
Abstract

Autism Spectrum Disorder (ASD) is characterized by persistent deficits in social communication and social interaction and restricted, repetitive patterns of behavior, interests, or activities, with symptoms presenting in the early developmental period. 1 In India, more than 2 million individuals are affected with ASD; the pooled percentage prevalence is estimated to be 0.11 (1–18 year age group) and 0.09 (0–15 year age group) in the rural and urban areas. 2
Longitudinal outcome studies conducted three decades ago demonstrated an overall poor prognosis for adolescents and adults with autism. 3 Though early intervention studies have reported positive developmental outcomes, nearly 50% of the population had poor outcomes during adolescence and adulthood. 4 The challenges with independent living are seen even among individuals with good cognitive abilities. Evidence points to the persistence of core deficits and impairment in functional domains across the lifespan, necessitating support to varying degrees for individuals across the spectrum.5,6
Legal Mandate for ASD Certification Procedure in India
As per the Rights of Persons with Disabilities (RPWD) Act, 2016, enabling access to social welfare benefits and necessary accommodations for holistic development and inclusive participation, ASD was recently recognized as a disability when the number of conditions was increased from 10 in the previous version of the Act, Persons with Disabilities Act, 1995, to 21. As per the statute and guidelines issued for disability assessment and certification, the INCLEN-Diagnostic tool for ASD (INDT-ASD) should be used for identification and diagnostic ascertainment of ASD, and the Indian Scale for Assessment of Autism (ISAA) for the disability certification. 7
The INDT-ASD was validated against the Childhood Autism Rating Scale (CARS) and the DSM-IV TR diagnostic criteria as the gold standard, and a high internal consistency and overall diagnostic accuracy of the tool for ASD has been demonstrated.
8
Similarly, ISAA is also an open-access tool, developed and tested in the Indian context and available in regional languages, and requires minimal training.
9
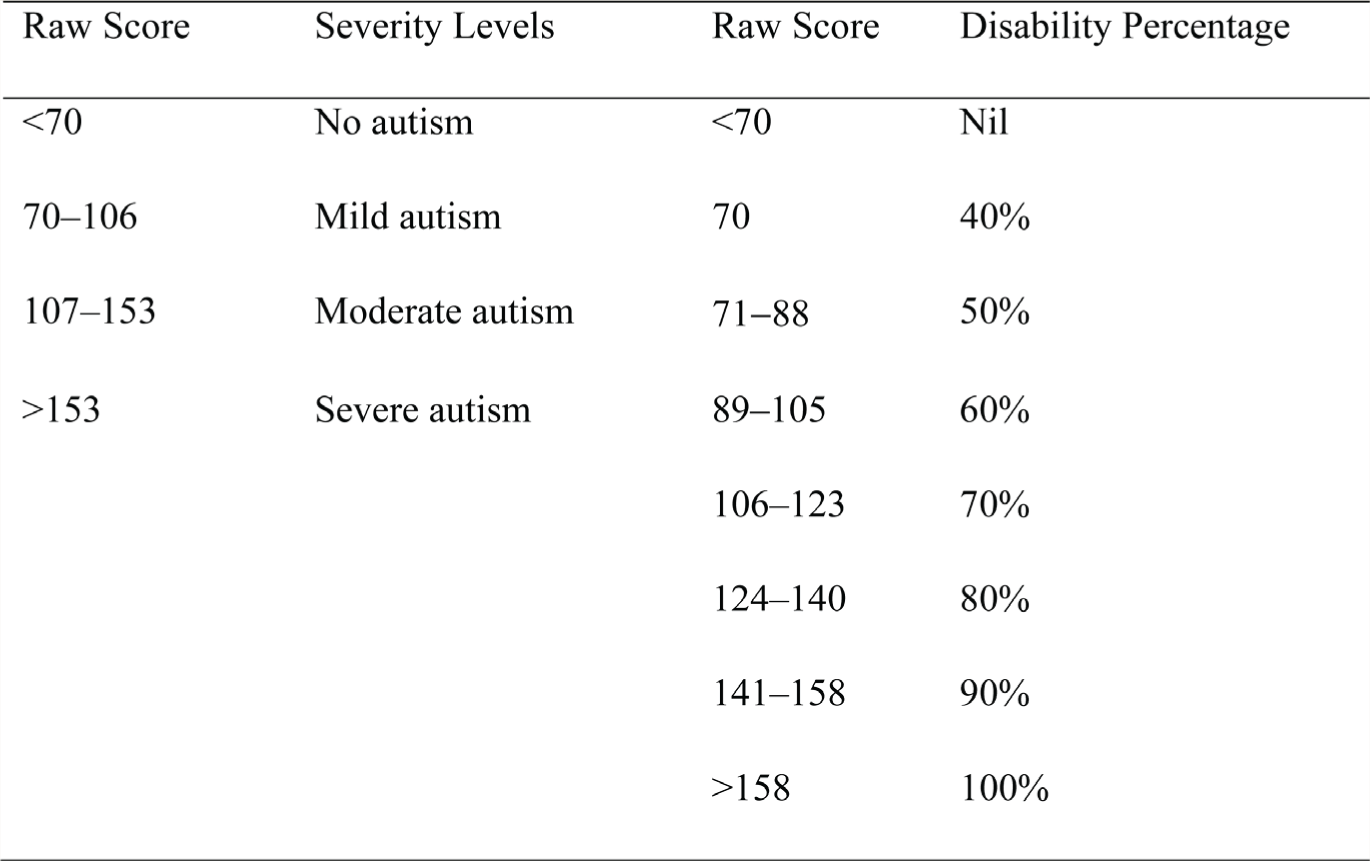
ISAA comprises 40 items represented as six domains: social relationships and reciprocity, emotional responsiveness, speech-language and communication, behavior patterns, sensory aspects, and cognitive components. Each item is assigned a Likert score ranging from 1 (rarely) to 5 (always), and the total ISAA scores range from 40 to 200. The total scores are used to ascertain the severity and the disability of ASD (
