
Abstract
Background:
Street children are vulnerable to adverse health and risk behaviors and drug use. Substance use among street children has been well documented in several countries. This study reports sociodemographic and peer, family, and stress-related factors associated with substance use and non-use in a representative sample of street children of Delhi.
Methods:
This cross-sectional survey was conducted through six NGOs working with street children, using Respondent Driven Sampling, in nine districts of Delhi (n = 766, 7–18 years). The multivariable model was developed by applying binary logistic regression analysis.
Results:
The rate of substance use was 49%. Significant association was found between substance use in the past year and increasing age [Odds Ratio: OR (95% Confidence Interval)] [1.22(1.12,1.33)], male sex [4.34 (2.28,8.26)], lacking psychosocial support from family/relatives [3.27(1.84,5.80)], being engaged in earning from illegal sources, [3.04(1.75,5.29)], family use of substance [2.59(1.38,4.89)], presence of substance-using peers [29.86(14.38,62.01)], lack of non-drug-using peers [2.35(1.46,3.79)], and not possessing basic amenities [2.26(1.31,3.93)].
Conclusion:
Multiple modifiable factors exist within the family and peer group, including risk and protective factors or a consequence of substance use. Some challenges in the form of difficulty in reaching out to them and poor treatment seeking by those using substances warrant intensification in both primary and secondary prevention initiatives.
Substance use among street children warrants public health concern. Family and peer group factors are important as risk and protective factors and targets for intervention.Key Messages:
Homeless or street children, as a population sub-group, exist worldwide and in significant numbers. 1 The actual count of street children is unknown because epidemiological surveys do not routinely collect that information. According to the United Nations Children’s Fund (UNICEF), report in 2021 tens of millions of children live or work on the streets of the world’s towns and cities. 2 As per a study conducted by an NGO in ten Indian cities, the estimate of street children was 202,765, with a maximum of 81,235 in the state of Delhi. 3 The causes for homelessness in developed and resource-constrained settings are dissimilar. In the developed world, familial conflict and child abuse are common factors. In resource-constrained settings, the interplay of poverty, child abuse, neglect, familial dysfunction, death of one or both parents, war, and socio-cultural and religious beliefs compels children to be on the street.4–9
Studies conducted in the last few decades have documented the causes of children living on the streets and their characteristics in several countries. 10 Street children are reportedly vulnerable to adverse health and risk behaviors and drug use.1,11,12 Substance use among street children has been well documented in countries like Bangladesh, Pakistan, Nepal, Iran, Kenya, Ethiopia and Brazil.5–12 For India, the existing data on street children are mostly in the form of small-scale regional surveys documenting reasons for their being on the street, the problems they face, and their occupational profile. 13 Some studies have reported substance use among boys from institutional settings like observation and shelter homes in Andhra Pradesh, Mumbai, and Delhi.14–16 Epidemiological studies from Bengaluru and Itawah (Uttar Pradesh) had documented the prevalence and/or types of substances used, while others described factors associated with substance use among street child samples at a national level.16–19 However, none of the previous studies from India is on a representative sample from a city or town. The present communication aims to assess socio-demographic, peer, family, and stress related factors associated with substance use and non-use on a representative sample of street children of Delhi.
Methods
The study was conducted by an Institute of National Importance in North India as the lead technical agency and implemented by six NGOs working with street children in Delhi. Using Respondent-driven Sampling (RDS), a cross-sectional survey, was conducted in all the nine districts of the National Capital Territory of Delhi among children aged 7–18 who fulfilled the operational definition of ‘street children’ (i.e., either living on or spending most of their time on streets with or without family), did not have any communication disability that hampered the process of participation in the interview, and were willing to participate in the study themselves and refer three of their peers for the survey as well. We considered the definition of street children given by UNICEF: children who reside in the street: children who have ran away from their families and live alone on the streets; children who work in the street; children who spend most of their time on the streets but who regularly go back to their homes; children from street families; children who live in the street with their families. 20
Street children are mobile and hard to reach. We partnered with six NGOs that have been working with street children for years. The interviews were conducted in 25 locations across all regions of Delhi, with one RDS center in each location. These interview sites were equipped with the required infrastructure of the NGOs. Therefore, it was possible to identify the initial seed (participants) in each of these locations with the help of the NGOs. The seeds themselves identified the subsequent participants based on the methodology of RDS.
To ensure penetration into the various sub-networks of street children and thereby ensure representativeness, a profile of “seeds” was decided on parameters of age,7–10,11–14,15–18 types of children (street working, alone on street, family on street), substance use (yes, no), type of substance(s) use (tobacco/alcohol/cannabis/inhalants/sedatives/opioids), registration with an NGO (Yes/No), and the history of treatment seeking for drug use (Yes/No). Data collection commenced on 29 August 2016 and ended on 28 January 2017.
