
Abstract
Background:
Depression is a common mental health disorder with a wide treatment gap despite the availability of a number of effective treatment options. Blended interventions adopt a novel approach in combining internet-based self-help with brief face-to-face sessions thereby combining the advantages of both approaches and offering scope to address the treatment gap. The present study examined the effectiveness of a blended intervention combining the use of guided internet-based self-help with four to six face-to-face sessions in the treatment of mild to moderate depression.
Method:
A single group, open-label design was adopted with baseline, postintervention, and three-month follow-up assessments. The sample comprised 60 individuals with a primary diagnosis of major depressive disorder, dysthymia, or recurrent depressive disorder of mild or moderate severity meeting eligibility criteria. Standardized measures (self-report and clinician-rated) were used to examine the effectiveness of the intervention in reducing depression, improving functioning, self-esteem, and psychological recovery. A total of 40 participants completed the intervention and follow-up assessments.
Results:
Significant improvements were noted from baseline to post-assessment for both completers’ and intent-to-treat samples, with medium to large effect size on most outcome measures and maintenance of gains at follow-up. Eighty-five percent of the completers showed clinically significant improvement. Subgroups of blended intervention participants with and without pharmacotherapy showed similar outcomes. Completers were higher on interest in learning self-help skills and on the Growth subscale of psychological recovery, compared to the dropouts at baseline.
Conclusion:
The blended intervention demonstrated effectiveness in reducing depression and improving self-esteem, and functional and psychological recovery.
Keywords
The study examined effectiveness of a novel blended intervention in reducing depression. An 8-week blended intervention that integrated an internet-based self-help program with 4-6 face-to-face therapy sessions was effective in reducing depression, improving functioning, self-esteem and psychological recovery. Medium to large effect sizes and clinically significant changes were noted. The gains were maintained at 3-month follow-up. Blended intervention for depression holds promise for improving access to psychotherapy in the urban Indian context.Key Message:
Depression is one of the most common mental health disorders and is associated with significant personal and socio-economic burdens. 1 A large proportion of individuals affected by depression remain without treatment.2,3 Even among treatment seekers, a significant proportion of those treated adequately with medication continue to experience residual symptoms and sub-optimal recovery.4,5 Despite its utility and guidelines advocating the use of psychological interventions for depression, 6 psychotherapy is often underutilized in outpatient settings.7–9 While several patients express a preference for psychotherapy,8,10 under-resourced outpatient settings with the non-availability of trained therapists or a limited number of overworked professionals pose challenges in providing wide-scale access to evidence-based therapies. 11
There is a vital need to increase efforts to deploy innovative interventions that can be flexibly implemented while ensuring fidelity in low-resource settings. 11 Technology has a high potential to enhance access to mental health care. 12 The use of technology to deliver self-help and guided internet-based psychological interventions has shown promising results and can help cater to a more significant number of individuals seeking treatment. 13
Internet-based interventions have several advantages, such as convenience, anonymity, privacy, and self-determined pace of use, among others.14–16 They could be an appealing and acceptable form of treatment for many.10,17 Studies on internet-based interventions for depression suggest they could be effective in reducing the severity of symptoms.18,19
Unguided internet-based interventions are self-help programs that do not involve therapist contact during the intervention. Individuals work on structured and standardized self-help programs, usually within a specified timeframe. These are likely practical self-help methods for individuals with milder concerns and those who can utilize such programs without external support. Therapist-guided internet-based interventions combine self-help programs with regular but brief therapist contact. 20 The therapist’s role in such guided self-help interventions is usually supportive or facilitative and restricted to providing basic support, encouragement, and reinforcement for the individual’s work with the self-help material.15,16 Therapist contact is brief and can be synchronous, such as personal, telephonic, or asynchronous through e-mail or written feedback. Therapist-guided interventions result in better outcomes in terms of improvement and adherence rates when compared to unguided internet-based interventions.19,21 Seeking to combine the advantages of face-to-face psychotherapy and internet-based interventions, another recent approach, blended interventions, involves combining online intervention elements or modules with standard psychotherapeutic care in either integrated or sequential format.22,23 Blended interventions involve a higher level of support from a therapist as compared to brief therapeutic contact in guided interventions and include brief psychotherapy sessions and internet-based self-help programs. These offer better scope for therapeutic alliance and individualization and for addressing the needs of patients with higher severity of symptoms. At the same time, these can decrease the number of face-to-face sessions required, lead to a more intensive therapy experience for patients by ensuring continuity between or after face-to-face sessions, promote patient engagement, and motivate them to take a more active role in their treatment.23–26
Preliminary evidence considering the effectiveness of blended interventions is promising.23,27–31 There are fewer studies on blended interventions when compared to unguided and guided internet-based interventions, and implementation in routine clinical practice is still in its infancy.20,32,33 A majority of studies on internet-based interventions have been conducted in high-income countries, questioning their relevance and effectiveness in the treatment of mental disorders in developing countries.13,34,35 There is a virtual absence of studies examining blended interventions for depression in India.
The Telecom Regulatory Authority of India regulates the telecommunications sector and its services in India 36 . It estimates that 829.30 million people in India have access to the internet, with rates increasing steadily. The rising internet penetration and smartphone usage could serve as an enormous impetus to the development of “mobile mental health” in India to address mental health care needs.37–39
The present study is conceptualized in the above context of rising common mental health concerns in the Indian context and a vast treatment gap on the one hand and the need to employ available and innovative strategies on the other hand to address structural barriers and resource constraints. Considering the growing internet penetration rates and the potential of blended interventions in the treatment of common mental health disorders, the current study seeks to examine the effectiveness of a blended intervention protocol in the treatment of depression in the urban Indian context.
Objectives
The present study aimed to examine the effectiveness of blended intervention in reducing depressive symptoms and improving functioning, self-esteem, and psychological recovery in individuals with mild to moderate depression.
The study also examined differences between subgroups of participants who received blended intervention and medication and those who received only blended intervention. Variables differentiating between intervention completers and drop-outs were additionally explored.
Methods
Design and Sample
The study adopted a single-arm, open-label design with baseline, post-assessment, and a three-month follow-up assessment. The sample selection criteria are presented in
Sample Selection Criteria.
