
Abstract
Background:
Cannabis use among youth is increasing; this study aimed to assess college students’ knowledge, attitude, and expectancies toward cannabis use.
Methods:
Cross-sectional survey using standardized tools among undergraduate and postgraduate college students in urban Bangalore, India (N = 405).
Results:
Ten percent reported past three-month cannabis use, with 1% reporting daily use. Users were significantly older (median age 21, IQR 22,20 [vs. 20, IQR 21,19], p < .001) and belonged to families with higher monthly incomes (p = .02). Use was significantly higher among males than females (65.9% vs. 34.1%, p = .006) and postgraduate students than undergraduates (51.2% vs. 48%, p = .001). Users were also significantly more favorable toward cannabis use (median score 4, IQR 6,2 [vs. median 3, IQR 4,2], p = .005) and had more positive expectancies from use (median score 2, IQR 3,2 [vs. median 2, IQR 2,0], p = .001). Nearly 30% were unaware that cannabis can affect a person’s ability to drive safely or that it can affect executive functions, including academic performance. Over one-third were unaware of the current legal status of cannabis in India. Overall, 36%, 25%, and 17%, respectively, said that cannabis use is safe when used for recreational purposes, cannabis should be legalized as it helps to relieve stress, and cannabis use among youngsters should be acceptable in society as it is “part of college life.”
Conclusion:
Findings build on existing literature on cannabis use among college youth in India, which can guide preventive interventions and policies for this vulnerable group.
A significant proportion of the students were unaware of the health harms of cannabis use, including impaired academic performance and driving ability. A significant proportion believed that cannabis use should be more acceptable and legal, as it is a stress reliever and part of college life.Key Messages:
The rising use of cannabis products has become a global concern. According to the WHO, cannabis has become more closely linked to youth culture, with the age of initiation being usually lower than for other drugs. In prior studies from overseas, cannabis was one of the most frequently used drugs on college campuses, with prevalence ranging from 44% to 55%.1–3 An alarming concern with the use of cannabis is the decreased perception of associated risks, positive expectancies from use, and perceived benefits from use.2,4 The concerns surrounding cannabis use are different from those related to other psychoactive drugs. More importantly, the use of cannabis has been the subject of debate regarding safety risks versus benefits, including medical uses (unlike substances such as alcohol and tobacco). Several states in the United States have legalized cannabis use for medical and recreational purposes, with consequent prevention, management, and policy issues.
In India, cannabis (known in the vernacular as ganja or bhang) holds cultural significance because of its use during festivals and rituals. Cannabis use rates ranging from 6.8% to 36% have been reported among college students in India,5,6 with poor academic performance, school drop-out, and cognitive impairment noted among users.7,8 On the other hand, previous authors from India have documented an increasing trend to focus on the benefits of cannabis, which can decrease the risk perception about cannabis use among college students. Prior studies among college students in India have reported decreased perceived risk or ambivalence about harm from cannabis use.6,9 As in overseas studies, students have reported positive expectations from use, such as relaxation, stress relief, and the ability to work responsibly.6,8,9 At the urban community health service run by the present authors, young students regularly ask “Cannabis is legalized in other countries; is it beneficial to health? Is cannabis use legal in India?” “Can we use cannabis instead of tobacco, as tobacco is harmful, whereas cannabis is safe and helps to concentrate,” “Does cannabis relieve pain?” etc. A recent article argued about the need for legalizing cannabis use in India, as the country stands to benefit in terms of the medical uses of cannabis, revenue for the government, and decreased unemployment and crime rates. 10
The above is in the face of growing scientific literature on the adverse impact of cannabis use, including various respiratory illnesses and infections, cardiovascular disorders, cognitive impairment, mental health issues, poor academic performance, impaired judgment, high-risk behaviors, impaired driving ability, and increased risk of motor vehicle accidents.2,4,11–15 Furthermore, youth is a period of continued brain growth and change when the brain is most sensitive to the detrimental effects of psychoactive drugs, including cannabis, so young people are especially vulnerable to these harmful effects.14,16
Given the various pressures and challenges during this phase, college students are an important group to study, which can often cause them to use maladaptive coping measures, including psychoactive substance use. The present study was undertaken against this background among college students, and the objective was to explore their knowledge, attitude, and expectancies regarding cannabis use. While expectancies related to cannabis use have been documented in prior literature, 9 the current study also reports the knowledge and attitude of college students toward cannabis use. The findings can add to the current understanding of cannabis use among young people in India and guide preventive interventions and policies for this vulnerable group.