Using standard RDS methodology, each recruited seed was interviewed and provided (a) one incentive for their own participation and (b) three coupons for referring their peers. The respondent could collect a primary incentive after completing their interview and then could collect up to three more incentives for each successful referral, that is, a maximum of four incentives. The incentives were provided for getting interviewed as well as the referring interview (first, second, and third). These included a wristwatch (getting interviewed), T-shirt (for referring first peer), wallet (referring second peer), and backpack (referring third peer). The detailed sampling methodology and the actual field settings for implementing the RDS survey are available from our previous report. 21
Data from each participant were collected by trained interviewers using a specially prepared semi-structured questionnaire in the Hindi language with 82 questions, categorized under different sections viz. socio-demographics, family, peers, stress, physical and psychological factors, and access and willingness to seek treatment. The questionnaire was finalized after pilot testing on five street children. The questions were in the form of continuous data (age), categorical responses (0: No, 1: Yes), multiple responses (with whom did you live usually during the last 1 month, what made you come or spend time on the streets, etc.), or open-ended question (money earned during the last month, age at initiation of various substance, etc.). There were no Likert-type questions.
Ethical considerations
The study was approved by the ethics committee of the All India Institute of Medical Sciences (AIIMS), New Delhi. Informed consent was obtained from the guardian/parent (if available) or the NGO staff as surrogate guardians. Assent from the participating children was also taken. They were given the option of opting out of the interview. The survey was filled anonymously, and no personal identifying information was collected. Participants with identified health and welfare needs were referred to appropriate service providers.
Data Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) software, version 21.0 (SPSS, Chicago, IL, USA). The weighted estimates of different psychoactive substances obtained by performing analysis from Respondent Driven Sampling Analysis Tool (RDSAT) have already been reported in our previous study. 21 The present report focuses on factors associated with substance use in the last one year; therefore, the exact (unweighted) frequencies were utilized for this purpose. The bivariate association of the sociodemographic (Table 1), family and peer-related (Table 2), and physical and psychological (Table 3) characteristics were assessed through the frequency and percentage across substance-using children (SC) and non-substance-using children (NC). The association across all categories for the three domains was evaluated to depict the overall distribution of the SC and NC across different variables. In the case of variables for which multiple responses were elicited, we assessed bivariate association for all responses. The results were interpreted in terms of the χ2 statistic, degrees of freedom, and p value. The adjustment in p value was done by applying the Bonferroni correction (Tables 1, 2, and 3 last column). We reported the exact p value (α) for the level of significance. For the scenario where α was less than 1% (on bivariate χ2 analysis or accounting for multiple comparisons), we reported (p <0.001).
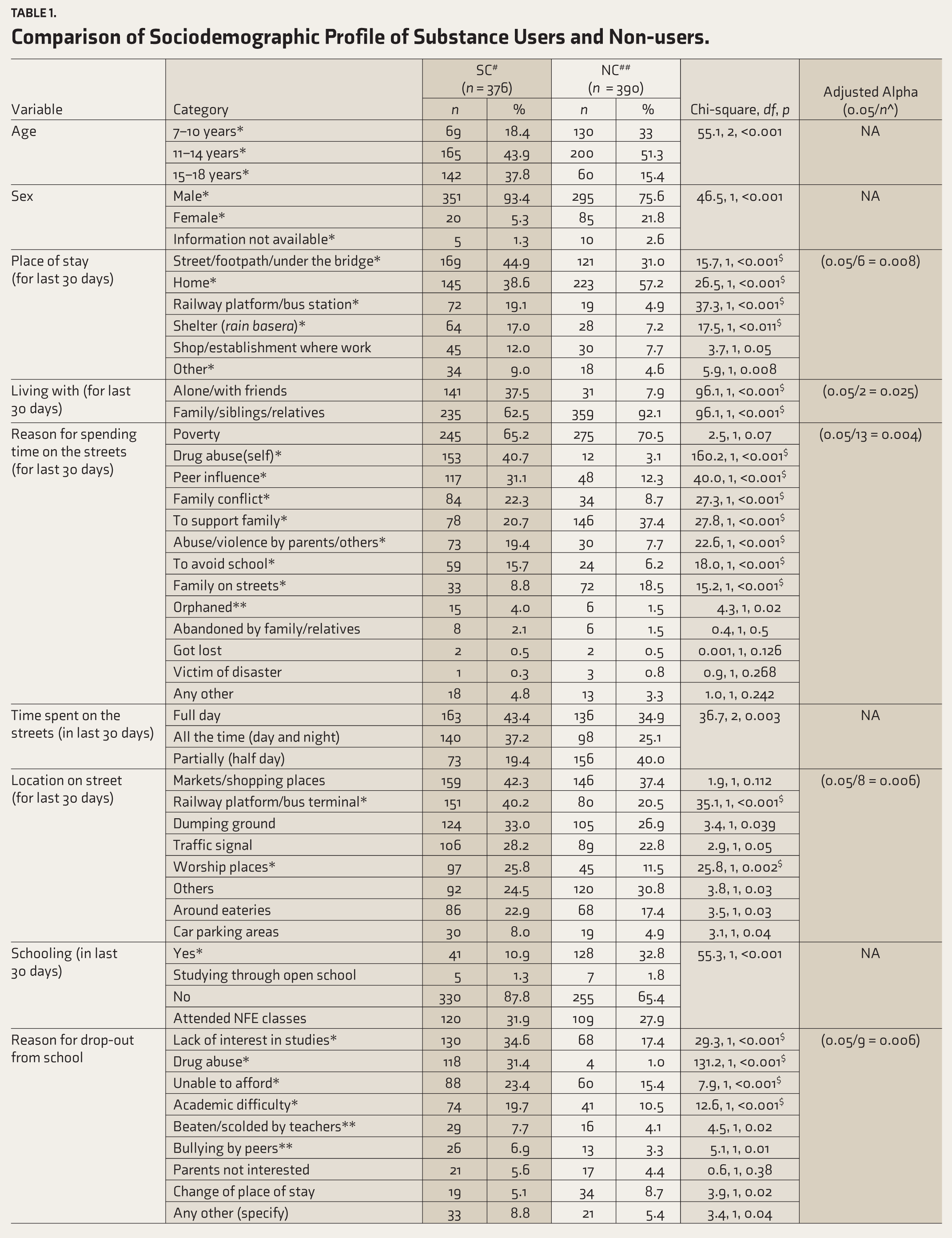
Comparison of Sociodemographic Profile of Substance Users and Non-users.
