
Abstract
Background:
The relationship between imprisonment and mental illness is bidirectional. The clinical outcomes of prisoners with mental illness have not been widely studied, especially in developing countries. This study was conducted to assess the same among male inpatients under judicial custody with charges of homicide.
Methods:
A retrospective chart review of male forensic ward inpatients admitted between January 1, 2003, and December 31, 2016, was conducted. Diagnosis in the files was based on the International Classification of Diseases (ICD)-10 criteria. The Clinical and Global Improvement—Severity (CGI-S) scale was used to measure the severity of illness. Mean CGI-S assessment was carried out at baseline, end of 1 year, 5 years, and 15 years. The data were analyzed using descriptive statistics, Friedman’s test, and Dunn’s post hoc test.
Results:
Schizophrenia spectrum disorders and other psychotic disorders, mood disorders, and alcohol use disorders were diagnosed in 62(49.6%), 22(17.6%), and 44(35.2%) subjects, respectively. Forty-one (32.8%) subjects had at least one readmission. The average CGI-S score for the total subjects was 5 (markedly ill) at baseline and 2 (borderline ill) at the end of their latest contact with the tertiary care hospital. For the 34 subjects (27.2%) who had follow-up information of 15 years, the average CGI-S score was 1 (normal, not at all ill) at the end of 15 years (P < 0.001).
Conclusion:
Clinical outcomes of prisoners with mental illness seem promising, subject to the seamless availability of services. Studies from other parts of the country are required for a more systematic understanding of the requirements of care.
Studies from developed countries have highlighted an important issue of clinical deterioration among prisoners following discharge from their hospitals. In our study, Schizophrenia spectrum disorders, mood disorders, and alcohol use disorders were diagnosed in 49.6%, 17.6%, and 35.2% out of the 125 patients studied. The average Clinical and Global Improvement—Severity (CGI-S) score was 5 (markedly ill) at baseline and 2 (borderline ill) at the end of their latest contact with the tertiary care hospital. For nearly 27% patients (who had follow-up information of 15 years), the average CGI-S score was 1 (normal, not at all ill) at the end of 15 years. In this study, the clinical outcomes of patients improved which was possibly secondary to availability of mental health services inside prisons and liaison facilities.Key Messages:
Prisons have a disproportionately high prevalence of mental illness or substance-use-related problems across the globe. 1 Trans-institutionalization, importation hypothesis, and psychosocial adversities in the prisons have been reported as important factors responsible for the higher prevalence.2, 3 Therefore, it is imperative to ensure the care and treatment of prisoners with mental illness. The right to care and treatment has been identified through various international and national conventions on prisoners’ rights and their legislation.4–6 In this context, India, one of the largest low- and middle-income countries, has made several legal provisions for the treatment of prisoners with mental illness under the Mental Healthcare Act, 2017. 6 The method, modalities, and procedure for transfer of prisoners to the medical wing of the prison or a Mental Health Establishment have been listed under section 103(6), while standards and procedures of mental health services in prison, such as screening, ensuring availability of medications, protocols for dealing with high-risk behavior, availability of psychosocial interventions, etc., have been listed under section 103(7). 6 Despite such provisions, the treatment of prisoners with mental illness might be hampered due to the lack of available resources in the prison, particularly in low- and middle-income countries.7, 8
The complexity of this scenario increases when the prisoners have serious charges against them, such as homicide. Invariably, these individuals have a compromised social support system due to perceived dangerousness, stigma, and lengthy legal proceedings, adding to their psychological distress. The prevalence of mental illness in homicide perpetrators ranges widely from 4% to 40%.9, 10 Similarly, the presence of psychosis increases the odds of homicide to as high as 19.5 folds. 11 These show the bidirectional relationship between mental illness and homicide in the prison. 11
Psychosis, depression, substance abuse, and personality disorders are important mental health conditions reported to be highly prevalent among prisoners, with prevalence rates between 14% and 20%. 1 These conditions are treated in the hospitals established within the prison or in various health establishments outside the prison. However, little is known about what happens to the clinical conditions of the prisoners in the long-run. Studies from the developed nations, with follow-up periods ranging from 3 to 29 years, have found that the hospital readmission rates of homicide offenders with mental illness following discharge from a hospital have been 33%–80%.12–14 This highlights an important issue among prisoners of clinical deterioration following discharge. Similar studies are lacking from low- and middle-income countries. Studies from India have examined the clinical profile of prisoners with mental illness cross-sectionally; however, no study could be identified that has examined the long-term clinical outcomes of prisoners with mental illness. 15 Given this context, this study was conceptualized to explore the clinical profile, course, and outcomes of male inpatients with the charges of homicide in a forensic psychiatry setting.
