
Abstract

To the editor,
Communication disorders, which include language disorder (LD), speech-sound disorder, and so on, often occur with Attention Deficit Hyper- activity Disorder (ADHD).1, 2 Among children with ADHD, 35%–50% have LD. 3 The co-occurrence of LD and ADHD negatively affects academic and social aspects. 4 The language and communication profile of ADHD includes delays in first words, word combinations, receptive- expressive language deficit, poor pragmatics topic maintenance, inappropriate physical proximity, excessive verbalization, frequent interruptions, and articulation problems.5, 6 Though Diagnostic and Statistical Manual 5 (DSM 5) uses the term LDs, the tool used in this study uses communication problems (CoP). Hence, in this paper, the term LD has been attributed to CoPs.
It is imperative to study CoP in preschool children with ADHD (ADHD-PS) due to (a) varied communication profile, deficits in multiple domains, and their impact on several aspects, and (b) the dynamic/complex nature of language and the variability in its acquisition in the preschool period. However, referrals to identify CoP in ADHD-PS are often delayed due to dominating behavioral issues, creating a gap in service delivery. This necessitates the utilization of a specific tool for early identification of CoP in ADHD-PS in India too, as the country is linguistically and socio-culturally diverse. This should then be followed by intervention, which is critical to alleviate further socio-behavioral and academic problems.
One tool is Children’s Communication Checklist-2 (CCC-2). 7 It (a) is a quick and reliable parent-report measure, (b) helps identify significant CoP in a busy OP, (c) measures different domains of language, which otherwise requires detailed assessment and is time-consuming, and (d) effectively differentiates communication profile of ADHD and Typically Developing (TD) children.7, 8 Initially normed for the United Kingdom (UK), it has been translated into different languages, including Kannada. CCC-2 studies in different regions and languages report 52.6%–82.1% of CoP in ADHD children (5–15 years).6, 9 This is a preliminary attempt to identify CoP in Kannada-speaking ADHD-PS compared to age-matched TD children, using CCC-2.
Methods
Two groups, ADHD-PS (n = 10) and TD (n = 17) were recruited for this study. ADHD-PS were recruited from the Department of Child and Adolescent Psychiatry of a tertiary care center after obtaining parents’ consent. Children with ADHD-PS were recruited based on the following criteria: (a) Kannada speaking, (b) aged 4–6 years, (c) confirmed diagnosis of ADHD with no comorbid neurodevelopmental disorders (NDDs) such as, Autism Spectrum Disorder and Intellectual Developmental-Disability (IDD), and psychiatric-conditions such as anxiety disorder as determined by a child and adolescent psychiatrist with an experience of >15years, using Diagnostic and Statistical Manual-5 criteria, 2 as well as Clinical Best Estimate (parental interview and multiple play sessions), and (d) having a social quotient > 70 (SQ- Vineland Social Maturity Scale, a proxy for Intelligence Quotient) to exclude IDD. 10 TD children matched for age, gender, and language, with SQ > 70, and no family history of neurological and NDDs were also recruited. The ADHD-rating scale (ADHD-RS) was used to measure the severity of ADHD in ADHD-PS children. 11
The primary measure was CCC-2. 7 It measures the communication profiles of children aged 4–16 years on ten scales with seven items each (i.e., a total of 70 multiple-choice items). The scales are speech, syntax, semantics, coherence [which measures structural language (SL)], inappropriate initiation, stereotyped language, use of context, nonverbal communication [which measures pragmatic language (PL)], social relations, and interests (which measures behaviors impaired in autism). 7 CCC-2 provides scale scores and two composite scores: (1) General Communication Composite (GCC), where GCC < 55 indicates clinically significant CoP, and (2) Social Interaction Deviance Composite (SIDC), which identifies the profile of autism and is considered for interpretation only if GCC is <55. Individual scale scores of <4 on any two or more scales indicate CoP of clinical significance. For this study, CCC-2 in Kannada, available in the department, was applied by a Speech-Language-Pathologist (SLP), after a co-author obtained permission for the same, through personal communication, from Pearson-Clinical, India. This study was approved by Institute Ethics Committee. This study is a part of larger study titled “Language characteristics in preschool children with ADHD”, conducted at the Department of Speech Pathology and Audiology, at a tertiary care center. Information was collected from parents via interviews. The primary respondents were parents/mothers.
Mann-Whitney U test and Chi-square test were used to analyze the group difference for demographic variables. Quade’s Analysis of Co-variance (ANCOVA) was used to analyze the group differences on composite and scale scores, adjusting for family income and SQ, using IBM SPSS 28.
