
Abstract
Background:
Investigating the underlying psychosocial factors is a cornerstone of planning need-based intervention for adult males accused of rape. Unresolved debates on its etiology, mediation, or interaction among causal psychosocial variables fuel curiosity to scrutinize it further. Hence, we studied potential influence of and relation between adverse childhood experiences, aggression, empathy, and psychopathology in adult males accused of rape in India and investigated the risk factors for the same.
Methods:
With a correlational research design, 40 literate and consenting adult males medically confirmed for rape were recruited using convenient sampling. The assessment was done on Adverse Childhood Experiences, Aggression Questionnaire, Symptom Checklist-90, and Interpersonal Reactivity Index. Descriptive statistics, Pearson’s product–moment correlation, and stepwise linear regression analysis were calculated.
Results:
Approximately 75% of the participants experienced at least one category of Adverse Childhood Experiences. Scores above cut-off points were obtained on anger, hostility, fantasy, and personal distress. Significant correlations were obtained between adverse childhood experiences and psychopathology; between hostility and psychopathology, perspective taking, and personal distress; and in case of indirect aggression, with perspective taking and empathetic concerns. Regression analysis revealed that an increase in Symptom Checklist-90 global scores increases hostility and that lower personal distress predicts higher scores on hostility on Aggression Questionnaire.
Conclusions:
Adverse childhood experiences, aggression, and psychopathology play a critical role and, therefore, should be included as core components of the prevention of rape or relapse prevention programs at the community level.
Commitment of rape has been associated with single or multiple adverse childhood experiences, and hence, must be assessed comprehensively while conceptualizing the etiology of offense or development of sexually violent behavior. Anger, hostility, and psychopathology are associated with the commitment of rape. Hostility in men accused of rape should be explored within interpersonal relationship difficulties as well as psychopathology (if any) experienced. Psychological intervention for men accused of rape must incorporate a two-fold focus: adequately addressing early childhood trauma and the psychosocial distress they experience.Key Messages:
India has witnessed a massive increase in violent sexual crimes against females. A total of 32,559 rapes were reported in 2017, and as many as 109 children were sexually abused every day in 2018, which was a 22% jump in such cases. 1 Extensive research over the past three decades in the West suggests diverse mental health issues that underlie sexual violence and offending. Over the years, research on factors leading to sexual offenses has focused on the family and personal characteristics of the offenders. The role of a pathological family atmosphere, early traumatic sexual experiences, sexual interest, and sexual frustration 2 has been emphasized. Research on personal characteristics highlighted the role of adverse childhood experiences (ACE) such as sexual abuse, physical abuse, and dysfunctional family relations, which could affect offenders’ capacity to form secure attachments and develop healthy adult relationships. 3 Higher ACE in general population have been associated with poor mental and physical heath. 4 In sexual offenders, ACE are reported more frequently when compared to criminals with nonsexual offenses and males in the general population. 5 In fact, history of at least one ACE is described by majority of the male sexual offenders, and nearly half disclose four or more such experiences. 5 Although researchers agree that myriad factors likely interact to lead to perpetration of sexual assault, the exact combination of which likely varies among perpetrators. 6
For many men, the origin of violence towards women has been shown to lie in childhood, with men who later rape reporting much greater exposure to abuse and adversity in childhood. Such experiences induce intimacy deficits, 7 with insensitive and detached interpersonal style of relating 8 and dismissive attachment pattern characterized by hostility to, suspicion of, and unempathetic and callous attitudes toward attachment figures. 9 The findings are intriguing and sometimes have been scrutinized for the use of multiple methodologies (e.g., the use of emotionally laden terms such as “abuse”) having potentiality to impact the results in a skewed manner. 10 A fairly large body of research across the past two decades has employed the Adverse Childhood Experiences Scale (ACES) and has been able to obtain corroborative and reliable pieces of evidence on the association between abuse and adult criminality. Coagulative evidence suggests that sexual offenders report nearly four times as many adverse events in childhood on ACES compared to 16% to 17% of sexual victimization reported in the general male population.11,12 The findings necessitate indigenous scientific inquiry to its prevalence on the ACES.
In fact, aggression and deficits in empathy have long been speculated to be the probable mechanism. Though separate pieces of evidence exist for each, 13 a connection between the two was proposed by Feshbach. 14 According to Feshbach, an empathetic observer experiences high distress when witnessing aggression. Such distress was hypothesized by Feshbach to act as an inhibitor of aggression and violence. However, men who are sexually violent, especially those with history of committing multiple offenses, are more likely to lack empathy or remorse for their victims and tend to blame their victims for the rape. 13 A moderately large body of literature in West has also emphasized that ACE, 6 empathy deficits, sex-related cognition, 14 and family history of sexual offense 15 are some of the primary factors associated with commitment of sexual offenses.
