
Abstract
Background:
Persons with severe mental illness (SMI) reportedly have a high mortality rate due to metabolic syndrome (MS). However, lifestyle modification (LM) offers effective management of some components of MS. This study aimed to evaluate the effectiveness of LM in reducing body-weight-related parameters in SMIs.
Method:
Eighty participants with SMI were assigned randomly to either LM (n = 40) or treatment as usual (TAU; n = 40) groups using block randomization (eight blocks of n = 10). The LM group and their caregivers received a structured LM package that included nutrition counselling, recommendations on a balanced diet, and physical activity. The two groups were assessed on body weight, body mass index (BMI), waist circumference (WC), waist–hip ratio (WHR), and quality of life (QOL) at baseline and after three months. Thirty-one LM and 33 TAU participants completed the study.
Results:
The LM and TAU groups were comparable on sociodemographic and clinical characteristics and baseline variables of body weight, BMI, WC, and WHR (all P > 0.08). Repeated-measures analysis of variance (RM ANOVA) showed that the LM group had significantly reduced body weight, BMI, WC, and WHR (all P < 0.001) than the TAU group. Similarly, the LM group also showed improvement in their QOL (P < 0.001), whereas TAU showed no improvement.
Conclusions:
LM is an effective way to reduce body-weight-related parameters of MS and improves the QOL among persons with SMI in the short term. The caregivers’ inclusion during LM contributed to the weight reduction. However, the long-term effect of the intervention could not be assessed.
Keywords
Over three months, the lifestyle intervention group had significantly reduced body weight, body mass index, waist circumference, and waist–hip ratio than the treatment- as-usual group. The lifestyle intervention improved the quality of life also.Key Messages:
Compared to the general population, metabolic syndrome (MS) is two-to-three fold more prevalent in persons with severe mental illnesses (SMI), 1 reducing their life expectancy by 20 years and increasing the risk of premature death.2–4 Persons with SMI are reported to have a 32%–50% prevalence of MS.5–8 Among the components of MS, in SMIs, overweight/obesity is considered the most serious and is associated with several psychosocial complications like poor quality of life (QOL), poor psychosocial adaptation, poor treatment adherence, poor self-esteem, and an increased mortality rate.9, 10 Obesity/overweight also increases the probability of other metabolic complications like diabetes mellitus in SMIs. 11
MS in SMIs may be linked to biological risk factors such as endocrinal imbalance, insulin resistance, and genetic predisposition and psychosocial risk factors such as emotional disturbances, amotivation, poor social support, chronic familial or workplace conflicts, and chronic stressful life events. Other related factors could also be responsible for MS, such as a sedentary lifestyle, poor dietary intake, and side effects of psychotropic medications, especially second-generation antipsychotics. 6
Various lifestyle interventions reportedly appear to have a positive role in managing MS.11–13 Randomized controlled trials (RCTs)14–17 had reported that short-term lifestyle intervention, with the combination of a healthy diet, structured physical activity, and smoking cessation, combined with stress management, motivation counselling, psychoeducation, and behavioral or cognitive behavioral therapy resulted in a mean weight loss of 1.09–4.60 kg. However, the primary outcome measures included in the earlier studies were either body weight and body mass index (BMI) or body weight and waist circumference (WC).15, 17–19 The previous studies also had other limitations such as being carried out in in-patient settings and not incorporating patients’ caregivers, despite the fact that the patient has to practice the lifestyle modification (LM) components in their home environment and need assistance in the process. Furthermore, primary outcome measures such as body weight, BMI, WC, and waist–hip ratio (WHR) have not been evaluated together in the previous RCTs. Similarly, the previous studies did not include clinically stable participants on stable medications though it helps avoid possible confounds of medication on body weight and to make the groups comparable. To the best of our knowledge, no Indian studies have examined the effectiveness of psychosocial intervention in persons with SMI for MS. clinically stable, on medication for at least two months.
This study sought to improve upon some of the methodological shortcomings of earlier studies. Furthermore, given the high prevalence (45%) 20 of MS in SMIs in the Indian population and the lack of any literature on interventions, the present study investigated the effectiveness of short-term LM in persons with SMI for MS.
Materials and Methods
Study Design and Setting
An RCT was conducted using a block randomization method, where persons with SMI and their caregivers were randomized to LM or TAU groups using an online tool, Sealed Envelope. 21 A total of 80 participants (40 in each group) were randomized into eight blocks, and each block comprised ten participants (five in each group). The author VKS was responsible for the sequence generation and recruitment of the participants and was aware of the randomization sequence before recruitment. The participants were recruited from psychiatric outpatient department (OPD) services at National Institute of Mental Health and Neuro Sciences (NIMHANS), Bengaluru, Karnataka, India, and during the recruitment, all participants were informed about the randomization process. Participant recruitment began in April 2018 and ended in February 2019. However, the trial was completed in May 2019 after the completion of the follow-up visits. The two groups were assessed on body weight, BMI, WC, WHR, and QOL at baseline and three months.
