
Abstract
Psychotherapeutic developments in the management of anxiety disorders are evolving, with notable evidence in obsessive compulsive disorder (OCD). Third-wave therapies significantly contribute to the reduction in psychopathological symptoms and, thus, provide a positive turning point in the socio-occupational spectrum of the patient. One such third-wave approach is meta-cognitive therapy (MCT), which addresses cognitive attention syndrome (CAS) and directly prohibits ritualistic behavior, thereby decreasing the burden of symptoms. In India, it seems there is a dearth of literature exploring the effectiveness of MCT. The present case report provides a detailed insight into the psychotherapeutic treatment using MCT, in which 10 sessions were provided to an OCD patient along with pharmacotherapy. The treatment shows a noteworthy improvement in thought fusion, obsessional beliefs, meta-cognitive beliefs, and psychopathology. The symptoms gradually waned during the three- and six-month follow-up baseline period. Therefore, the case report demonstrates the effectiveness of combined medication and MCT in treating OCD. Additionally, it shows the potency of MCT in prolonged improvements in cognitive flexibility and inflated feelings of responsibility and perfection.
Obsessive compulsive disorder (OCD) is characterized by obsessive thoughts, compulsive behavior, or a combination of these. Obsessive thoughts are persistent, repeating, and distressing ideas that are often nonsensical and illogical. Contrastingly, compulsive behaviors entail ritualistic behavior intended to reduce anxiety triggered by obsessive thoughts. According to estimates, OCD affects 2% of people throughout their lifetime, 1 and exposure response prevention (ERP) is the conventional psychotherapeutic treatment used to manage the symptoms. Given the significant attrition rates of clients treated using ERP, an alternate or complementary treatment approach seems necessary.
Nonetheless, recent advancements in third-wave therapies, like meta-cognitive therapy (MCT), have enhanced the understanding of the mechanisms underlying emotional regulation in OCD. A meta-analytic review reveals that MCT shows statistically significant improvement in symptoms when compared to the controls 2 in disorders such as OCD, post-traumatic stress disorder (PTSD), and generalized anxiety disorder (GAD). These improvements were significant immediately post-treatment and after 12 months of post-therapy results. The trans-diagnostic meta-cognitive paradigm postulates that cognitive attentional syndrome (CAS), a perseverative thinking style, is linked to the maintenance of psychopathology. 3 A line of questioning, also known as meta-level Socratic dialog, helps in understanding the process of worrying rather than challenging the content of cognitions laid out in formulation. Therefore, the present case attempts to demonstrate the value of meta-Socratic dialogues and strengthen the validity of MCT in the management of OCD.
The Case
Mr. S, a 23-year-old male diagnosed with OCD, displayed a range of symptoms, including ritual recurrences such as rereading, rewriting, fear of specific numbers, fear of buying products from particular brands, fear of sending inappropriate messages on WhatsApp, and fear of seeing, hearing, or reading about people who had suffered acid attacks. These symptoms have been present for the past four years. Throughout the illness, the nature and severity of the symptoms changed. Mr. S was initially prescribed 100 mg of fluoxetine and 50 mg of clomipramine in combination in the OPD of the psychiatry department of King George’s Medical University, Lucknow, for about two months, but no improvement was reported. Consequently, no objective measures were administered at that point.
S had challenges in other spheres of his life. He could not concentrate on his college academics. He became anxious, and his constant preoccupation with thoughts was bothering him. The symptoms further disrupted his daily routine, which made him avoid socializing with friends and family and studying. The patient stopped practicing numerical and logical reasoning because he feared seeing specific numbers, which increased his vulnerability. He eventually left the coaching center and began studying on his own.
Additionally, he refrained from using his phone for fear that he might send inappropriate messages to people. As a result, S became quite agitated and helpless. In addition, S’s feelings of loneliness and depression worsened as his thoughts became more intense, and he was unable to cope at home. Also, he felt excessive discomfort thinking about the pictures of people who had survived acid attacks. He said he found it quite uncomfortable when he saw those images on media. Overall, he was constantly threatened by these thoughts, believing that one day, his family may experience something similar.