Material and Methods
Setting, design: The Institute Ethics Committee approved the study. The study design involved a cross-sectional survey of knowledge, attitudes, and expectancies concerning cannabis use among college students in South Bangalore.
Sample size: The sample size was estimated as follows: Assuming that 50% of the students will have adequate knowledge about the health impact of cannabis use, for a precision of ±6% at a 95% confidence level, the minimum required sample size is 267. Considering the design effect of 1.5, the final sample size was estimated at 400.
Recruitment: Students were eligible to participate in the study if they were studying undergraduate/postgraduate courses in the respective colleges and could speak, read, and write English. For recruiting the students, two separate lists of colleges (government and private) in South Bangalore were made. Using a table of random numbers, five colleges were randomly selected from the lists (three private and two government). Formal permission was obtained from the college authorities for conducting the study. Next, in each of the five selected colleges, two separate lists (one for undergraduate and one for postgraduate) were made with the help of the college administrators. Eighty students were chosen from each college using a table of random numbers, ensuring that undergraduate and postgraduate courses were represented in the group, achieving a final sample of 405 (85 from one college). These students were given a brief introduction to the study and its purpose, and a copy of the Informed Consent Form was given to them. They were requested to go through and sign the Form if they consent to participate in the study. The data collection period was between October 27 and November 29, 2021.
Measures
The Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) (WHO 2002) 17 : Baseline information was obtained from the students, including their drug use, assessed through the ASSIST. A risk score for each substance groups those with substance use into “low,” “moderate,” or “high” risk. The risk score determines the level of intervention recommended.
Knowledge assessment questionnaire: It was developed to assess the students’ knowledge regarding cannabis use. The Questionnaire comprises 15 multiple choice questions related to the health impact of cannabis use on different body systems (e.g., lungs, brain, heart, impact on executive functions, driving ability) and current legal status in India (e.g., NDPS Act, fines). Each item had one correct answer, which received a score of 1. The maximum score was 15, with increasing scores reflecting better knowledge.
Attitude assessment scale: It was developed to assess the students’ attitudes toward cannabis use. The Scale consists of 10 items in a Likert-style format (e.g., “Cannabis use is just for recreation/time pass, there is no need to view it as a big issue,” “Legalisation of cannabis for recreational purposes should be supported”), with responses ranging from “strongly disagree” (scored 0) to “strongly agree” (scored 3). Thus, the total score ranges from 0 to 30, with increasing scores reflecting a favorable attitude toward cannabis use.
The Marijuana Effect Expectancy Questionnaire (MEEQ-B) 18 : It is a standardized questionnaire used to assess the students’ expectancies regarding cannabis use. It is a five‑point Likert scale with six items in which the students are required to record their responses in terms of how they think cannabis affects the user, ranging from “disagree strongly” (scored 1) to “agree somewhat” (scored 5) (irrespective of whether they have tried cannabis or not). The MEEQ-B has two components/scales: MEEQ-Bp (items 2–4), reflecting positive cannabis expectancies, and MEEQ-Bn (items 1–6), reflecting negative expectancies. The higher the score on a scale/component, the higher the expectancy. The average score of a scale/component is used for interpretation. The MEEQ-B has been used in prior Indian studies.9,19
The items in the Knowledge and Attitude tools were included based on a literature review, the research team’s experience with college students, and consultations with experts in psychoactive substance use disorders. Furthermore, the items were guided by thematic content analysis of focus group discussions conducted with the college students, which explored their perceptions about cannabis use patterns, their beliefs about use, medical use, and legalization, and the potential impact of cannabis use on academics, relationships, and health.