Material and Methods
Study Set-Up and Design
This is a retrospective review of case charts of the patients admitted to the prison psychiatry ward at the National Institute of Mental Health and Neurosciences (NIMHANS), a tertiary care hospital (TCH) in South India, between January 1, 2003, and December 31, 2016. The year 2003 was chosen because a dedicated male prison psychiatry ward was started and a separate registry for these patients was maintained at the TCH starting this year. Female prison patients were not included in the study due to the absence of an exclusive registry for female prison ward admissions. The TCH provides outpatient and inpatient forensic psychiatric services to prison patients with mental illness (both under-trial or convicted). The Bengaluru Central Prison (BCP) refers the patients to the TCH. A psychiatrist admits a patient to the TCH based on clinical complexities involved in the case management or court orders. It is emphasized here that, generally, not all patients referred to TCH are admitted. Only if there is a clinical indication for admission, such as diagnostic clarification, need for a supervised and longitudinal assessment, or a court order for evaluation/treatment/certification, is the patient admitted. After admission, the diagnosis is made by a consultant psychiatrist after serial interviews and assessments. The consultant psychiatrists at TCH follow the International Classification of Diseases (ICD-10) criteria for the same. After discharge from the TCH, patients return to the BCP from where they either continue staying there or are referred back to their primary prisons (en-route prisoners). En-route prisoners are those who are referred from other prisons throughout the state of Karnataka to the BCP and thereafter to TCH for treatment. The model of the network between various prisons, the BCP, and the TCH has been illustrated in Figure 1.
