
Abstract

Lithium salts are used in the treatment of bipolar affective disorder (BPAD). With a narrow therapeutic index, acute lithium toxicity is often associated with cardiotoxic effects, gastrointestinal symptoms, and late developing neurological signs, whereas chronic forms manifest primarily as neurological symptoms including confusion, myoclonus, and seizures and carry a considerable risk of kidney diseases such as nephrogenic diabetes insipidus and tubulointerstitial nephritis. 1
SARS-COV-2 predominantly affects the lungs. However, recent evidence suggests it can affect the nervous, cardiovascular, gastrointestinal, and renal systems. 2 In critically ill patients, commonly seen specific and nonspecific factors, such as mechanical ventilation, hypoxia, etc, might also contribute to injury to and functional decline of kidney. 3 Hence, clearance of lithium, 95% of which is excreted by the kidneys, can be hampered, leading to its increased serum levels even at previously well-tolerated therapeutic doses and cause toxicity. 4 BPAD patients on lithium maintenance therapy have been reported to come to emergency units with manifest signs of lithium toxicity after contracting COVID-19.5,6
Here, we report the management of two such patients of BPAD who came to a tertiary COVID care center a few weeks apart. We highlight the need for early identification of and intervention for toxicity in BPAD patients on lithium therapy who contract COVID-19.
Patient 1
Mr V, a 68-year-old married male with BPAD for 20 years, presented to the emergency unit after testing positive for COVID-19. He has been in remission with 1200 mg/day of lithium carbonate for the past four years. There was no history of use of any other nephrotoxic medications or polyurea or polydipsia. He presented with a history of fever, malaise, and two episodes of loose stools in the past five days. For the past three days, there was slurring of speech, unsteady walking, repeated falls, dizziness, and blurring of vision. On examination, he was disoriented to time, place, and person and febrile (102°F). Blood pressure was 140/90 mmHg, pulse rate was 92 bpm, SpO2 was 86%, and ECG was normal. Muscle fasciculations were seen in the eyelids and anterior aspects of the thigh. Neurological examination revealed bilateral hyperactive deep tendon reflexes and truncal and gait ataxia. Examination of other systems revealed no abnormalities. Speech was incoherent, mood was irritable, and thought, perception, and higher mental functions could not be examined. Venous blood samples were sent for routine inflammatory markers and serum lithium levels (Table 1). Major derangements evident were serum lithium of 2.4 mmol/L, creatinine of 2.4 mg/dL, sodium of 150 mmol/L, and potassium of 5.6 mmol/L. A high- resolution CT scan (HRCT) chest showed a COVID-19 Reporting and Data System (CORADS) score of 6 and a CT severity score of 19/25 (severe).
Serial observation of blood parameters in Patient 1.