The tools were content-validated by six experts in addiction disorders and their management (Addiction Medicine, Child & Adolescent Psychiatry, Clinical Psychology, and Psychiatric Social Work). The experts rated each item in the respective tools in terms of their relevance and clarity on a scale of 0–3 (0 = not relevant/clear, 1 = highly relevant/clear). Further, the experts were also requested to provide their remarks on each item, supporting their rating and suggestions for modification/improvement. After the experts’ validation, some items were revised/dropped, and some new items were added. The revised tools were re-sent to the experts for any further comments. The tools were pretested on 50 college students, and minor changes were made in the wording of a few items based on the students’ feedback about their comprehensibility and language clarity. The tools were then finalized for use in the final survey.
Statistical analysis: Data from the survey were checked, entered, and verified again for accuracy. Summary statistics were computed for baseline information. The Spearman’s rank correlation coefficient was computed to assess the association between the key variables (knowledge, attitude, expectancies). The Mann–Whitney test examined key variable scores (knowledge, attitude, expectancies) differences by discrete baseline variables (gender, type of family, course of study). Analyses were conducted using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, NY, USA).
Results
Description of the sample: Mean age of the participants (N = 405) was 20.16 years (SD: 1.70), 55% were females, 94% were unmarried, 67% belonged to nuclear families, 70% were pursuing undergraduate courses, 74% were residing in Bangalore urban area, mean family monthly income was INR 56,700 (SD: 84,613) (approximately 696 USD).