Ethical Considerations
Approval was obtained from the Institute Ethics Committee, NIMHANS, Bengaluru. The participants and caregivers were recruited into the study after obtaining written informed consent. At the end of the study period, the participants of the TAU group also were offered the LM package.
Sample Size Calculation
We estimated a sample size of 80 patients based on RM ANOVA using G*Power 36 version 3.1.9.2. Expecting a medium effect size of 0.5 for the body weight loss with a level of significance at 5%, a power of 90%, by keeping the number of repeated measurements 2, and a nonsphericity correction of unity, the total sample size required was 46. Furthermore, anticipating an attrition of 30%, the total sample size required was 66 (33 per group). We rounded it off to 40 per group.
Inclusion and Exclusion Criteria
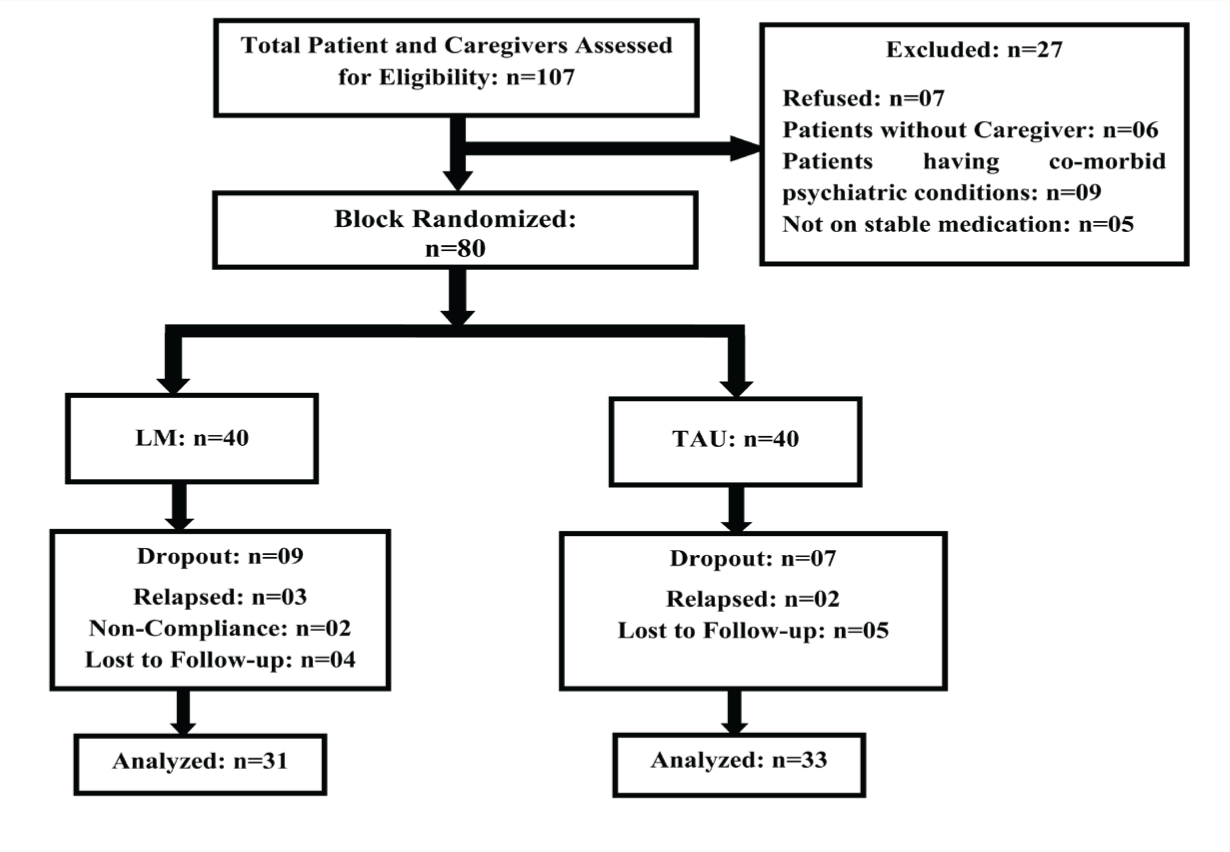
Participants with an SMI (schizophrenia, bipolar affective disorder, or major depressive disorder) as per ICD-10, 22 diagnosed by two clinicians independently, who had a BMI 23 > 25 kg/m2, who were aged 18–50 years, clinically stable, on medication for at least two months, and attending OPD along with their family caregivers (n = 80) were included. Exclusion criteria were presence of comorbid psychiatric illness except for nicotine dependence, requiring a change in medication during the intervention period, or experiencing symptomatic exacerbations after recruitment. The participant recruitment flowchart is shown in Figure 1.