#Substance-using street children.
##Non-substance-using street children.
*Significant difference between the proportion of individuals across two groups for the characteristics.
^n: Number of categories in the respective contingency table for which separate chi-square statistic is calculated.
NA: Not applicable as an adjustment in p value is not required due to single comparison.
$: Scenario where the p value remained significant even after adjustment for multiple comparisons (Bonferroni’s Correction).
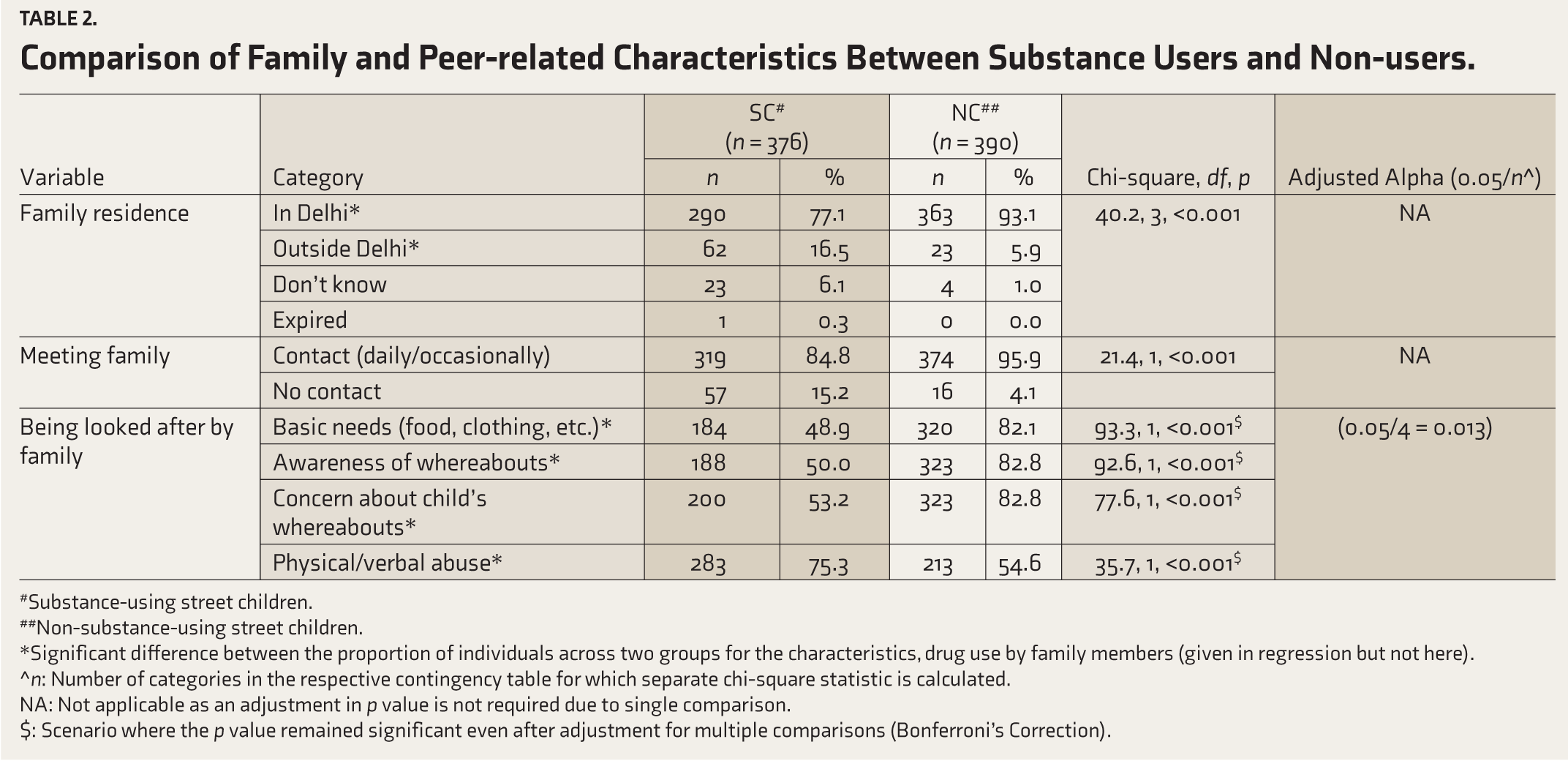
Comparison of Family and Peer-related Characteristics Between Substance Users and Non-users.
