
Abstract
Background:
Early psychiatrists inferred that obsessive-compulsive symptoms (OCS) represent a defense against psychosis and prevent the progression of schizophrenia. However, recent clinical research has yielded inconsistent results across studies regarding the link between OCS and the symptom domains of schizophrenia and the influence OCS have on a patient’s functioning and quality of life (QOL).
This study aimed to determine whether OCS has any association with the symptom severity, functioning, and QOL of schizophrenia patients.
Methods:
This cross-sectional study done in a tertiary care hospital consecutively recruited 85 outpatients of schizophrenia in clinical remission over one year. Positive and Negative Syndrome Scale (PANSS), Yale-Brown Obsessive Compulsive Scale (Y-BOCS), WHO Quality of Life Brief Version (WHO QOL-BREF), and Global Assessment of Functioning (GAF) scales were applied.
Results:
Eighteen patients (21.2%) had OCS (Y-BOCS score of ≥8). Patients with OCS had higher PANSS scores (mean±SD of total score 77.16± 16.4, P < 0.001), suggestive of more severe psychosis, poor functioning overall (mean GAF score 37.35 ± 15.62, P < 0.001), and poor QOL in the psychological domain (P < 0.001). In addition, significant associations were present between the Y-BOCS score and the PANSS (r = 0.65), GAF (r = –0.61), and WHO QOL BREF scores in the physical (r = –0.39), and psychological domains (r = –0.41) (P < 0.001 on all of the above).
Conclusions:
Patients with OCS have more severe symptoms and a lower QOL. A significant association exists between the intensity of OCS and schizophrenia symptoms, global functioning, and QOL.
The greater severity of psychosis in schizophrenia patients with obsessive-compulsive symptoms aligns with most reports that project a clinical picture of poorer social functioning and prognosis for these patients. This is contrary to earlier reports which suggested that such patients have a better prognosis, thus emphasizing on the need for longitudinal studies, which could help in formulating targeted interventions for this population.Key Messages:
Obsessive-compulsive symptoms (OCS) have been reported in schizophrenia for more than a century. Bleuler characterized OCS in schizophrenia as “automatisms,” i.e., “action, thinking, and feeling detached from the will.”1,2 In the last few decades, their incidence has been increasingly reported in schizophrenia, with a recent meta-analysis reporting a prevalence rate of 30.3%. 3 Moreover, the prevalence rates of OCS in schizophrenia are much higher than the lifetime prevalence rate of 1.3% in the general population. 4 In comparison, in India, the prevalence rates of OCS in schizophrenia are 10%–28% as opposed to the lifetime prevalence rate of 0.6%–3.3% in the general population.5–10 Further, in schizophrenia, the prevalence of OCS is higher in outpatients than inpatients, indicating that OCS is more easily detectable after the remission of psychosis. 11
Early psychiatrists inferred that OCS could also retard the development of “malignant schizophrenia” and may represent a defense against psychosis and prevent the progression of schizophrenia. 12 However, recent clinical research has shown that patients of schizophrenia with OCS frequently have severe psychotic and depressive symptoms and, consequently, lower social functioning. 1 Regarding the quality of life (QOL) and disability, a few studies have suggested more significant social impairment, poor overall performance in neuropsychological tests, and poor QOL.13–15 However, some studies have reported better global functioning in such patients. 16
In the Indian context, so far, studies have been mixed. For example, Devi et al. found that schizophrenia patients with OCS had lower positive symptom scores and better QOL. 6 Singh et al. found the OCS group to have significantly higher general psychopathology and total score on the Positive and Negative Syndrome Scale (PANSS), with a significant positive correlation between total Yale-Brown Obsessive Compulsive Scale (YBOCS) scores and PANSS positive subscale scores suggestive of more severe psychopathology. 7 Rajkumar et al. discovered that schizo-obsessive individuals were likelier to have paranoid symptoms, first-rank symptoms, and a lower level of disability. 17
While several studies have characterized the prevalence and clinical correlates of OCS in schizophrenia, they have yielded inconsistent results, leaving many questions unanswered, such as:
What is the link between OCS and the symptom domains of schizophrenia? What influence do OCS have on a patient’s overall functioning and QOL?
Given the knowledge gaps, this study aimed to determine whether OCS affects the symptom severity, functioning, and QOL of schizophrenia patients. Also, we aimed to determine which domains of schizophrenia were most strongly influenced by the presence of comorbid OCS. Our hypothesis was that symptom severity and QOL are worse in patients with schizophrenia with clinically significant OCS than those without it. We also postulated that patients with severe OCS are likelier to have more severe psychosis than those without.