Recruitment and Participation Flowchart.
Operational Definitions
Family Caregiver
Family caregiver refers to a member of the family who takes care (unpaid) of the emotional and physical health of persons with SMI having MS, within the family setting.
Body-Weight-Related Parameters
Body weight, BMI, WC, and WHR are considered body-weight-related parameters.
Lifestyle Modification Group (LM; n = 40)
The LM group participants included patients and their caregivers, and they received a structured LM intervention package in addition to the usual clinical care. The caregivers were included in the intervention sessions so that they can supervise the intervention components at home.
Treatment as Usual Group (TAU; n = 40)
The TAU group received pharmacological and psychosocial interventions and advice on LMs, along with referrals as appropriate, in an unstructured format, but did not receive any additional structured training or supervision like the LM group.
Lifestyle Modification Package
The LM package had components that included psychoeducation, motivational counselling, nutritional and physical activity counselling, and problem-solving skills. The face and content validation of the LM package was done by five experts: Two psychiatrists, a psychiatric social worker, one dietician, and one physical educator, whose suggestions were incorporated. The experts opined that the final LM package was comprehensive, simple to understand, organized systematically, covered adequate information, and served the study’s purpose.
The LM package consisted of eight sessions, delivered in four sittings over four weeks; one sitting included two sessions per week and between two sessions, there was a break of 15–30 min. The sessions were delivered one-to-one and included both patient and the caregiver. Further details of the LM package are provided as supplementary material (Table 1).
Outline of Lifestyle Modification Package.
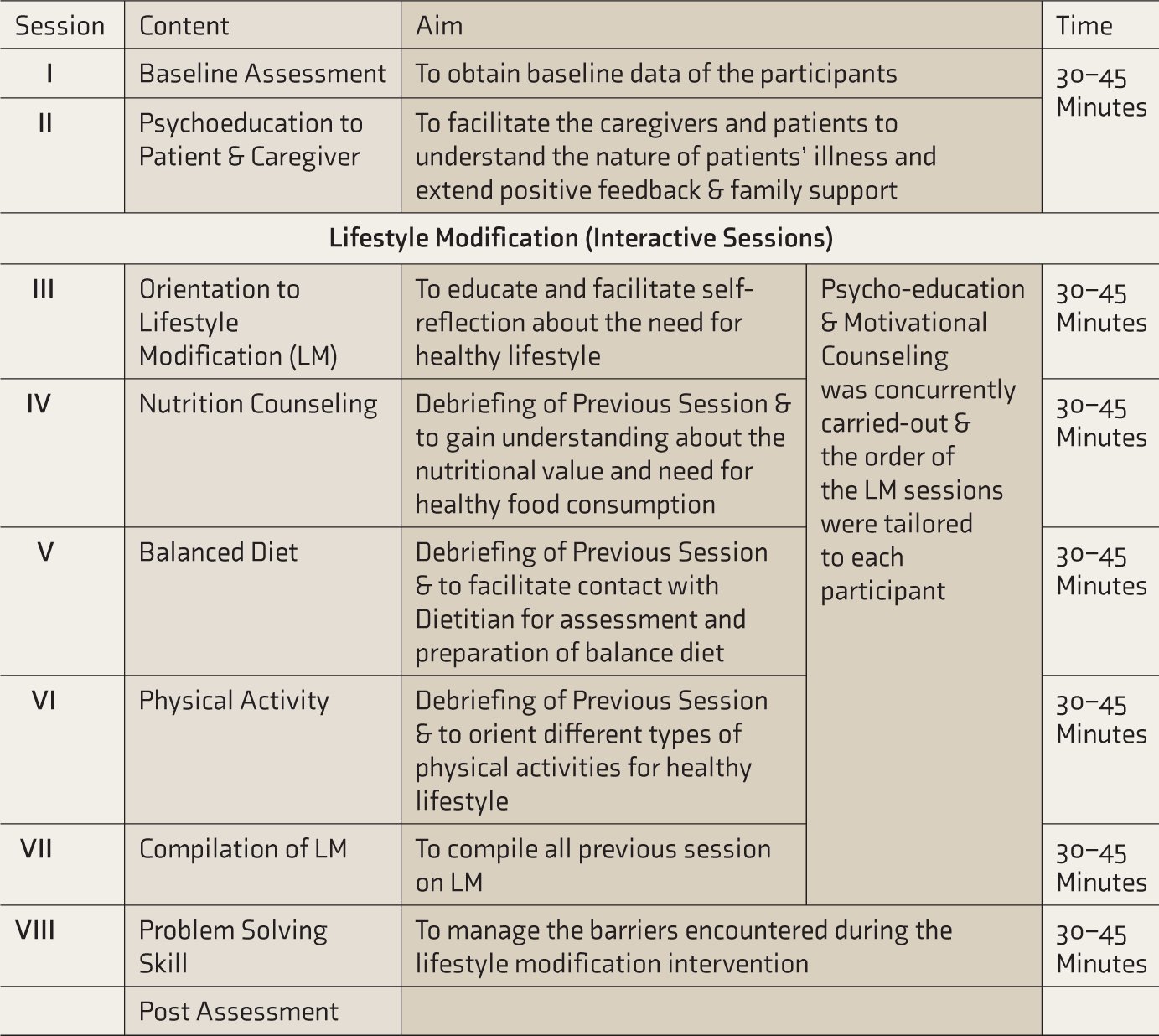
Physical activity should be performed in three stretches and each stretch should last for 10 minutes duration. 30 minutes per day (5 days in a week for 30 minutes) of moderate intensity physical exercise or do at least 15 minutes per day (5 days in a week for 15 minutes) of vigorous-intensity physical exercise or combination of both moderate and intense activity. The moderate intensity physical activity should be increased to 60 minutes per day (5 days in a week) or engage in 30 minutes of vigorous intensity physical activity per day (5 days in a week) or combination of both moderate and intense activity, for further health benefits.
Physical activities were tailored made to each individual as per their exercise capacity and health requirements.