#Substance-using street children.
##Non-substance-using street children.
*Significant difference between the proportion of individuals across two groups for the characteristics, drug use by family members (given in regression but not here).
^n: Number of categories in the respective contingency table for which separate chi-square statistic is calculated.
NA: Not applicable as an adjustment in p value is not required due to single comparison.
$: Scenario where the p value remained significant even after adjustment for multiple comparisons (Bonferroni’s Correction).
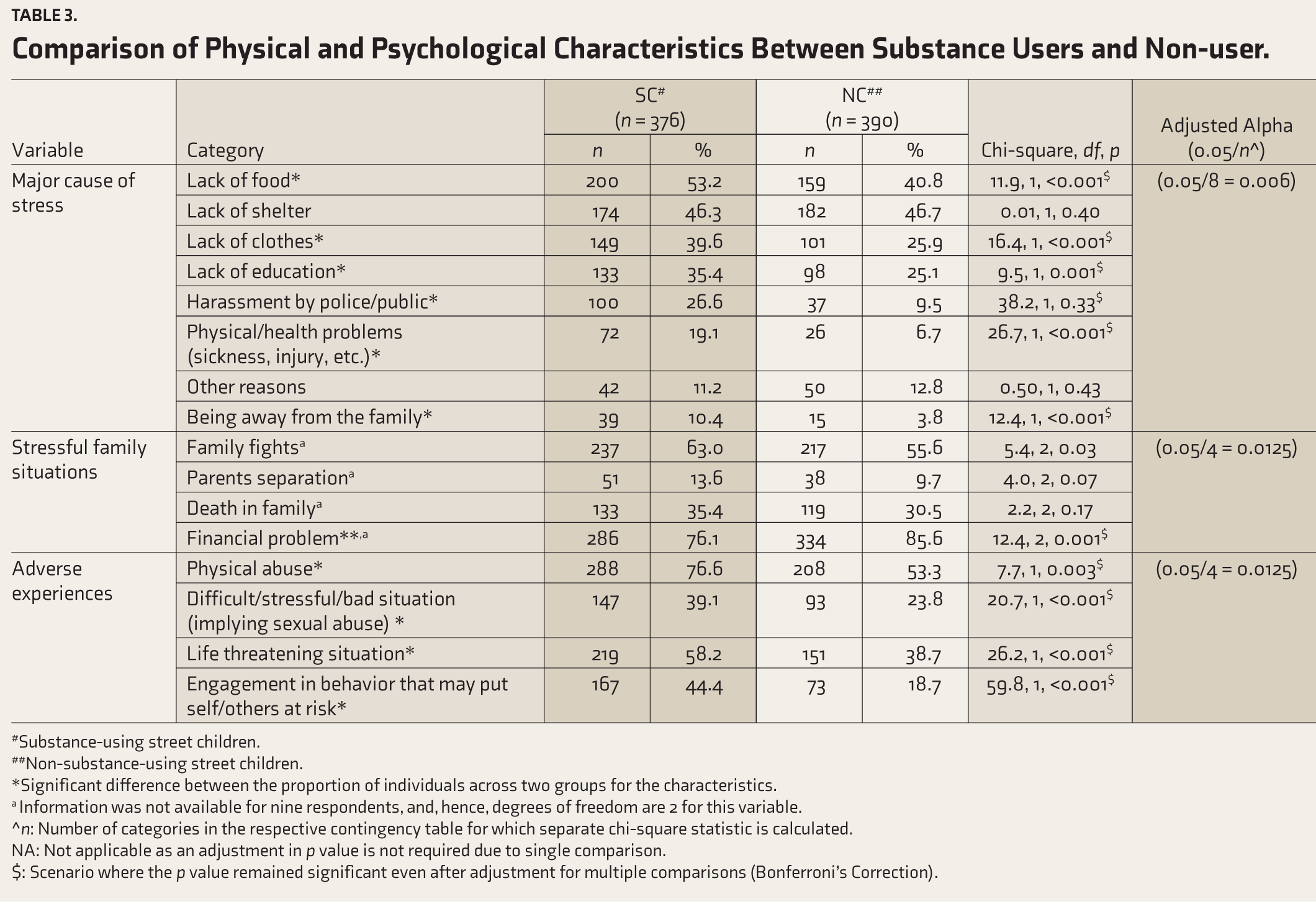
Comparison of Physical and Psychological Characteristics Between Substance Users and Non-user.