Materials and Methods
Sample
For this study, the patients were recruited from the outpatient department of Government Hospital for Mental Care, Visakhapatnam. All patients diagnosed with schizophrenia (as per ICD-10 DCR criteria) at least six months ago and were in clinical remission at the time of this study, aged 18 to 60, and willing to give informed consent, were included. Patients with schizoaffective disorder, comorbid affective disorders, substance use, intellectual disability, or organic brain disorders such as epilepsy were excluded. Using the prevalence rate of schizo-obsessive disorder of 30% from the review by Montcel et al., 1 with an error rate of 10%, we estimated the minimum sample size to be 81. Accounting for anticipated nonconsent and dropouts during the study (presumed at 20%), the final sample size was 97.
Study Design
This cross-sectional, hospital-based study recruited patients consecutively over a year, starting in September 2020.
Operational Definitions
For identifying obsessions and compulsions in the presence of psychotic symptoms, guidelines by Bottas et al. were utilized:
A repetitive act was considered a compulsion only if it occurred in response to an obsession AND not in response to psychotic ideation (e.g., repetitive checking in response to paranoid fears would not constitute a compulsion). If a recurring, intrusive thought revolved solely around delusional concepts, it was not termed an obsession (e.g., persecutory or referential ideas).
12
Following the method chosen by Nasrollahi et al. in their clinically relevant OCS diagnosis study, patients with a score of >7 on the Y-BOCS were labeled as having OCS. 18
To determine clinical remission, we used the Andreasen criteria, according to which patients had to score ≤3 on PANSS items P1, P2, P3, N1, N4, N6, G5, and G9. In addition, the symptoms were rated based on the patient’s history from six months before recruitment. 19
Study Tools
A self-designed semi-structured questionnaire was used to collect personal and sociodemographic details.
Methods
The Andhra Medical College Institutional Ethics Committee, Visakhapatnam, approved the study. Demographic data, illness, and treatment variables were collected, and PANSS, Y-BOCS, WHO QOL-BREF, and GAF scales were, applied. Those with a Y-BOCS score of >7 were put in the “OCS group,” while the others comprised the non-OCS group.
By the end of the study, 12 patients were excluded due to withdrawal of consent during the study, presence of comorbidities, etc. Eighty-five patients were finally included. All the assessments were performed by the principal author, who was trained in administering the instruments by the senior consultant.
Statistical Analysis
Statistical Package for the Social Sciences, Windows version 25 (SPSS-25), was used to analyze the data. Data distribution was determined, and the Kurtosis range of ±2 was considered in the parametric range. The mean, standard deviation, and median were calculated for continuous variables. Frequencies and percentages were used to analyze categorical variables. Comparison of socio-demographic and clinical characteristics was done using the chi-square test. Comparisons of means were made by using the Mann-Whitney U test. Correlations were evaluated using Pearson’s correlation coefficient before and after controlling for PANSS scores, and Spearman Rank Test was used to correlate Y-BOCS scores with each item of PANSS. All the tests were two-tailed, and significance was set at a conservative P value of ≤0.001 after Bonferroni correction for 50 correlation comparisons for subgroup analysis.
Results
Sample Characteristics
Out of the 85 patients, 67 belonged to the non-OCS group and 18 to the OCS group (Y-BOCS>7). Twelve patients out of 85 scored >16 on the Y-BOCS scale (14.12%), indicative of significant OCD. The mean (SD) of YBOCS total, obsessions, and compulsions scores were 21.83 (7.54), 11.39 (3.8), and 10.44 (4.17), respectively. The most common compulsions were cleaning type (72.2%, n = 13) and miscellaneous type (need to tell, ask, or confess; need to touch, tap, or rub, 27.8%, n = 5). The most common obsessions were of contamination type 72.2% (n = 13), followed by sexual (38.8%, n = 7) and religious (22.2%, n = 4) types.
In 27.8% (n = 5) of the OCS group, OCS preceded the onset of schizophrenia symptoms, while eight (44.4%) patients developed OCS during the chronic course of schizophrenia. In three patients OCS was apparently drug induced, with one patient being on clozapine and the remaining on olanzapine.
Table 1 compares some sociodemographic and clinical variables of both groups.