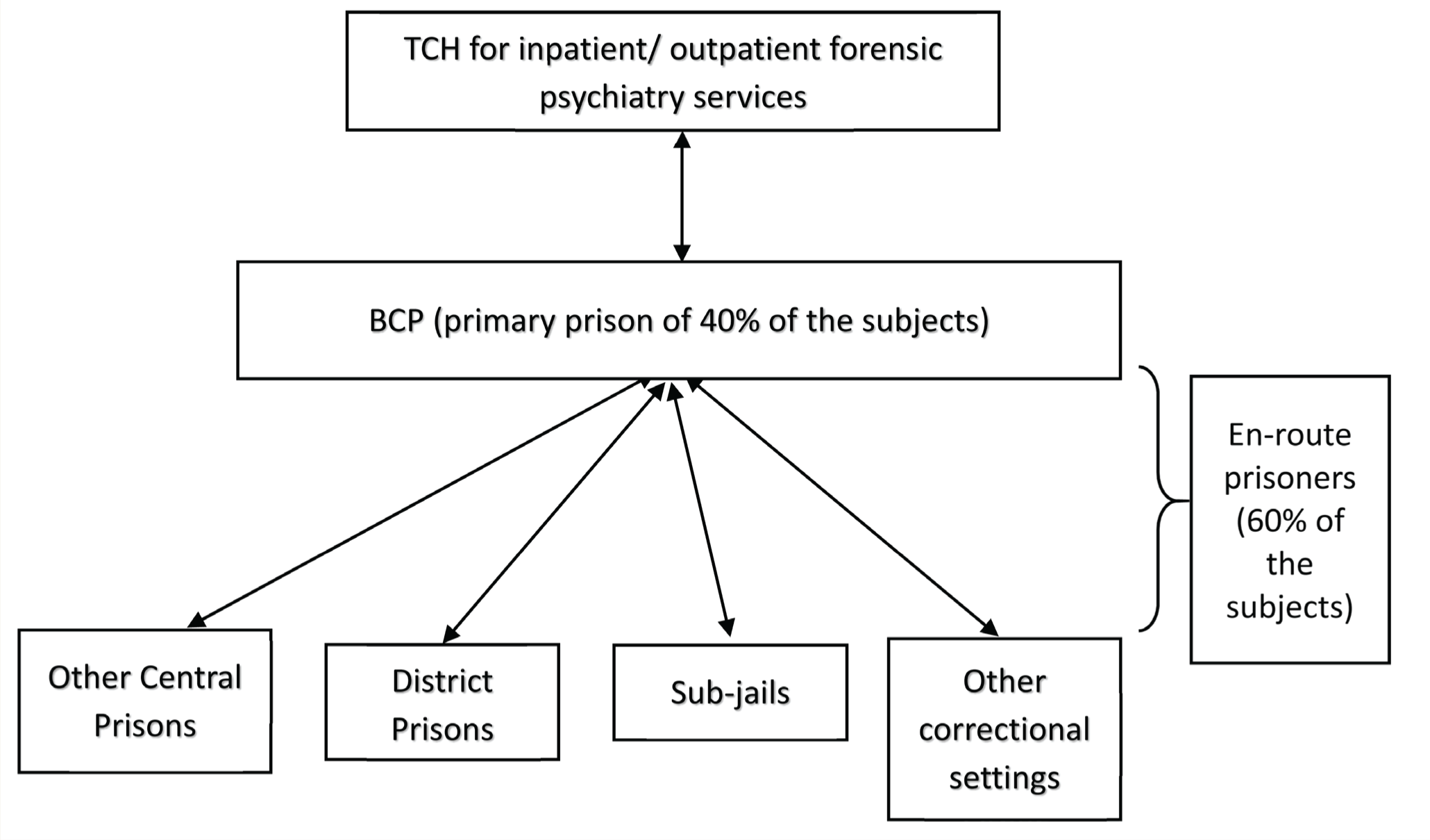
BCP: Bengaluru Central Prison, TCH: Tertiary Care Hospital.
Inclusion Criteria: All male patients, aged more than 18 years, meeting ICD-10 criteria for a psychiatric diagnosis, and charged (under-trial or convicted) under section 302 of the Indian Penal Code (punishment for homicide). In case the subject had multiple admissions at the TCH, the admission in which the patient first had the charges of section 302 IPC (and falling within the study period) was considered the point of entry into the study. Exclusion criteria: Those prisoners who were inpatients at the TCH but did not fulfill the ICD-10 criteria for a psychiatric diagnosis (e.g., diagnosis of malingering).
Procedure and Assessment Tool
Figure 2 illustrates the screening procedure used to recruit the subjects for the study. A modified version of the structured data extraction tool used by Kumar et al. was utilized. 15 Modification in the tool was done to incorporate the longitudinal data. The modified tool had two components: (a) sociodemographic profile and (b) clinical variables. To ascertain the clinical severity of symptoms, all the follow-up dates and the Clinical Global Impression- Severity (CGI-S) scores at each follow-up of the patient were obtained based on the clinical notes in the file. All the data was collected by a psychiatrist (BV). If there was difficulty deciphering the information in the files, the same was clarified with the consultant psychiatrist (CNK). Also, CNK was involved in supervising the entire process of data collection. After the data collection was completed, 10% of the files were randomly chosen, and data entry was reviewed by BV to assess if there was any inaccuracy in documenting the data. The outcome was measured using the change in the CGI-S of the patients during various time points in comparison with their baseline CGI-S scores.