#Substance-using street children.
##Non-substance-using street children.
*Significant difference between the proportion of individuals across two groups for the characteristics.
a Information was not available for nine respondents, and, hence, degrees of freedom are 2 for this variable.
^n: Number of categories in the respective contingency table for which separate chi-square statistic is calculated.
NA: Not applicable as an adjustment in p value is not required due to single comparison.
$: Scenario where the p value remained significant even after adjustment for multiple comparisons (Bonferroni’s Correction).
Binary logistic regression analysis was performed to quantify the risk conferred by selected characteristics for the propensity towards substance use. The variables included sociodemographic, family and peer-related, stress, physical and psychological health-related characteristics. In the regression analysis, the last one-year substance use in any form was the dependent variable (0: NC, 1: SC). The independent variables were extracted from the complete dataset. The list of potential risk factors was used to develop the model which has interpretative value and good convergence in terms of stable parameter estimates. Allowing variables in their raw form would have distorted the estimates of parameters in the regression analysis due to low cell counts. Therefore, the selected variables were re-categorized appropriately from their original form for developing the univariate and the multivariable model. Our consideration for selecting the levels of the independent variable was based on the known factors predisposing to substance use based on the literature and the consensus by the authors. The regression model was developed by the stepwise approach. The threshold level of significance (i.e., of p value) as a criterion to include a covariate in the multivariable analysis was considered as less than 0.25.22,23 This is preferred because consideration of a conventional level of p as 0.05 often fails to identify variables of known importance. The rationale for the stepwise procedure was based on its robustness to provide the most optimal and interpretable model, as it allows the assessment of each independent variable at every step. 24 The overall fitness of the model was assessed by performing the Hosmer and Lemeshow test of goodness of fit test and bivariate cross-tabulation of the observed status of the respondent (substance users and non-users) and classified membership (substance users and non-users). 25
Results
Sociodemographic Characteristics
A total of 766 interviews were included in the final analysis. Among them, 375 (49%) were SC (any substance used in the last year), and the rest NC (those who had never used or not used any substance in the last year). A comparison of the sociodemographic differences between SC and NC users has been represented in Table 1. The mean (SD) age of the SC was 13.3 (2.6) years. The SC were older in age with 37.8% children aged ≥15 years as compared to 15.4% NC. Besides, 18.4% of the SC were in the age range of 7–10 years. The SC had significantly more males (93.4% vs 75.6%). The information on sex was not available for 15 children.
The percentage of NC who slept at home was significantly higher than those who were SC who slept on locations like streets/footpaths/under the bridge, on railway platforms/bus stations, or in shelters. Time spent on streets was higher in SC. A higher proportion of SC were spending time on railway platforms/bus terminals and worship places.
Both SC and NC reported being on the streets mainly due to poverty. A major percentage of SC mentioned peer influence, family conflict, and abuse/violence by parents /others to avoid school and being orphaned as reasons for being or for spending time on the streets. In comparison, a higher proportion of NC mentioned that they were on the streets to support their families who also lived on the streets.
Though a large percentage of children in both groups attended non-formal education (NFE) classes, a higher percentage of NC attended school. The reasons for dropout reported more often among SC included lack of interest in studies, drug use, inability to afford schooling, academic difficulty, being beaten up or scolded by teachers, and bullying by peers. More than 30% of SC responded in the affirmative when asked if they would like to attend if given an opportunity to attend school and skill training.