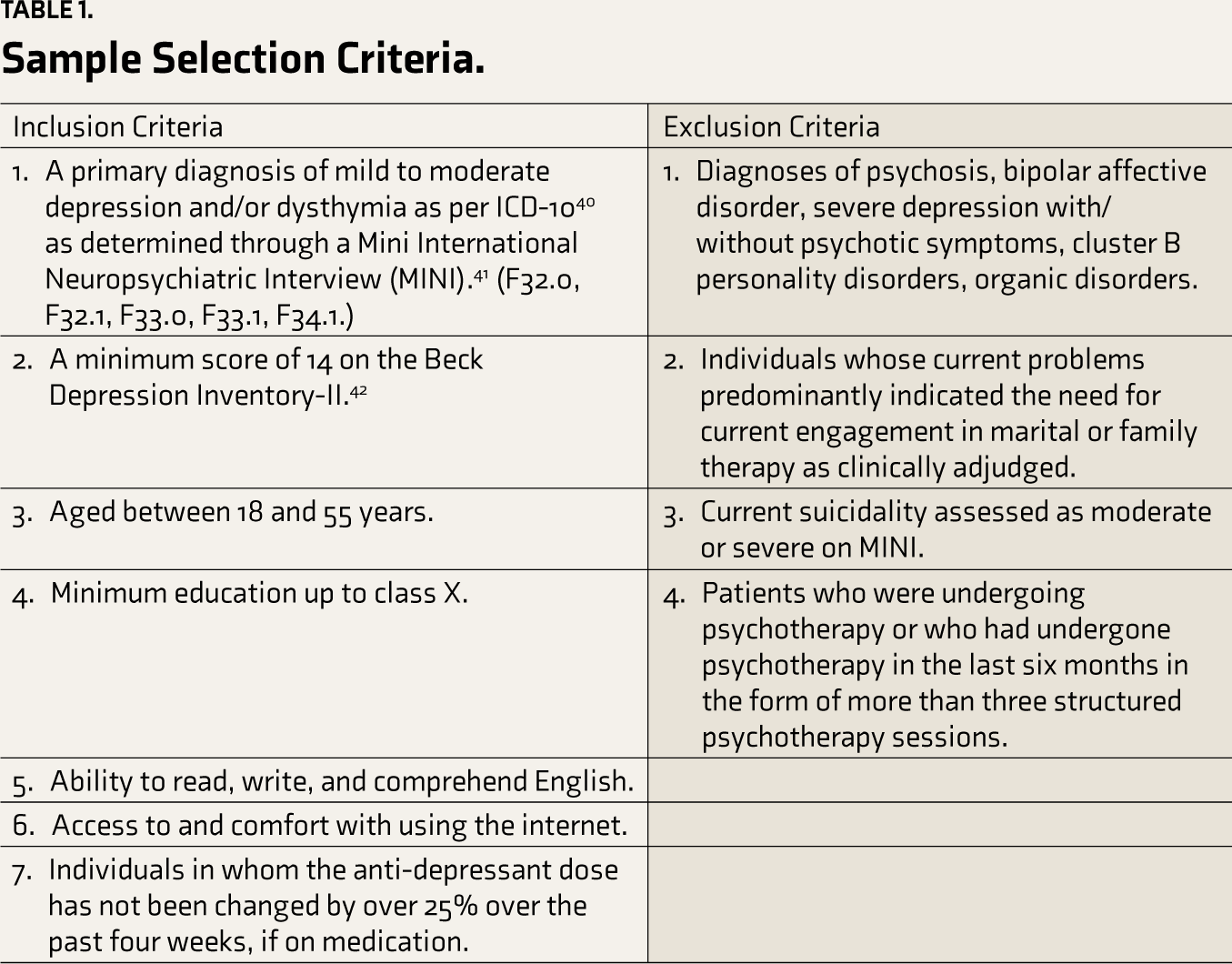
With an intent-to-treat analysis plan, a sample of 60 had about 80% power to detect a standardized mean difference of 0.5 on the Beck Depression Inventory (BDI-II), 42 with an alpha of 0.05. Patients seeking treatment from outpatient services in a tertiary care setting and a community well-being setting and those referred by psychiatrists in private practice were screened for suitability for the study based on the inclusion and exclusion criteria. The eligible participants were enrolled after obtaining written informed consent.
Intervention
The blended intervention was a brief, eight-week integrated intervention that combined an internet-based self-help program for depression called PUSH-D (Practice and Use Self-help for Depression) interspersed with four to six face-to-face sessions with the first author (in-person/video-based sessions) under supervision of the second and third authors. The format of the blended intervention on the whole and the number, structure, and spacing of sessions were finalized based on a review of the literature and observations during the pilot phase. The present study used the integrated form of blended intervention wherein face-to-face sessions and internet-based self-help were integrated and ran in parallel, focusing on internet-based guided self-help and four to six face-to-face sessions. The researchers periodically monitored participants’ engagement with the internet-based program at the backend. They provided therapeutic support and inputs through telephonic support and feedback messages apart from face-to-face sessions. The details of the blended intervention have been described elsewhere.
43
The participants who attended at least three face-to-face sessions, completed five of the 10 essential sections of PUSH-D in eight weeks, and provided baseline and post-assessment data were considered completers of the blended intervention. The details of assessment measures are provided in
Details of Tools Administered.
