
Abstract
Background:
In anxiety disorders, culture is important in symptom presentation and help-seeking. Most tools for anxiety disorders are not validated in India and thus might not capture culture-specific aspects of anxiety. This study aims to identify and generate culturally specific terms to describe symptoms of anxiety as part of the development of the Kannada version of the Panic and Anxiety National Indian Questionnaire (PANIQ). The PANIQ is a tool under development to identify anxiety and panic in Indian settings.
Methods:
This study used qualitative methods like focus group discussions (FGDs) and in-depth interviews (IDIs) to identify and generate items related to anxiety and panic in Kannada from stakeholders like individuals with anxiety disorders, their caregivers, healthcare workers, and mental health professionals who treat individuals with anxiety and panic disorders. Five FGDs (n = 28), one triad (n = 3), and 34 IDIs (n = 34) were conducted.
Results:
The mean age of the participants was 38.9 (standard deviation: 12.28) years; 57.1% were from rural areas. We generated 615 Kannada items. These were classified into 21 domains and facets. Items in domains like Somatic symptoms, Fear, and Impairment in day-to-day life were higher than those noted in existing tools for anxiety that focus more on cognitive symptoms of anxiety.
Conclusions:
This study generated culturally specific items of anxiety through a qualitative process of tool development incorporating subjective experiences of persons with anxiety disorders and other stakeholders. This is among the first steps toward the development of PANIQ.
This study shows a feasible process of tool development that incorporates the subjective experiences of persons with anxiety disorders and other stakeholders, taking into account their respective cultural backgrounds. This process of involving terms generated from the community helps to create a culturally appropriate tool rather than translating westernized tools into the local language.Key Messages:
Anxiety disorders (ADs) affect 3% of the Indian population.1, 2 The heritability factor estimates for ADs are in the range 30–60%, indicating that they are influenced by ethnic, racial, and cultural factors.3, 4 Culture-dependent variations in beliefs about such illnesses, along with prevailing social contextual norms, are factors that could bear upon the development of ADs and associated help-seeking. 5
The nature of anxiety symptoms differs across cultures. 6 These differences could alter how anxiety is identified in individuals and impact epidemiological findings. 7 Healthcare providers need to be aware of the impact of culture on the clinical presentation of symptoms, as research has shown that the provision and utilization of mental health services by immigrants differ from the locals, due to divergence in beliefs and experience of illnesses. 8
Anxiety scales, such as Hamilton Anxiety Rating Scale (HAM-A) and Beck’s Anxiety Inventory (BAI), focus on symptoms de- rived from International Classification of Diseases (ICD) and Diagnostic and Statistical Manual of Mental Disorders (DSM). Lewis-Fernández et al. noted that descriptions of clinical symptoms incorporating local cultural aspects were absent from DSM IV-TR. 9 The authors inferred that this led to limited validity for the diagnostic criteria, lack of measurement equivalence, and exclusion of cultural presentations of anxiety in the existing tools. The exclusive dependence on the existing tools that have not taken local idioms and expressions of anxiety into consideration could lead to an underdiagnosis of ADs in different cultural groups. 9
Srinivasan and Neerakal found that Indian patients with panic disorder reported fewer cognitive symptoms like depersonalization than those from English-speaking countries. 10 The authors have argued that Dhat or “Semen-loss syndrome” is an example of a condition with prominent anxiety that has instead been consigned to the category of culture-bound syndromes in current classificatory systems. 8
Authors postulate that Indian culture lays greater emphasis on collectivism as compared to individualism. 8 People who deviate from such collective norms might experience and show embarrassment and shame that manifest as anxiety that might not get recognized. 11 The incorporation of these culture-specific factors in clinical evaluations could help in the identification and treatment of ADs. 7
Most existing tools for ADs are not validated in India and might not capture culture-specific aspects of anxiety. In this background, we report on a study conducted in India that aimed to generate terms describing anxiety.
Materials and Methodology
This study aimed to identify and generate culturally specific terms or symptoms of ADs in an Indian setting as part of the development of the Kannada version of the Panic and Anxiety National Indian Questionnaire (PANIQ). The PANIQ is being developed as a National Task Force Project (NTFP) by the Indian Council for Medical Research. The study is conducted across three sites: New Delhi, Raipur, and Bengaluru. As part of the NTFP, each site was responsible for developing items in respective local languages, that is, Kannada, Hindi, and Chhattisgarhi. The study arm in Bengaluru was approved by the Institutional Ethics Committee, and we have obtained written informed consent from all participants—professional and clinical—interviewed for the study. This study was conducted from April to October 2019.
As part of the NTFP, the development of PANIQ is conducted in three phases (Figure 1):
Flowchart of the Methodology.