Severity Levels and Disability Percentages Based on the Total Score on ISAA.
Issues with ISAA in its Current Form
While ISAA is a simple and useful tool for clinical assessment, 10 it has potential limitations in diagnostic and severity assessments. ISAA is demonstrated to have suboptimal utility in young children (<9 years), especially 2-, 3-year-olds. Despite high sensitivity, positive predictive validity, and a valid cut-off for ASD caseness (>70 total scores), it had lower specificity and lower agreement with CARS, especially in younger children.11,12 Owing to improving awareness about ASD and the need for early identification and intervention, the number of families seeking services for their children at a younger age (<3 years) is ever increasing.13,14 Given the developmental nature of ASD, the manifestation of the core symptoms is dynamic though age-dependent. For this reason, the core features of socio-communicative deficits in ASD in young children may be under-recognized on ISAA as a function of age.
Despite high sensitivity and specificity for ASD diagnosis, ISAA does not match the clinical best estimate of ASD diagnostic severity. Studies assessing the psychometric properties of ISAA have demonstrated discriminant validity; however, they have not adequately accounted for the neurodevelopmental comorbidities in ASD.9,11,12 Conversely, children with comorbid Attention Deficit Hyperactivity Disorder (ADHD) and Intellectual Developmental Disorder (IDD) with varying severity of ASD could score high on ISAA because of the overlapping symptom profile and unspecified behavioral clusters. Also, overlapping developmental concerns could result in false positive “ASD caseness” on ISAA if not utilized in a balanced manner alongside comprehensive clinical assessments. For example, the inability to respond to social/environmental cues due to intellectual disability, hyperactivity/restlessness, or aggressive behavior due to ADHD can contribute to a “false caseness” of ASD, especially among children with multiple comorbid neurodevelopmental conditions of higher severity. We know that comorbidity is often the rule rather than the exception in neurodevelopmental disorders, so making differentiation of these disorders in children with severe impairment in multiple domains is difficult. Therefore, ISAA may not reliably distinguish functional impairment/disability due to ASD vs. non-ASD developmental comorbidities. ISAA may, therefore, have a role primarily in disability assessment rather than diagnostic assessment.