It was suggested that he seek both medication and psychotherapy when he visited the outpatient department for consultation. The therapist obtained a thorough case history and performed a mental status evaluation, which suggested no history of any past psychiatric illness of himself or in his family, although the premorbid personality was suggestive of anxiety and overthinking.
Mr. S received an explanation of the meta-cognitive therapeutic framework. It was stated that the goal of this therapy was to eliminate rituals and activate the meta-mode, which aids in recognizing the beliefs around inner experiences, primarily thoughts and feelings. S chose MCT as his treatment modality because he preferred to critically examine his responses to intruding thoughts as opposed to using the unhealthy coping mechanisms of thought suppression or covert neutralization. The Yale–Brown Obsessive Compulsive Scale (YBOCS), 4 the Meta-cognitive Questionnaire (MCQ30), 5 the Obsessional Belief Questionnaire (OBQ-44), 6 and the Thought Fusion Instrument (TFI) 7 were used to conduct a baseline assessment before the intervention. After the intervention, a second assessment was conducted using two distinct baselines for the three- and six-month follow-up periods.
Meta-cognitive Model/ Therapeutic Model
Intervention
The model and techniques of MCT were delivered to the patient in 10 sessions (Figure 1). Each session was conducted every week and lasted for about 1 hour. The standardized treatment of OCD with MCT is broadly done in four phases as follows: case conceptualizing and identifying meta-cognitive beliefs, modifying meta-cognitive beliefs about obsessive thoughts, modifying meta-cognitive beliefs about ritual behaviors, and relapse prevention. These phases are elaborated in the session details.
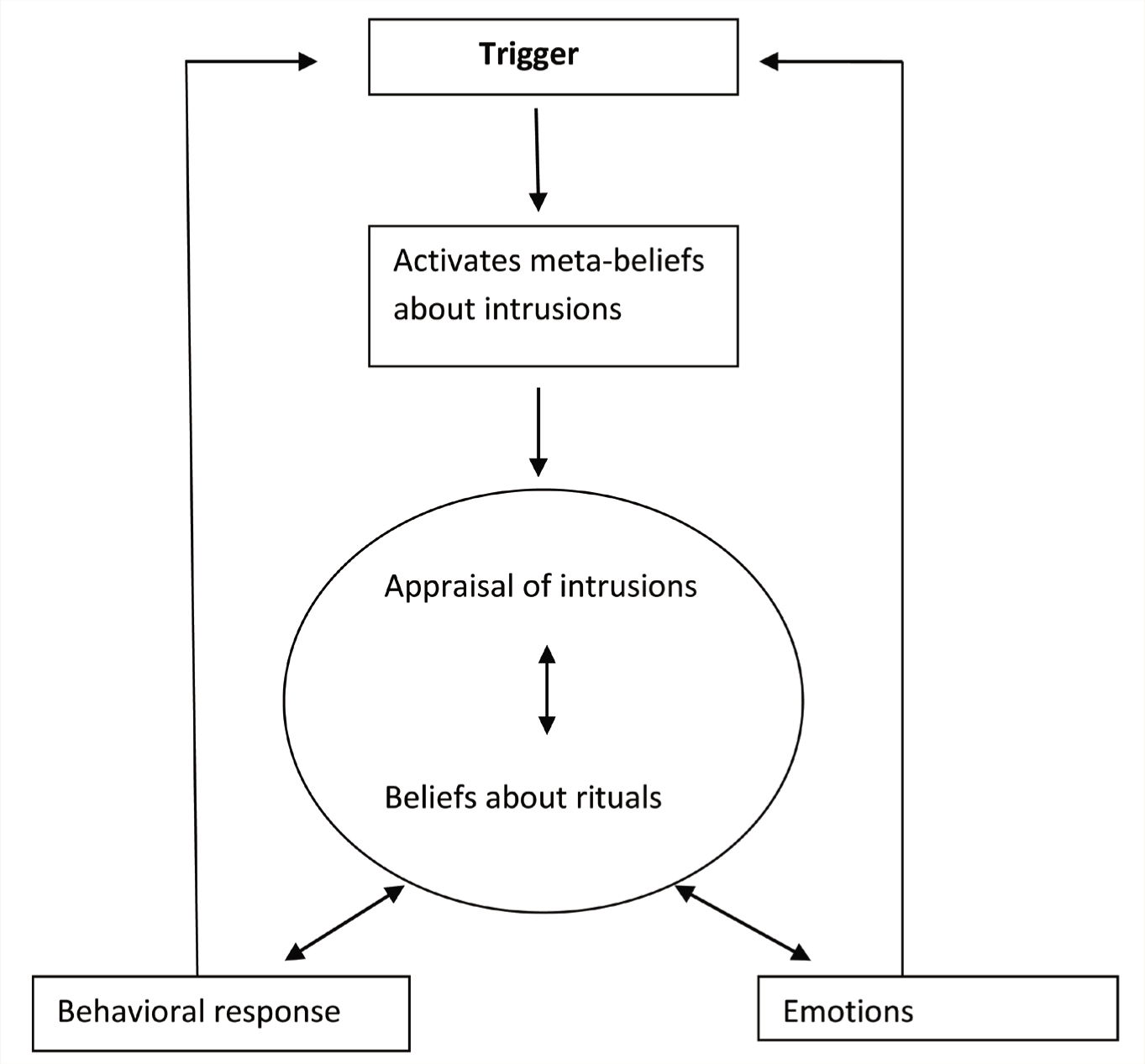
Wells (1997)
The blueprint of the therapy process was discussed with the patient. Closing each session was accompanied by homework, and before beginning the next session, a brief overview of the last session and the obstacles experienced in any work assignments were addressed. This was consistent throughout the 10 sessions.
