
Abstract

Dear editor
Drug-induced angle closure glaucoma (ACG) is an ophthalmological emergency that can lead to irreversible vision loss. 1 Up to one-third of ACG can be caused or precipitated by medications. Among psychotropics, olanzapine, ziprasidone, citalopram, and venlafaxine have been associated with ACG. 2 Aripiprazole has partial agonism at 5HT1A and dopamine type 2 receptors and antagonism at 5HT2A, 5HT2C, and 5HT3. 3 Its common adverse effects are nausea, headache, dizziness, fatigue, akathisia, salivary hypersecretion, constipation, weight gain, and extrapyramidal symptoms. 3 Here, we report a case of acute ACG precipitated by increasing the dose of aripiprazole in a patient with paranoid schizophrenia.
A 52-year-old married lady with schizophrenia presented with worsening psychotic symptoms for one month, characterized by auditory hallucinations, delusion of persecution, and socio-occupational dysfunction. No family or past history of psychiatric illness were present. She was not on any medication for systemic diseases. She was admitted for detailed assessment and management, and a diagnosis of Paranoid schizophrenia, episodic course with stable deficits, was confirmed according to the International Classification of Diseases 10th Edition (ICD 10). 4 Routine blood investigations and ECG were unremarkable. Baseline score on the Positive and Negative Syndrome Scale (PANSS) was 58.
She was started on oral aripiprazole 10 mg as it has good efficacy and fewer side effects among people of older age. 5 The dose was increased to 20 mg after a month as she had only partial improvement. She reported improvement in symptoms within a week of increasing the dose. The PANSS score was 32 after a week of increasing the dose, revealing around 45% improvement.
However, after five days, she suddenly started reporting severe frontal headache, bilateral orbital pain associated with nausea, vomiting, blurred vision, and bilateral congestion of eyes. All these symptoms lasted for 48 hours.. Evaluation by ophthalmologist showed that visual acuity in both eyes was 20/20. Anticholinergic agent was not used for ophthalmological examination. Goldman applanation tonometry measurement of intraocular pressure (IOP) revealed increased IOP. The right and left eye IOPs were 24 and 25 mm of Hg, respectively. So, a diagnosis of acute bilateral ACG was considered. Prednisolone, pilocarpine, and brimonidine eye drops were prescribed. Within two days, her conjunctival congestion and pain subsided, and within a week, the IOP in both eyes returned to normal limits.
A literature review revealed that a sudden increase in Aripiprazole dose could precipitate acute ACG. 6 Hence, the dose was reduced to 10 mg. Naranjo adverse reaction probability scale was administered and revealed a score of 8, which means a probable adverse effect due to the drug. 7 On subsequent follow-up, the patient maintained well, with a PANSS score of 21, and her IOP was within normal limits. Written informed consent was taken from the patient for publication purposes.
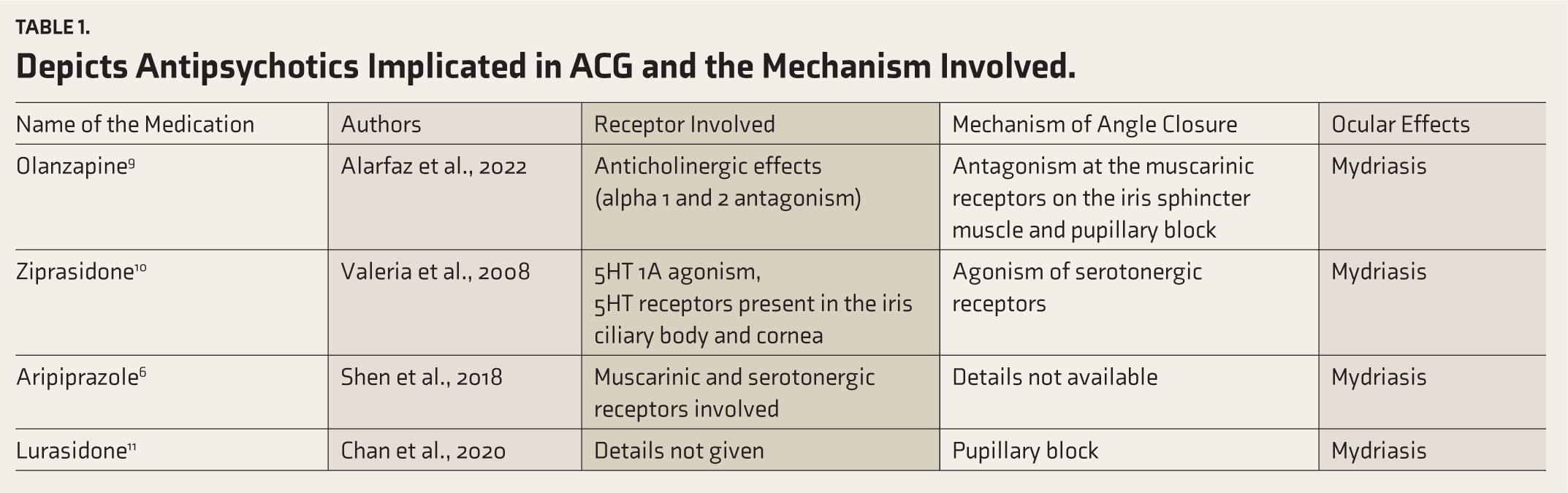
Acute angle closure occurs when the aqueous outflow is obstructed by the opposition of the iris within the iridocorneal angle in the eye. The rapid increase in IOP leads to permanent axonal nerve damage in retinal and optic nerves, termed glaucoma. 1 Antipsychotic-associated angle closure may be secondary to the anticholinergic effect leading to pupillary dilation and pupil block in patients with narrow iridocorneal angles.7, 8 Table 1 shows antipsychotics implicated in ACG. The ciliary body and iris have serotonin and muscarinic receptors, which helps in pupillary dilation. Although the precise mechanism of how serotonin influences the anatomy or physiology of the ciliary body and iris complex is unknown, it relaxes the iris sphincter, causing mydriasis and narrow-angle confrontation.5, 9 However, with aripiprazole, the anticholinergic effect is the least, compared to other antipsychotics. 8 In our case, probably, 5HT1A agonism and 5HT2A antagonism by aripiprazole in the iris and ciliary body led to pupillary dilation. Other risk factors associated with acute ACG are female sex, advanced age, shallow anterior chamber depth, short axial length, plateau iris configuration, and anteriorly positioned lens. 1 But, in our patient, as per ophthalmological evaluation, apart from age and sex, other risk factors were not found. There was no family or past history of a glaucoma attack. So, the bilateral glaucoma attack is likely to have been secondary to aripiprazole.
Depicts Antipsychotics Implicated in ACG and the Mechanism Involved.
Our findings support the view that patients on medication with a higher affinity for serotonergic receptors like aripiprazole should be monitored for ophthalmological adverse effects. Risk factors may be assessed, and a baseline ophthalmological evaluation may be helpful in those with multiple risk factors. Also, future studies can investigate the serotonergic effect on the occurrence of secondary closure glaucoma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.