Comparison of Clinical Characteristics of OCS and Non-OCS Groups.
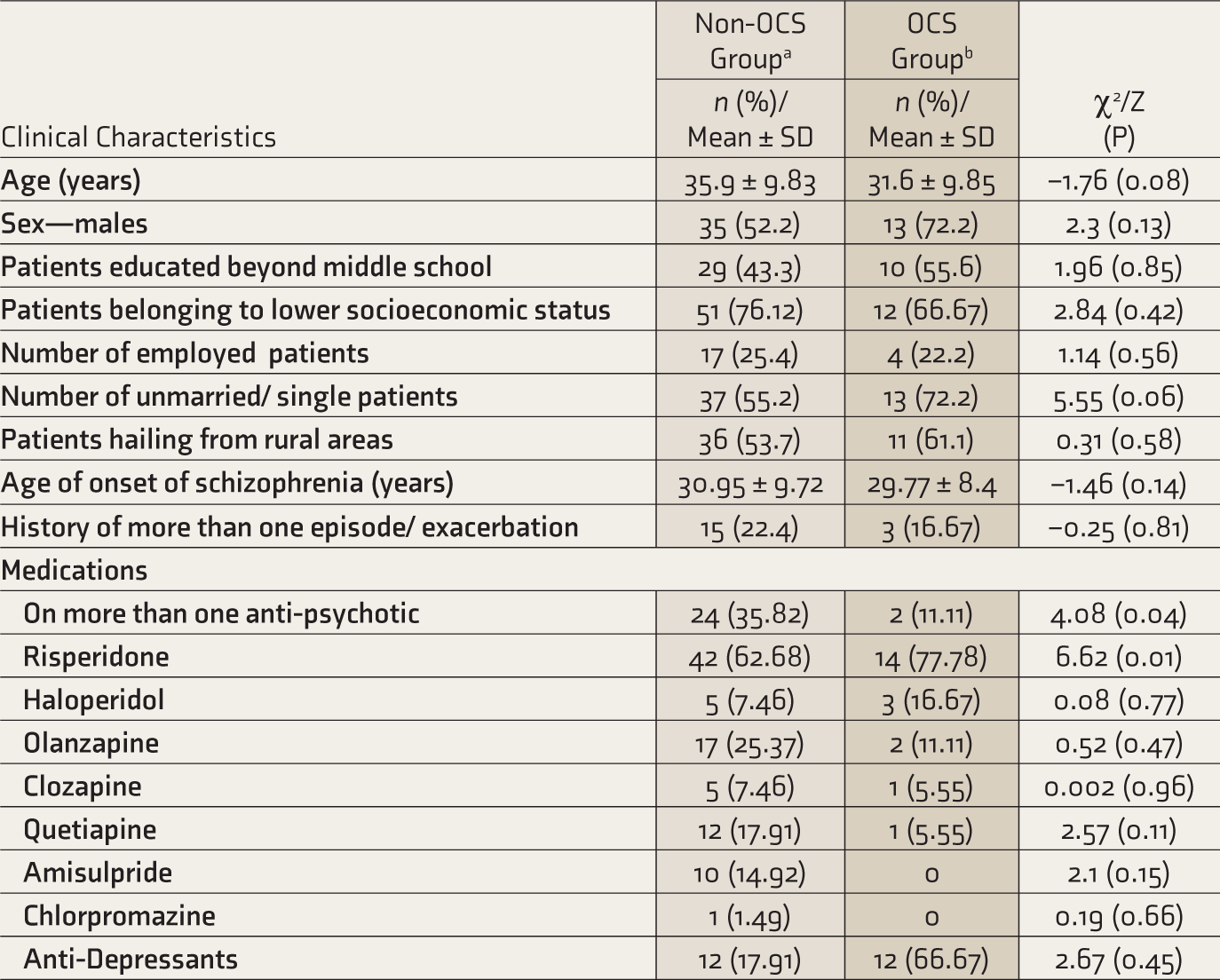
aSchizophrenia patients without obsessive-compulsive symptoms. bShizophrenia patients with obsessive-compulsive symptoms.
OCS: Obsessive-compulsive symptoms.
Most patients who reported OCS were male, unemployed, and unmarried at the time of the survey. There were no statistically significant differences between the groups based on sociodemographic or clinical characteristics. The most prescribed antipsychotic was risperidone in the whole sample, Olanzapine in the non-OCS group, and haloperidol in the OCS group.