Cannabis use: Ten percent of the sample reported past three-month use of cannabis, with 1% reporting daily use. Table 1 shows the differences between past three-month users and non-users. Briefly, cannabis users tended to be significantly older (p < .001) and belonged to families with higher monthly income (p = .02). Use was significantly higher among males, compared to females (65.9% vs. 34.1%, p = .006) and postgraduate students, compared to undergraduates (51.2% vs. 48%, p = .001). Users also tended to be significantly more favorable toward cannabis use (p = .005) and had significantly more positive expectancies from use (p = .001).
Comparison of Past Three-month Cannabis Users and Non-users by Key Study Variables (N = 405).
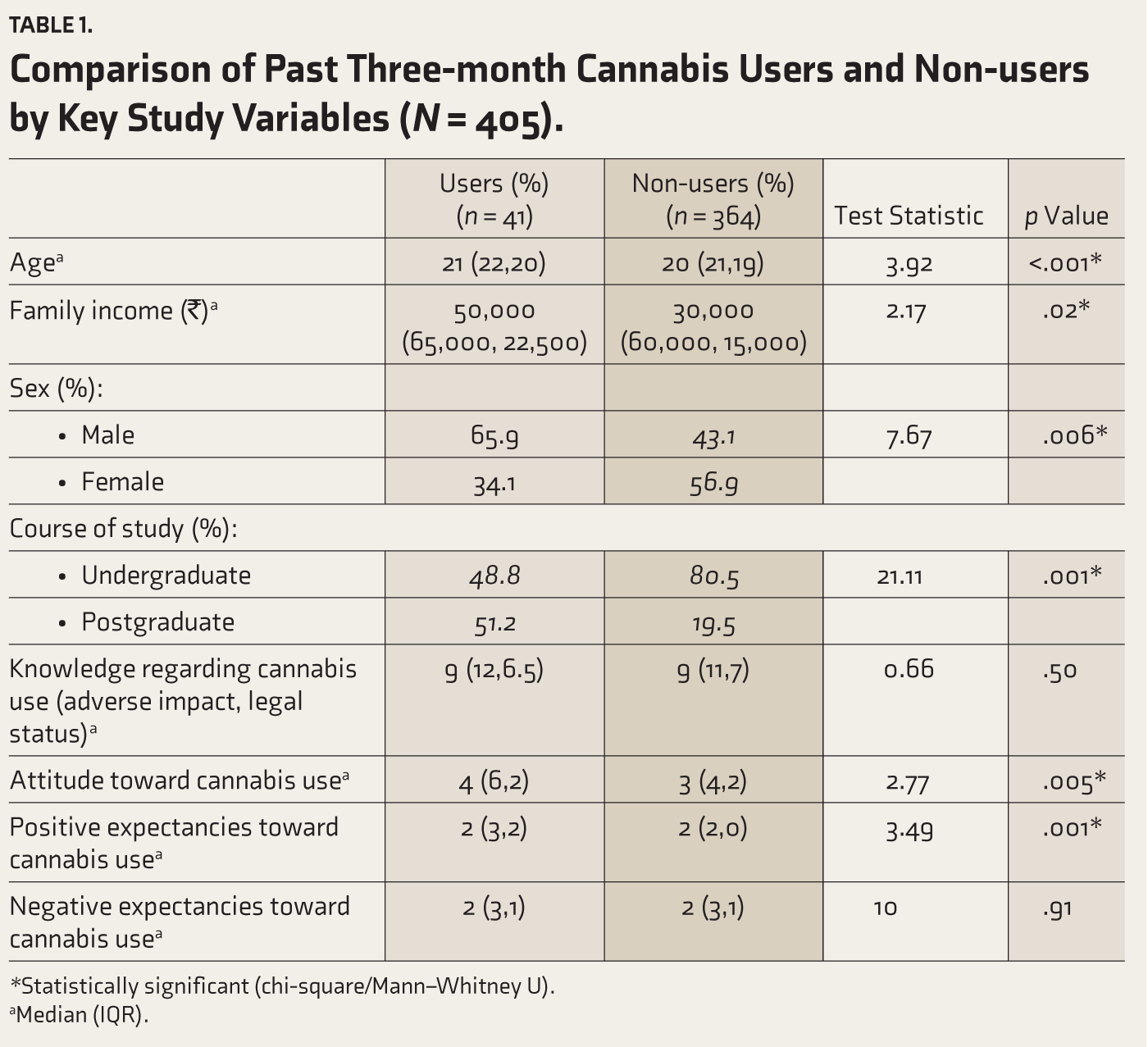
*Statistically significant (chi-square/Mann–Whitney U).
aMedian (IQR).
Source of information about cannabis: Forty-two percent of the sample said that they had seen cannabis-related content in movies or television programs, while 32% said that they had browsed the internet for information on cannabis products. Thirty-nine percent said they had obtained information about cannabis from their peers and 17%, from family members.
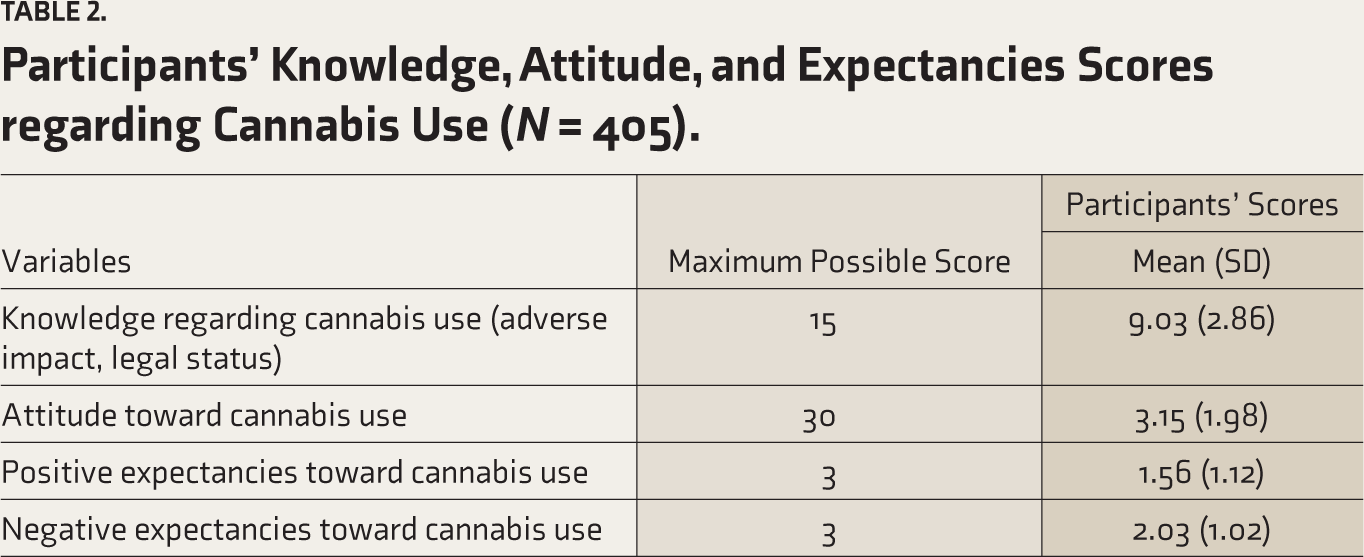
Knowledge, attitude, and expectancies related to cannabis use (Table 2): About knowledge, one-third to half of them were unaware of the various adverse health effects of cannabis. Nearly 30% were unaware that cannabis can affect a person’s ability to drive safely or that it can affect executive functions, including academic performance. Over one-third were unaware of the current legal status of cannabis in India.