Similarly, questions around whether psychopathology has a causal link with sexual offense remain debatable. Some postulate that psychiatric symptoms might contribute to sexual aggression, 16 while others speculate that they may be just co-existing, not contributory. For example, it has been reported that those diagnosed with schizophrenia are four times more likely to commit serious sexual offense than those without history of any such mental illness. 17 In most cases, the causation of the offense is multifactorial. Thus, in order to delineate this complex set of factors, a comprehensive assessment is essential.
At the international level, currently, efforts on relapse prevention among sexual offenders (e.g., rape relapse prevention and others) are being clinically tested. 18 However, in India, studies on sexual offenders are only limited to case study, 19 a few descriptive studies, 20 and a few forensic studies. 21 Despite the urgency of the research discussed, there is a lack of meaningful research on sexual offenders in India, which highlights a serious lacuna in the knowledge and skills required to manage mental health factors that underlie criminal activities. 22 Although qualitative studies do support the findings of global research on the relationship between ACE and adult sexual offending, there is not even a single Indian study establishing that. Besides, the psychosocial relapse prevention and other intervention programs, which gained popularity in bringing down the incidences of repeat sexual offenses in the West, cannot be planned in India without exploring the emotional-social-cognitive and psychopathology profile of the offenders. Hence, this study attempts to find out some such risk factors with an intention of developing relapse prevention intervention for this group in the future.
The present study aimed to explore the association among ACE, aggression, empathy, and psychopathology in adult males accused of rape and, using regression analysis, to identify risk factors for rape.
Materials and Methods
Participants
The study adopted a correlational design and used a purposive and consecutive sampling method. All the adult males accused of rape presented for medical examination at Department of Forensic Medicine and Toxicology in All India Institute of Medical Sciences were approached. Samples were recruited only after it was medically confirmed of rape but when already in police custody with ongoing legal proceedings. The inclusion criteria were as follows: (a) 18–60 years of age, and (b) have been accused with a case of sexual assault after confirmation of rape through a medical examination. After providing them with due information on the study, those who gave written consent for participation were recruited for the study. Initially, a total of 44 participants were approached (during a period of 6 months) after taking verbal approval from the police. However, out of 44, 2 refused to participate and another 2 refused to complete all the measures; therefore, 4 accused were excluded from the sample. Thus, a total of 40 adult males were included.
The term “accused” in the present study refers to adults above 18 years of age who have been charged with committing a crime of rape either once or repeatedly and have been booked under the law of the land for the same. The definition of “rape” was adopted as defined in the Criminal Law (Amendment) Act, 2013. 23
Tools Used
Semistructured Sociodemographic Data Sheet was constructed for the study. It included information regarding the participant’s personal history, along with a description of the nature of the sexual crime committed.
Hindi Translation
The scales were translated into Hindi following the WHO scale translation method and pilot tested on a sample of five adult males accused of a sexual offense. The result of the analysis suggested language refinement, which was subsequently incorporated. These five pilot participants were not included in the final sample.
Procedure
A clinical psychologist administered all the above mentioned tools, beginning from the semistructured sociodemographic sheet. After data collection, detailed debriefing session was planned. However, due to time limitations imposed by police officials for the visit of the participants at the center, it could only be done in a brief way.
Data collection commenced in August 2016 and was completed by March 2018.
Statistical Analysis
The data analysis was done using SPSS 24.0. Frequency and percentage analysis were done for sociodemographic characteristics of the respondents and ACES, while mean and SD were calculated for SCL-90, AQ, and IRI. Pearson’s product–moment correlation was computed between scores from ACE, SCL-90, AQ, and IRI. Significant correlations were then subjected to stepwise multiple linear regression analysis for which the basic assumption of linearity, normality, and homoscedasticity were met. To conduct the analysis, a list of all possible independent variable pool was tested for each of the dependent scale variables, i.e., aggression, empathy, and psychopathology, which led to a set of independent variables using the bidirectional elimination process. The only limitation, however, was the small sample size such that despite being representative, five observations per variable could not be achieved. Thus, the model may be expected to have low accuracy.
Ethical Considerations
The present study declares compliance with all the ethical standards as mentioned in the Helsinki Declaration (2013). Additionally, the study also received clearance from the Institute Ethics Committee. Written informed consent was obtained from all the participants prior to data collection, along with assuring their right to withdraw at any point during the study and confidentiality.