The patient explained the meta-cognitive model during the first session, which involved the case formulation. This allowed him to identify the meta-cognitive elements that were sustaining his OCD symptoms, and it could be achieved by invoking recent occurrences of obsessional thought, urge, or neutralization. Further, the therapist enquired about the patient’s associated emotion with the trigger, generating an assessment and belief regarding the ritual. Next, the type of behavioral responses and the client’s perceptions of the necessity of talking with them were addressed. During this session, the patient was also introduced to the “Tiger Task,” a detached mindfulness method that provides an alternate perspective to obsessing thoughts. As with any neutral activity, it assisted the patient in observing the idea. During the task, the patient was instructed to visualize a tiger and hold the image in his mind without allowing it to move or engage in any activity. The patient gained insight into the tiger’s unique behavior and ability to be detached and neutral through the tiger task. This helped the patient get insight into all those intruding thoughts. Applying the detached mindfulness approach to the intrusions was given as the session’s homework.
A quick recap of the first session was accompanied by feedback on the homework task in the second session. Primarily, the session introduced the socialization paradigm and an additional detached mindfulness practice. The “Passenger Train Metaphor” method was described to the patient. Using this technique, the patient was asked to picture himself as a passenger on a railway platform through which many trains keep passing. He was asked to imagine his thoughts and feelings as passing trains, which he does not have to board but should stay on the right track. He was asked to ignore these thoughts and feelings as irrelevant trains as they passed through a busy station in his mind.
Further in the session, the patient was explained exposure response commission (ERC) or ritual postponement. In this experiment, the patient can carry out the routines, but only as long as they are conscious of their obsessive thoughts. This action facilitates detachment from the thought and strengthens the meta-level experience of the incursion. The homework for this session was to practice ERC.