We used a problem-solving session to manage the barriers encountered during the LM intervention, such as problems that arose while practicing physical activity, balance diet, maintaining motivation, and enhancing family support.
Further, to track the components of the intervention package, an “Activity Sheet” was developed and given to the caregivers at the first session of intervention. They were suggested to put a tick-mark for all the activities followed by the patient and a cross-mark for others.
Adherence with LM
In case of absence in the scheduled session, the patients and their caregivers were contacted over the phone and prompted for the session. The mean and the standard deviation (mean±SD) number of sessions attended was 6.95±2.01, and 72.5% (n = 29) of patients and their caregivers attended all eight sessions.
However, at the end of the last session, only 13 caregivers brought the activity sheet, as eight of them had lost it and ten could not either fill it completely or return it to the researchers, despite multiple reminders. Consequently, out of the 31 participants, only 13 could return the activity sheet. Hence, we were unable to compare between high and low adherence groups.
Measures and Assessments
A semistructured sociodemographic and clinical data sheet was used to collect details on the age, sex, education, occupation, and socio-economic status of the patients and the caregivers and the patient’s relationship with the caregiver. The clinical details of the patients collected were diagnosis, age at onset, duration of illness, number of episodes, and the number of hospitalizations.
Primary and Secondary Outcome Measures
Primary outcome measures included participants’ body weight, WC, WHR, and BMI. The secondary outcome measure was the QOL scale by the World Health Organization (WHOQoL-BREF). 24
Screening Tools
Screening tools were used to screen/rate the severity of the different psychopathologies. These were the Hamilton Depression Rating Scale (HAM-D), 25 the Young Mania Rating Scale, 26 the Scale for the Assessment of Positive Symptoms, 27 and the Scale for the Assessment of Negative Symptoms 27 as appropriate.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics was computed to describe the characteristics of the participants. The Shapiro–Wilk test was performed to check the distribution of the variables. Depending on the distribution, the baseline characteristics between the study groups were compared using independent samples t-test or Mann–Whitney U-test. The test of association between categorical variables was carried out using the chi-square test. The effectiveness of the intervention was evaluated by examining the time×group interaction effects for body weight, BMI, WC, and WHR, using RM ANOVA. The level of significance was fixed at 5%.