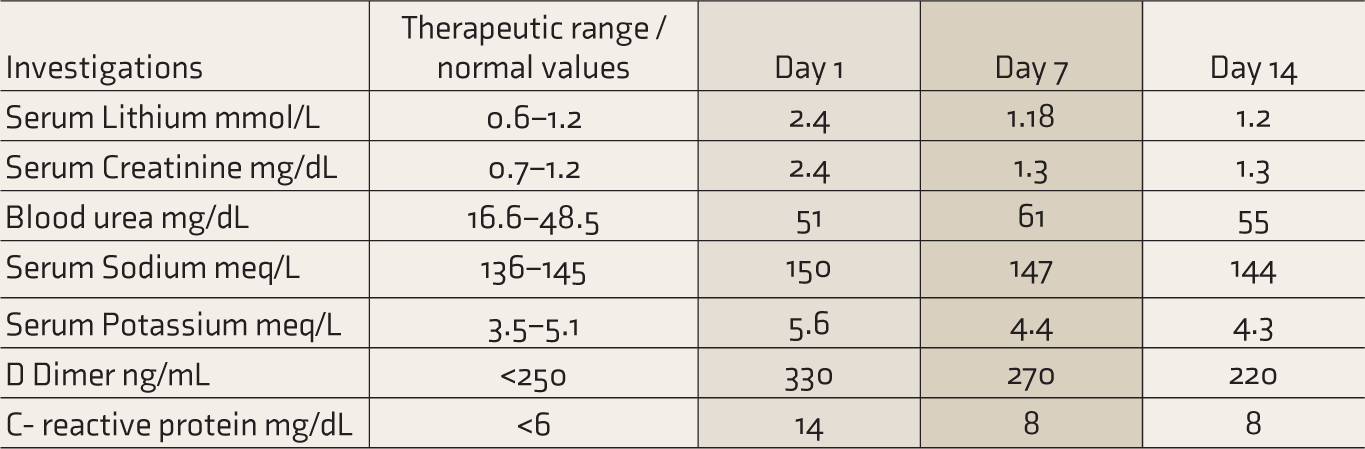
Diagnoses of pneumonia associated with COVID-19, 7 acute kidney injury (AKI), hypernatremia, lithium toxicity, BPAD, and delirium were made and the patient was shifted to ICU. Lithium was stopped, and treatment was initiated according to pre-approved guidelines (Inj. Ceftriaxone 1 g iv BD, T. Zinc 50mg OD, T. Vitamin C 500mg BD, Inj. Dexamethasone 4 mg iv BD, and unfractionated heparin 5000 IU SC). 7 Hyperkaliemia was managed with 50 ml of 50% dextrose with eight units of insulin. Normal saline (0.45%) was given twice daily for the next four days in view of AKI and hypernatremia. Oral feeds were initiated after four days. By the 7th day, the electrolyte parameters were normal and oral hydration was continued. His urine output was around 2 L/day. By day 10, his urine output improved and the delirium resolved. Patient was started on T. Olanzapine 5 mg/day which was gradually increased to 10 mg/day over 1 week. He was discharged by day 14 and was asked to continue T. Olanzapine 10 mg/day and evaluated further in subsequent follow-ups.
Patient 2
A 42-year-old married female, diagnosed with BPAD 10 years ago, in remission with divided doses of 1050 mg/day of lithium carbonate, was brought with a history of fever, shortness of breath, and myalgia for the past two days. She was diagnosed with COVID-19. On examination, she was oriented to time, place, and person. She was febrile with 101°F. Her BP was 90/70 mmHg, pulse rate was 90 bpm, SpO2 was 80%, and ECG was normal. Systemic examination and higher mental functions were within normal limits. There was no history of use of any other nephrotoxic medications or any history of polyurea or polydipsia. The speech was normal, and no abnormality was detected in mood, thought, or perception. Venous blood samples were sent for routine inflammatory markers (D-dimer and C- reactive protein) and serum lithium levels, which came as 0.9 mmol/L (Table 2). HRCT chest showed a CORADS score of 6 and a CT severity score of 18/25 (severe). Diagnoses of pneumonia associated with COVID-19 (severe category) and BPAD currently in remission were made. 7
Serial observation of blood parameters in Patient 2.