ISAA can also underreport the severity of ASD in specific conditions. This is especially applicable in the case of high-functioning individuals with ASD and in children who have shown developmental gains with intervention but still have a clinical diagnosis of ASD. Children with ASD who have good expressive language abilities but have deficits in lack of socio-communication due to pragmatic language impairment, may not be effectively captured on the ISAA. Similarly, children with ASD and comorbid IDD who may not have “savant abilities” or “unusual memory” are penalized as they lose points for not possessing these abilities. Similarly, in domains such as speech-language and communication, the scoring system favors those with atypical speech or regression but not those who have never developed communication skills. Sensory sensitivities are not a static phenomenon; children with ASD may outgrow some or all of them or be unable to express their particular sensory sensitivities, which may not be captured on the ISAA.15,16
Hence, on many aspects of the core symptom domains of ASD, the assessment of disability severity on ISAA does not reflect the ‘true’ functional impairment, which in turn impacts effective assessment and utilization of the current support needs.
Convergent Validity of ISAA with ASD Rating Scales
The CARS is commonly used for assessing the severity of autism. It is a 15-item clinician-rated instrument used in terms of total scores and percentile. 17 The total scores on CARS ranging from 30–36 suggest mild-moderate severity and >36 suggest severe ASD. CARS has also been used as a standardized measure to establish the convergent validity of INDT-ASD, which is mandated for clinical diagnosis of ASD, before administering ISAA.
The diagnostic accuracy of ISAA has been evaluated against CARS in previous studies and across disorders such as ADHD, Intellectual Disability, and typically developing children. 9 However, a study by Russell et al. suggested that the cut-off for considering ASD caseness among Indian children should be ≥33 instead of the original cut-off of >30. 18 However, the study did not comment on whether the cut-offs also need to be modified and revisited for ascertaining the severity levels as well. This again leaves us with the same question of whether the severity of autism is concordant between ISAA and CARS.
Recommendations
It is important to note that over the last 50 years, the conceptualization and understanding of autism has gone through a paradigm shift from being understood as largely a behavioral disorder to a disorder of atypical neurodevelopment. Gold-standard diagnostic tools such as Autism Diagnostic Observation Schedule (ADOS) and Autism Diagnostic Interview (ADI) are aligned with the current conceptualization of ASD; however, they require intensive training for clinical and research reliability and are not open access. In this regard, we suggest that ISAA be validated against standard diagnostic tools of ASD and measures of socio-adaptive behavior. A domain-wise analysis will help understand discrepancies in clinical severity and functional impairment as a result of ASD-related disability.
The same scale cannot be utilized for disability and diagnostic assessments, as their purposes differ. Criteria are strictly applied for diagnosis, but impairment is assessed from a transdiagnostic and functional perspective. It is necessary at this point to re-examine the ISAA’s purpose and, therefore, evaluate its domains and scoring to suit the purpose of assessment or functional impairment.
Though ISAA was field tested among children aged 3–20 years, the suboptimal performance of ISAA among children <5 years has been demonstrated. 12 This is an important consideration as the number of children diagnosed with autism in the first three years of life is increasing, and a disability assessment, albeit temporary, would be essential to apply for welfare schemes such as health insurance. It is paramount that the lower age range for valid assessment of ISAA is re-examined. This may also aid in the review of the legal mandate for autism disability certification. 1 *
The assessment kit described in the ISAA test manual is not applicable for older adolescents or adults with autism who require disability assessment and certification. The assessment procedures for ISAA should incorporate age-appropriate and age-relevant measures for effective disability assessment across the lifespan.
A multi-informant approach to assess symptom severity across various domains would be helpful to assess challenges and impairment across settings (e.g., parent, other caregivers, interventionist). Adopting a multi-informant approach will help mitigate factors impacting objectivity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.