Participants’ Knowledge, Attitude, and Expectancies Scores regarding Cannabis Use (N = 405).
About attitudes, 36% said that cannabis use is safe when used for recreational purposes, 25% opined that cannabis should be legalized as it helps to relieve stress, 17% expressed that cannabis use among youngsters should be acceptable in society, as it is “part of college life.”
Participants’ responses on the MEEQ-B (item-wise) appear in Table 3. Since responses for “disagree somewhat” and “agree somewhat” were too few, and there was no endorsement on the “uncertain” category, they are presented as the percentage of students who “Agreed” or “Disagreed” with each item on the MEEQ-B.
Participants’ Expectancies with Regard to Marijuana Effects (N = 405).
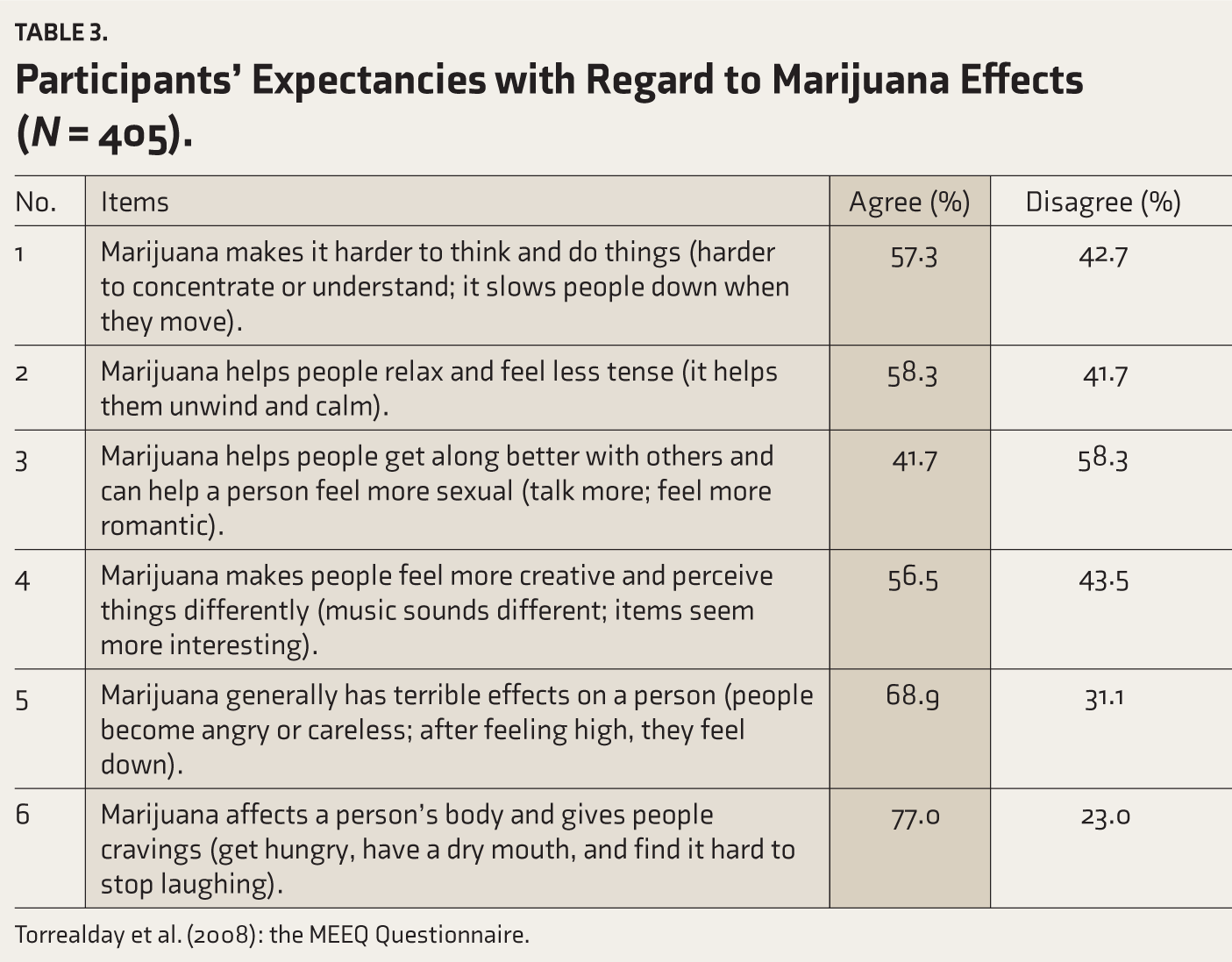
Torrealday et al. (2008): the MEEQ Questionnaire.
Relationship among key variables: Knowledge scores were negatively correlated with attitude scores, implying that an increase in knowledge regarding the harmful effects of cannabis use was associated with a significantly less favorable attitude toward use (r = –0.154, p = .002). Further, the mean knowledge score was inversely correlated with mean MEEQ-Bn scores, indicating that an increase in knowledge was associated with negative expectancies from the use of cannabis (r = –0.32, p < .001).
Discussion
The present study reports the knowledge, attitude, and expectancies about cannabis use among college students in urban Bangalore. In India, prior authors have documented the use of cannabis among young people. These studies, although sporadic, have reported important trends in cannabis use among youth in the country concerning prevalence, reasons for use, and other associated factors.5,7,9 Some of these trends are noteworthy and in line with the present study’s findings. For instance, in the present study, the overall knowledge and attitude scores indicated that the students seemed fairly knowledgeable about the harmful effects of cannabis use and were not very favorable toward use. However, most of the current sample were unaware that cannabis use can cause driving impairment and lower academic performance. Similar findings were noted in a prior study among college students in Mumbai, where about half were unaware that cannabis use could cause cognitive and behavioral impairment. 