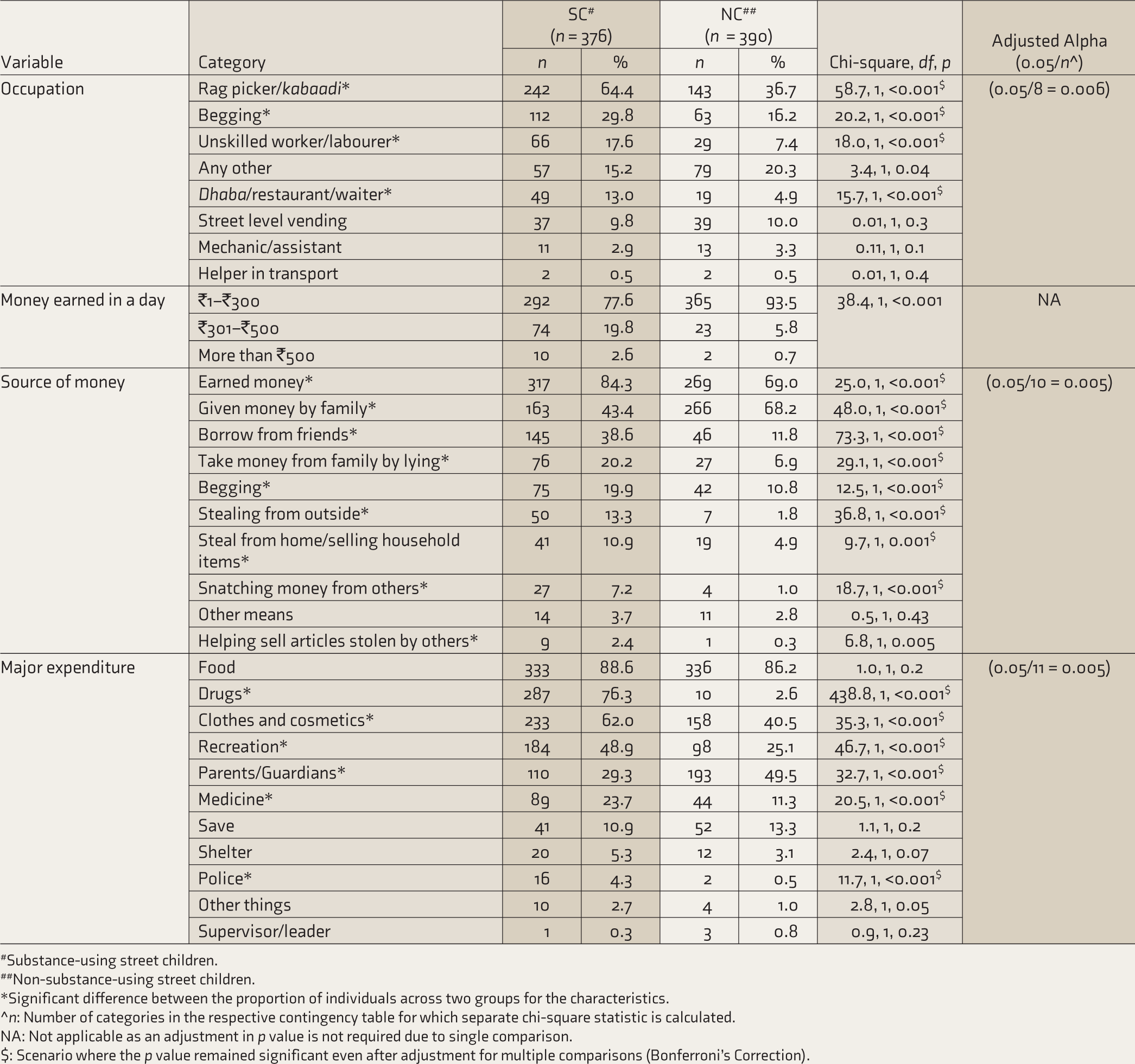
A significantly greater proportion of SC was employed, and this group was more often involved in rag-picking, begging, unskilled work, and working in hotels than NC. More substance users earned money, and they also earned more money in a day. A smaller proportion of SC reported being given money by the family compared to NC. More SC reported borrowing from friends, taking money from family by lying to them, begging for money, stealing from outside or from home, selling household articles, snatching money from others, and helping sell articles stolen by others. However, besides drugs, SC were spending more money on clothes, recreation, medicines and to give to police, while a smaller percentage gave money to parents/guardians as compared to NC.
Family- and Peer-related Characteristics
While family members of most SC lived in Delhi, a higher percentage of SC reported that their family was outside Delhi. A larger percentage of SC (15.2%) reported not being in contact with their families in the past year. Most NC reported that their family was looking after their basic needs, but half of the SC reported that the family did not look after their basic needs, and this difference was significant. Almost half of them also thought that the family was not concerned about how they spent their time. More NC reported that the family was aware of and concerned over their whereabouts. Among SC, 75.3% had been beaten up or verbally abused by their family, which is significantly greater than non-users. The temporal relationship of this abuse with substance use was not inquired. A significantly higher number of substance-using children reported substance use among family members and friends. A higher number of NC reported having close friends who did not use substances (Table 2).
Stress, Physical, and Psychological Health
Although both users and non-users reported multiple psychosocial stressors, a significantly greater number of SC reported, as major causes of stress, a lack of food, clothes and education, harassment by the public/police, health problems, and being away from family. The SC also had greater financial problems in the family. They also reported having significantly greater adverse life experiences like physical and sexual abuse, involvement in life-threatening situations, and engaging in behaviors that may put themselves and others at risk (Table 3).
Family and peer-related factors significantly associated with SC were families living outside Delhi and having no/infrequent contact with them, perception that their basic needs were not taken care of by their families, frequent family fights, financial problems, physical and verbal abuse, substance use in the family, and close association with substance-using peers. Police and public harassment, along with adverse life experiences (sexual abuse, threat to life, and engagement in risky behaviors), were significant social factors associated with SC. Older age, male sex, living outside the home, dropout from school, earning money, greater daily income and illegal activities were some sociodemographic factors significantly associated with SC.
Factors significantly associated with NC included younger age, living with parents, poverty, lower daily income, unemployment, contributing to family finances, family residing in the same city, frequent contact with family members, and close association with non-substance-using peers.