Results
Baseline Characteristics of Participants
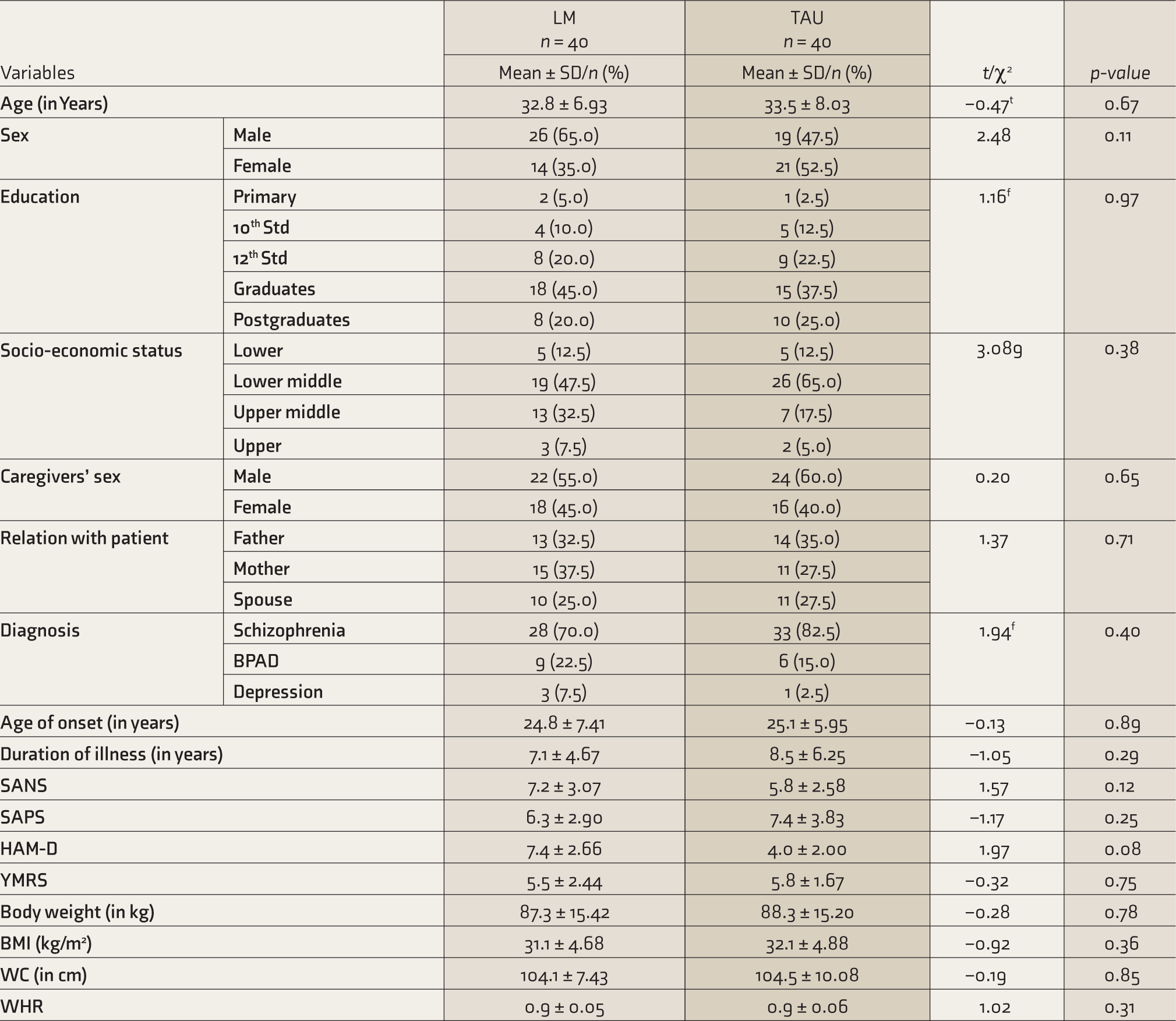
The mean±SD age of the LM group was 32.8±6.93 years and the TAU group was 33.5±8.03 years (t = –0.47; P = .6). The majority in both groups were male and graduates. There was no significant difference between the groups on sociodemographic variables (all P > .06). Mostly, the parents were the primary caregivers in both groups.
Most participants in both groups were diagnosed with schizophrenia (LM = 70%, TAU = 82.5%). The mean age of onset (LM: 24.8±7.41 years; TAU: 25.1±5.95 years) and duration of illness (LM: 7.1±4.67 years; TAU: 8.4±6.25 years) were not statistically significantly different (P > .29). Majority of the participants in both groups were not having any past history of medical illness (LM = 87.5%, TAU = 85%). The groups did not differ on any other measures, such as SANS, SAPS, YMRS, or HAM-D (for these measures total scores were taken to compute the mean; all P > .08).