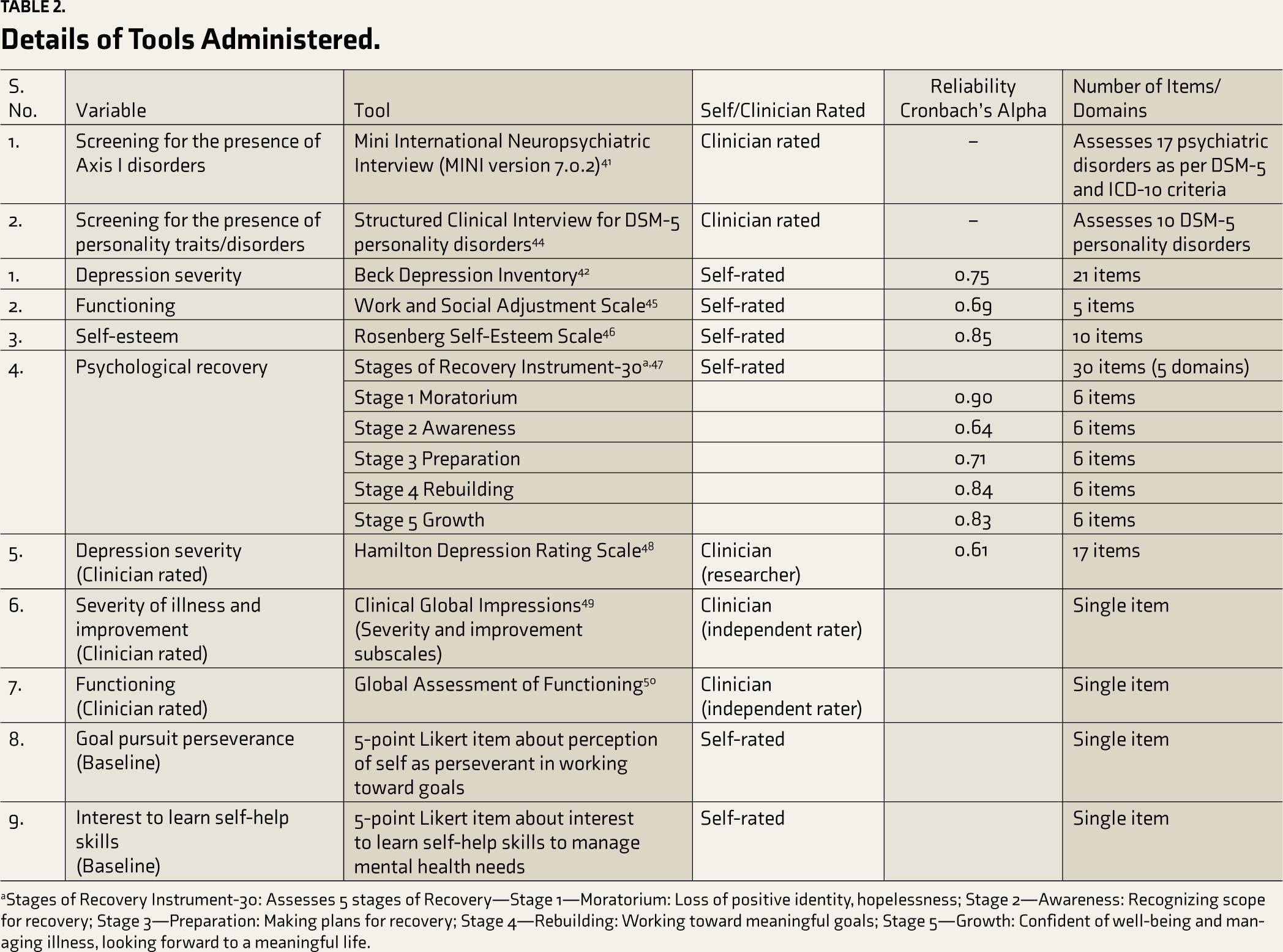
aStages of Recovery Instrument-30: Assesses 5 stages of Recovery—Stage 1—Moratorium: Loss of positive identity, hopelessness; Stage 2—Awareness: Recognizing scope for recovery; Stage 3—Preparation: Making plans for recovery; Stage 4—Rebuilding: Working toward meaningful goals; Stage 5—Growth: Confident of well-being and managing illness, looking forward to a meaningful life.
Assessments
Baseline assessment included basic sociodemographic and clinical details, items on interest to learn self-help skills and goal pursuit perseverance (5-point Likert scale single item questions), and standardized measures of depression, functioning, self-esteem as well as psychological recovery, which is about re-establishing a meaningful and fulfilling life following diagnosis. The details about these assessments at various time points are presented in Table 2. Both self-rated and clinician-rated measures of depression severity (Table 2) were used to corroborate the severity of symptoms prior to enrollment into the study and to assess improvement across time points.
Analyses
Repeated measures, ANOVA or Friedman Test, were used to examine changes in primary and secondary outcome measures across three-time points, baseline, post-assessment, and three-month follow-up assessment, based on the normality of the data. These tests were used to assess change across time points for both completers’ and intent-to-treat samples, as well as to study differences between participants on medication and not on medication for depression on outcome measures. Mean imputation was used to account for missing values. The effect size was calculated for post-assessment data using Cohen’s d. The Reliable Change Index was calculated using the Jacobson and Truax method 51 and the minimal clinically important difference. 52 The present study also assessed whether participants attained reliable clinical change on BDI-II (i.e., symptom change beyond what could be attributed to measurement error alone) and recovery, which refers to moving from clinical to subclinical severity level. In keeping with previous research and to facilitate comparison with other studies, standardized clinical significance criteria for BDI-II comprising a reliable change index of 8.46 and a cut-off point of 14 for recovery were used.24,53,54 Treatment completers and drop-outs were also compared on chi-square tests, independent sample t-tests, and Mann-Whitney U tests to assess for differences in baseline characteristics.