9 Further, in the present study, a significant proportion of students opined that cannabis use is safe for recreational purposes and that cannabis use is part of college life, which helps them to relax, be more creative, and feel more romantic. Similar findings were noted in studies from overseas where recreational motives influenced use, and positive perceptions were noted among cannabis users, including relief from anxiety and stress.2,16 Prior studies among college students from India also had noted positive expectancies as well as ambivalent attitudes from use.8,9,20
There can be several reasons for favorable attitudes or positive expectancies from cannabis use. For example, prior studies found that the students believed/used cannabis for relaxation, stress relief, enhancing creative abilities, better socialization, and increasing sexual desire.8,9,20 Prior authors from overseas and India have also highlighted the role of social motives, peer influence, and lack of adequate supervision, which can fuel cannabis use for various reasons.6,21 Furthermore, such positive attitudes or expectancies can place individuals at a higher risk for use. This was also reflected in the present study, where cannabis users had significantly more favorable attitudes toward cannabis use and had more positive expectancies from use. Prior literature has also documented positive expectancies and engagement in high-risk behaviors among cannabis users.2,14 It is also important to remember that inadequate knowledge can lead to more favorable attitudes and more positive expectancies from cannabis use. This was reflected in the present study’s findings, where knowledge about health harms was associated with a significantly less favorable attitude toward cannabis use and more negative expectancies from use. This fact can be very important when planning preventive interventions for this group.