Regression Analysis
The bivariate association significantly differed across all sets of considered factors (Table 4). The substance users were in significantly greater proportion male (users: 0.54/non-users: 0.45), living outside (0.58/0.42), earning through illegal sources (0.79/0.21), neither being in contact with family (0.86/0.14) nor being cared for by the family (0.78/0.22), having greater substance use in the family (0.52/0.48), having more of substance-using peers (0.68/0.32), having no non-drug using peers (0.73/0.27), and lacking basic amenities (0.51/0.49), as compared to non-substance users.
The rate of substance use was 49%. In the multivariable model, increasing age [Odds Ratio: OR (95% Confidence Interval)] [1.22(1.12,1.33)], male sex [4.34(2.28,8.26)], lacking psychosocial support from family/relatives [3.27(1.84,5.80)], earning from illegal sources, [3.04(1.75,5.29)], family use of substance [2.59(1.38,4.89)], substance-using peers [29.86(14.38,62.01)], no non-drug using peers [2.35(1.46,3.79)], and not possessing basic amenities [2.26(1.31,3.93)] were the significant factors associated with substance use in past one year. On the other hand, not working was found to be protective [0.31(0.17,0.58)]. The model adequacy was also good as the results under the Hosmer and Lemeshow Test of Goodness of Fit were statistically insignificant [(c2, df, p = 7.0, 8, 0.53)], with a classification accuracy of 82.2%. This indicates that approximately 8 in every 10 street children (either substance users or non-users) were correctly classified as users or non-users by the multivariable model developed.
Regression Analysis with Independent Factors Associated with Substance Use.
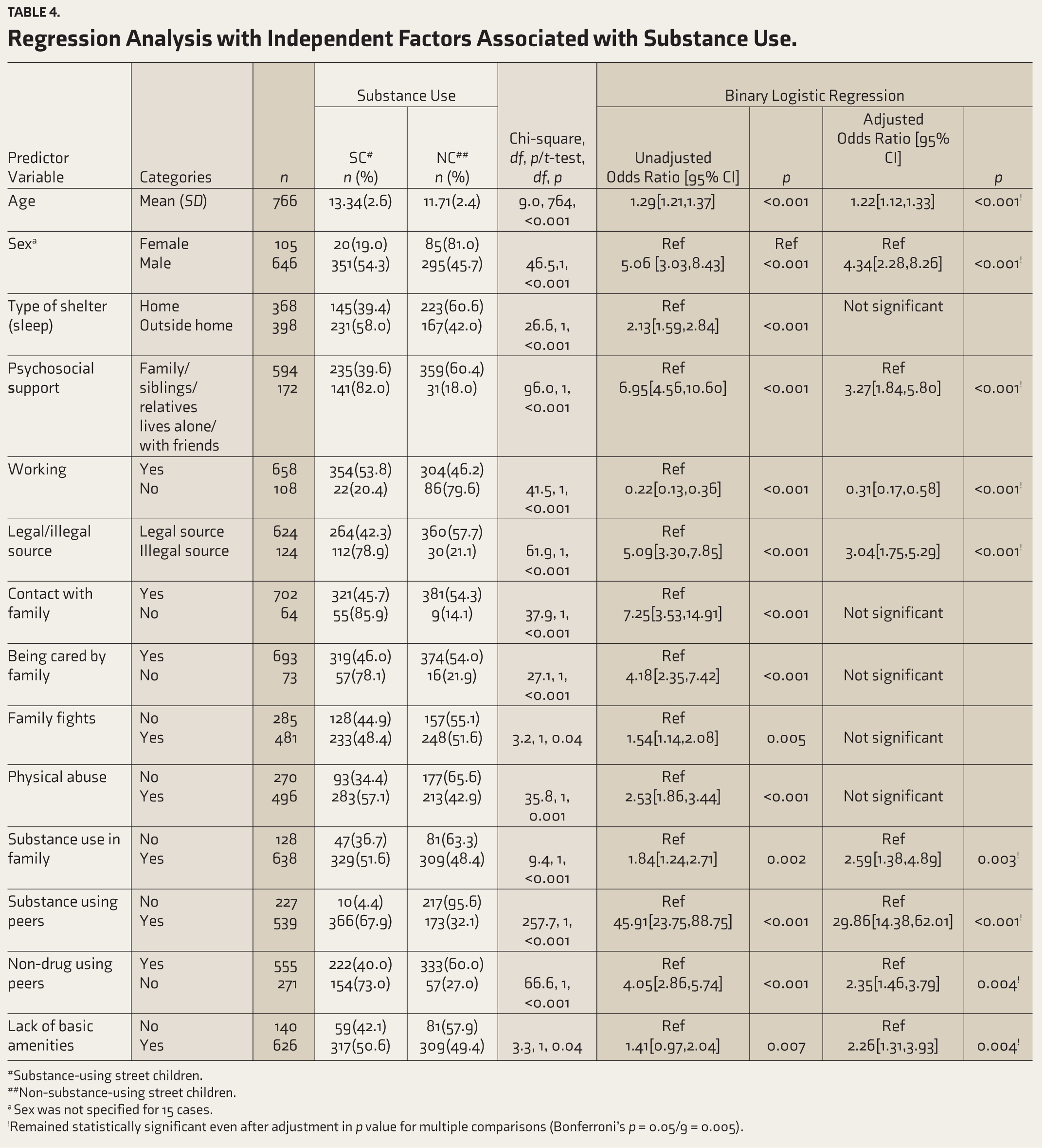
#Substance-using street children.