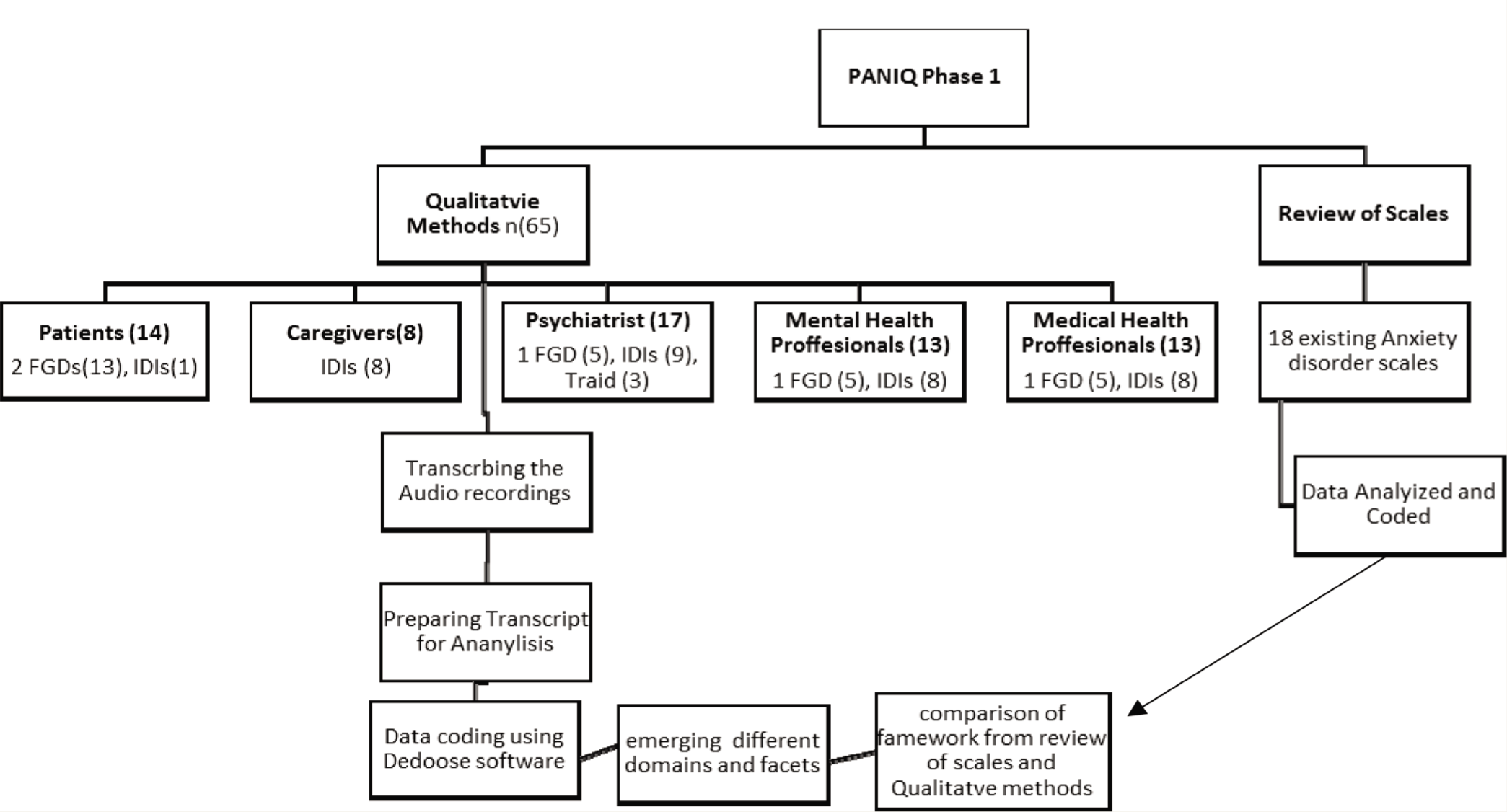
In this step, Sowmya and Sarah Ghani reviewed the existing scales for assessing anxiety and written sources of popular Kannada language literature to generate a list of terms describing anxiety. They also performed a retrospective review of charts of patients with ADs to obtain clinical descriptions of anxiety.
Qualitative study involved separate groups and individual interviews with (a) patients and their caregivers with ADs, (b) psychiatrists who treat patients with ADs, (c) other mental health professionals who treat patients with ADs, and (d) medical health professionals who come across patients with ADs in their clinical settings. This exercise generated the final list of items and led to a draft version of PANIQ for further testing and validation.
Such a mixed-method approach has been found to be useful in tool development. In this paper, we describe the qualitative study of Phase 1 that supported the generation of anxiety and panic terms in Kannada.
As part of Phase 1, we reviewed 18 existing AD scales like HAM-A, BAI, Hospital Anxiety and Depression Scale, Schedules for Clinical Assessment in Neuropsychiatry, Depression, Anxiety and Stress Scale (DASS 42), Patient Health Questionnaire (Prime-MD PHQ), and Panic Disorder Severity Scale. This review yielded multiple themes that were divided into 21 domains and further subdivided into facets. Based on the HAM-A scale items and other scales, domains were added further, and this was later discussed among all investigators and staff in the three centers to achieve consensus. We used these domains and facets as a deductive framework for analyzing the qualitative interviews. We used IDI, FGD, and triadic interviews to obtain terms of anxiety from participants. We used content analysis to derive the terms within the framework.