Next, the emphasis shifted to verbal challenging of thought event fusion (TEF), thought action fusion (TAF), and thought object fusion (TOF) starting in the third session and continuing till the sixth session. This covers the standard methods of challenging their evidence, obtaining the mechanism behind fusion effects, and looking for contradictory data. Dissonance, which arises from the patient’s general self-beliefs and meta-cognitive beliefs, further helps achieve this. This method demonstrates how the patient’s beliefs about his obsessions conflict with his self-awareness. The fusions of mental events were handled in the present and the past. The patient’s perception was combined with the event in the future because he believed that “if he sees the image of acid attack survivors, someone in the family shall be harmed, or some bad news may break.” Thus, the concept of leveraging the power of the mind to create favorable outcomes was presented to him. He was encouraged to try winning the lottery by just imagining it happening; there was another negative domain, where he was asked to try and imagine smashing the therapist’s table. The patient’s homework was to practice detached awareness, conducting particular behavioral tests, and giving up routines.
Moving further, in the seventh and the eighth sessions, exposure tests involving TEF, TAF, and TOF were conducted in addition to changing participants’ views regarding the rituals. This was accomplished by applying Socratic questioning to the evidence supporting ritual beliefs. An approach to increase awareness of the disturbances produced by these behaviors involved reviewing the benefits and drawbacks of rituals. In order to encourage change, the therapist sought to dispute the veracity of the benefits and to reaffirm awareness of various drawbacks. Overall, the session’s goal was to reframe the benefits of rituals in a way that calls into question the veracity of the acknowledged benefits. The session also focuses on innovative strategies for handling stop signals and knowledge requirements. In this case, the therapist worked with scripting a new set of techniques that included selecting suitable criteria for determining whether the incident had occurred, forbidding memory checks, and practicing detached mindfulness in response to uncertainties or intrusions. The redesigned strategy was also designed to address OCD symptoms. This further prohibited the maladaptive checking methods by focusing more on “seeing that” than “feeling that,” asking whether he delivered the appropriate message to the proper person on WhatsApp or other social media apps.
Finally, the last two sessions focused on relapse prevention and future therapy plans. This consists of a case formulation and blueprint entailing meta-cognitive beliefs and intrusions, along with evidence traced through verbal and behavioral methods. The sessions majorly focus on the disadvantages of ritual performance and a detailed plan for relapse prevention.
Overcoming Obstacles in Intervention
The patient was introduced to MCT, where he was explained how the case was put together, as well as how assessments and fusions contribute to the persistence of the threat and OCD symptoms. The critical challenge was switching from the “object” to the “meta” mode. This was addressed through detached mindfulness; the “do-nothing” approach, which is the opposite of coping; and CAS. It was discovered that the “recalcitrant child metaphor” strategy was effective. The patient was instructed to approach his ideas similarly to a misbehaving kid. Since a child’s attention-seeking behavior will increase in proportion to the attention provided to his maladaptive conduct, observing the youngster passively, without intervening, rather than actively interacting with them is preferable. It was reported that the pessimistic ideas and attitudes resemble the misbehaving child and that such behavior will continue if given attention, an attempt to exert control over them, or reprimanded. Therefore, watching everything as an observer is preferable to attempting to interact or exert control actively. This practice also aided in delaying worry and performing ritualistic actions. The detached mindfulness exercises had a vital role in the meta-model’s activation, and they also assisted the patient in becoming meta-aware of those thoughts.
After a few sessions, the patient became accustomed to using the meta-cognitive model. He discovered how to separate himself from the mental process, which enhanced his meta-level experience of the incursion rather than concentrating on the ritual.