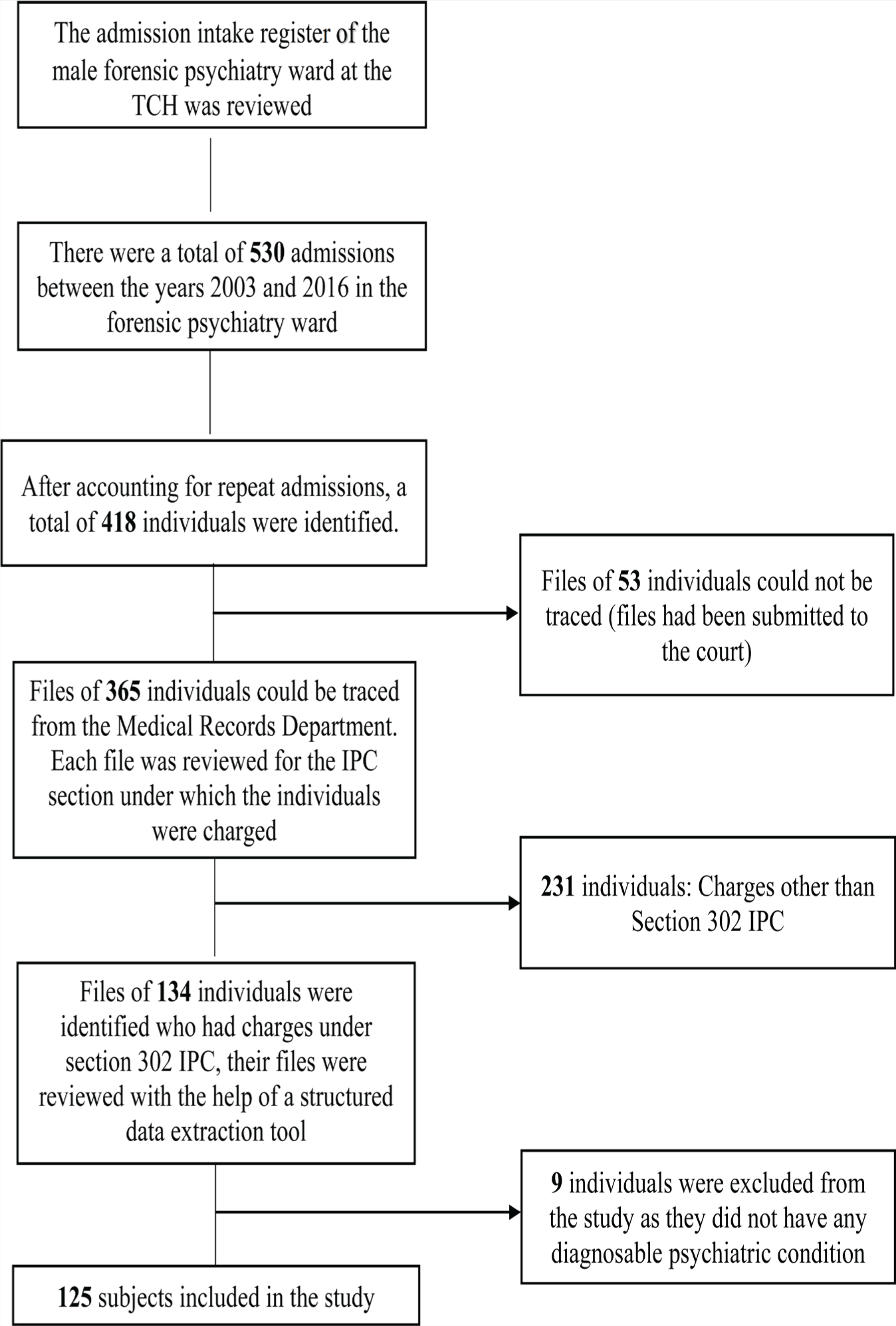
IPC: Indian Penal Code, TCH: Tertiary Care Hospital.
Statistical Analysis
The data was analyzed using IBM SPSS version 22 for Windows. Frequency and percentages have been used to describe categorical variables. The normality of continuous variables was assessed using the Shapiro–Wilk test. Since the variables were skewed, the median (Q1, Q3) has been reported for continuous/ordinal variables. Friedman test with Dunn’s post hoc test was used to assess the change in the CGI-S scores over the follow-up period for the subjects who had follow-up details for 15 years.
Ethical Aspects
Ethical considerations related to research in the vulnerable population (prisoners) as per the Indian Council of Medical Research guidelines were followed, and the Ethics Committee of the TCH approved the study.