Setting
This study was conducted in south India in the Psychiatry OPD of St. John’s Medical Hospital, Bangalore, which is an urban setting, and in St. John’s Medical hospital community health center, Mugulur, which is a rural setting. Sowmya and Sarah Ghani were trained in conducting FGDs and IDIs by Priya Sreedaran and Ashok Mysore, using mock FGD and IDI with the same interview guide.
The participants included:
Patients: Adult men or women above the age of 18 years, fluent in Kannada, with an ICD-10 diagnosis of ADs like generalized AD, mixed anxiety depression, phobic disorders, panic disorders, and other ADs. Caregivers of the patients mentioned above who were fluent in Kannada, but not necessarily caregivers of the same patients who participated in the group mentioned above. Medical professionals, including physicians with or without super specialization, from departments of general medicine, gastroenterology, cardiology, neurology, and emergency medicine, with a minimum experience of 2 years, who were fluent in both Kannada and English. We involved these professionals on the assumption that they would regularly encounter patients with anxiety as part of their clinical practice. Qualified psychiatrists with a minimum experience of 2 years of clinical practice who are fluent in Kannada and English. Mental health professionals like clinical psychologists, psychiatric nurses, and psychiatric social workers with a minimum of 2 years of clinical experience who are fluent in Kannada and English.
To ensure that no facets of the phenomenology of anxiety must be lost from our purview, there were no exclusion criteria.
Process
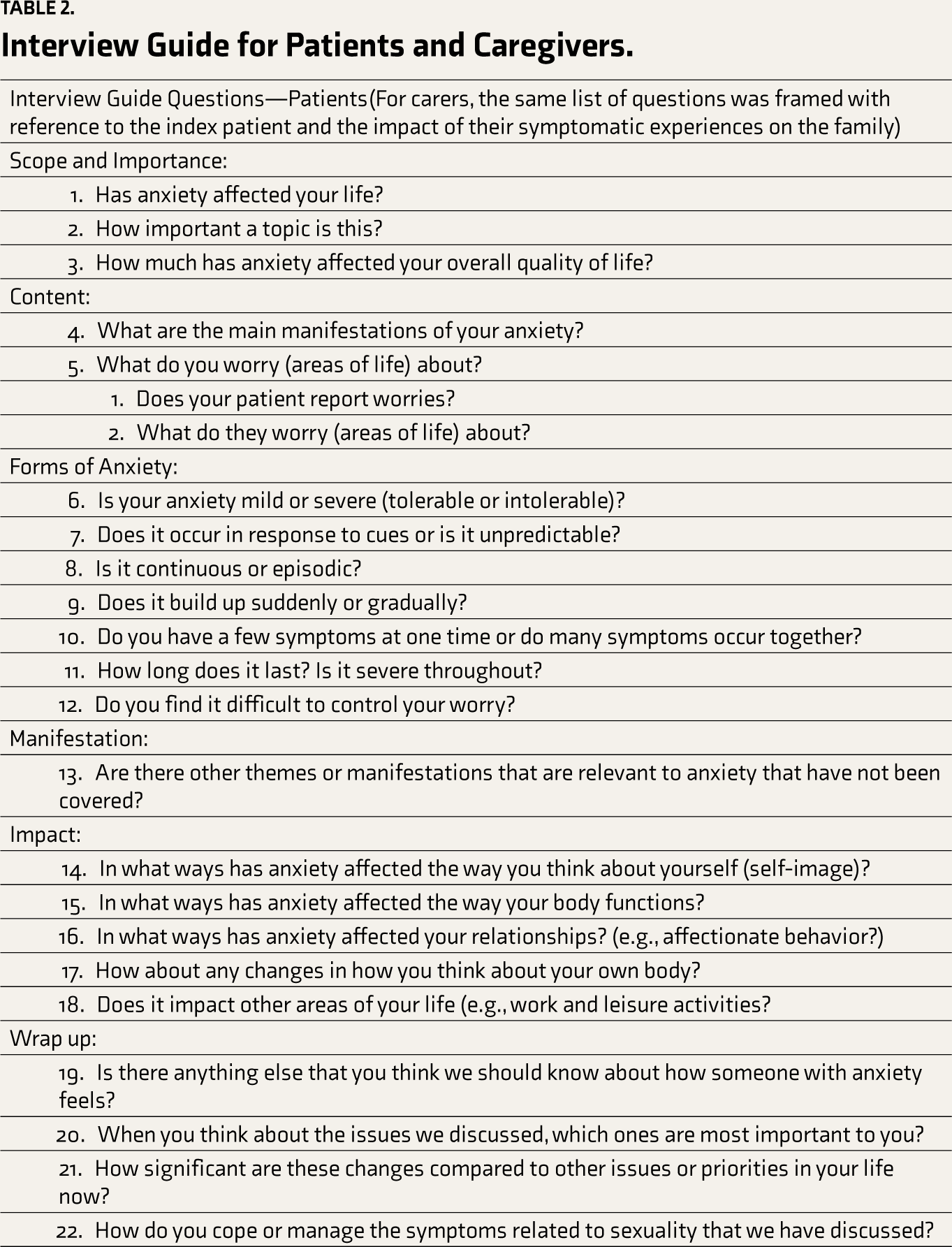
The patients from psychiatry OPD were approached face-to-face by researchers. Those who matched our inclusion criteria were explained about the purpose of the study, and those who consented were invited for either FGD or IDI. As part of this study, we translated to Kannada a semi-structured interview guide developed as part of the development of PANIQ. This translated interview guide was pilot-tested in the patient group (Tables 1 and 2).