Results
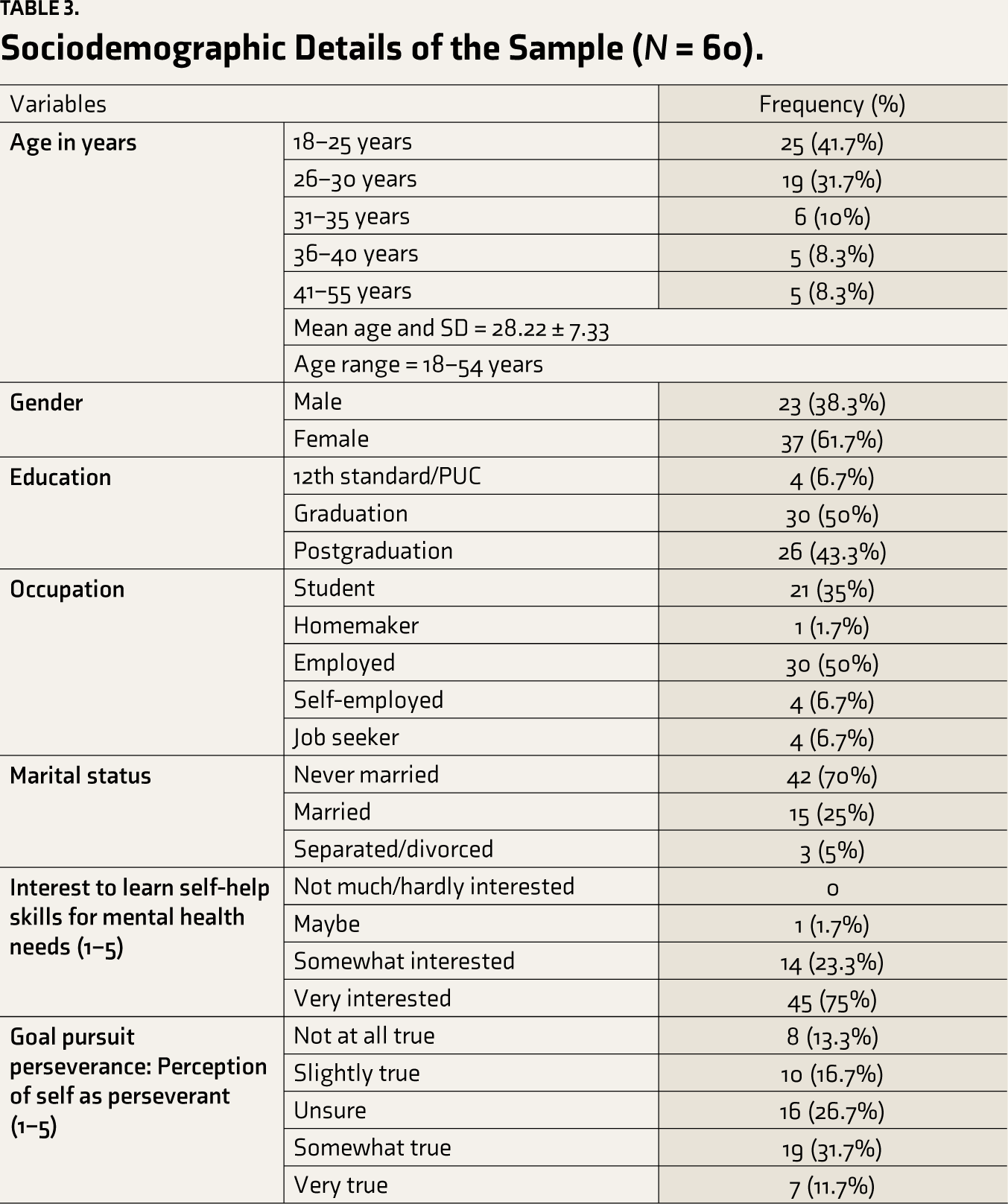
The sociodemographic and clinical details of the sample are presented in Tables 3 and 4.
Sociodemographic Details of the Sample (
Clinical Details of the Sample (
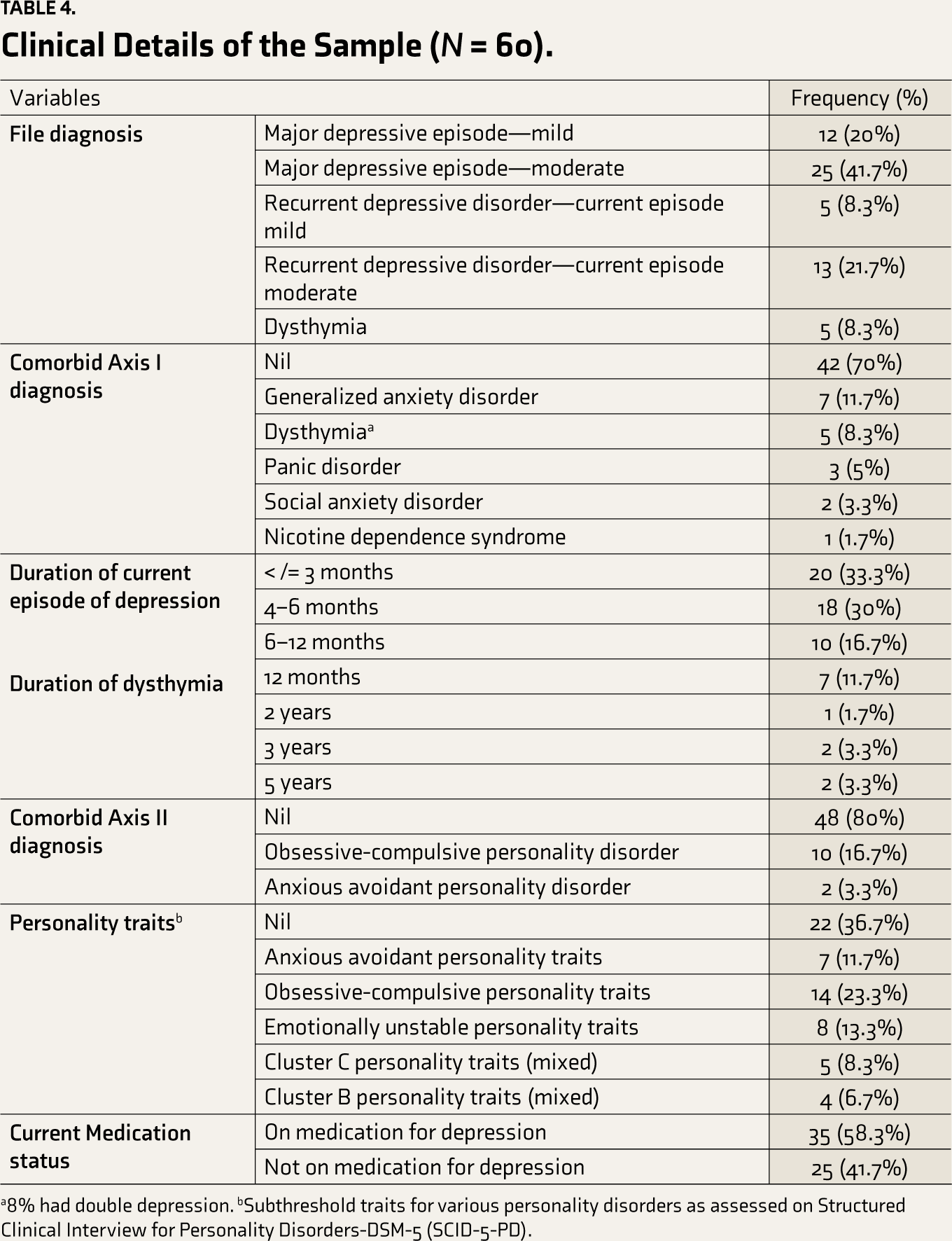
a8% had double depression. bSubthreshold traits for various personality disorders as assessed on Structured Clinical Interview for Personality Disorders-DSM-5 (SCID-5-PD).
