the monthly disability pension was her contribution to family income. Though women valued employment, “being employed” or “earning money” was not determined by their wishes alone. It depended on several other factors.
Medication adherence was a critical factor that facilitated employment. Families of persons with severe mental illness avail psychiatric services when they are available, accessible, affordable, and approachable. The CBR program was especially beneficial for women who did not have support in the form of someone to bring them to the hospital for treatment. The CBR program could reach out to the seven women interviewed when symptomatic and ensure regular treatment with help from various stakeholders (including family, neighbors, local community, and ASHAs). When symptoms improved with regular medications, functioning also improved. 21 The poor functioning of two women could be attributed to medication nonadherence. Addressing medication side effects and the underlying reasons for medication nonadherence can improve employment prospects. 22
The local community was supportive and facilitated employment for the women. The crucial role of family and co-workers’ support in facilitating employment has been reported earlier.6,13,34
In three families, the attitude toward women and perception of their need to work was a barrier to employment. 10 Though the women desired to earn for themselves, the men in their families preferred that they stay at home to take care of grandchildren, home, and livestock. 15 The accumulating disadvantages related to intersectional identities, such as being female, dealing with severe mental illness, and facing restricted autonomy in family decision-making, are often amplified by patriarchal attitudes that limit employment opportunities and financial independence. This family attitude must be addressed while working with women and their families. Choices about the nature of work should be offered to women with severe mental illness to increase their autonomy.
In our experience of running the Jagaluru CBR program, many persons with severe mental illness interested in augmenting their income lack funds to start an income-generation activity. SHG, primarily meant for women, is one option. 35 The barriers to accessing SHG include the following: being unable to join the group after it is formed, not having essential documents (Aadhaar card), the societal stereotype that a single woman without family responsibilities does not require additional income, doubts about their capacity to repay the debt when there is no other earning family member, and possibly stigma of mental illness (group members would have seen them during the symptomatic stage and will be hesitant to include them in the group). 36 This fear is understandable, as the local SHG members are expected to repay their debts with 1% interest weekly.
Women with poor social support who could get treated only after the CBR program had no assets and relied solely on seasonal agrarian wage employment for survival. They must be handheld to access the Aadhaar and BPL cards necessary to avail of various social welfare schemes. They need additional support for economic and social upliftment.
The family federation in Jagaluru taluk offers loans with monthly repayments without needing collateral property, similar to SHGs established exclusively for persons with mental illness through other CBR programs in different communities.16,20,37 Though all the women interviewed were poor, only five aspired for this loan, and two with experience availing local SHG finally availed it. The travel-related barriers to attending family federation monthly meetings can be addressed by gradually starting additional SHGs at well-connected PHCs to reach out to needy people.
Two women expressed their desire to learn new skills, which required travel outside their village to nearby towns and cities. Rural families may need more confidence to send them out alone, and women may hesitate to travel far. Limited transport facilities from interior villages are another challenge. Women travel by public transport or motorcycles owned by the family. Many women travel by public transport without being accompanied by men from the household. Poor women without social support cannot afford to buy a motorcycle. Even if the family owns a motorcycle, women do not ride in Jagaluru taluk villages. Some women hesitate to travel independently due to their social inhibition and not due to lack of skill, money, opportunity, or local role models. They may travel independently only when they have a desperate need, and training is unlikely to resolve it. Women must be offered options close to their residences to upskill themselves for locally relevant employment opportunities by partnering with various agencies.
Fortunately, there are government schemes like the MNREGA program, which guarantees 100 days of wage employment within 5 km of residence, 38 which has proven helpful for persons with disability.16,20,37 However, enrolling in such a program requires valid documents (Aadhaar card, BPL card, and disability certificate for persons with disability), and implementation varies across areas. The ground-level implementation challenges need to be addressed to benefit needy people.
Strengths and Limitations
The study’s qualitative approach facilitated a deeper understanding of the factors that supported or hindered women in maintaining employment. Interviewing women in their homes and communities helped to understand contextual realities. Data triangulation was attempted, and supersaturation was reached. Describing the context, setting, and methods ensures transferability and reliability.
However, there were a few limitations. More interviews with family caregivers and other stakeholders, such as community volunteers, SHG coordinators, and possible employers, would have added to the richness of the data. Qualitative in-depth interviews among women may be challenging in specific sociocultural contexts, especially if they are not used to expressing their thoughts and feelings. We used photo-elicitation to get richer narratives. However, photo voice and other nonverbal methods of expression may be more useful than interviews in this group and need to be explored.
Conclusion
Being employed is an important aspect of recovery for both men and women with severe mental illness. The family and local community were mostly supportive of women. Medication adherence helped in symptomatic and functional recovery. The barriers include a patriarchal attitude toward the employment of women, lack of women empowerment, and limited options for upskilling and funding locally relevant livelihood options.
A multi-pronged approach is needed to make a difference. The solutions lie in facilitating access to continued treatment, addressing family attitudes toward women with severe mental illness and employment, improving local connectivity and infrastructure, exploring avenues for upskilling in locally relevant livelihood options by partnering with various agencies, and starting additional special SHGs to address needs closer to their homes.
Footnotes
Acknowledgements
The authors would like to place on record their appreciation of the support provided by the Dept. of Psychiatry, NIMHANS (Bengaluru), National Health Mission (Bengaluru), District Health Officer (Davangere), District Leprosy Officer (Davangere), District Mental Health Program (Davangere), Taluk Health Officer (Jagaluru) and all the health staff in Jagaluru taluk. The work would not have been possible without the support of Mr. Janardhana A L (Director of the District Disability Development Program, Association of People with Disability (APD), Mr. Santhosh S, senior coordinator—CMHP project Association of People with Disability (APD), Mr. Dundesh (Junior Research Fellow, community mental health project, Jagaluru) Mr Hanumanthappa (Field staff, Jagaluru), Chittasanjeevani Charitable Trust, ASHA workers and officials/ key community members/stakeholders in Jagaluru. We would also like to thank Dr S Kalyanasundaram (Hon ‘Advisor), Richmond Fellowship Society (RFS) Bengaluru, Dr Jagadisha Thirthalli (Professor, Dept. of Psychiatry, National Institute of Mental Health and Neurosciences (NIMHANS)), Bengaluru, Dr Sreekanth Thekkumkara, (Assistant Professor, School of Health Sciences, University of Dundee, Scotland) and Dr James JW (Assistant Professor, School of Social Science and Languages, Vellore Institute of Technology(VIT)) Revathi (Faculty in Ramaiah Institute of Nursing Education and Research) for their valuable feedback in amending the article.
Compliance with Ethical Standards
All authors certify that they were involved in the study, analysis, and preparing the article and have seen and approved the final article. We meet the definition of an author, as stated by the International Committee of Medical Journal Editors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Approval for this study was granted by the NIMHANS Institutional Ethics Committee (NIMH/DO/BEH. Sc. Div./2021-22).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.S. was supported by research grants from the Indian Council of Medical Research (File No. 5/4-4/151/M/2017/NCD-I dated 15/06/2018) and The Live Love Laugh Foundation. M.J. was funded by the Indian Council of Medical Research (File No. 5/4-4/ 151/M/2017/NCD-I dated 15/06/2018) for 6 months. The funding agency was not involved in the study’s design, data collection, data analysis or interpretation, or article writing.
Informed Consent
The authors certify that consent has been obtained from the patient and the family members to report the clinical information.
Statement on Concurrent Submissions
We declare that we have not submitted this paper to any other journals.