FGDs, IDIs, and Triadic Interview Guide for Professionals.
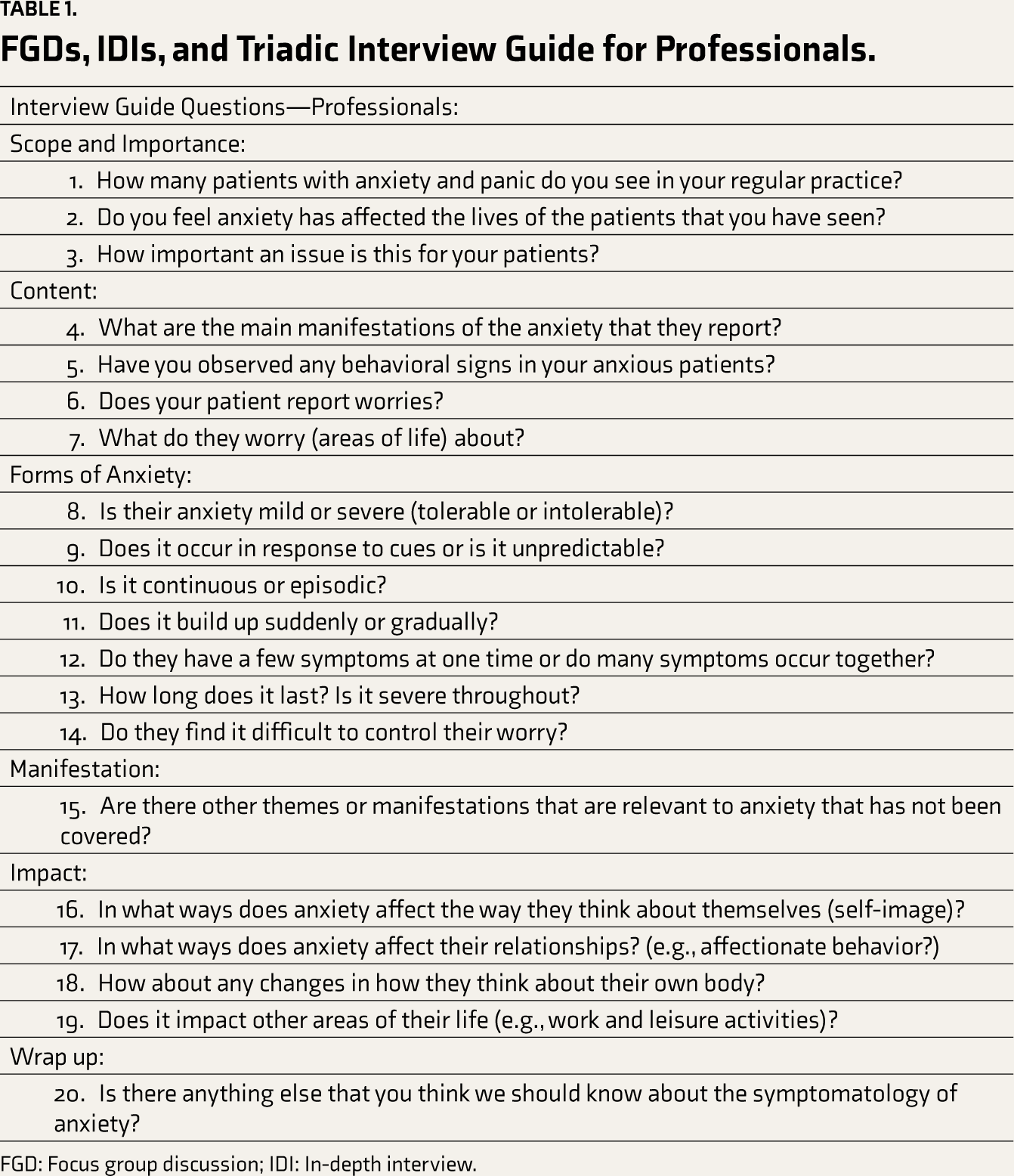
FGD: Focus group discussion; IDI: In-depth interview.
Interview Guide for Patients and Caregivers.
