
Abstract

Games are a ubiquitous part of human experience and conduct. India is the second largest growing digital population globally, with 692 million active internet users. 1 Children and teenagers frequently use the internet and play video games, putting some of them at risk for gaming addiction. 2 Internet gaming disorder (IGD) is defined as “repetitive use of internet-based games, often with other players, that leads to significant issues with functioning.” It is explicitly categorized as gaming disorder-predominantly online (6C51.0) in ICD-11 3 and as a condition for further study in the DSM-5-TR. 4
The prevalence of IGD in Korea was reported as 16.9%, of whom 32.2% used massive multiplayer online role-playing games (MMORPG) and 28.1% used first-player shooter games. 5 In India, the prevalence of problematic internet use among school-going students in Delhi was 19%, with higher rates in males, those in senior grades of schooling, and those who owned a personal device. 6 A study from Maharashtra reported a prevalence of 10.6% among high-school students, with male preponderance (15% vs. 3.5%). 7 Higher accessibility and affordability of internet, along with its impetuous use, have increased the chances of cyber-crimes targeting vulnerable individuals. A PubMed search using the keywords “internet gaming disorder”, “violence”, “homicide”, “suicide”, and “India” revealed no reports of patricide, suicide attempts, or socio-economic adversities in Indian youth with IGD. To our knowledge, this is the first series from India of four unusual cases of IGD with rare forensic presentations.
Case Series
