
Abstract

Obsessive-compulsive disorder (OCD) is a prevalent, chronic mental illness with a substantial negative impact on the quality of life. 1 Pharmacotherapy and Cognitive Behavioural Therapy (CBT) are effective first-line treatments for OCD. 2 In practice, the two are often used simultaneously, specifically in patients with severe OCD. 2
Compared to pharmacotherapy, CBT demands greater involvement from patients, carers, and treaters alike. Behavioural interventions such as Exposure and Response Prevention (ERP) 3 are integrated within the CBT framework, aiming at the extinction of learned compulsive responses and habituation to anxiety while facilitating guided discovery and correction of cognitive distortions. 4 CBT’s resource- and time-intensive nature makes it less accessible outside large metropolitan cities. This may result in a substantial burden to patients who must travel long distances.
The coronavirus disease (COVID-19) pandemic has accelerated the adoption of online platforms for delivering diverse healthcare services, including tele-mental health and tele-psychotherapy. 5 There is limited research from resource-constrained settings on the effectiveness of delivering psychotherapy using online platforms. 6 In this letter, we seek to report the successful delivery of CBT for OCD using a hybrid approach consisting of 1:3 fixed-ratio in-person and online psychotherapy sessions.
A young female presented with a two-year history of repeated hand washing and taking an inordinate amount of time to complete daily activities. After a detailed interview and examination, a diagnosis of OCD with fair to good insight (6B20.0 ICD 11) was considered. Yale-Brown Obsessive Compulsive Scale (Y-BOCS) 7 symptom checklist revealed current obsessions in the contamination domain relating to bodily waste or secretions and environmental contaminants. Excessive ritualized hand washing and excessive showering were noted to be the current principal compulsions. Additional symptoms included a compulsive need to remember, symmetry/ordering and pathological doubts and checking but these were not in the forefront.
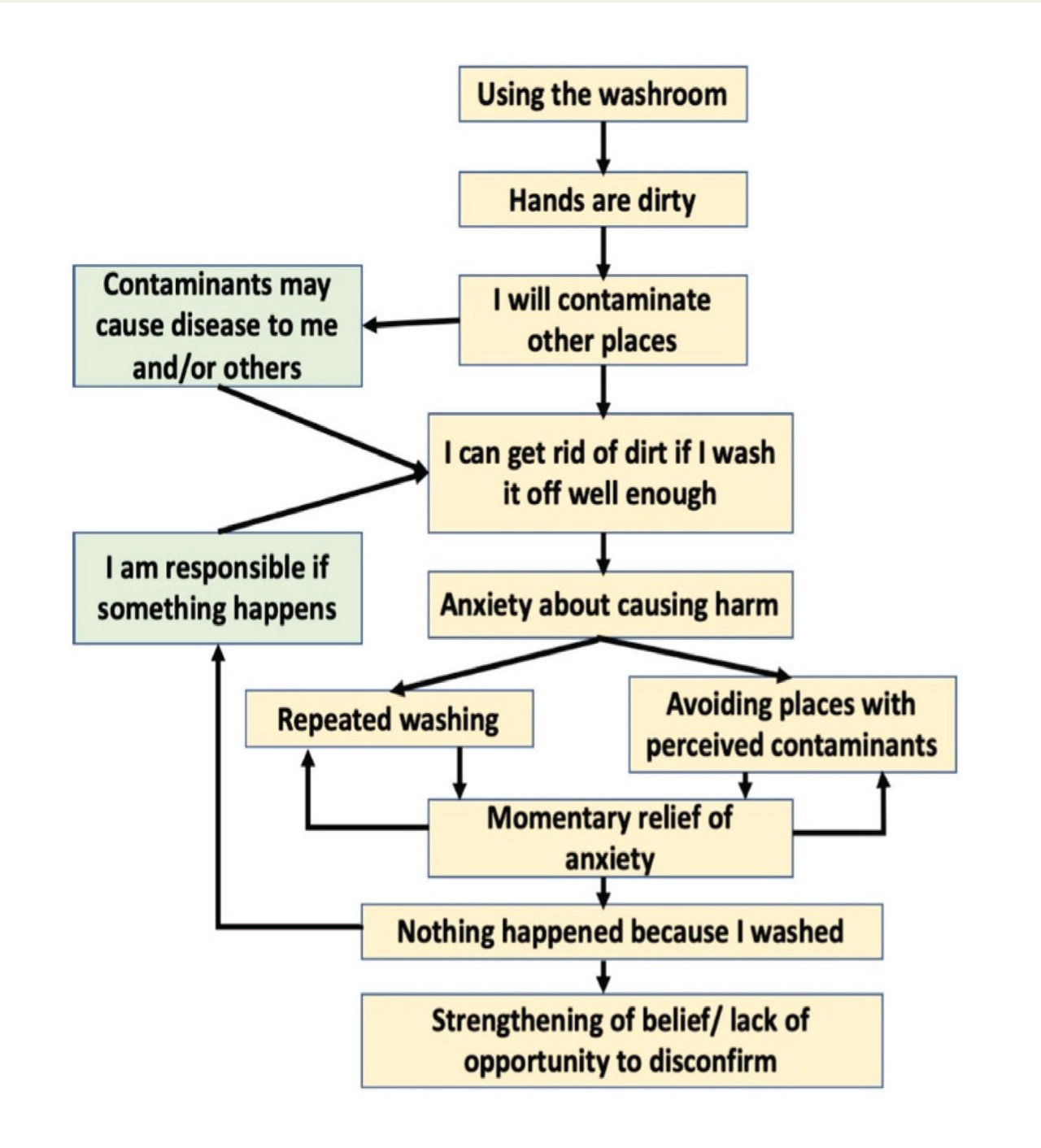
YBOCS scores of 18 and 17 were obtained for obsessions and compulsions, respectively, suggesting the presence of severe OCD 8 further qualified by fair insight and prominent avoidance behaviours. Clinical Global Impression severity score of 4 corresponding to moderate to severe symptoms, and limited functioning was noted. Patient’s presenting symptoms were conceptualized using the Cognitive Behavioural framework of OCD proposed by Salkowski and formulated using the template adopted from Reddy et al. 9 (Figure 1).