Results
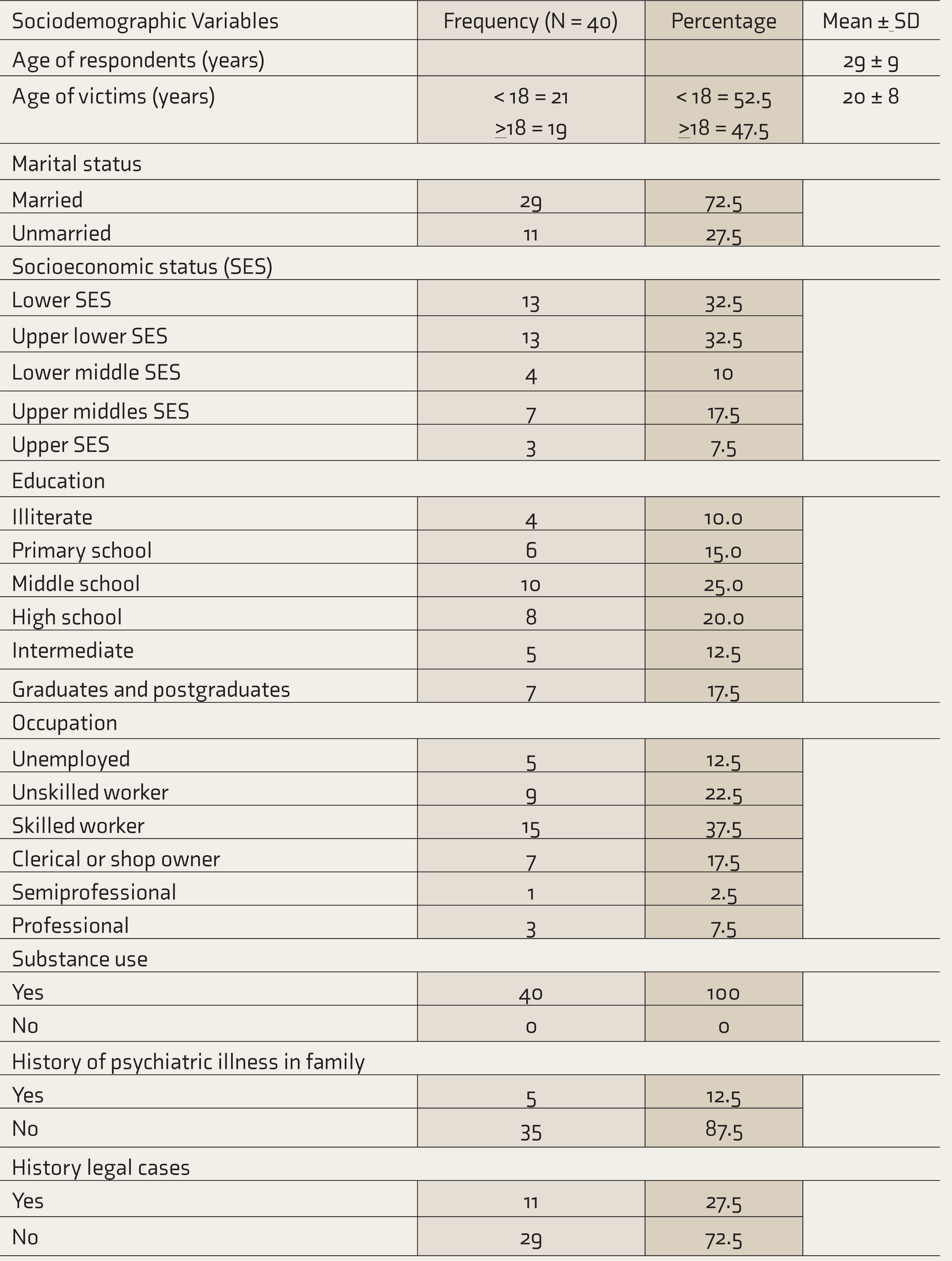
Table 1 presents the analysis of the sociodemographic details of the respondents. The mean age was 29 years (SD 9 years), with majority educated till middle (25%) or high school (20%) and employed as either skilled (37.5%) or unskilled worker (22.5%). Interestingly, 52.5% of their reported victims were below 18 years of age. Most of the respondents were married (72.5%) and belonged to lower (32.5%) or upper-lower socioeconomic status (32.5%) as assessed on revised Kuppuswamy socioeconomic status scales. 28 Nearly 50% reported consuming alcohol on a daily basis, while 42.5% consumed nicotine and opium, and 7.5% used some other substance. Thus, all the respondents (100%) reported a history of some kind of substance use, including alcohol, nicotine, opium, and other substances.
Sociodemographic Characteristics of the Respondents
Analysis across various score categories of ACE indicated that 30 (75%) participants had experienced at least one category of ACE. The difference between those reporting at least one category of ACE and those who reported no such experience was statistically significant (P < 0.001). While two (25%) participants reported experiencing at least two ACS, five (12.5%) people had a history of experiencing ≥5 ACS.
Table 2 presents the domain analysis of ACE categories.