Socio-demographic, clinical, psychosocial, and medico-legal profiles of four cases diagnosed with gaming disorder-predominantly online as per ICD-11, 3 are mentioned in Table 1. Details of internet usage, evaluation, treatment, and outcome are described in Table 2. IGD Scale-Short-Form (IGDS9-SF, score range = 9–45) 8 has nine items corresponding to the nine DSM-5 criteria of IGD, 4 with a cut-off score of ≥21 to distinguish disordered from non-disordered gamers. 9 Each item is rated from 1 (never) to 5 (very often) and has a Cronbach’s α index of 0.96, with an excellent internal consistency in Italian population. 9 The scale addresses the degree of severity as well as the consequences of IGD by assessing the patient’s online and offline gaming activity over the past 12 months in the following domains: preoccupation, tolerance, withdrawal, reduction/interruption, loss of interest, continuous use, deception, escape, and conflict. 8 Hamilton Depression Rating Scale (17-item; HAMD) was utilized to assess the severity of depression. 10
Socio-demographic, Clinical, Psychosocial, and Medico-legal Profile of Persons with Internet Gaming Disorder.
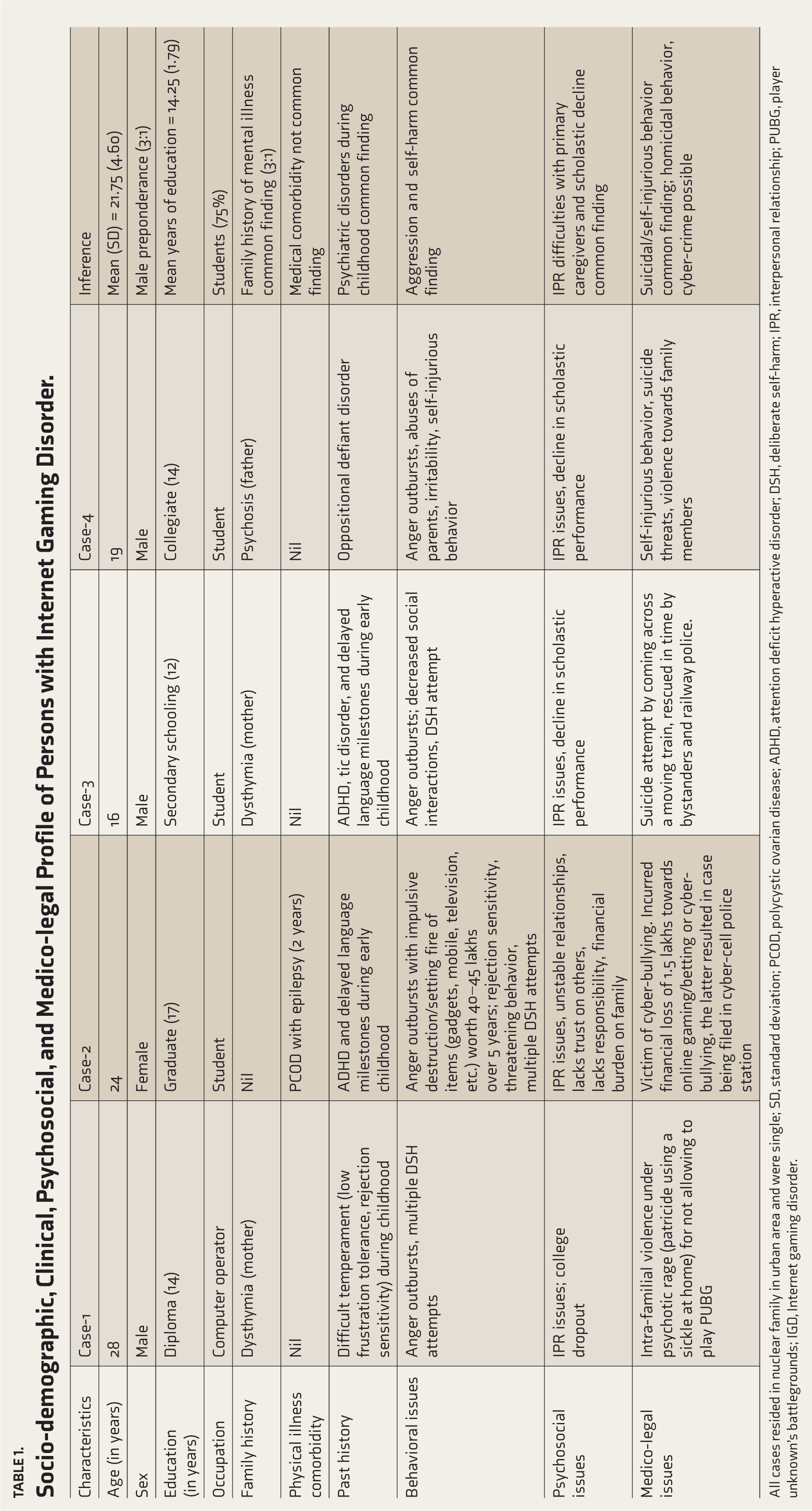
All cases resided in nuclear family in urban area and were single; SD, standard deviation; PCOD, polycystic ovarian disease; ADHD, attention deficit hyperactive disorder; DSH, deliberate self-harm; IPR, interpersonal relationship; PUBG, player unknown’s battlegrounds; IGD, Internet gaming disorder.
More Clinical Characteristics of Persons with Internet Gaming Disorder.
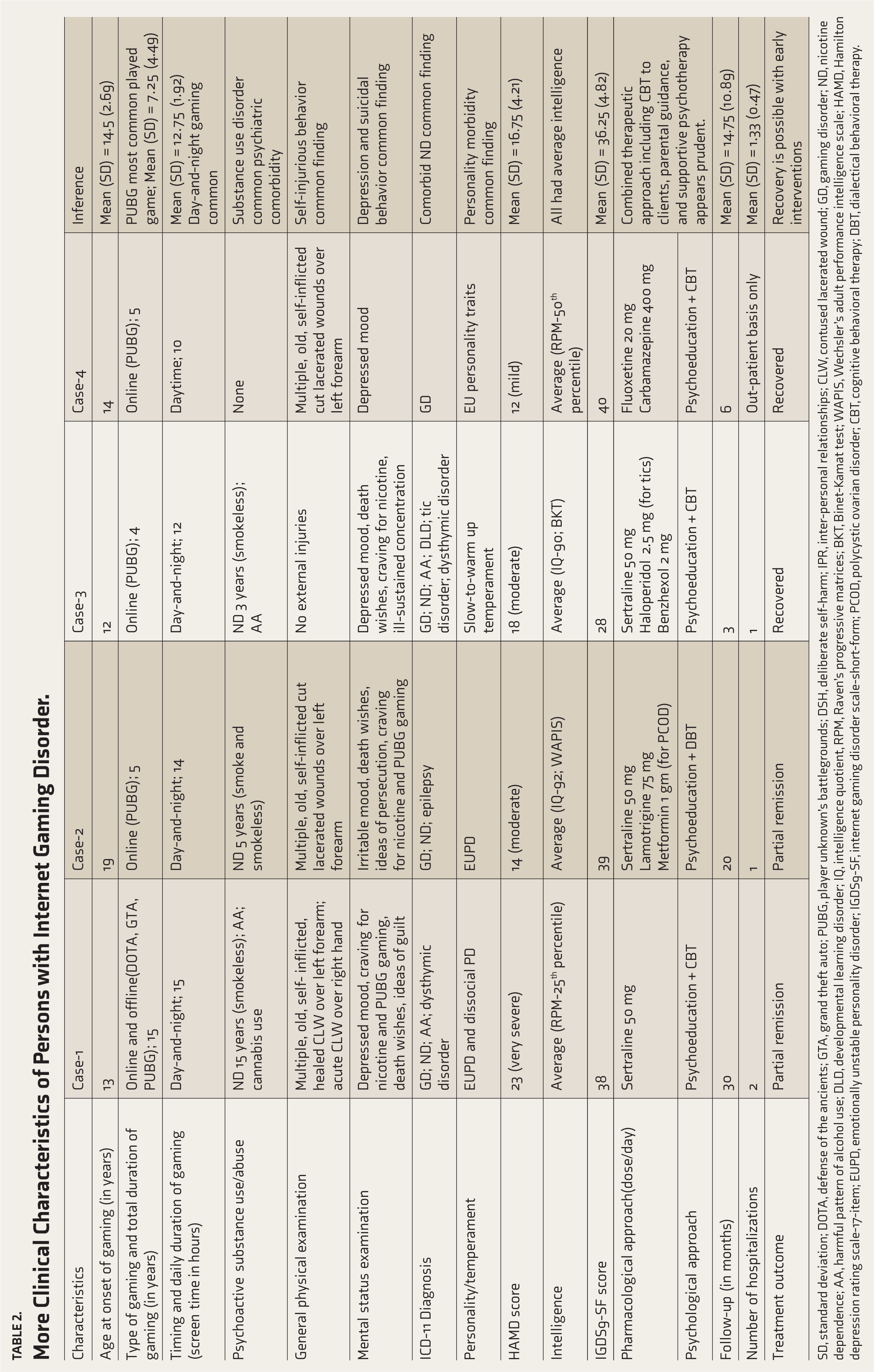
SD, standard deviation; DOTA, defense of the ancients; GTA, grand theft auto; PUBG, player unknown’s battlegrounds; DSH, deliberate self-harm; IPR, inter-personal relationships; CLW, contused lacerated wound; GD, gaming disorder; ND, nicotine dependence; AA, harmful pattern of alcohol use; DLD, developmental learning disorder; IQ, intelligence quotient, RPM, Raven’s progressive matrices; BKT, Binet-Kamat test; WAPIS, Wechsler’s adult performance intelligence scale; HAMD, Hamilton depression rating scale-17-item; EUPD, emotionally unstable personality disorder; IGDS9-SF, internet gaming disorder scale-short-form; PCOD, polycystic ovarian disorder; CBT, cognitive behavioral therapy; DBT, dialectical behavioral therapy.