FGDs: Each FGD consisted of six to eight participants. Groups were homogenous concerning the type of participants, that is, comprising only patients or only caregivers and so forth.
We conducted all FGDs in a well-ventilated and closed room in the hospital. We recorded all sessions after obtaining additional written consent for the recording. The first author moderated the session, while the second author observed and noted all the discussion points. We conducted the FGDs in the following fashion: introduction, use of a semi-structured guide, summarizing the session, and conclusion by thanking all the participants. Both the moderator and the second author were females. The moderator did not have any prior relations-hip with the participants. However, a few participants were the patients or colleagues of Priya Sreedaran and Manoj K Sahu. Both moderator and second author have been trained to avoid the interviewer’s bias. They were fluent in Kannada and had prior experience conducting FGDs and IDIs with different groups.
IDIs: Sowmya and Sarah Ghani individually conducted IDIs. This was conducted for participants who were interested in the study but could not participate in FGDs because of time and travel constraints and were given an option of IDIs using the same semi-structured guide.
Triad interviews: Given the challenges of getting busy medical and mental health professionals together, we used triad group interviews that involved interviewing three participants in a place commonly agreed upon by the participants. This was similar to another study. 12
After the interviews and FGDs, we transcribed all the audio recordings verbatim. We then read all the transcripts. Once the repetitive symptoms and terms arrived, we stopped doing further interviews, as data saturation was reached. Then we began coding using the deductive framework. We coded all symptoms, terms, and phrases in vivo using Dedoose qualitative software.
Sowmya and Sarah Ghani independently coded all similar symptoms under domain headings derived from the organ system. For example, symptoms/terms such as thought block, memory issues, and inability to take decisions were grouped and coded under the cognitive domain. Symptoms like palpitations, racing of the heart, and so forth related to the heart were grouped as the cardio-vascular domain, and issues related to breathing were grouped as the respiratory domain.
Sowmya and Sarah Ghani further classified the resulting codes and domains into the framework based on the review of 18 anxiety measures. Investigators of the broader study later verified this. All disagreements were resolved by consensus. The goal of the coding and the analysis was to generate as many terms as possible so as to not miss out on any of the culturally relevant expressions of anxiety.
Results
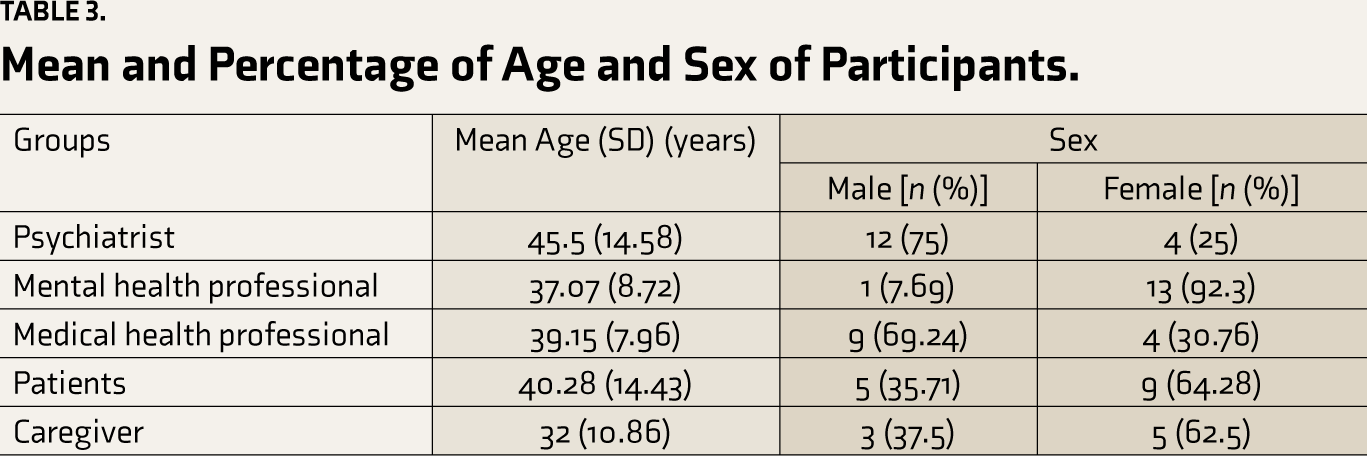
We conducted qualitative interviews with 65 participants in five groups: (a) patients—two FGDs (n = 6 and 7 in each) and one IDI; (b) caregivers—eight IDIs; (c) psychiatrists—one FGD (n = 5), nine IDIs, and one triadic interview (n = 3); (d) other mental health professionals—one FGD (n = 5) and eight IDIs; (e) medical professionals—one FGD (n = 5) and eight IDIs. The FGDs lasted 45 minutes to 1.5 hours, the triad lasted 1 hour, and IDIs lasted 30 minutes to 1 hour. There were 18 dropouts (six from the patient, eight from caregivers, and four medical professionals groups) from this study due to time constraints, fear of symptoms triggering, and lack of interest (Tables 3 and 4).