Results
Sociodemographic Profile, Baseline Referral Status, and Clinical Features
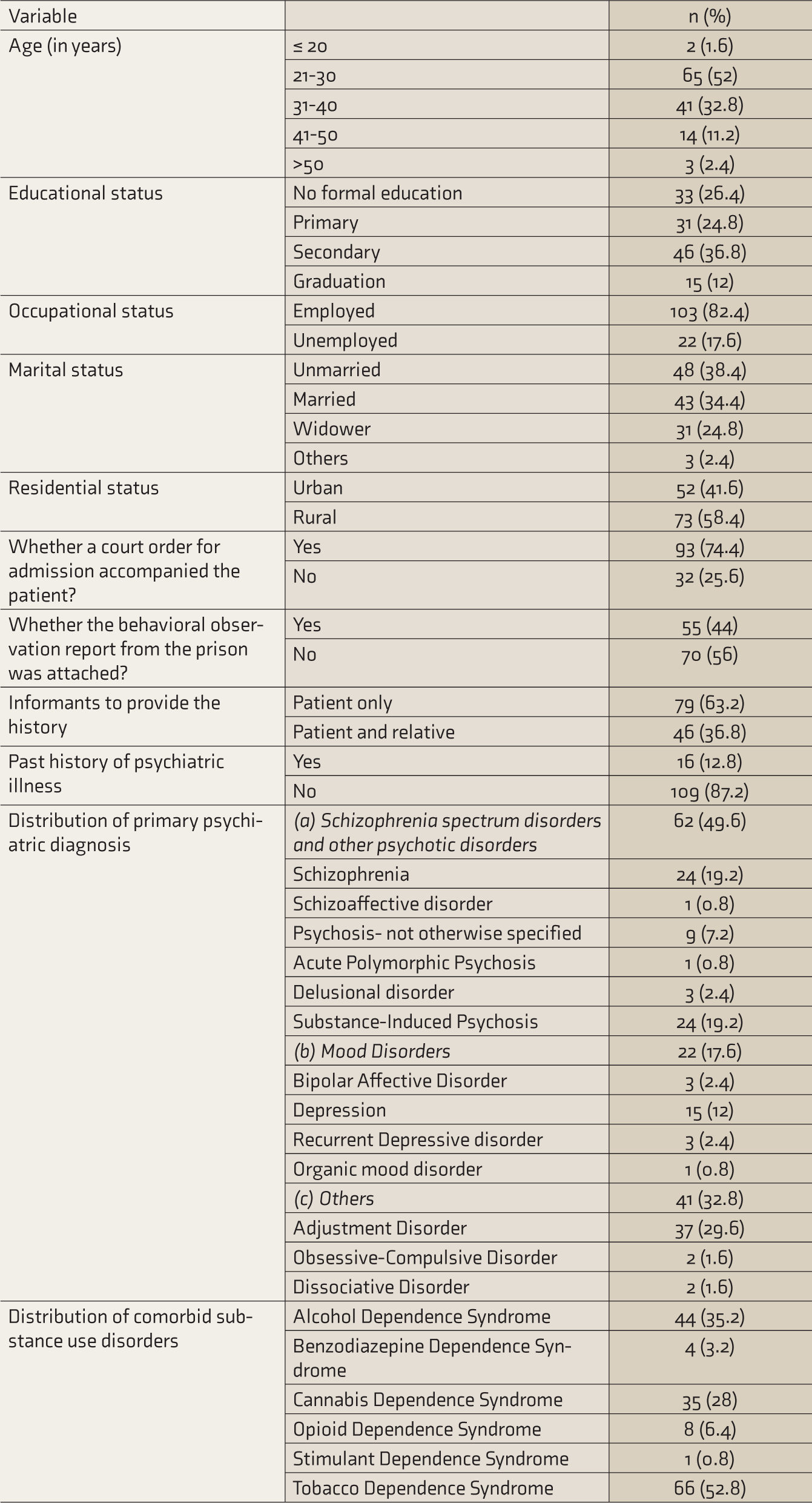
The total sample size was 125, with a median age of 30 (26, 36) years and education of 9 (0, 14) years. Sixty percent were en-route prisoners. The remaining 40% had BCP as their primary prison. The median duration of imprisonment before the first admission was 12.5 (2.38, 48) months. The median duration of admission at the TCH and the duration of illness before the first contact with the TCH were 26 (16, 39) and 75 (14, 730) days, respectively. Other sociodemographic variables, baseline referral status, and clinical characteristics of the patients after assessment and management at the TCH are in Table 1.