The mean body weight (LM: 87.3±15. 42 kg; TAU: 88.2±15.20 kg), BMI (LM: 31.1±4.68 kg/m2; TAU: 32.1±4.88 kg/m2), WC (LM: 104.1±7.43 cm, TAU: 104.5±10.08 cm), and WHR (LM: 0.9±0.05; TAU: 0.9±0.06) were comparable at baseline (all P > .06; Table 2).
Baseline Characteristics of Participants.
Body-Weight-Related Parameters at Three Months
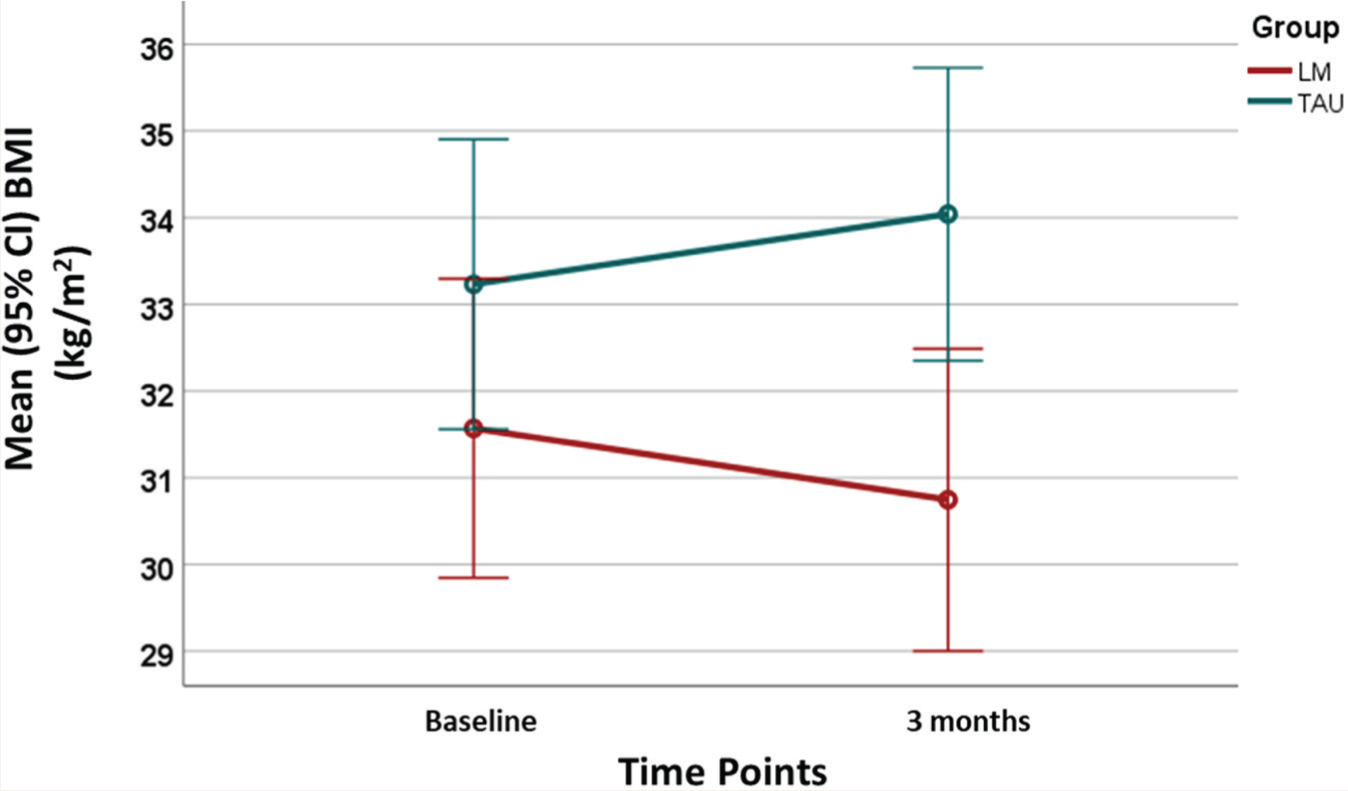
Time×group interaction effects from RM ANOVA showed that the two groups differed significantly at the treatment endpoint on body weight, BMI, WC, and WHR. Over three months, the LM group lost weight, whereas the TAU group gained weight (Table 3). In other words, difference in weight change over the time points was statistically significant between the study groups. The partial Eta-squared, η2partial, was used as the effect size in RM ANOVA. η2partial of time×group interaction-effects for all primary outcomes was >0.5; implying a large proportion of the total variance in the participants’ body weight, WC, WHR, and BMI measured at 3 months from the baseline were associated with the differences between the LM and TAU groups. The result for the BMI change was shown in Figure 2.