Outcome
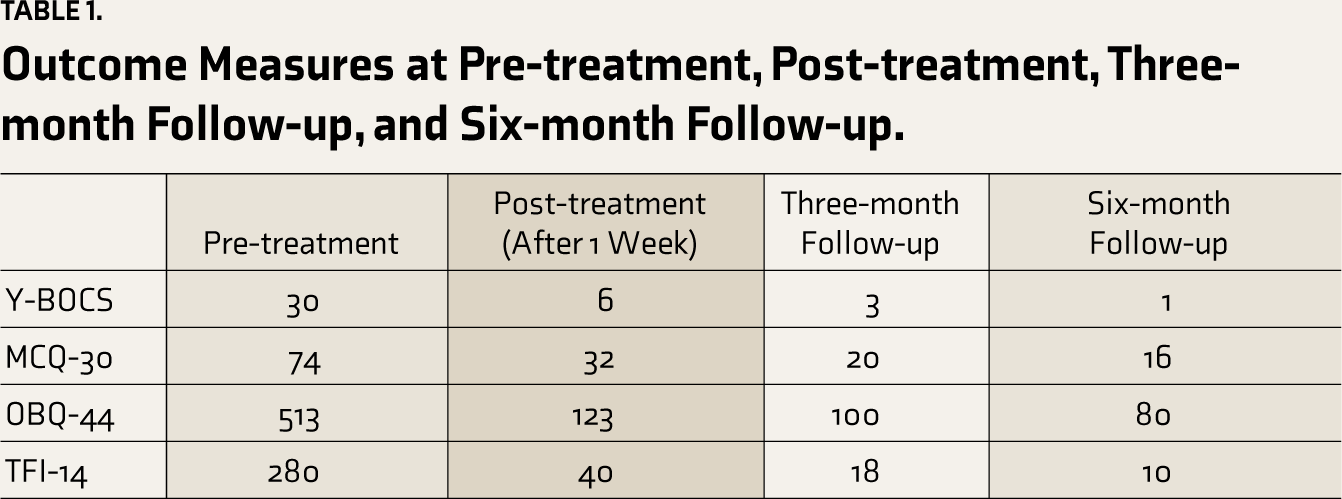
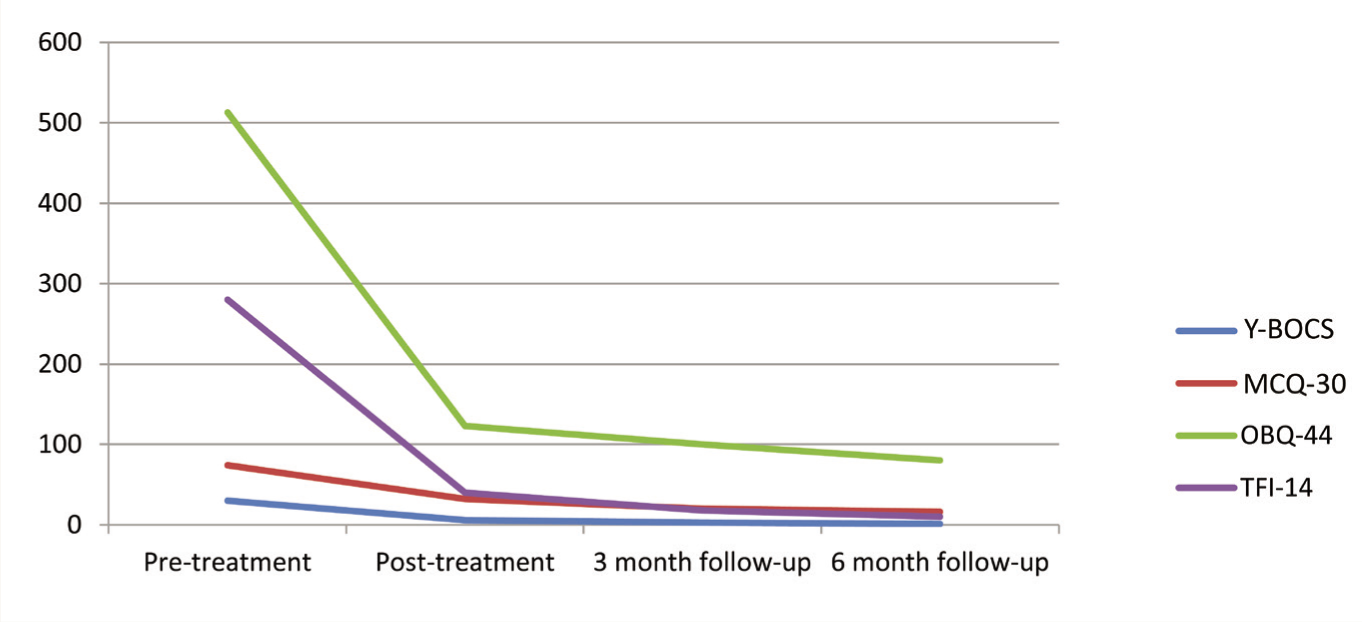
After completing the 10 sessions, the patient was reassessed on Y-BOCS, MCQ-30, OBQ-44, and TFI-14 after one week. The assessment was repeated at three and six months of follow-up period. The outcome measures are represented in Table 1 and Figure 2.