Mean and Percentage of Age and Sex of Participants.
ICD Diagnosis of Patients.
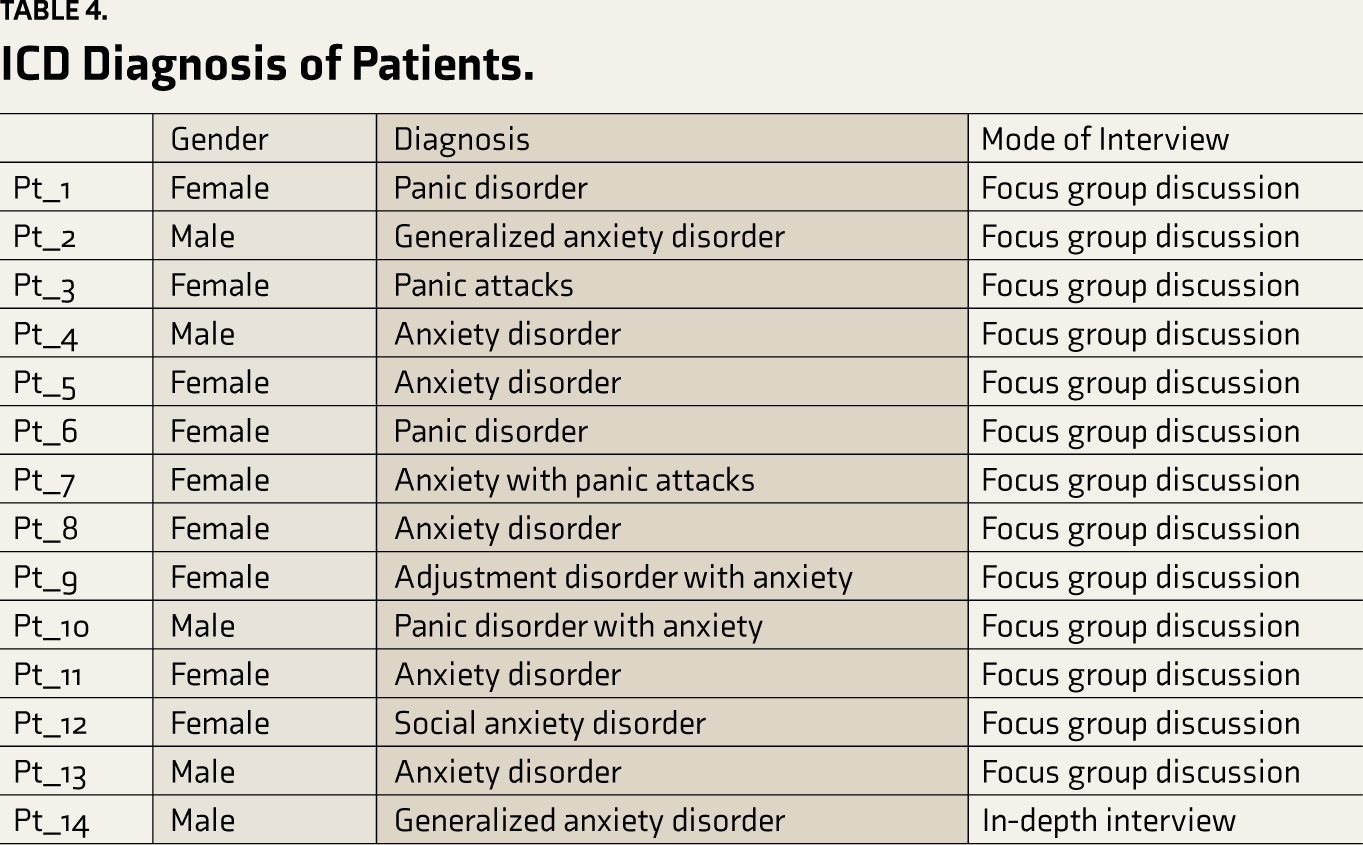
The mean age of the participants was 38.9 (standard deviation [SD]: ±12.28) years; 57.1% (n = 8 out of 14) of the patients were from rural areas. All medical and mental health experts were from urban backgrounds, and experience in treating patients with AD ranged from 3 to 30 years.
We generated 615 Kannada items from qualitative interviews. We derived 23 themes that were further grouped into 21 domains and facets based on the pre- existing deductive framework (Table 5).
Domains Arrived at from Qualitative Interviews.