The participants’ ages ranged between 18 and 54 years. A majority were in the age range of 18–35 years (83%); the sample comprised more women (62%) than men (38%). A majority of the participants were graduates (50%). Regarding occupational status, salaried employees (50%) and students (35%) comprised the bulk of the sample.
As can be seen, close to half the sample were diagnosed with a moderate depressive episode (42%). A majority did not have a comorbid mental health condition (70%), while generalized anxiety disorder was the most common comorbid diagnosis (12%). A majority of the sample (80%) did not have any comorbid diagnosis of personality disorder, while the most common personality disorder noted was obsessive-compulsive personality disorder (17%). Similarly, subthreshold obsessive-compulsive personality traits were the most common (23%). More than half the sample were on a stabilized dose of medication for depression (58%) at recruitment, and the remaining were not on any medication for depression (42%). Two-thirds (75%) reported being very interested to learn self-help skills to manage their mental health needs. About 44% reported a moderate to high sense of goal-pursuit perseverance.
The results indicated a statistically significant difference across the time points on all the outcome variables, with a reduction in depression severity assessed on BDI and HDRS, a reduction in functional impairment, and an improvement in self-esteem in the completers’ sample (
Changes on Outcome Measures Across Study Time Points in Completers’ Sample (
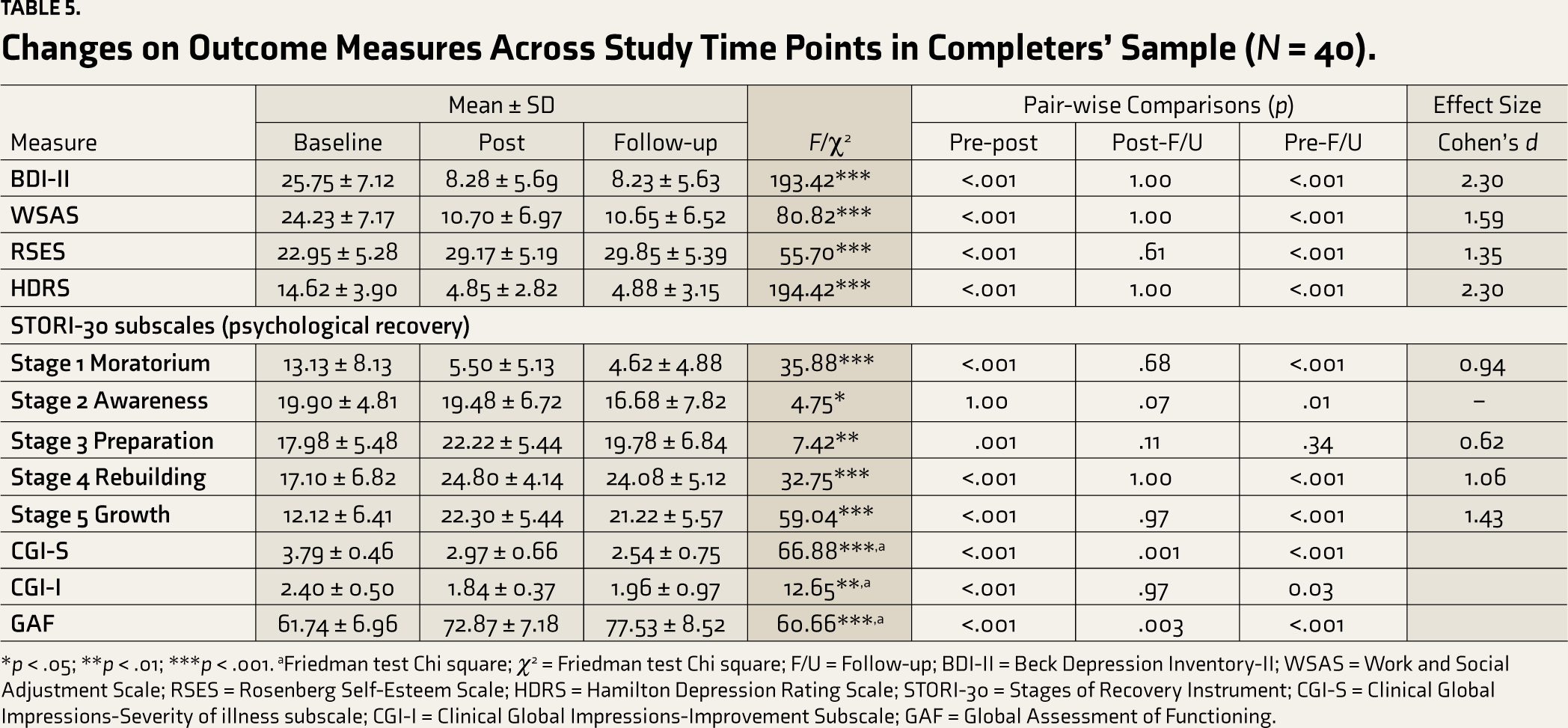
*p < .05; **p < .01; ***p < .001. aFriedman test Chi square; χ2 = Friedman test Chi square; F/U = Follow-up; BDI-II = Beck Depression Inventory-II; WSAS = Work and Social Adjustment Scale; RSES = Rosenberg Self-Esteem Scale; HDRS = Hamilton Depression Rating Scale; STORI-30 = Stages of Recovery Instrument; CGI-S = Clinical Global Impressions-Severity of illness subscale; CGI-I = Clinical Global Impressions-Improvement Subscale; GAF = Global Assessment of Functioning.
Similarly, on psychological recovery, statistically significant changes were noted on all the subscales, with a reduction in the moratorium and improvement in awareness, preparation, rebuilding, and growth subscales. Pair-wise comparisons showed that significant changes occurred from baseline to post and follow-up assessments, and these gains were maintained from post to follow-up assessment. The distribution of participants on the stages of psychological recovery indicated that while two-thirds of participants were in the moratorium and awareness stages at baseline (70%), more than two-thirds (73.8%) were in the rebuilding and growth stages at post-assessment.
The intent to treat analysis results was similar to the completers’ sample. They indicated a statistically significant difference across the time points with a reduction in depression severity and functional impairment as well as improvement in self-esteem and psychological recovery. The findings are presented in Table S1.