Discussion
In our series, IGD was noted in young individuals (mean 21.75 years; SD = 4.6), especially males, as in other Indian studies.6,7 They presented with patricide, cyber-victimization, cyber-bullying, and suicidality. The mean age at onset was 14.5 years (SD = 2.69), with the mean duration of IGD being 7.25 years (SD = 4.49). The mean IGDS9-SF score of 36.25 (SD = 4.82) suggested adolescent-onset gaming addiction. Dropping out of school/college, decline in academic performance despite average intelligence, and being preoccupied in online gaming for >50% of daytime (mean 12.75 h; SD = 1.92) reflect salience, negative impact on educational attainment, and developing ‘psyche’ at a tender age.
The presence of moderate depression [mean HAMD score 16.75 SD (4.21)] reflects underlying mood changes in our disordered heavy gamers, who also showed impulsive acts such as self-harm and suicidal or homicidal behavior, upon restriction of gaming behavior by caregivers; this is similar to the finding by Messias et al. 11 who reported a higher risk of depression, suicide ideation, and suicide planning in heavy gamers (screen time ≥5h per day). IGD is strongly associated with depressive symptoms, 12 impulsivity, 13 aggression, 14 violence, 15 and suicidal ideation/attempts11,16 that necessitate clinical attention and risk mitigation. Comorbid substance use disorder (nicotine 75%, alcohol 50%, and cannabis 25%) was commonly noted in our MMORPG (e.g., PUBG) users, similar to a Korean study that reported frequent use of psychoactive substances such as alcohol and nicotine among MMORPG users, 5 possibly suggesting a common pathophysiological basis or common gateway for the addictions.