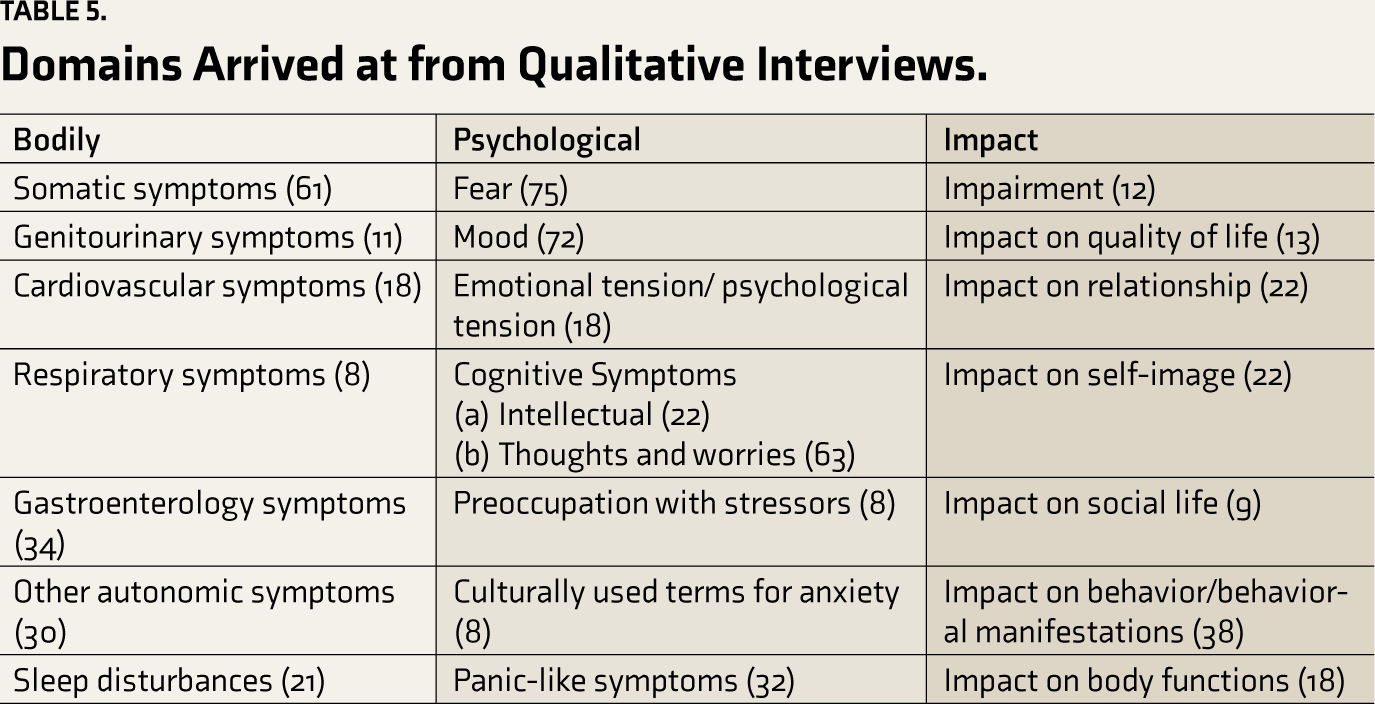
When we compared the items generated from our study with those from the review of existing scales (Table S1), we observed a higher number of facets recorded in domains such as Somatic symptoms, Fear, and Impairment in day-to-day life. Even though some items feel similar, the expression of that item is different, so it was considered a new item only. For example, from the review of scales reported, profuse sweating from FGD was translated into ಮೈಯಲ್ಲಾ ಬೆವರು (sweat all over).
We also generated an additional domain called preoccupation with stressors, as several patients reported the presence of stressors as a source of anxiety. Several colloquial expressions of anxiety symptoms reported by participants are listed in Table S2.
The other domains and facets derived from the content analysis and not present in standard anxiety identification tools were “doctor-shopping behavior” and “worries of shame”. All three groups—patients, caregivers, and professionals—reported these domains.
We found that professionals used clinical terms found in ICD-10/DSM IV such as palpitations, profuse sweating, worries, and so forth as presenting symptoms of anxiety. On the other hand, caregivers emphasized that the behavior changes due to anxiety and worries in the interviews.
CG-2: “My dad always used to visit many doctors.”
CG-1: “She gets irritated a lot for small things.”
CG-4: “My son worries about what his friends will think of him.”
CG-5: “ಕೈಯಲ್ಲಿಏನೋ ಕೆಲಸ ಮಾಡುತಿರುತ್ತಾರೆ” “always they keep doing something in the hand” “Feeling fidgeting in hand” Patients reported symptoms such as somatic complaints, shame, vague sensations in the body, worry, and impact of anxiety on their work, social relationships, self, body image, and so forth using colloquial expressions. Most of the terms used were colloquial expressions such as“ಏನೋ ಒಂದು ತರ ಆಗುತ್ತೆ” which translate to “somewhat indescribable feeling.” Some patients repeated the same words in an attempt to emphasize the gravity of the symptoms, like “ಗಾಬರಿಗಾಬರಿ ಆಗುತ್ತೆ,” which translate to “frightened” in English, but is used to emphasize that they are “very much tensed.”