Large effect sizes were observed on depression (both self-rated and clinician-rated measures), functional impairment, and self-esteem, as well as rebuilding and growth subscales of psychological recovery in the completers’ sample at post-assessment.
Clinically significant change was coded in cases that demonstrated reliable change and recovery.24,51 A total of 34 out of 40 follow-up participants (85%) met the criteria for clinically significant change. No reliable deterioration was noted at follow-up in any of the completers. Another approach was also used to determine the clinical meaningfulness of changes. Button et al. 52 observed that minimal clinically significant difference (MCID) is best measured on a ratio scale as a percentage reduction in the score as compared to the baseline score. They estimated MCID on BDI-II according to the optimal threshold above which individuals report feeling “better” and found a 17.5% reduction in scores from baseline scores.
Further, they noted that the corresponding estimate for individuals with longer duration of depression who had not responded to antidepressants was higher at 32%. The present study data on completers indicated that all the participants experienced a more than 17.5% reduction in BDI-II compared to their baseline scores. All except two participants experienced at least a 32% reduction in these scores. These findings underscore the clinical meaningfulness of the reduction in depression scores observed in individual participants’ data following the blended intervention.
Participants receiving blended intervention along with pharmacotherapy and those receiving blended intervention alone did not differ significantly in age, gender, education, and duration of illness (Table S2). No significant difference between these two groups emerged following the intervention on any outcome variables, suggesting that these groups exhibited comparable improvement. There was no significant interaction effect. The results of these analyses are presented in Table S3.
A total of 14 participants dropped out before completing the intervention and post-assessment. As per the baseline assessment, they differed significantly in their interest in learning self-help skills, with completers reporting significantly higher interest than drop-outs. Completers also perceived themselves as generally able to work on goals they set for themselves to a greater degree when compared to drop-outs. The completers had a longer duration of illness compared to drop-outs, considering the presence of a diagnosis of dysthymia among 12% of completers. A significant difference was also observed in the presence of personality disorder, with slightly more than a quarter of completers (26%) having a comorbid personality disorder and no diagnosis of personality disorder among drop-outs. On further analysis, it was found that close to a quarter of completers (24%) had a comorbid diagnosis of obsessive-compulsive personality disorder, which differed significantly from drop-outs (X 2 = 4.05, p = .04). There were no significant differences in the presence of other personality disorders. Completers scored significantly higher on the psychological recovery—Growth subscale (when compared to drop-outs). A trend toward significance was also noted on the Moratorium and Rebuilding subscales of psychological recovery. These findings on comparing completers and drop-outs are presented in Table 6.
Comparison of Dropouts (
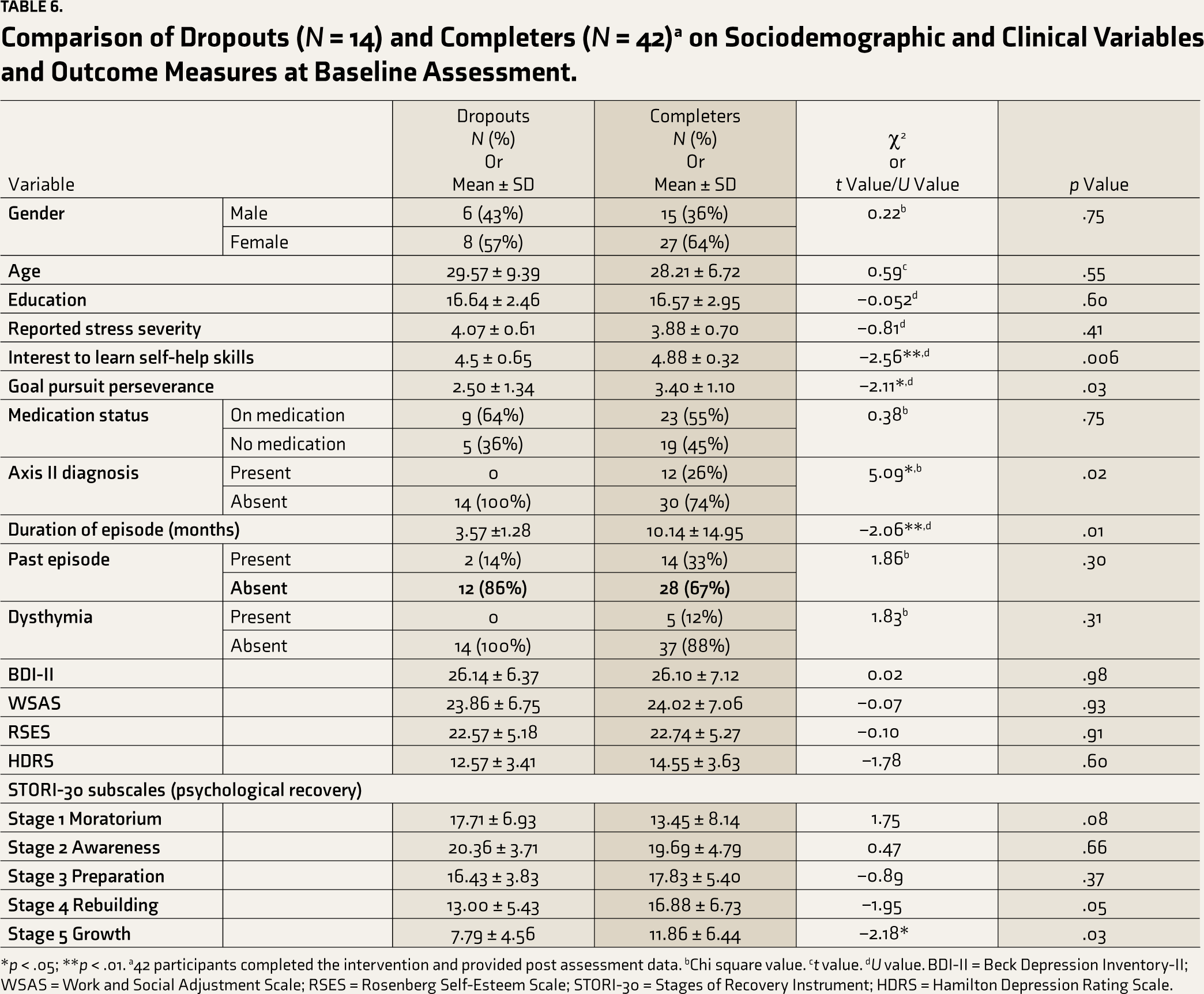
*p < .05; **p < .01. a42 participants completed the intervention and provided post assessment data. bChi square value. ct value. dU value. BDI-II = Beck Depression Inventory-II; WSAS = Work and Social Adjustment Scale; RSES = Rosenberg Self-Esteem Scale; STORI-30 = Stages of Recovery Instrument; HDRS = Hamilton Depression Rating Scale.