Comparing Symptom Severity, Functioning, and QOL
Overall, the OCS group had a more severe illness, with higher scores on all three dimensions and the total scores of PANSS. The severity was significantly higher in the OCS group in four out of seven symptoms on the positive scale, i.e., delusion, conceptual disorganization, suspiciousness (P < 0.001 for all), and hallucinatory behavior P = 0.001), and three out of seven symptoms on the negative scale, i.e., emotional withdrawal, poor rapport, and stereotyped thinking (P < 0.001 for all). In general psychopathology, 12 out of 16 parameters, particularly symptoms like anxiety and guilt, were significantly more severe in the OCS group (P < 0.001). Comparing the symptom severity and overall functioning, patients with OCS had significantly lower scores on the GAF scale. On the WHO QOL BREF scale, OCS patients fared poorly only in the psychological domain (P = 0.001,
Comparison of Scores on PANSS and Its Subdomains, GAF, and WHO QOL BREF in Non-OCS and OCS Groups.
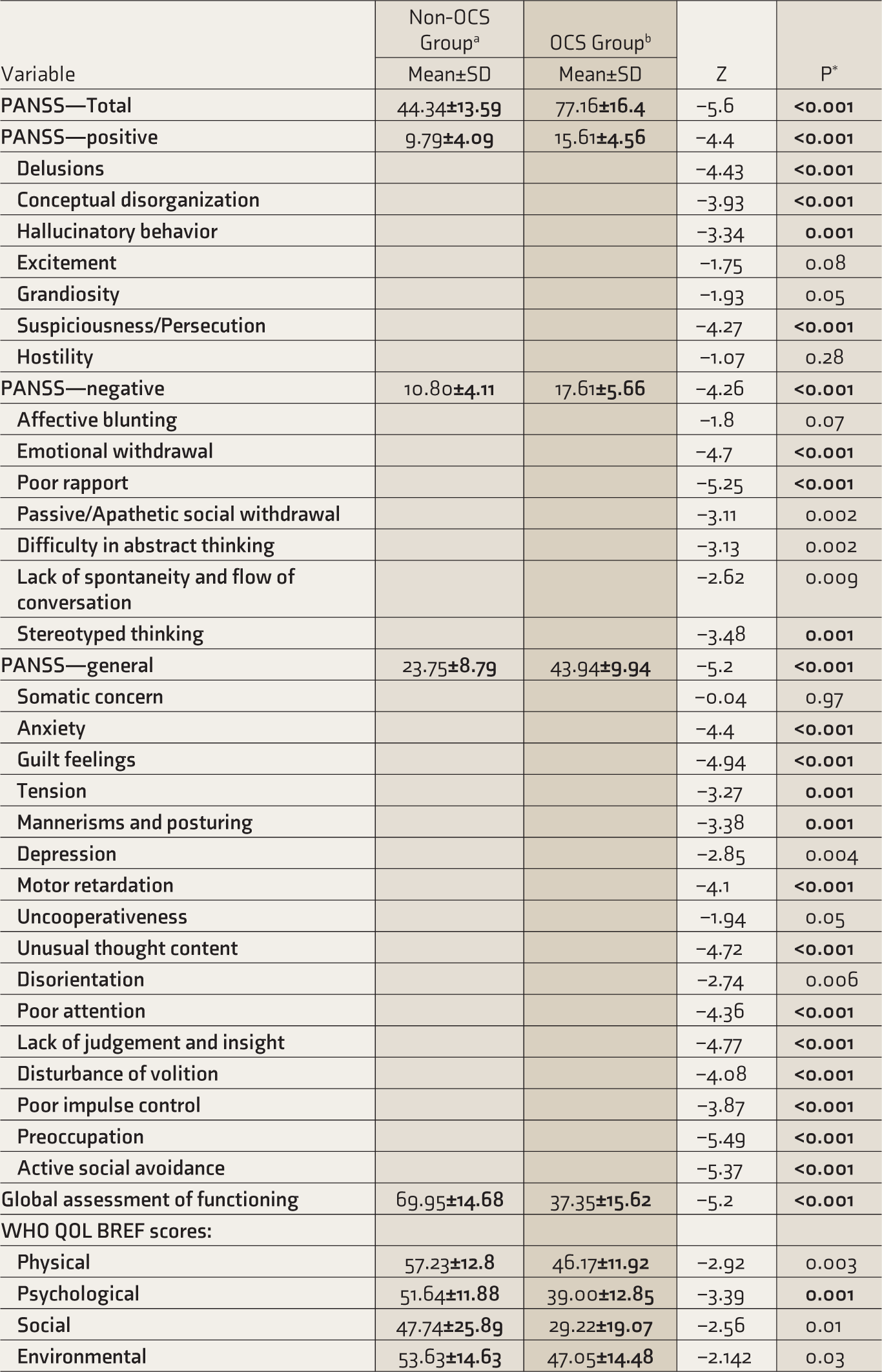
aSchizophrenia patients without obsessive-compulsive symptoms. bSchizophrenia patients with obsessive-compulsive symptoms.