Socio-Demographic Profile and Clinical Characteristics (n=125)
Clinical Course and Outcome of the Patients
The duration of contact with TCH was defined as the period between the first admission at the TCH till the latest follow-up on an inpatient or outpatient basis with the TCH. The median duration of contact with TCH was 24 (3.7, 68.5) months and ranged 0.13–240 months. The median number of follow-up visits with the TCH post-discharge was 6 (1, 10) and ranged 0–28. Patients with follow-up of up to 15 years were 34 (27.2%). Forty-one (32.8%) had readmissions. The median number of admissions at the TCH was 1 (1, 2). Common reasons for readmission were self-harm attempts, recurrence or relapse of symptoms, assessment of fitness, and substance-related behavioral disturbances.
The median CGI-S score for the total subjects (n = 125) was 5 (markedly ill) at baseline and 2 (borderline ill) at the end of their latest contact with TCH (P < 0.001). For subjects who had follow-up information for 15 years, the median CGI score was 5 (markedly ill) at the baseline, 3 (mildly ill) at the end of 1 year, 2 (borderline ill) at the end of 5 years, and 1 (normal, not at all ill) at the end of 15 years. The results of Friedman’s test with Dunn’s post hoc analysis indicated a significant change in the CGI-S scores (P < 0.001) from baseline to 15 years. The analysis was also carried out within each diagnostic group. There was a significant change in the CGI-S scores in Schizophrenia spectrum disorders and other psychotic disorders (x 2 = 129.03, P < 0.001), mood disorders (x 2 = 48.24, P < 0.001), and “others” diagnostic categories (x 2 = 64.9, P < 0.001). Table 2 depicts the change in the CGI-S scores of patients during the follow-up period.
The Change in the CGI-S Scores.
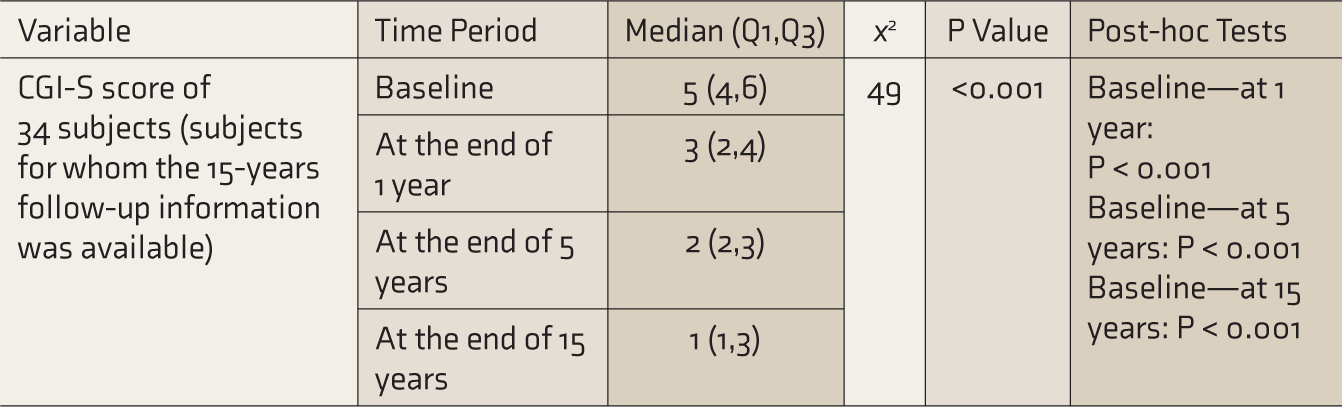
CGI-S: Clinical and Global Improvement—Severity.
Discussion
To authors’ best knowledge, this is the first longitudinal study on the clinical outcome of patients admitted to a forensic psychiatry ward in India. Nearly three-fourths of the patients had a court order for admission. About half had a diagnosis of Schizophrenia Spectrum Disorders or Tobacco Dependence Syndrome, and around one-sixth had a history of psychiatric illness before the alleged crime. The median CGI-S score for the total subjects (n = 125) was 5 (markedly ill) at baseline and 2 (borderline ill) at the end of their latest contact with TCH. Around one-third of the patients had readmission, and about one-fourth of the patients (with follow-up treatment records of 15 years) showed significant improvement in their clinical condition over time, as depicted through the change in the average CGI-S scores.