##Non-substance-using street children.
a Sex was not specified for 15 cases.
!Remained statistically significant even after adjustment in p value for multiple comparisons (Bonferroni’s p = 0.05/9 = 0.005).
Discussion
In the present study, the prevalence of substance use among 766 street children was 49.0% (376/766). This unweighted prevalence was well within the range of 40–70% from previous studies among street children in India.1,26 The variability in rates could be due to the use of non-representative sampling in the other studies.
The characteristics of street children aligned with other reports, with the majority being males, location of stay on the street, and experience of physical abuse and substance use by family members and peers. 10 Some of the SC were very young (<10 years), as has been reported in other studies on street children. 15
The available evidence on the characteristics distinguishing a SC from a NC is scanty except from one study from Guwahati, Assam. 26 Increasing age was strongly associated with substance use in our bivariate analysis. This observation corroborated findings from Assam, Bangalore, and Mumbai, where the prevalence of substance use in older children was higher than in younger age groups.15,26,27 Substantial research indicates male sex to be a significant risk factor for substance use, and this study’s bivariate analysis echoed the available evidence from India.15,16,27 A higher percentage of SC were employed and had larger sums of money in hand but contributed lesser money to family finances. This can be explained by the need for money to procure substances, leaving little to save or contribute to family expenses. This need also explains a greater engagement in illegal activities among children who use substances.16,18
This study found many factors associated with substance use by developing a multivariable model. However, since the study did not explore the temporality of the characteristics with substance use, it is difficult to comment about the nature of this association in terms of causality.
Studies have associated poverty and lack of basic amenities with substance use.14,16,28 Earlier studies among adolescents and young adults have reported similar adversities in daily living and family environments that formed risk factors for the initiation of substance use in this young population. 27 Children who grow up in a family with nourishing and supportive relationships, regular monitoring, some rule setting, and discipline possess greater skills at adjusting to society and are at a lower risk of initiating substance use. 29 Also, absence of parents, stressful family environment, domestic violence, and physical abuse have been reported as significant risk factors for psychological disturbances and substance use among adolescents and early adults. 29 Many studies have reported substance use by family members as a risk factor for substance use among adolescents. Strategies that focus on strengthening street children’s links with their families and fostering stability in family relations are vital for prevention. This may be challenging in such a vulnerable population. A pragmatic approach to addressing this issue would be information education communication (IEC) activities especially directed toward the street children and their family members and family interventions.
Some associations significant in univariate and bivariate analysis failed to reach the significance level in the multivariable model. The variables that were significant in bivariate analysis but did not emerge significant in multivariable analysis were “living outside,” “not being in contact with family” and “not being cared for by the family.” The response on some variables was low, and their relative contribution could not be captured in the multivariable model. A stepwise regression method was utilized for developing the multivariable model. In stepwise regression procedure, the relative contribution of each considered variable is assessed at every step by setting the probability of entry (0.05) and exit (0.10) in the model. This enables arriving at the most optimal model by discarding variables that do not fulfil the probability level of entry (0.05–0.10). It might also be the case that some of the variables turned out to be statistically insignificant due to confounding effects. Some intervening variables may have partially obscured the association of a particular variable with substance use. Such hidden associations would have been unraveled by applying more advanced statistical analysis, such as the mediation analysis. However, this was not the focus of the present study. Nonetheless, the overall fitness of the multivariable model was good, as evident from the classification accuracy and test of goodness of fit.
The limitation of the study is that the temporality of the associations cannot be commented upon. Its main strength is a large sample size and inclusion of girl children too. As the study participants were selected using RDS, the findings are generalizable to the street children in NCT Delhi.
Conclusion
The study demonstrated a significant association of substance use with the following sociodemographic and peer-, family-, and stress-related factors: increasing age, male sex, lacking psychosocial support from family/relatives, earning from illegal sources, family use of the substance, substance-using peers, no non-drug-using peers, and not possessing basic amenities.
These findings call for consideration while planning effective preventive initiatives for substance use among street children and therapeutic interventions for substance users. Some challenges include difficulty accessing street children and poor treatment seeking by those using substances.
Footnotes
Acknowledgements
The participating officials from different Non-government Officials (NGOs): Butterflies, Childhood Enhancement through Training and Action, Don Bosco Ashalayam, Prayas, Saalam Baalak Trust and Society for Promotion of Youth and Masses) are duly acknowledged.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the Ministry of Social Justice and Empowerment, Government of India, and commissioned by the Department of Women and Child Development, Government of National Capital Territory of Delhi. ID: IEC/NP-253/03.07.2014, RP-15/2014. The funding agency was not involved at any stage of data analysis for the present work.