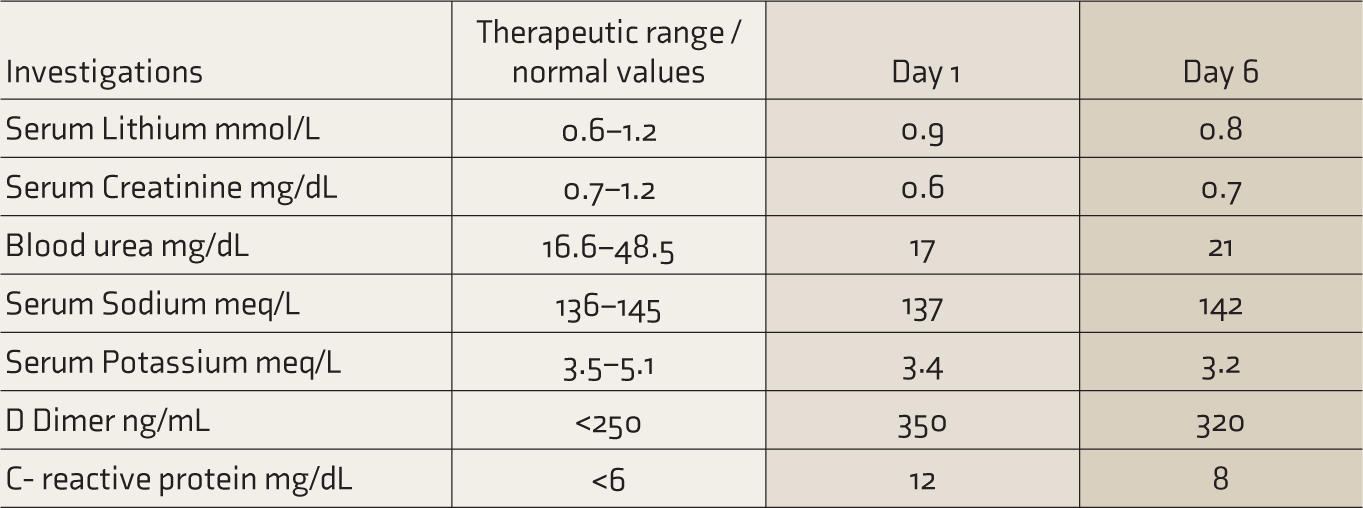
Treatment was started according to the Revised National Clinical Management Guideline for COVID-19, 2020. Supplemental oxygen was given, with an NRBM, at a rate of 10 L/min. She was also started on remdesivir 200 mg IV in 100 ml NS on day 1, followed by 100 mg IV in 100 ml NS for the next four days. A tapered dose of oral lithium carbonate 600 mg/day was given in divided doses. Oral aripiprazole 5 mg/day was started and gradually increased to 10 mg/day by day 3. By day 3, gradual improvements were noted in her saturation levels (98% on non-NRBM 4 L/min) and her fever had subsided. There was a marked decrease in the inflammatory markers but they were still not within normal limits.
By day 5, the patient’s BP was 100/70 mmHg, pulse rate was 98 bpm, and SpO2 was 96%. She was discharged after seven days. Oral lithium carbonate 600 mg/day was continued. A week after discharge, the general physical examination and higher mental functions were within normal limits. The speech was normal and no disturbance was detected in mood, thought, or perception. All indicators of renal function were found to be within normal limits, and the dose of lithium was up-titrated to a maintenance dose of 1050 mg/day, which the patient had been taking before. It was planned to taper off the oral aripiprazole over two weeks.
Informed consent was obtained from both subjects regarding sharing of their clinical information for educational purposes and publication.
Discussion
Lithium has been used extensively in the maintenance therapy of BPAD. Lithium is almost completely absorbed through the intestinal mucosa and freely crosses the glomerular membranes; renal excretion accounts for 95% of its elimination.8,9 The use of lithium seems to be related to a higher incidence of renal dysfunction; the longer the duration of lithium exposure, the higher the risk of renal failure and subsequent complications. 10
Recent reports and the cases mentioned above highlight the fact that in BPAD patients who were maintaining well on lithium, SARS-COV-2 infection can result in lithium toxicity at therapeutic doses. The first case was COVID-19 positive and presented with a history of five days of fever and developed altered sensorium and signs of lithium toxicity by day 8 of the illness. This may suggest that the higher the number of days of lithium exposure in COVID-19, the higher the chances of renal complications.
In the second case, a similar severity of COVID-19 warranted admission. Prewarned by recent reports of toxicity, on contracting COVID, in patients who are on lithium, and our experience with the first case, we checked lithium levels and screened for renal and electrolyte damage.5,6 These parameters were within the normal range (Table 2).