A key observation was the role of English words and phrases in the local dialect. In the interviews and discussions, participants used terms to describe their symptoms with a combination of English and Kannada, popularly known as Kanglish language, for example, Tension aguttha ide (I am tensed), heartbeat ಜಾಸ್ತಿ ಆಗ್ತಾಯಿದೆ ide, shivering ಆಗ್ತಾಯಿದೆ, “bp ಜಾಸ್ತಿಯಾಗಿದೆ”, “nervousness ಆಗುತ್ತೆ,” and so forth.
Discussion
The results indicate that many colloquial terms express the subject’s anxiety. We opine that clinical and mental health professionals be familiar with these terms, as this will help identify anxiety. In our view, these cultural variations in the expressions of anxiety are important in identifying ADs in clinical settings. These terms should also find a place in tools identifying ADs in a particular culture.
It is necessary to emphasize that tools to identify and evaluate anxiety should be derived from those who experience and witness anxiety and be adapted to reflect the impact of culture. This will help prevent the underdiagnosis of ADs. 11 The current study has helped identify cultural idioms of expressions of anxiety that will form the eventual items of the PANIQ tool. Stevens and Palfreyman have similarly argued that terminologies and symptoms derived from the patient population add greater value to the tool. 13 Trivedi and Gupta also reported that culture could affect symptom presentation, explanation of the illness, and help-seeking. Importance given to the symptoms, and meaning assigned by the physician, also differ across cultures.14,15
Our review of anxiety scales found 21 domains, whereas the qualitative study derived 23 themes further grouped into 22 domains and facets. Domains including impairments and impact on social life, self-image, and quality of life were reported by participants, while these are rarely captured in scales such as HARS, HAM-D, PHQ Scales, and the existing standardized anxiety scales.9,16 The anxiety scales such as HADRS, STAI, and Generalized Anxiety Disorder Scale-7 mainly focus on ICD and DSM-IV criteria for anxiety, whereas Beck Anxiety Inventory focuses on domains such as cognitive and somatic domains. The Anxiety Disorder Diagnostic Questionnaire focuses on domains such as fear, anxiety, worry, avoidance behavior, physiological and distress symptoms, and interference. 16 The current study has shown a greater recording of items that represent symptoms such as somatic, fear, mood, and worry. This is different from other existing AD scales with a greater focus on cognitive and behavioral symptoms.7,17
Results showed a difference in the expression of an individual’s experience of anxiety and the way treating mental health and medical professionals perceive this. This disparity suggests a possibly prevalent lack of being conversant with patient experiences; hence, these differences might serve as potential barriers to identifying anxiety and providing necessary clinical intervention.15,18,19 Given that we selected professionals who we believed were more conversant with local idioms and so forth, this finding is striking. It highlights the need for scales such as the one under construction. A review on idioms of distress in India also indicated the need for psychiatric evaluation and examination of health and illness through the lens of idioms of distress. Otherwise, it creates cultural blind spots in clinical practice. It helps to establish a rapport and build the type of empathic connection that comes from the patients. 20
This study used qualitative methods, which offer several advantages like the involvement of populations who will be the end user of the tool later and the generation of items and dimensions through the involvement of patients, caregivers, and their treating professionals. We believe that the domains and items will be relevant to target populations. We hypothesize that this study will contribute to an increase in the face and content validity of the PANIQ once it is developed. The results show that the three groups report different domains and terminologies of symptoms. We infer that this is a consequence of the triangulation of data sources from patients, caregivers, and professionals. This is similar to the study by Choudhary et al., who also used qualitative methods with triangulation of parents, professionals, and children having a history of sexual abuse, while developing a multi-dimensional scale to measure trauma associated with child sexual abuse. 21
In the current study, the patient sample mostly reported symptoms related to physical distress, bodily discomforts, or symptoms like pulling sensation, pain in extremities, pain in different parts of the body, numbness sensation, and “jhuma-jhuma” sensation in different parts of the body. A study conducted in rural Nepal also emphasized the “jhuma-jhuma” sensations, which are correlated with depression symptoms. 19 This suggests that these kinds of expressions have underlying psychological value across different places. Some expressions might have similar meanings attached to them, while others differ.
Another finding was that English words are being adapted and colloquially used in many Indian languages. English words, like “tension” instead of udvega, “time,” “control,” “fit,” “off,” “heart,” “shivering,” “tension,” and “stress,” are increasingly being used in metropolises as part of regional language, instead of the local language equivalent words. Such expressions of symptoms and commonly used English words as part of the Kannada language need to be kept in mind while constructing the items for the tool. The limitation of the study is that the current sample was collected in and around Bangalore. Recruiting samples for FGDs from across Karnataka may have been more representative. We have addressed this limitation through further refinement of the tool using additional reviews by professionals across Karnataka and will highlight the same in subsequent publications.
Conclusions
This study shows a feasible process of tool development that incorporates subjective experiences of persons with ADs and other stakeholders, taking into account their respective cultural backgrounds. This process of generation of new terms to describe symptoms is among the first steps toward the PANIQ tool.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
The Study was funded by the Indian Council of Medical Research (ICMR) under the Task Force for “Development of Panic and Anxiety National Indian Questionnaire”.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.