Details on Adverse Childhood Experience Scale (ACES)
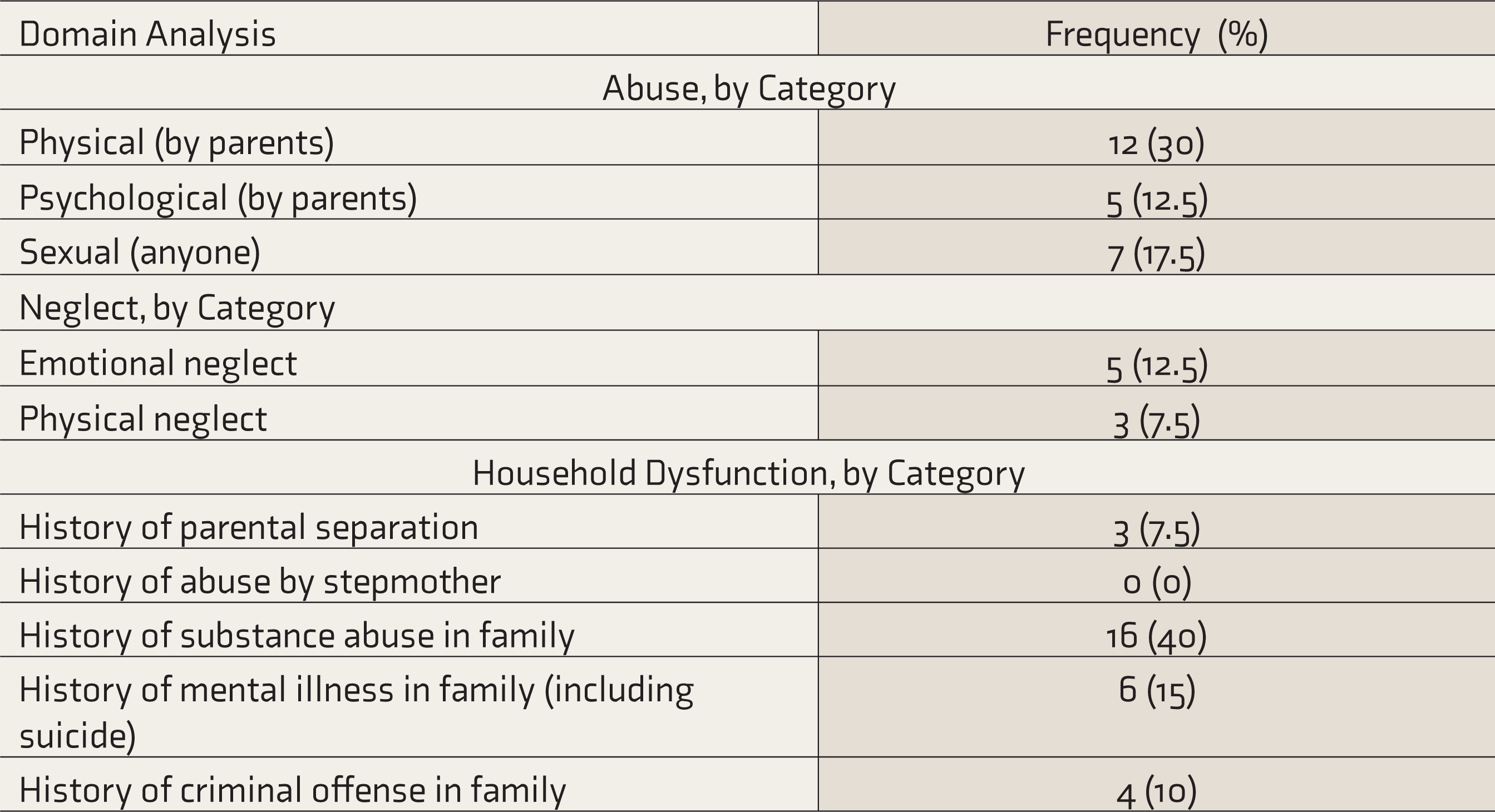
Table 3 shows the mean and SD scores across various scales and their domains. Comparative analysis of scores based on norm value taken indicated that the mean score on aggression (AQ) total is above its norm values. The domain analysis indicated higher subdomain scores on Anger (A) and hostility (HO). On the IRI, respondents scored above norm value on the FS and PD scales.