Discussion
Most participants were adults aged 18–35, comprising about 80% of the sample. This finding is consistent with intervention studies with similar populations in the Indian setting,55,56 as well as a study using internet-based intervention for depression in the Indian setting. 57 A possible explanation for the preponderance of young adults in the sample in the current study could be due to a wide prevalence of distress 58 and ease of access to the internet in this age group59,60 as well as the appeal of interventions that are conveniently accessible and involve self-help components. Previous studies suggest that youth and young adults prefer self-reliance, and the convenience of access offered by internet-based mental health services may help break barriers to seeking help.17,61
The current study had a somewhat higher representation of women participants than men. This aligns with other blended intervention studies that have reported a higher or almost equal representation of men and women.27,62–64 This may be due to the higher prevalence of depression observed in women 3 , women being at a greater risk for developing depression,65,66 and higher levels of help-seeking for depression observed in women when compared to men.67,68
Fifty-eight percent of the participants were on stable dosages of medication. This mirrors research that finds that a significant proportion of patients diagnosed with depression are treated with medication.69,70 Previous research in tertiary mental health care settings in India has found that between 40% and 75% of patients with common mental health disorders are on pharmacotherapy.8,55,71,72 The number of participants on medication is also consistent with other studies on blended interventions, where 40%–60% of participants were on pharmacotherapy during the intervention.27,73,74 In contrast, the PUSH-D study 75 , which involved guided internet-based intervention, noted that less than a quarter of the participants were on pharmacotherapy. That was a community study that appealed to non-treatment seekers. On the other hand, blended interventions, as in the case of the present study, are likely to offer therapeutic intervention to those who may not otherwise receive combined treatment or those who do not prefer/cannot be prescribed pharmacotherapy for various reasons.
Blended internet-based intervention studies for depression with or without control/comparison groups have found these to be effective in reducing depressive symptoms and maintaining gains over follow-up periods ranging from 3 to 12 months.24,63,76–79 A few have found both face-to-face interventions and blended interventions to be equally effective.28,79–82 A few other studies25,27,74 report that blended interventions could be more effective than face-to-face psychotherapy and suggest the possibility that blended interventions could provide an opportunity for treatment intensification and result in additional and longer-lasting outcomes. There is scope for further research on the benefits of augmenting psychotherapy using a blended approach.
Only a few studies assessing the effectiveness of blended interventions have utilized clinician and self-report measures.29,79 The current study demonstrated significant changes in depression on both self-rated as well as clinician (researcher) rated measures of depression in keeping with Wright et al.’s study. 79 In addition, participants were also rated by an independent rater on the severity of illness on the Clinical Global Impressions Scale. A significant reduction in illness severity across time from baseline to follow-up assessment was observed. Considering the current study’s single-group study design, independent raters could not be blinded to the intervention received by the participant. However, the raters were not involved with the intervention and were not aware of intervention progress, and an attempt was made to have raters familiar with the patient’s history to judge improvement or worsening from the baseline.
The effect size estimate for depression was d = 2.30 in the current study, indicative of a large magnitude of change in depression severity as assessed on BDI-II and HDRS. Medium to large effect sizes ranging from 0.65 to 2.43 have been found in other studies assessing the effectiveness of blended interventions for depression.24,27,63,74,76, 79, 82
A statistically significant change does not necessarily translate to clinically meaningful change. Rather than merely comparing groups or two-time point data for a single group, examining within-person changes at the individual level is also necessary, thereby reflecting an idiographic approach to understanding change following an intervention. Hence, an attempt was made in the present study to go beyond examining the statistical significance of change following intervention and effect size (magnitude of change in the sample) and determine the proportion of participants in whom the improvement in depression severity could be considered clinically meaningful. This was assessed using clinically significant change 51 and minimal clinically important difference. 52 Overall, 85% of the completers exhibited clinically significant change by meeting the reliable change and recovery criteria. All the participants experienced a more than 17.5% reduction in BDI-II compared to their baseline scores and met the minimal clinically important difference (MCID) criterion. These results lend further support to the effectiveness of blended intervention for mild to moderate depression. Only a few studies on blended interventions for depression have examined the clinical significance of change, and varying rates of recovery have been reported, with studies generally reporting rates of recovery between 50% and 85%.24,28,63,76, 80, 82
A significant reduction was noted in functional impairment from baseline to follow-up assessment in the completer’s sample with a large effect size, suggesting that the blended intervention was effective in improving work and social functioning. Participants were also assessed on the clinician-rated measure of functioning by an independent rater. The results corroborated findings of significant improvement as self-rated by participants. Only a few studies on blended interventions have incorporated clinician-rated measures of functioning, and fewer still both self-rated and clinician-rated measures. 81
The findings of improvement in self-esteem in the current study are in keeping with research that finds that psychotherapy for depression could have secondary effects on improving self-esteem. 83 The components of the internet-based program PUSH-D address similar components, such as dysfunctional thinking and self-criticality, which may partially explain the improvement in self-esteem. The study findings are also comparable to the findings of the PUSH-D pilot study. Low self-esteem is often seen as part of a constellation of depressive symptoms. However, few studies have examined changes in self-esteem with psychological interventions as a predictor of long-term outcomes. Dinger et al. 84 found that changes in self-esteem during psychotherapy predicted depressive symptoms six months after the termination of therapy, even when controlling for within-treatment changes in symptoms. More studies are needed to assess improvement in self-esteem or psychological recovery following blended interventions. 74 The role of positive shifts in self-esteem following blended intervention in reducing relapses and recurrence over time is worthy of examination in further research.