OCS: Obsessive-compulsive symptoms.
PANSS: Positive and Negative Syndrome Scale. WHO QOL BREF Scores: WHO Quality of Life Brief Scale. *P values in bold indicate significant values (P ≤ 0.001).
Association of Severity of Obsessive-Compulsive Symptoms with Clinical Variables
In the OCS group, positive correlations of YBOCS score were seen with the total and three subdomain scores of PANSS, implying that patients with more severe OCS had worse positive, negative, and general symptoms of schizophrenia. A statistically significant negative correlation was seen with quality of life, especially in physical and psychological health domains, thus implying that patients with more severe OCS had worse quality of life. Similarly, patients with more severe OCS had a statistically significant worse overall functioning on the GAF (Table 3). In the OCS group, on partial correlation after controlling for the total PANSS score between the total Y-BOCS score and all domains of WHO QOL BREF (physical, psychological, social, and environmental) and GAF scores, a statistically significant negative correlation was seen only with GAF (r = –0.4, P ≤ 0.001) (OCS group n = 18).
Association Between Y-BOCS Score and Clinical Variables.
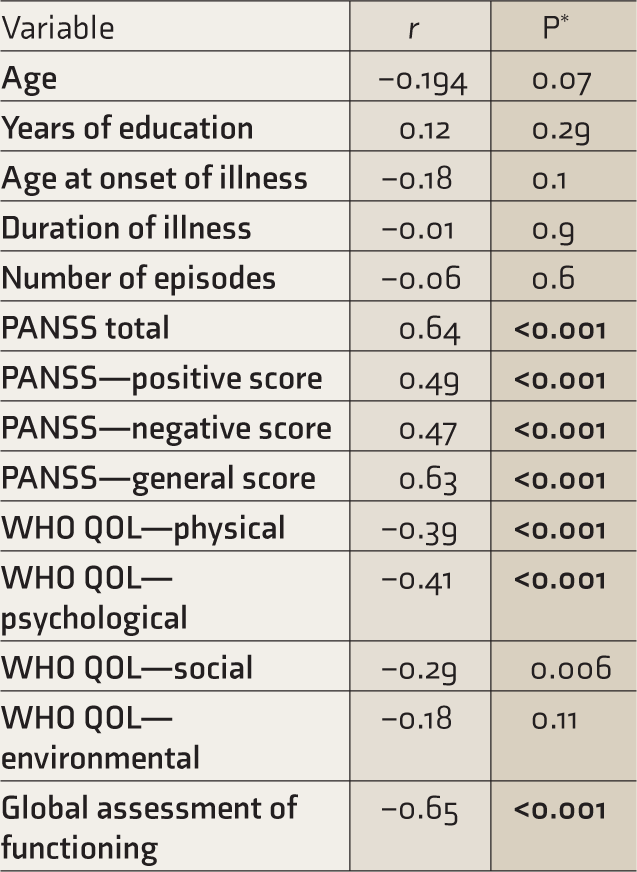
*P values in bold indicate significant values (P ≤ 0.001). PANSS: Positive and Negative Syndrome Scale. WHO QOL BREF Scores" WHO Quality of Life Brief Scale.
Y-BOCS: Yale-Brown Obsessive Compulsive Severity Scale.
When correlation analysis was done between the Y-BOCS total score and each item of PANSS in the OCS group, a significant positive correlation was seen with delusions (ρ = 0.42, P < 0.001) emotional withdrawal (ρ = 0.49, P < 0.001), anxiety (ρ – 0.51, P < 0.001) guilt (ρ – 0.52, P < 0.001) and depression (ρ – 0.35, P < 0.001) (OCS group n = 18) (Table 4).
Correlation between Y-BOCS Score and PANSS Domains.