Interestingly, 9 inpatients (6.7%) were excluded from the study as they did not have a diagnosable mental illness clinically and as per ICD-10 criteria. This is reflective of the usage of psychiatric illness as a possible loophole and for personal benefits of the prisoners, such as bail on medical grounds, gains in the legal proceedings such as acquittal, delay in the trial due to unfitness, etc. Forensic psychiatrists should be aware of this and routinely assess for the possibility of malingering in their clinical practice.
Most patients were in the third or fourth decade of their life, and the median years of their education were 9 years, consistent with earlier studies.15, 16 Nearly half of the patients were diagnosed with Schizophrenia Spectrum Disorder and other psychotic disorders. This could be due to reasons such as (a) the behavioral disturbances in patients with psychosis such as muttering to self, disorganized behavior, aggression, food refusal, etc., may be easily identified by the prison staff who facilitate the referral, while conditions such as somatization or mild depression may not be identified and hence not referred, (b) fitness to stand trial is usually compromised in patients with psychosis and therefore they get referred from the court for assessment and treatment, and (c) patients with psychosis require a long-term intervention as against conditions such as adjustment disorders, thereby providing a larger window for referral. Earlier studies done at referral centers for prisoners with mental illness have also reported similar numbers.13, 15 One-third of the patients had a neurotic illness, consistent with earlier studies. 17
One-third of the subjects were readmitted at least once. A study from the west reported readmission rates of 33% within two and 80% within 15 years of discharge. 16 High rates of readmission in developing countries could be due to the following factors: (a) forensic psychiatric services differ in developed countries, which offer closer supervision of patients into the community post-discharge, and (b) most studies done in the developed countries have looked at the clinical course post-discharge from the prison when the patient is either acquitted or has obtained a conditional discharge.12, 16
A total of 34 (27.2%) patients had follow-up for 15 years. This reflects possibilities such as: (a) Recency of the admission. For example, those admitted in 2016 had shorter treatment records in comparison to those admitted in 2003. (b) The primary reason for referral to a higher center being already fulfilled, as seen in cases requiring certification, etc., and the subsequent treatment being managed locally by the psychiatrists posted in prisons.
The trend of change in clinical status of the 34 subjects with treatment records of 15 years points towards a significant improvement in the average CGI-S scores. The possible factors for promising clinical outcomes could be the availability of mental health professionals, treatment in prisons and effective collaborative liaison psychiatric practice. Earlier studies in the community settings as well as prisons have highlighted the success of collaborative care services between a psychiatrist and health care providers in a peripheral center, facilitating capacity building and service delivery.18–20 This collaboration could be onsite or through telemedicine. Through this study, we recommend (a) that prison settings need to have networking and collaborative liaison psychiatric services with mental health establishments for seamless availability of treatment for prisoners with mental illness, and (b) mandatory screening of prisoners with mental illness and substance use for timely initiation of treatment/referral to higher center.
This is the first real-world, longitudinal, comprehensive study on the clinical outcomes of patients admitted to the forensic psychiatry ward of a hospital in India. In addition, the study has a large sample size specific to prisoners with charges of homicide and is without any pre-formulated hypothesis, preventing investigator bias. However, the study has the following methodological limitations (a) retrospective nature of assessment including the CGI-S scoring that was done retrospectively based on the data available in files; (b) female prison patients were not included; (c) the diagnosis of personality disorders was not included in the study primarily because to establish this diagnosis, most often, corroborative and reliable source of history is required and we need the patients to cooperate for the assessments, in the absence of which there is a possibility that the data may be skewed. Hence, we decided not to include this as a diagnosis for the patients in this study; and (d) there may be a Berksonian bias as the study was conducted in a TCH where patients with greater clinical complexities are usually referred.
Conclusion
Schizophrenia, mood, and substance use disorders are common psychiatric diagnoses among male inpatients with mental illness with the charges of homicide. The study shows promising clinical outcomes for prisoners with mental illness in terms of improving the severity of illness, possibly due to effective networking and availability of collaborative psychiatric services between the prisons and the TCH. However, studies from other parts of the country are the need of the hour for a more systematic understanding of the nuances and requirements of care.
Footnotes
Acknowledgements
The authors thank for the support received from all the stakeholders and the staff of Central Prison Bengaluru, India
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.