Comparison of Body Weight, BMI, WC, and WHR Between the LM and TAU Groups at Three Months Using RM ANOVA.
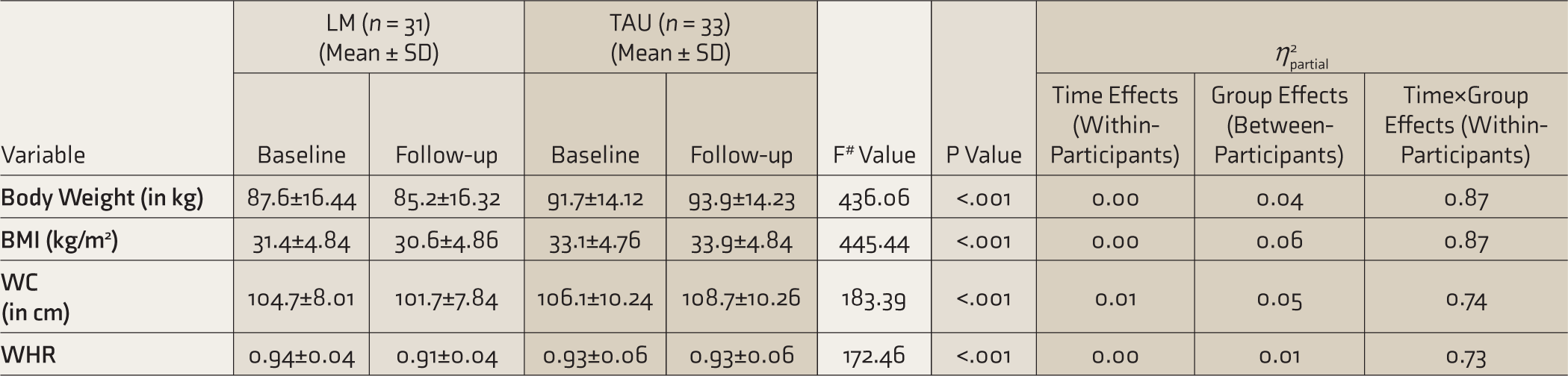
LM: lifestyle modification, TAU: treatment as usual, BMI: body mass index, WC: waist circumference, WHR: waist hip ratio. #Time×Group interaction effects from RM ANOVA: Wilks’ Lambda Multivariate Test. The partial Eta-squared, η2partial, was used as the effect size in RMANOVA. Time×Group is the interaction effect.
Mean (95% CI) of Body Mass Index at baseline and after three months of follow-up in LM (n=31) and TAU (n=33) groups.
Comparison of WHO QoL-BREF Scores at the Endpoint
At the end of three months, the LM group showed improvement in their QOL (higher the score, better the QOL) on all four domains of WHOQoL, whereas the scores of the TAU group remained unchanged. The groups differed significantly in all four domains of QOL (Table 4).
Comparison of WHOQoL-BREF Scores.
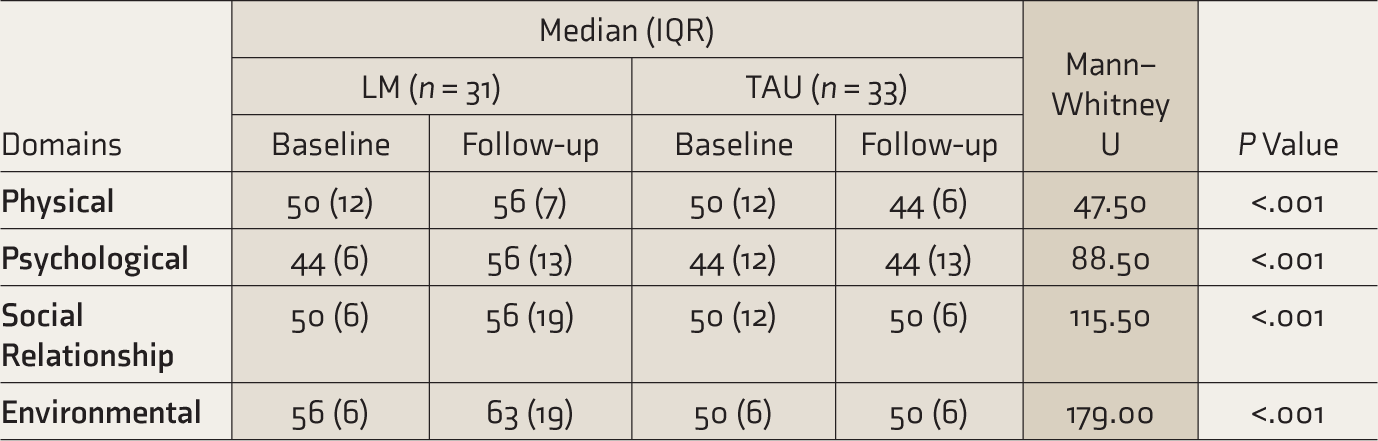
LM: lifestyle modification, TAU: treatment as usual, WHOQoL: World Health Organization quality of life. Interquartile range (IQR) = Q3 – Q1.