Descriptive Analysis of Scores across SCL-90, AQ, and IRI
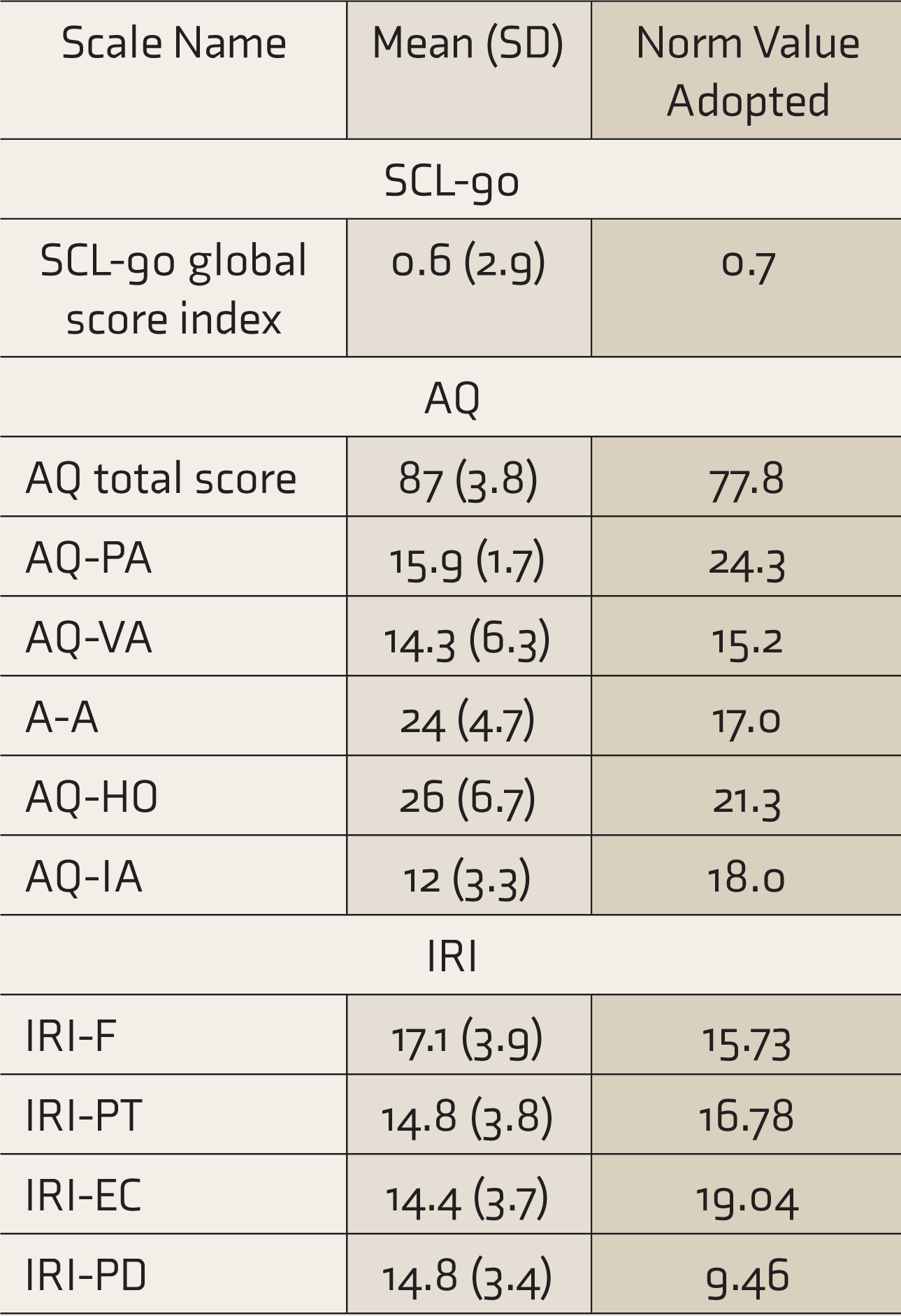
AQ, Aggression Questionnaire; AQ-A, AQ Anger; AQ-HO, AQ Hostility; AQ-IA, AQ Indirect Aggression; AQ-PA, AQ-Physical Aggression; AQ-VA, AQ Verbal Aggression; IRI, Interpersonal Reactivity Index; IRI-EC, IRI Empathetic Concern; IRI-F, IRI-Fantasy Scale; IRI-PD, IRI Psychological Distress; IRI-PT, IRI-Perspective Taking; SCL-90, Symptom Checklist-90.
Table 4 reveals the correlations between scores on various scales and their subdomains, which indicated that ACE shared a significant positive correlation with SCL global scores. Further, AQ-HO shared a significant correlation with SCL global cores, IRI-PT, and IRI-PD. IRI subdomains PT and EC shared a significant correlation with indirect aggression. All the other scale subdomains shared significant positive relationships with each other.