Our case series demonstrates the medico-legal and socio-economic adversities due to IGD, like patricide by decapitation using a sickle when the father confiscated the smartphone while the patient was engrossed in playing PUBG; suicide attempt, recurrent self-injurious behaviors, or suicide threats to procure money for PUBG gaming and betting; and cyber-crime (cyber-bullying and cyber-victimization during PUBG gaming). These adversities were particularly experienced when the addictive gaming behavior was restricted or disallowed by the caregivers, causing huge financial loss and caregiver burden. Adolescents and adults involved in risky gaming can fall prey to cyberbullying and cyber-victimization. 17 Internet addiction, cyber-victimization, and cyber-bullying can be reduced if both the players and caregivers pursue controlled and secured internet practices for gaming. 18
IGD must be understood as an endangering disorder with a complex psychosocial background. 2 A potential pathway to IGD appears to be rooted in childhood with depleted self-concept, which can lead to addictive activity, necessitating appropriate therapeutic approaches during the development and maintenance of the disorder. 19 Psychological factors such as negative peer pressure, high novelty seeking, cognitive “myopia”, and identity crisis, especially in young adolescents, laced with social factors such as poverty, social exclusion, poor parental warmth and connectedness, poor parental competence and supervision, and inconsistent parental behavior, all pose a risk to early-onset addictive behaviours.2,20
Our series suggests psychosocial factors such as staying in a nuclear family, being single, male sex, poor parenting style, and inter-personal relational difficulties with primary caregivers; psychological factors such as early childhood psychiatric comorbidities (ADHD, difficult temperament, oppositional defiant disorder, depression), early-onset substance use disorders (especially nicotine and alcohol abuse), suicide threats, salience, aggression, impulsivity, and personality/temperamental morbidity; and gaming characteristics such as early childhood internet/gaming exposure (<15 years of age), day-and-night gaming screen-time of >10 h/day, disordered online gaming (scoring >36 on IGDS9-SF), and playing online games with high immersion/aggression quotient (MMORPG genre) to have a potential and synergistic role in predisposing or perpetuating IGD, with consequent medico-legal and/or socio-economic adversities, in vulnerable youth. Hence, the evaluation and early appropriate management of these psychosocial factors appear prudent.
Our clinical observations support the assumption that problematic online gaming in adolescents should be viewed with a developmental approach, including key aspects of emotional development, that can represent significant targets for therapeutic interventions. 21 Pharmacotherapy options with different mechanisms of action have been tried in IGD, including antidepressants (escitalopram and bupropion), antipsychotics (olanzapine and quetiapine), opioid receptor antagonists (naltrexone), methylphenidate, atomoxetine, glutamatergic drugs (memantine, riluzole, and metabotropic glutamate receptor agonists), mood stabilizers (antiepileptics and lithium), and alpha-2 adrenergic receptor agonists. 22 We managed our cases with combined short-term cognitive-behavioral and pharmacotherapeutic measures (antidepressants, low-dose antipsychotics, and/or anticonvulsants) for a mean duration of 14.75 months (SD = 10.89). Early interventions resulted in recovery in two cases, while those with comorbid personality disorders had guarded prognosis. The choice of medications was based upon the presence of comorbidities (e.g. tic disorder, epilepsy, and personality disorder) and the severity of provoked or unprovoked aggression (homicide, suicide, and violence).
Conclusion
Gaming (except MMORPG genre) in moderation may have social, motivational, emotional, cognitive, and conational benefits (improves hand-eye coordination, concentration, creativity, memory, language, and teamwork; aids coping with stress; and teaches life and job skills). 23 Our series demonstrates the rare but potential forensic aspects of gaming addiction in triggering serious psychosocial and medico-legal adversities, including violence, suicide, homicide, and cyber-crime, in vulnerable individuals, necessitating risk mitigation, early detection, and comprehensive management. Future research appears prudent to clarify cut-off scores for IGDS9-SF in the Indian context to identify disordered gamers, as consensus is lacking across studies in different countries.9,24–27 Further research needs to explore the prevalence and psychosocial risk factors associated with the medico-legal adversities in relation to IGD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.