One-fourth of our sample supported the legalization of cannabis, claiming it helps to relieve stress. Similar findings were found in a recent qualitative study among college students in urban Bangalore, 20 where the students said that cannabis and tobacco go hand in hand, that there is “research evidence” about the medical benefits of cannabis, and that its use should be legalized. These findings are important, given the debate surrounding the legalization of cannabis use worldwide, with countries like Uruguay, Canada, and several states in the United States having enacted laws allowing the use of cannabis for medical or recreational purposes. In general, public opinion on the legalization of cannabis use is increasingly becoming favorable, 4 which may be attributed to a growing literature alluding to the potential medical benefits of cannabis without exposing people to the health risks.14,22,23 Prior authors from India also have suggested that legalization can help curb young people from using unknown products. 6 However, research has documented the increasing use of cannabis among young people following legalization, with associated high-risk behaviors.3,4 There is also growing evidence of the significant negative impact of cannabis use on the education and career of young people through impairment of executive functions.2,4,7,8,14,24 Prior literature emphasizes that cannabis use during adolescence can cause long-lasting changes in brain functions, jeopardizing educational, professional, and social achievements. 14 The harms from use may also extend to others since there is an increased risk of accidents due to impaired driving ability.12,13
Another concern is the cannabis-related information available to young people via the media or online. For instance, in the present study, 42% had viewed cannabis-related content in movies or television, and more than one-third had browsed the internet for information on cannabis products. The influence of mass media on cannabis use and negative health outcomes in young people has been documented in prior literature. 25 In a study, the college students spoke at length about the influence of the media: “Today’s youth is educated and searches online. And there is a lot of information… including studies supporting the medical benefits of cannabis and that its use should be legalized….” 20
Given that prior literature in India focusing on awareness among youth with regard to cannabis use and associated risks is scanty, the current findings add to the literature and emphasize the need for targeted interventions for this group. However, this brings to question the content that should be included in such interventions and the strategies that should be adopted to convey this content. For instance, how does one convince youngsters to quit cannabis in the face of an onslaught of questions backed by purported claims or “research” about the benefits of use? In India, there has been a significant increase in the promotion of medicinal cannabis products, as in overseas, where prior authors have documented medicinal cannabis advertisement and marketing by medical cannabis dispensaries. 25 Further, considering that there are no clear-cut health warnings about cannabis use in India, the plethora of cannabis-related information on various platforms seems to be catching on among youngsters. College students asked the present authors why cannabis use should be restricted, particularly when alcohol and tobacco are legally available to the public despite their well-established health harms. They explained that in India, cannabis is part of the culture and that if cannabis becomes more acceptable in society, they can access it and benefit without worrying about punishment. The present study’s findings also reflect this, as the participants seemed ambivalent and divided regarding their knowledge of, attitude toward, and expectancies from cannabis use.