Cognitive Behavioural Formulation Used in Ht-CBT Module for the Principal Obsession and Compulsion in the Contamination-washing Domain.
Hybrid tele-CBT (Ht-CBT) Intervention
Rationale
Considering the severity of the patient’s OCD a combination of pharmacotherapy (Tab Fluoxetine 20 mg increased up to 80 mg) with CBT was mutually agreed upon. Accessing weekly therapy was a significant challenge as it required the patient to travel more than 12 hours to reach the hospital. After discussion and consent from the patient, a hybrid mode of in-person and online therapy in a fixed ratio of 1:3 was agreed upon. This was largely due to pragmatics as once a week session was deemed necessary and the patient could visit the hospital once every month.
Structure
Both in-person and online sessions were planned for 45–60 minutes duration. Demonstration of ERP principles and initial exposure to a novel obsession-compulsion targets were planned during in-person sessions. During online sessions, continued practice of exposure was ensured along with cognitive restructuring. For online behavioural experiments, the patient’s mother was identified as the co-therapist with patient’s consent. The co-therapist was actively engaged through both in-person and online sessions, including initial psychoeducation.
Outcome
By the completion of 18 Ht-CBT sessions including four in-person visits and 14 online sessions, the patient experienced significant improvement in OCD. YBOCS scores reduced to 3 each on both severity subscales and CGI improvement score was 5 suggesting much-improved state. The patient gained considerable insight and was able to recognize and label intrusive thoughts, ideas, and fears. She resumed her educational pursuits and successfully engaged in it with minimal interference from OCD symptoms. The improvement was maintained, and the patient continued to be in remission 8 at six months post-intervention. The patient was adherent to pharmacotherapy during CBT which is likely to have contributed to the improvement.
This report highlights the successful delivery of CBT using an innovative approach blending in-person and online psychotherapy. While this appears to be a pragmatic choice, there are few reports utilizing such approaches. Some emerging evidence supports the efficacy of telehealth approaches in OCD. 10
Ht-CBT offers several advantages. It was found to be convenient and acceptable by the patient and the therapist. For the patient, it reduced the cost and burden of frequent travel translating to a reduction of INR 9000/month in treatment-related expenditure. The reduced burden further enhanced the patient’s motivation and ensured adherence to in-person sessions.
The in-person sessions allowed application of challenging aspects of CBT such as the initial demonstration of ERP principles, and exposure to triggers eliciting most distressing obsessions. Periodic in-person contact permitted better expression of therapist-related non-specific factors such as empathy, positive regard, non-judgmental attitude, hope, and expectation. Some patients in traditional in-person CBT may fail to develop sufficient distress during hypothetical exposure experiments or display covert compulsions undermining both extinction and generalization. The online sessions allowed design of ERP experiments in patient’s natural environment where she most frequently experienced her OC symptoms. Qualitatively, a better rapport and engagement in therapy were perceived both by the therapist and the patient during in-person sessions possibly due to the absence of technical difficulties encountered in online sessions. An empathizing co-therapist, in the present case the patient’s mother, played a crucial role during the initial online sessions by serving as a bridge between the therapist and the patient.
A significant challenge during the online sessions included disruptions in audio-visual communication due to problems with internet connectivity. In the current case, the therapist had access to state-of-the-art equipment, custom-designed web meeting platform, and soundproofed room for tele-consultations. The patient attended most of the online sessions using a mobile device with limited data speed. During more than half of the online sessions (9/14), a temporary disruption in connectivity was experienced and the therapist and the patient had to log in to the same session multiple times. These disruptions could potentially contribute to a loss of motivation and/or frustration for both the therapist and the patient. In the absence of a willing co-therapist, the patient may also face the risk of not completing ERP experiments or experiencing severe anxiety in the absence of a therapist’s neutral support.
In summary, Ht-CBT is a promising option to effectively deliver CBT for OCD with significant advantages in resource-constrained settings. While this strategy appears to be only a pragmatic choice there is a definite need for additional research on the promotion and regulation of use of tele-platforms in therapy. From the limited experience arising out of this case report, we note that patient factors such as ease of using teleconsultation technologies, empathizing co-therapist, and adherence despite temporary disruptions may play a vital role in successful adoption of tele-consultation methods. Further systematic investigations are needed to delineate client suitability including symptom profile and co-morbidity that may delineate the indications-contraindications for tele and hybrid approaches. Furthermore, differential outcomes in comparison with traditional in-person CBT approaches need systematic evaluation.
Footnotes
Acknowledgements
We thank the patient for her consent for publication, and a review and approval of the report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.