Results
The mean (SD) age of ADHD-PS was 61 (11.05) months and TD was 62.88 (9.15) months. The majority were males in both groups: 80% in ADHD-PS and 70.6% in TD. Most families were from urban backgrounds (ADHD-PS: 86%, TD: 100%). In both groups, most parents were graduates and above (ADHD-PS: fathers 60%, mothers 70%; TD: both parents 100%). Most parents were professionals (doctors and engineers) or semi-professionals (college lecturers) (ADHD-PS: fathers 80%, mothers 60%; TD: fathers 100%, mothers 70%). The primary caretaker of all the children in both groups were mothers. In both groups, most children hailed from nuclear families (ADHD-PS: 70%, TD: 88%) and the upper class (ADHD-PS: 70%, TD:100%). Two ADHD-PS parents did not disclose their education or occupation. Significant differences were noted in mean(SD) and median(IQR) values between the groups in family income [mean(SD) of ADHD vs TD- (60,200(64,354) vs 1,69,882(85,452)) and median(IQR) (32,500 (16,500, 93750) vs 1,50,000 (1,00,000, 2,00,000)); p = 0.001] and SQ [mean(SD) of ADHD vs TD- (94.70(6.733) vs 104.44(7.20)) and median (IQR) (95.5 (91.96, 99.09) vs 105.26 (98.16, 110.90)); p = 0.004]. The mean score of ADHD-RS, in ADHD-PS group, was 35.1 (5.93). One child (10%) in the ADHD-PS group had a family history of IDD in a third-degree relative; others did not report any family history of NDD. Regarding the nature of CCC-2, the parents/respondents reported the questions being easy to understand and not too lengthy.
Table 1 describes the group mean (SD) and median (IQR) composite and scale scores of CCC-2. After adjusting for SQ and family income, a significant difference (p < 0.05) between the groups was observed in composite and scale scores, with ADHD-PS children performing poorer.
Comparison of the Two Groups on Composite and Scale Scores.
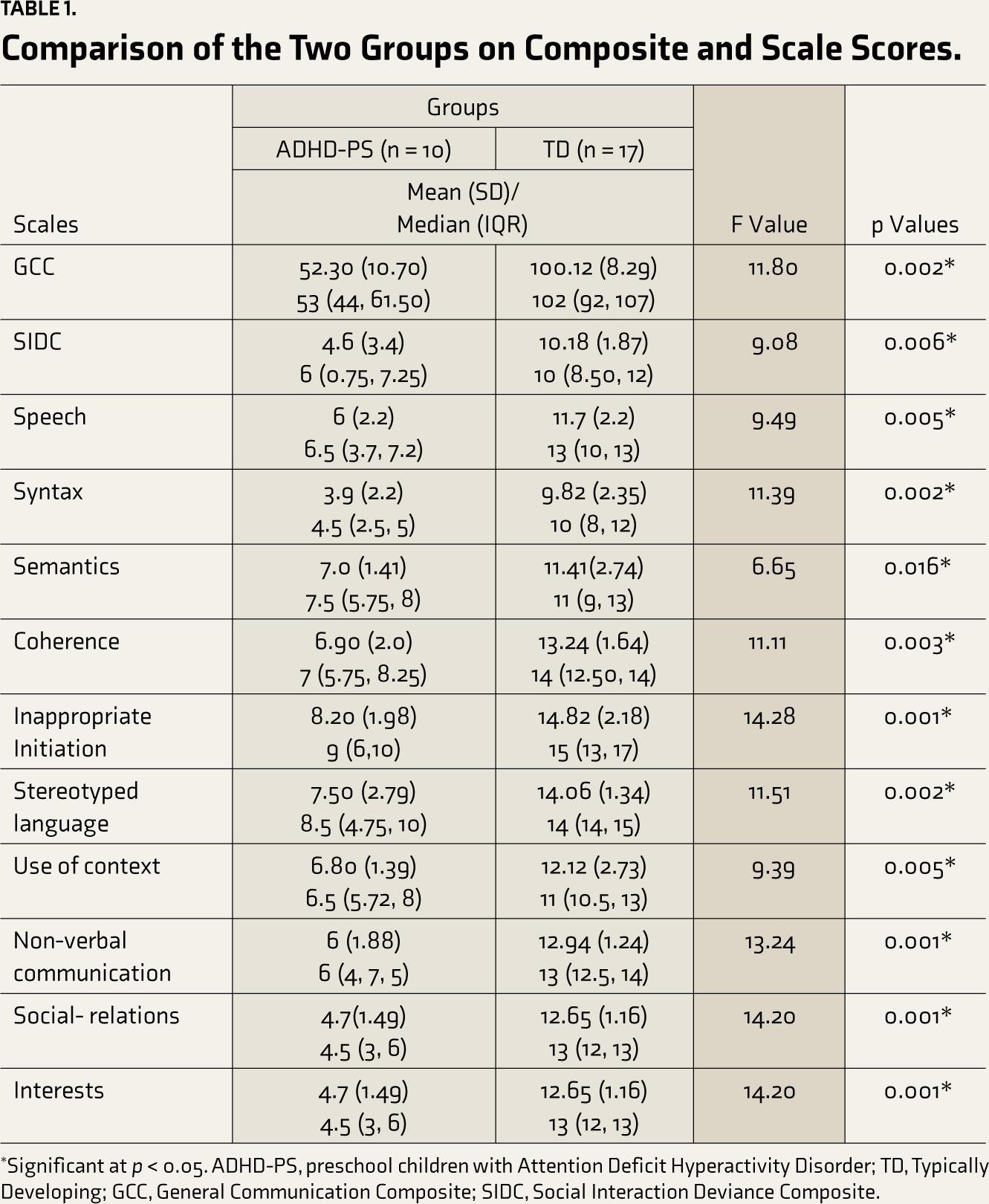
*Significant at p < 0.05. ADHD-PS, preschool children with Attention Deficit Hyperactivity Disorder; TD, Typically Developing; GCC, General Communication Composite; SIDC, Social Interaction Deviance Composite.
In the ADHD-PS group, five children (50%) had GCC < 55, while no TD children had GCC < 55. Also, ADHD-PS children who scored GCC < 55 did not score SIDC < 0. Six (60%) children in ADHD-PS scored <4 on ≥2 scales. Of the six children scoring less than 4 on two or more scales in ADHD-PS group, 2 children had deficits in speech scale, 4 in syntax, 1 in coherence and stereotyped language, 2 in non- verbal communication and 4 in social relations and interests scale. One ADHD-PS child had GCC = 38 and SIDC = 9, indicating a profile of Developmental- Language-Disorder (DLD).