Correlation of Scores on Scale ACE, SCL-90, AQ, and IRI
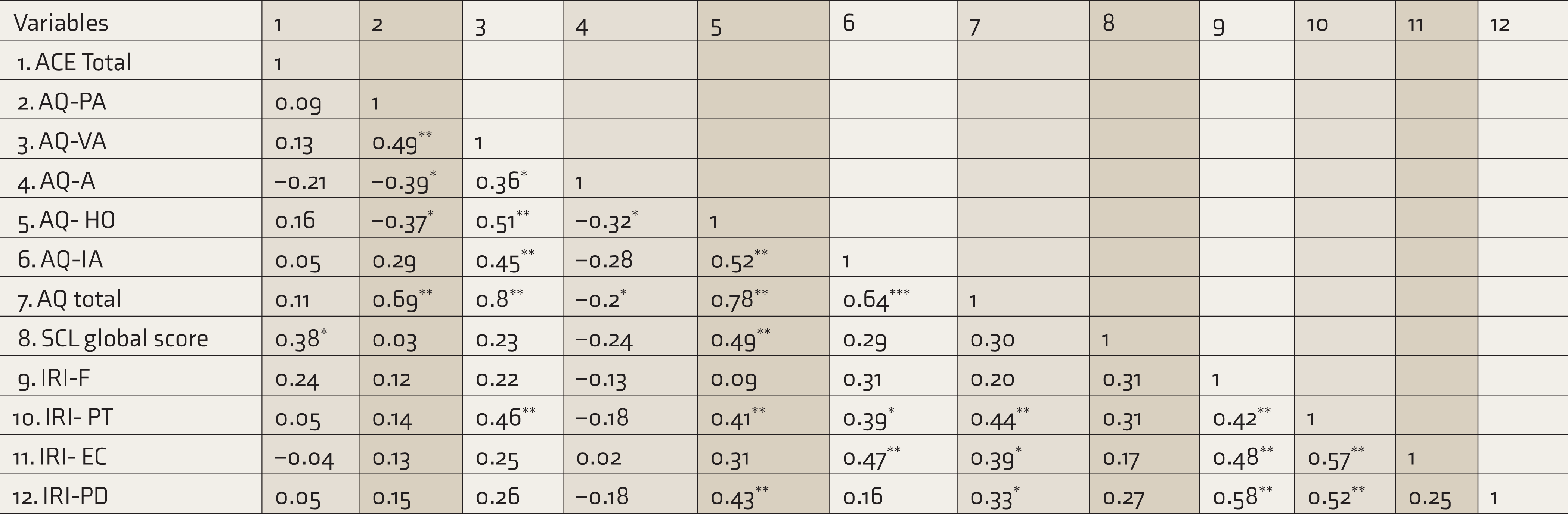
ACE, Adverse Childhood Experiences; AQ, Aggression Questionnaire; AQ-A, AQ Anger; AQ-HO, AQ Hostility; AQ-IA, AQ Indirect Aggression; AQ-PA, AQ-Physical Aggression; AQ-VA, AQ Verbal Aggression; IRI, Interpersonal Reactivity Index; IRI-EC, IRI Empathetic Concern; IRI-F, IRI-Fantasy Scale; IRI-PD, IRI Psychological Distress; IRI-PT, IRI- Perspective Taking; OCD, obsessive compulsive disorder; RES, Rape Empathy Scale; SCL-90, Symptom Checklist-90 *P < 0.05. **P < 0.01. ***P < 0.001.
Table 5 reveals that across multiple models tested, significant results were obtained only for a model that had ACE, SCL global scores, and IRI, all domains as independent variables, with AQ hostility as the dependent variable. The regression model was significant (F = 6.291; P < 0.001), with an R 2 of 0.534, indicating that the model has satisfactory explanation power for explaining the AQ hostility scores. Though the relationship between variables is complex, it is interesting to note the additive nature of the predictor variables in determining AQ hostility. As the table shows, ACS alone contributed 15% of the variance; combined with psychopathology, they together contributed 39%. Thus, 24% variance was added alone by the psychopathology of the participants. Similarly, another 18% of the variance was contributed by personal distress, thus taking the total variance to 57%. Moreover, these three variables contributed positively to the hostility of offenders towards the victims.
Stepwise Regression on Aggression (Hostility)
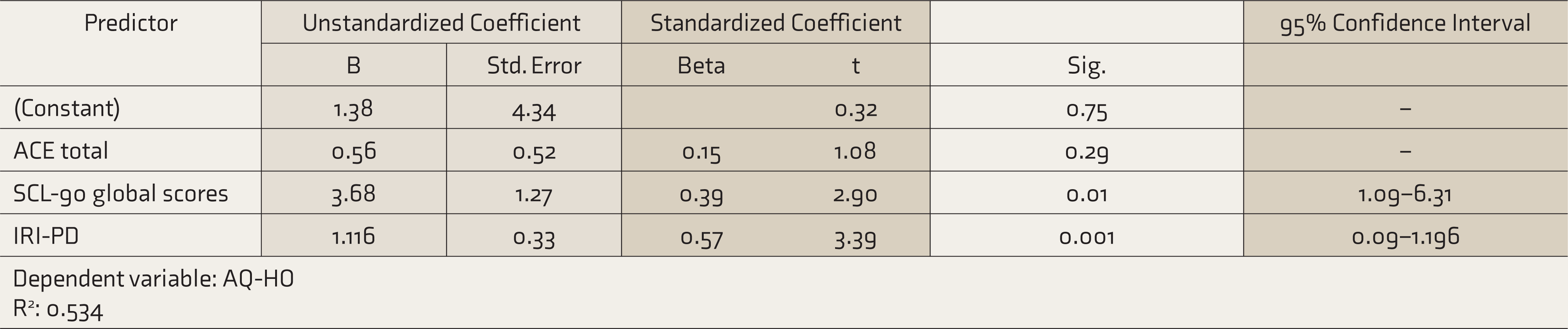
ACE, Adverse Childhood Experiences; AQ-HO, AQ Hostility; IRI-PD, IRI Psychological Distress; SCL-90, Symptom Checklist-90.