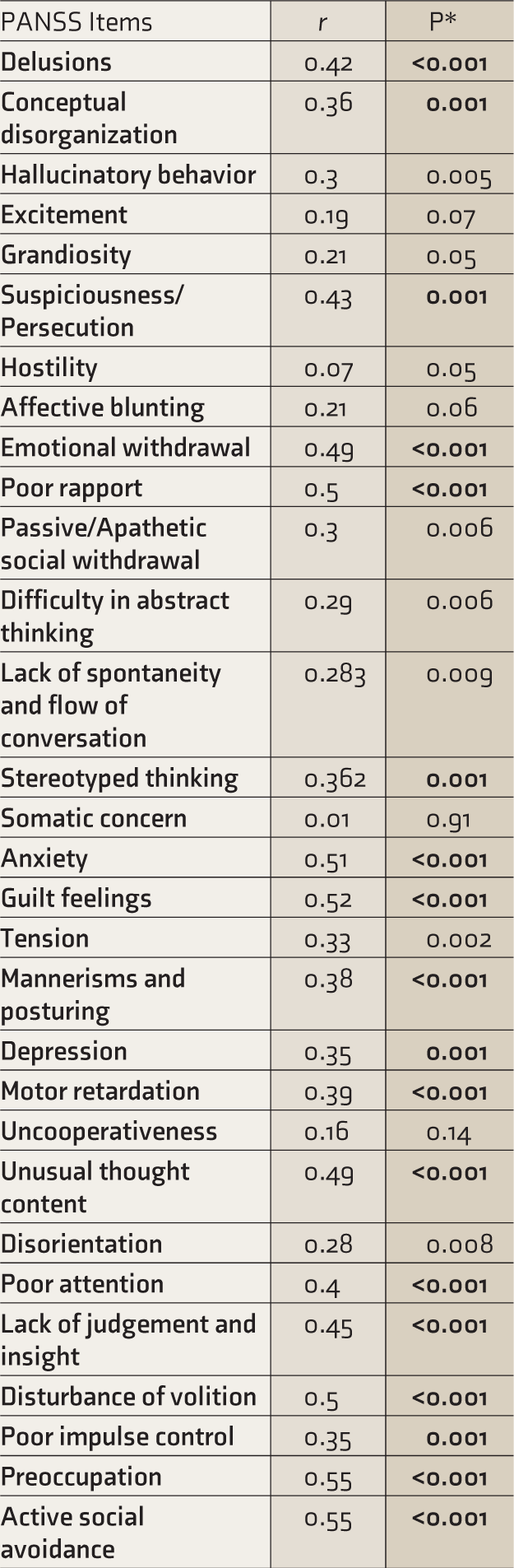
*P values in bold indicate significant values (P ≤ 0.001). PANSS: Positive and Negative Syndrome Scale.
Y-BOCS: Yale-Brown Obsessive Compulsive Severity Scale.
Discussion
The impact of OCS on psychotic symptoms in schizophrenia has been widely assessed, with inconsistent results. We checked whether there is any correlation between the severity of schizophrenia and OCS.
There is no consensus on the relationship between sociodemographic factors and OCS in schizophrenia. Some studies reported that patients with schizophrenia and Obsessive-Compulsive Disorder (OCD) are more likely to be males, hail from a lower socioeconomic status, be employed, and have a higher level of education.16,25–27 Others have observed a lack of relationship with sociodemographic variables, like this study, wherein no significant differences were observed between those with and without OCS on any sociodemographic characteristics.15,27 Also, no statistically significant relationship or difference was established between the groups based on their illness characteristics. However, researchers such as Grover et al. have shown a positive correlation between the duration of schizophrenia and the severity of OCS, and significantly higher Y-BOCS scores in patients with a history of recurrent episodes compared to first-episode schizophrenia patients. 25
In this study, patients with OCS had greater severity of formal thought disorders and delusions. In contrast, some previous studies have reported greater severity of bizarre behavior and lower severity of delusions, hallucinations, and formal thought disorder.28,29 Also, regarding negative symptoms, while we found more severe negative symptoms in general, except for affective flattening, where no significant difference was noted, various studies have reported both greater and lesser severity of affective flattening and lower anergia.18,28 These differences may be attributed to different sampling strategies, assessment instruments, and study design.