The above findings have several critical implications for planning preventive educational strategies for college students, a highly vulnerable group, given that they are going through a turbulent developmental stage of life, coupled with various academic and other challenges. First, there is a need for a balanced perspective about the potential adverse health impact of cannabis and an informed approach toward prevention and harm reduction. Specific interventions and youth awareness strategies to strengthen cannabis-protective behavioral strategies can reduce the quantity and frequency of use and minimize harm. 26 Second, planning youth awareness/intervention programs can help to increase knowledge about the health harms of cannabis and clarify any misconceptions that the students may have about cannabis use by providing authentic health information, which can, in turn, enhance youth health and safety. A prior study from India indicated that college students who were aware of the harmful effects and legal status were more motivated to quit cannabis. 9 Third, such awareness programs also need to consider any demographic trends associated with use (e.g., in the present study, cannabis users tended to be older, male, from higher-income families, and pursuing postgraduate courses). The finding that the cannabis users tended to be older or postgraduates could be because students may be non-users when they join college and gradually pick up the habit as they go through their courses of study due to various influences (e.g., peers). This points to the need for prevention/intervention programs to be introduced early as part of college student development initiatives. Fourth, the present findings can help sensitize college peer volunteers, teachers, and administrators regarding these trends among students and train them to identify cannabis use, provide necessary clarifications and advice, and make referrals as necessary. Fifth, the information can aid in developing and delivering primary prevention interventions through community youth outreach programs and incorporated into workshops and training programs conducted periodically in colleges. Such programs should also reiterate to the students that cannabis use is not exactly part of the Indian culture—its ritualistic use is restricted to very specific sub-cultural groups. This should not be equated with “safety” or “acceptability” of cannabis. Cannabis is recognized as an intoxicant and a drug of dependence, with attendant health harms, adversely impacting young people’s education and careers. Another important fact that needs to be featured in youth health education programs is that the high levels of tetrahydrocannabinol (THC, the main psychoactive ingredient of cannabis) present in the high-potency forms of street cannabis have been linked to a variety of mental disorders, including psychotic, bipolar, depressive, anxiety disorders, as well as suicide. 27 Conversely, cannabidiol, the other important ingredient of traditional cannabis, which is being explored for its medicinal value, is not present in street cannabis. Thus, the notion that cannabis use can be made more acceptable or supported for health benefits is grossly misplaced, and it is important to clarify this important distinction. This would help young people to be cognizant of the health harms associated with the various street forms of cannabis that are becoming increasingly available.
Lastly, the present study can provide some direction for policymaking in the context of the legalization of cannabis. Prior studies have documented that post-legalization of cannabis, there was a significant increase in the use of cannabis, high-risk behaviors among users, and decreased risk perception about cannabis use.2,4 Cannabis is not a legal drug in India; however, as indicated by the present study’s findings and prior literature,6,10 there appears to be some support or argument regarding legalization. Tobacco and alcohol are legal drugs, which probably is the reason why they contribute to a huge morbidity and mortality burden. If cannabis use is also legalized, would it result in more young people consuming it? Would there be a manifold increase in the existing disease burden, also keeping in mind that cannabis and tobacco are often smoked together? At a time when the adolescent brain is more vulnerable (compared to a mature brain) to long-term environmental insults such as THC in cannabis, 14 would our youth be at a much higher risk of contracting major illnesses as well as face a higher risk of fatal accidents due to its adverse influence on driving ability? These are significant concerns to be pondered upon, which can inform preventive programs and social policy about social/cultural permissiveness and legal sanctions for cannabis. Future research should examine the kinds of repercussions legalization of cannabis can lead to, particularly in the Indian context. For example, how do we operationalize the legalization of cannabis in India? This is important because the available experience of cannabis legalization is from other countries. But in India, where implementing laws regulating substance use may not be very stringent, the possible impact and potential consequences on our society must be thoroughly examined. Further research can also focus on designing a tailor-made intervention/primary prevention program for youth and examine its impact on their knowledge, attitude, perceptions, and expectancies about cannabis use, as well as cannabis consumption trends among youth over some time.
The present study was the first phase of a parent investigation to develop an intervention for college students in the context of cannabis use, which is informed by the student’s knowledge, attitudes, and expectancies. However, the study has some limitations. First, it was conducted among English-speaking urban college-going youth, which limits generalizability to other student groups (e.g., rural/non-English speaking). Another limitation is that the data obtained with regard to the students’ cannabis use, knowledge, attitude, and expectancies are based on self-report measures. Self-report data can be subject to social desirability or recall biases, under- or over-reporting, which can limit the generalizability of the findings. Nevertheless, the study has provided important information that builds on existing literature on cannabis use among young people. Based on this information, as well as inputs obtained from the students from focus groups, which were also conducted, the intervention has been developed and tested for feasibility among the students. The authors intend to report the findings shortly.
Footnotes
Acknowledgements
We thank the college administrators for their cooperation and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for this article’s research, authorship, and/or publication.