Both patients had increased levels of inflammatory biomarkers, which is consistent with COVID-19. The first case had lithium levels in the toxicity range, with manifest signs of toxicity. The rapid onset of deranged renal functions was evident by increased creatinine, hypernatremia, and hyperkalemia (Table 1). 11 The persistence of electrolyte imbalance in the first patient is suggestive of progressive renal injury. Functional renal impairment among patients with SARS-CoV-2 infection varies from 3.2% to 28.5%. 12 The S1 domain of the SARS-CoV-2 spike protein has been noted to bind to the Angiotensin Converting Enzyme 2 (ACE2) receptor to enter human lung cells. 13 These cells are also present in the kidneys, mainly in proximal tubules, afferent arterioles, collecting ducts, and the thick ascending limb of Helen and are the site of possible pathological processes related to SARS-COV-2. 14 Furthermore, a temporal connection of this derangement with COVID-19 was hypothesized in our cases, as there were no other obvious underlying pathologies and etiologies.
The second patient presented to us early in the infection. She had normal serum electrolytes and renal function tests and serum lithium level was within the normal range, suggestive of healthy renal functioning. The pathophysiology of COVID-19-induced nephrotoxicity involves local and systemic inflammatory and immune responses, endothelial injury, and activation of coagulation pathways and the renin–angiotensin system. 15 Cytokine storm syndrome, characterized by elevated TNF-α, interleukin (IL)-1, IL-6, IL-12, and interferon (IFN)-α secreted by the host immune system, leads to multiple organ failure, including kidney damage. 16 Other commonly seen comorbidities that can precipitate acute kidney damage in SARS-CoV-2 infection can be dehydration, electrolyte and acid-base imbalance, hypotension, cardiac insufficiency, disseminated intravascular coagulation, and drugs like NSAIDs, antibiotics, and antivirals. 17 All the factors mentioned above could have contributed to the increased lithium levels in the first patient. In the second patient, an early presentation, identification, and intervention in the nascent stage of the disease could be the reason why electrolyte and lithium levels were normal.
The above-mentioned aspects reveal a clear correlation between COVID-19 and its renal complications. 18 BPAD patients on long-term lithium therapy are at an increased risk of renal complications if they have comorbid COVID-19. Our experience in managing the first case, which had a late presentation to our center, a prolonged hospital stay, and overt signs of lithium toxicity, made us act proactively with the second patient. Once serum lithium levels were found to be in the normal range, the dose of lithium was reduced from an initial maintenance dose of 1050 mg/day to 600 mg/day in divided doses.
Furthermore, there is recent evidence of renal damage associated with remdesivir. 19 In the second case, we found that the co-administration of two nephrotoxic drugs, lithium and remdesivir, did not cause any impairment in renal function. This could be attributed to the reduction of the lithium dose.
Conclusion
During the COVID-19 pandemic, several cases were reported where BPAD patients on previously well-tolerated doses of lithium presented with increased serum levels and subsequent toxicity. AKI leading to decreased lithium clearance could be the underlying pathophysiological process leading to increased serum lithium levels. Nephrotoxic properties of lithium, kidney damage seen in COVID-19, and, at times, the use of nephrotoxic drugs like remdesivir have been implicated as the causes. Our cases highlight the need to proactively screen and identify cases with comorbid COVID-19 and BPAD who are on lithium maintenance therapy. Prompt intervention with a reduced dose of lithium yielded good results in our setup and prevented further nephrotoxicity. Even though our experience with these cases is limited, larger and more robust study models will go a long way in formulating recommendations based on factors such as age, gender, ethnicity, etc. In the COVID-19 pandemic, health services, including mental health services, had taken a huge setback. Abrupt interruptions in the treatment course and infrequent follow-ups were seen widely. We highlight the need for the primary treating physicians to be able to identify such cases, because early and prompt intervention goes a long way in reducing mean hospital stay and preventing further complications associated with COVID-19.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.