Outcome Measures at Pre-treatment, Post-treatment, Three-month Follow-up, and Six-month Follow-up.
Outcome Measures at Pre-treatment, Post-treatment, Three-month Follow-up, and Six-month Follow-up.
Discussion
The case study sheds light on the effectiveness of MCT in treating OCD. There is a scarcity of Indian studies assessing MCT as a psychotherapeutic treatment for OCD. Hence, this case study aims to comprehend the function of MCT as an alternative to conventional interventions such as CBT and ERP. The meta-model for treating obsessions has forced the patient to consider the idea without explicit understanding or information. The MCT focuses on two kinds of meta-cognitive changes: first, the patient’s relationship to and experience with thoughts and, second, their beliefs about thoughts. Overall, the treatment has profound implications; it is directed toward the methods that enable patients to form fresh connections with their ideas and convictions. Since dysfunctional meta-cognitions are associated with maladaptive thought patterns, which are difficult to control and are repetitively negative, instead of contesting the veracity of ideas and opinions as in contrast to traditional CBT, the therapist assists in modifying the meta-cognitions in MCT. Through the findings of the present work, additional support is generated for MCT. These findings suggest that MCT is aimed at something other than habituation or reality testing. Instead, it focuses on behavioral experiments that modify the meta-cognitive beliefs through ERC or ritual postponement, which is a new learning through this treatment modality. Also, the outcome of the report helps in understanding the beliefs about the rituals that exist as discrete knowledge packets apart from beliefs regarding compulsive thoughts and emotions. The strategies discussed in this case report contribute to the understanding of the clinician about how the reaction toward obsessive thoughts is modified without engaging in the active performance of compulsive behaviors.
Improvement has been effectively observed using behavioral tests and strategies such as ERC, adaptive checking, detached mindfulness, meta-Socratic inquiry, and ritual performance. Furthermore, about 30% of OCD patients avoid ERP or stop receiving treatment. 8 For this reason, MCT may work as a therapeutic strategy for this group of patients. 9
In the current case report, the patient was eventually classified as asymptomatic on the Y-BOCS, the most stringent criterion for defining recovery. 10 In the post-treatment, the score on Y-BOCS met the criteria for reliable change as it was below the cutoff score of 7, which indicates an absence of OCD symptoms. 11 The other outcome measures also showed a notable reduction, claiming that the intervention has served its purpose. Of the few studies conducted in India, 12 none could study the follow-up beyond three months. This study has attempted multiple follow-up periods of three and six months to understand the symptom maintenance and progress. The treatment appeared well tolerated by the patient, and it has the advantage of using only brief exposure, which may be easier to implement. 13
Conclusion
The study highlights the role of MCT and pharmacotherapy in OCD. However, only a handful of studies have been done using this therapy. Nevertheless, the therapy has also provided an alternative to ERP, which is considered the conventional treatment, although it has high attrition rates. Empirical evidence from randomized controlled trials will further help understand the study’s clinical significance among patients.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The ethical approval was taken from the Institutional Ethics Committee of King George’s Medical Un iversity vide no 1194/Psy/23 with Ref code: 124th ECMIIB-PhD/P2.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors certify that the patient has given their consent to have the relevant clinical information reported in the journal.