Discussion
The results from composite and scale scores align with previous studies 9 and signify CoP in ADHD-PS children. Based on GCC, 50% of the ADHD-PS children had significant CoP; earlier studies also had reported 35%–50% LD 3 and 52.6% CoP using CCC2 in ADHD children. 9 ADHD-PS children with GCC <55 did not score SIDC < 0, indicating no PL problems in this group of children, which contradicts previously published reports of PL problems in ADHD children. 9 The scale/domain deficits might suggest general CoP. Also, for one child the profile of CCC-2 was suggestive of DLD (GCC = 38, SIDC = 9), which is further supported by the literature that has reported that ADHD children have subclinical DLD. 12
Though preliminary, the ability of CCC-2 to identify and differentiate CoP in ADHD-PS with TD is comparable with previous studies. 9 The deficits in CCC-2 domains can further help develop domain-specific speech-language intervention goals, thus reducing potential social and academic problems in ADHD-PS children. In a busy OP set-up, in a small Kannada-speaking ADHD-PS group, this tool aided in picking CoP. However, the results should be interpreted with caution since CCC-2 (a) is normed for the UK population, (b) must not be used as a standalone tool but to gain information for further SLP evaluation, and (c) must be validated against appropriate language-assessment tools.
Strengths of this study include (a) strict exclusion criteria to rule out other NDDs that might have impacted the findings, (b) use of more or less appropriately matched TD-children as controls, and (c) results obtained after applying appropriate statistical methods to control for confounders, SQ and one aspect of socio-economic factor (family income, which might have contributed to CoP). Limitations include (a) the absence of other language tools to validate CCC-2, (b) a small sample size, and (c) basing the results purely on parental interviews.
Though the sample was small and included only Kannada speakers, this study has demonstrated that ADHD-PS have CoP. Thus, routine screening for early identification of CoP in ADHD-PS is essential to improve assessment and short/long-term management outcomes. Further, the contribution of socio- environmental factors to the CoP in ADHD-PS could be studied. Also, for uniformity in methods, parents interviewed on CCC-2 did not find the questions lengthy; thus, this tool could be validated and implemented on a large-scale, especially in the Indian context, to reduce the gap in service delivery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.