Our correlation analysis revealed that the severity of obsessions and compulsions are associated with more severe psychosis, higher dysfunction, lower functioning, and QOL. Furthermore, even when PANSS total score was employed as a covariate, the relationship between global functioning and the Y-BOCS score remained. The above findings thus suggest that OCD/OCS may deleteriously influence patients in clinical remission. This contrasts with early research that indicated that OC symptoms could predict a favorable prognosis by slowing the “personality breakdown” associated with schizophrenia, even indicating a psychotic remission.30,31 However, this notion has been disproved by recent studies showing that OCS may adversely influence the course of schizophrenia, usually entailing greater severity and poorer prognosis.1,25 Moreover, patients with schizophrenia and OCS seem to have more severe psychotic and depressive symptoms and lower social functioning and disability.11,27,32,33 However, some recent studies have suggested that the impact of schizophrenia may vary depending on the stage of schizophrenia, with early schizophrenia having a shielding effect and chronic schizophrenia having a deleterious effect. 34
In this study, delusions and OCS were found to have a positive correlation, supporting the view that these reflect a manifestation of over-valued ideas lying on a continuum of obsessional doubts to delusional certainty, suggesting a common underlying mechanism that may be related to a decreased capacity to inhibit behaviors or thoughts. 11 In addition, it has recently been argued from a dimensional research perspective that OCS are linked to the thought disorder dimension, which encompasses psychotic symptomatology and the internalizing dimension. 35 Also, present neurobiological evidence suggests that a hyperdopaminergic state in the ventral striatum can cause excessive valuation or selection of repetitive behaviors and directly contribute to OCD-related compulsivity. 36 These findings, thus, further support the presence of a psychopathological continuum between obsessive-compulsive and psychotic phenomena. Further, this study shows that OCS may indicate worsening schizophrenia, with such patients having poorer functioning and QOL. But whether it is a cause, effect, or a pre-existing morbidity amplified remains a question. However, it should be noted that the recent report by Devi et al. did not reveal any differences in the severity of schizophrenia symptoms between schizophrenia pati-ents with and without OCS, warranting the need for large-scale, prospective research on this topic.5,25,37 Some studies have also suggested that discrepancies in diagnosing obsessions in the presence of delusions could contribute to a positive association between OCS and positive symptoms, pointing towards the need for a consensus definition for diagnosis and research in this area. 34
In this study, OCS were associated with higher degrees of impairment in general functioning and QOL. This contradicts the findings of Devi and Wehbe, who found no influence on the QOL.5,37 One reason for the initial results implying a poor QOL in this study could be the severe symptoms seen in schizophrenia patients with OCS. Another reason could be that OCS often compound other symptoms or are signs of a specific pathophysiologic pathway intimately associated with maladaptive or lack of adaptive behavior.38,39 According to some research, in schizophrenia, OCS are linked to higher pessimism and avoidant-focused coping methods. 40 Suicidal ideation and attempts are also more common in schizo-obsessive individuals than in schizophrenia patients. 41 In this study, a positive association was seen between the severity of OCS and guilt, anxiety, and depression components of PANSS, which is in line with other studies.7,25 These symptoms alone may contribute to these patients’ poor functioning and QOL.
This study looked at OCS in schizophrenia patients in remission, thus demonstrating the importance of examining OCS even after clinical remission since they affect cognitive skills and overall functioning. 42 However, it was limited by a smaller sample size than similar previous studies. Also, as this was a cross-sectional assessment, it does not give a definite idea of the effect of OCS on schizophrenia symptoms throughout the disease course. As the study sample was taken only from one source (hospital-based) and only in one phase of the illness, i.e., remission, the findings have limited generalizability. Before recruitment, the subjects were on psychotropic medications, which could have ameliorated or worsened specific symptoms. Including a group of patients with primary OCD or affective disorder as a comparator could have provided more detailed information regarding the prevalence and characteristics of OCS/OCD in schizophrenia.
For future studies, a bigger sample, recruited preferably from the community, will give a more complete idea of the extent of the illness in question. Consensus definitions may be used to enhance the comparability of the results across findings. Considering that there is a dearth of longitudinal studies on this topic on Indian populations, future studies should consider such design as they may help establish the temporal relationship between schizophrenia and OCS and how OCS affects patients’ long-term functioning.
Conclusion
Schizophrenia patients with OCS have more severe symptoms and a lower QOL. There is a strong correlation between the intensity of OCS and schizophrenia symptoms, global functioning, and QOL. Future research in this area should include a comparison group, such as people with primary OCD, and a longitudinal design to determine the actual effects of OCS on other elements of the patient’s life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.