The results on domains of psychological recovery indicate that participants showed a significant reduction in moratorium and improvement in preparation, rebuilding, and growth from baseline to follow-up assessment. An improvement in self-agency and taking responsibility for positive changes has been described previously in studies on blended interventions,85,86 and it has been suggested that internet-based interventions, including blended interventions, could help foster greater autonomy, self-efficacy, and a sense of responsibility as participants work on cultivating self-help skills more independently when compared to traditional psychotherapies.26,33,63,79
No differences were observed in outcomes in subgroups of participants receiving blended intervention with or without medications. A greater preference for psychotherapy over pharmacotherapy in patients with common mental health disorders has been noted.10,87 A recent study in the Indian setting also found that most patients expressed a preference for psychotherapy alone or combination treatment involving pharmacotherapy and psychotherapy. 8 Patients receiving preferred treatments are also likely to report better outcomes.88,89
The National Institute for Health and Care Excellence (NICE) provides evidence-based guidelines for managing various health conditions. The revised NICE guidelines recommend the use of psychological interventions in combination with pharmacotherapy for moderate or more severe forms of depression right at the outset. In contrast, psychological interventions such as guided self-help or group or individual cognitive therapy are advised as a first line of treatment for less severe depression. 6 A network meta-analysis that compared the relative effects of psychotherapies, pharmacotherapies, and their combination in treating depression found combined treatment to be more effective than psychotherapy alone or pharmacotherapy alone. 90 It was also noted that the patients considered combined treatment and psychotherapy more acceptable than pharmacotherapy. These observations could explain the finding of relatively equal improvement in both groups in the current study, where participants were not randomly assigned to treatments and likely received either combination treatment or preferred choice, opting for psychotherapy.
While recent literature points to the most effective form of treatment possibly being a combination treatment, routine use could not only prove expensive; however, it would also require increased access to psychological therapies.91,92 The use of collaborative care models in primary health care settings can offer opportunities for improved dissemination of combined treatments, with guided self-help and internet-based interventions employed along with brief sessions to reduce cost and improve access. 90
Completers and drop-outs differed significantly in their interest in learning self-help skills to manage mental health concerns. It is plausible that completers were more open to and interested in an intervention involving structured self-help than drop-outs and were more likely to complete the intervention. Literature suggests that clients are more likely to drop out of interventions that do not match their preferences or those they are dissatisfied with.88,89,93 Internet-based interventions require participants to be relatively self-regulated to complete an Internet-based program, mainly when no or minimal support is provided. 94 In the present study, a significant difference was observed in goal pursuit perseverance, with completers more often perceiving themselves as perseverant when compared to drop-outs, as assessed at baseline. In the previous PUSH-D study, authors highlighted the need to examine self-regulation deficits in the non-completion of internet-based programs. In the present study, despite higher levels of guidance and contact with the therapist through face-to-face sessions, self-rated goal-pursuit perseverance still emerged as a significant differentiator between completers and drop-outs. A higher sense of perceived perseverance may serve as a helpful factor in completing blended interventions.
There was no significant difference between drop-outs and completers on medication status. Preference for receiving therapy inputs via the blended approach along with initial interest in learning self-help and the convenience factors associated with blended intervention (not requiring frequent commutes for therapy sessions) may have helped sustain the motivation to initiate and complete blended intervention in the group, which was already receiving medication, and this may have contributed to lack of difference between the two groups on drop-out rates.
In the current study, completers had a longer duration of illness when compared to drop-outs, although the severity of depressive symptoms was not different. Participants who had a longer duration of illness likely perceived a greater need for learning self-help and receiving psychotherapy inputs. This hypothesis on the association between chronicity of symptoms and motivation for and adherence to blended intervention warrants examination in further studies. Completers in the present study were more likely to have a personality disorder diagnosis than drop-outs, but this was mainly attributable to the fact that a quarter of the completers met the criteria for a diagnosis of obsessive-compulsive disorder compared to the drop-outs who did not have a comorbid personality disorder diagnosis. Perhaps participants with a diagnosis of obsessive-compulsive disorder found it appealing to work on a structured self-help intervention with regular feedback and guidance, which might have helped them to sustain motivation and complete the intervention when compared to the drop-outs. However, there is a need for further research on this. No significant differences were found between completers and drop-outs on the severity of depression, functional impairment, and self-esteem at baseline. The completers and drop-outs did differ significantly on the Growth subscale of psychological recovery, and trends toward significance were noted on the Moratorium and Rebuilding subscale at baseline. Together, these findings suggest that completers may have been more hopeful and perceived themselves to be more prepared or motivated to address their ongoing mental health concerns. This is corroborated by a study that explored participants’ motivation to persist with blended interventions, wherein hope for recovery and a desire to regain control over one’s life were noted as intrinsic motivators along with other factors. 86 As a corollary, the present study findings imply that individuals lower on growth or higher on moratorium scores on psychological recovery may benefit from more face-to-face sessions at the beginning to enhance their motivation and engagement in blended interventions and minimize drop-out risk.
Strengths and Limitations
Some of the study’s strengths were the use of an indigenously developed blended protocol attempts to assess a broad range of outcomes, including symptomatic, functional as well as psychological recovery, the use of self-rated and clinician-rated measures, and the assessment of clinical meaningfulness of changes. The study has its share of limitations. It used a single-group design. Future research could use controlled designs and longer follow-ups to examine the robustness of the findings. The blended intervention developed could be compared with other established interventions for depression, including face-to-face therapy, to understand its comparative effectiveness. The generalizability of the findings could be further improved by studying the effectiveness of the intervention in diverse samples such as those including a better representation of personality disorders as comorbidities, non-treatment seekers, treatment seekers in varied settings such as community health care centers, private hospitals, varied age groups and individuals from urban and semi-urban backgrounds and by utilizing vernacular versions of the internet-based intervention. The scope of delivery of the blended intervention by trained non-specialists using a stepped-care approach could also be examined for potential large-scale implementation.
Conclusion
To the best of our knowledge, the current study is among the first blended intervention protocols for depression to be developed and tested in India. It used an indigenously developed internet-based intervention that was combined with brief face-to-face sessions in a sample of treatment seekers with mild to moderate depression with significant functional impairment. The intervention demonstrated preliminary effectiveness on multiple outcomes with medium to large effect sizes and clinically significant changes maintained at follow-up.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Institutional Ethics Committee (National Institute of Mental Health and Neurosciences, NIMHANS) No. NIMH/DO/IEC (BEH.Sc.DIV)/2019.
Funding
The first author gratefully acknowledges funding support received from the Indian Council of Medical Research for her doctoral work on which this article is based.
Informed Consent
The eligible participants were enrolled after obtaining written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.