Discussion
One of our first and primary findings suggests that 75% of the participants reported experiencing at least one category of ACE. In fact, domain analysis indicated that physical abuse was one of the most commonly reported abuses, followed by sexual abuse, psychological abuse, and neglect. Importantly, while one in four participants reported having at least two ACE, one in eight had experienced five and more adverse childhood events; this is a crucial finding of this study. Thus, one of the most deleterious consequences of childhood maltreatment is that victims are predisposed to become perpetrators of crime as a result of experiencing various psychosocial difficulties. A substantial number of studies support the pattern and predict that maltreated children are two to six times more likely to commit criminal offenses in young adulthood than those with no such history.
29
The findings of our study also support earlier findings such as:
At least one ACE is reported by majority of the male sexual offenders and nearly half report undergoing four or more such experiences in childhood.
5
Higher exposure to childhood abuse and adversities is associated with increased violence in most male sexual offenders.30,31 The sexually abused-sexual-abuser hypothesis proposes that victims with history of sexual abuse in childhood are at risk of becoming an abuser later in life. However, weaker support to the hypothesis was obtained by a prospective study examining birth cohort of 38,282 males with history of childhood maltreatment. The study nevertheless asserted that polyvictimization (i.e., exposure to multiple types of maltreatment) may significantly be associated with risk of both sexual violent and general offending.
36
In the general population, history of early childhood maltreatment and household dysfunctions are associated with poorer physical and mental health outcomes in adulthood, along with increasing the chances of committing high-risk behavior.
4
Several studies have also shown that sexual offenders with history of ACE are likely to experience significant difficulty in developing healthy adult relationship.
37
Research suggests that most of their adult interpersonal relationships are characterized by intimacy deficits, insensitivity, aloofness, hostility, and dismissive attachment pattern.
11
This suggests that adverse family background facilitates the development of aggression and perhaps dysregulated sexual behavior.38,39 A history of childhood sexual and/or physical victimization has been particularly identified more frequently in sexual offenders compared to nonsexual offenders.
40
Although this study did not have a control group, other studies report that childhood sexual abuse is reported more frequently in samples of sexual offenders when compared to criminals with nonsexual offenses (odds ratio = 3.36, 95% confidence intervals of 2.23-4.83).
11
The offender group even reported nearly four times as many ACEs than an adult male normative sample.
5
From the evidences presented above, however, it must not be assumed that childhood victimization automatically leads to sexual offending. Our findings, in fact, are different from those of many studies that found that men accused of rape have higher rates of sexual abuse in their histories than would be expected in the general population, 41 as the majority of perpetrators in our study were physically abused as a child and only 17.5% reported sexual abuse in childhood. Here, social learning theory provides a reasonable explanation of the process through which learning happens with such ACE. For example, a child who has internalized the victimization experience as normal or pleasurable in some way is more likely to adopt a belief system that is favorable to offending. For example, a person may come to believe that, “This must be normal,” or “It isn’t a bad thing, it happens to many of us.” A child who internalizes these thought processes in reaction to his or her own abuse is more likely to grow into an adult who views sexually abusive acts as less harmful. 42
Interestingly, the offenders reported experiencing high anger and hostility, both of which are cognitive and affective subtraits of the multidimensional concept of aggression measured on AQ. 43 The pattern has been confirmed in previous study where anger and hostility were commonly reported as one of the few problematic psychosocial features common to sexual offenders, pedophilic offenders, exhibitionists, and offenders with multiple paraphilias. 44 In fact, hostility often becomes the key parameter that differentiates the group of sexual offenders from nonsexual offenders. 45 A recent meta-analysis also reported that elevated levels of hostility significantly predicted sexual recidivism, violent recidivism, and general recidivism among sexual offenders. 46 The theoretical link between anger and sexual aggression has been confirmed in the literature with most studies estimating small to moderate range of associations between anger and sexual offending. 47 Our findings of a higher prevalence of physical aggression and substance use among the offenders are confirmed by research studies reporting elevated risk of sexual offending, criminal recidivism, personality disorder, and psychological comorbidity among those having history of physical abuse and substance addiction.48–50