Discussion
Our main finding is that LM effectively reduces the body weight, BMI, WC, and WHR of patients of SMI with MS. The study also established that LM produces tangible results among an Indian sample of persons with SMI, even though participants of the LM group were on psychotropic medication during the intervention period. While continuing psychotropic medication might be the only choice, our findings highlight that LM is an important addition to usual clinical care for persons with SMI to manage weight-related parameters in their home environment.
The groups differed significantly in body weight, BMI, WC, and WHR after three months. The LM group lost an average of 2.35 kg of body weight, whereas the TAU group experienced an average 2.20 kg of weight gain. The LM group also experienced a reduction in BMI, WC, and WHR. The mean weight loss of 2.35 kg at the end of three months of intervention is consistent with the findings of previous studies.13, 15, 28–33 Those studies reported that psychoeducational lifestyle intervention is possible in persons with SMI and effectively reduces body weight/BMI (weight loss ranged 0.40 to 2.27 kg). A meta-analysis 34 included 19 studies on lifestyle/non-pharmacological weight management programs for persons with SMI for 2–18 months. Seven of the 19 studies included cognitive/behavioural therapy and 12 used psychoeducational interventions. The meta-analysis reported that irrespective of intervention duration (short or long), intervention type such as psychoeducational or cognitive/behavioral therapy, or treatment settings, lifestyle intervention was effective in reducing weight in the intervention group (−0.64, 95% CI −0.89, −0.39, Z = 5.03, overall effect P < .001) than in the TAU group.
The caregivers also were included in the study with the objective that they would supervise the components of the LM intervention at home. Caregivers’ participation during LM appears to have motivated the patients to follow the components of the intervention and led to a significant weight reduction, which is marginally higher than what is reported in the literature (–2.35 kg vs –2.27 kg).
The LM group showed improvement in all domains of QOL. The significant weight loss might have favorably affected the QOL of the LM group. In contrast, the QOL remained unchanged in the TAU group. An RCT 35 reported that physical exercise significantly impacted the overall QOL, functioning, fitness, and psychiatric symptoms of persons with SMI. Another study 36 compared the QOL and BMI in persons with schizophrenia and found poor QOL to be associated with excess BMI, which can be improved with proper weight management. Similarly, a few studies also reported that lifestyle intervention was not only effective in reducing body weight but also improved the QOL, general health, and psychological well-being of persons with SMI.28, 31, 33, 37–40 Our findings reflect those reported in such literature.
Our study has several strengths. To the best of our knowledge, this is the first Indian study to examine the effectiveness of psychosocial intervention in persons with SMI to reduce their weight-related parameters of MS. We included all indicators of overweight/obesity (body weight, BMI, WC, and WHR), which was not done in the previous studies. This is the first study to include caregivers of persons with SMI as cotherapist for supervision of LM in the home environment, and this probably resulted in a higher effectiveness of LM.
The limitations include lack of allocation concealment and that blinding could not be done for logistical reasons. Furthermore, the long-term effect of the intervention could not be assessed as the study period was limited to three months. To assess the long-term effect of the LM intervention, a considerably large study would be required. Besides, we did not record the medication details of either group, and medications can affect the parameters under study. We included clinically stable participants on stable medications; hence, our findings may not be generalizable to currently ill patients and those requiring a frequent change in medications. We did not investigate the impact of LM intervention on the blood/biochemical parameters. The TAU group received only usual care and did not receive the similar parallel intervention or contact with healthcare professionals like the LM group, hence, it will be interesting to investigate the same in future studies.
In conclusion, our study provides evidence that psychoeducational LM is significantly more effective than no structured intervention in persons with SMI for handling their body-weight-related parameters. The LM group lost significant weight and improved their QOL. The caregivers’ inclusion during LM appears to have motivated the patients to follow the components of the intervention and contributed to the weight reduction. Hence, the LM intervention may be an important addition to usual clinical care for persons with SMI to manage their weight-related parameters in the short term.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
This article is the part of PhD thesis which was supported by the University Grant Commission, New Delhi, India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
The study was registered with Clinical Trial Registry- India vide CTRI/2016/06/006994;(
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.