On the scale IRI, high scores were obtained on the FS and PD scale. This is corroborated by other studies reporting that men accused of rape tend to deny commitment of their offenses, minimize the extent to which the victim suffered, and provide rationalizations for why their actions are not criminal. 51 This finding has a strong link with the cognitive distortions reported by sexual offenders. The implicit theories proposed 52 that some of the key cognitive distortions found among the rapists are that women convey their sexual needs through revealing clothes; women are sex objects and meant to be used only; male sex drive is uncontrollable and if not used immediately, it may cause premature ejaculation; males have a right to ask sex from a female they want; and research has found evidence for such beliefs. 29 Thus, sex-related cognitions play a key role in empathy deficits, and psychological treatment improves empathy levels in men accused of rape. Although we did not focus on men accused of repeated rape or find significant empathy deficits, a few studies reported sexually violent men who lack empathy and remorse for their victims and blame their victims for the rape to be often committing repeated rape. 13 Multiple offenders or repeat offenders in our study might have been guarded while answering on the scale items. Further, researchers have also suggested that IRI scores are severely affected by the social desirability response bias. Therefore, the scale may not accurately elicit adequate knowledge about the empathy of sex offenders. 53
The finding of a significant correlation between ACE and psychopathology demonstrated that ACE has a negative impact on the psychosocial well-being in adulthood.4,54 Developmental psychopathology theorists argue that pathological relational environment created due to child maltreatment deprives children of the very experiences which promotes adaptive functioning across life span.55,56 The findings can be further understood within Marshall and Marshall’s 3 well-articulated vulnerability model, which proposes that a poor parent–child attachment leads to cognitive, social, and affective deficits, which are considered as “critical elements” in understanding the etiology of sexual offending behavior.
Further, AQ-HO was found to share a significant correlation with SCL global scores. In fact, on regression analysis, it was found that higher global scores on SCL even acted as a predictor for higher hostility in men accused of rape. Though evidence exists for the link between sexual offending and psychopathology 57 and hostility,45,58 the inter-relation rewinds the debate questioning the causal link of psychopathology to sexual offending.16,17 The findings of the present study propose that psychopathology and subsequent hostility are one of the causal pathway leading to sexual aggression. However, further evidence will be required to explore and establish the same.
Regression analysis further added that lower PD on IRI predicts higher aggression in men accused of rape. Thus, a person is likely to be sexually aggressive when they lack the empathetic ability to experience distress and discomfort of the victims. 59 These findings confirm the Feshbach theory 14 that empathy acts as an inhibitor of aggression and violence. In fact, researchers have also speculated here that empathic distress acts as a precursor to the development of feelings of guilt, which further reduces aggression directly, and the absence of this connection may simply work in the opposite manner in sexual offenders. 60 Thus, the present study provides evidence for the causal link between empathy deficits and aggression.13,45
The findings from the present study bring forth the applicability of the integrated theory of sexual offending, which proposes multifactorial pathways to sexual offending. 61 Though from the outcome variables, the role of ecological and agency-level factors seems to be prominently involved, the implicit role of emotional regulation difficulties can also be derived. For example, a person with history of ACE may remain preoccupied with unfulfilled emotional need for closeness or attachment. When such emotional needs are experienced in conjunction with high sexual desire over which there is poor impulse control, propensity towards commitment of sexually aggressive crime is escalated. This may be especially true with triggered risk factors such as substance use, anger, or emotional collapses. 61 Similarly, the results from the ACES highlight the pertinence of the criminal pathway model, which explains that sexual violence against women is favored by childhood exposure to criminogenic models leading to a developmental trajectory characterized by deviance, poor frustration tolerance, and low self-control. 62 Thus, etiological pathways interact in a complex way, leading to sexual offenses, and hence, clinicians are prompted to take into account a variety of causal variables when formulating a case, to think dynamically with respect to the interactions, and to appreciate the role of ecological factors in both creating the conditions of abuse and shaping the vulnerabilities.
Limitations
The findings of this exploratory study with a small sample size, convenient sampling from accused than legally proven participants, cannot be generalized. Nevertheless, this indicated a trend of findings in this area and also facilitated the process of modification of existing commonly used scales to suit the cultural appropriateness. The study should be expanded further with a comparative sample of men not accused of rape.
Conclusions
Men accused of rape may have a history of single or multiple adverse childhood experiences, which should be routinely assessed while conceptualizing the case. They may also report significantly higher anger and hostility, which must be understood in terms of their poor perspective taking ability, empathy deficits, or the causal pathway proposed between psychopathology and hostility. The study overall brings forth the urgent need to develop a treatment framework for them which should be focused on addressing current psychosocial difficulties, childhood attachment disturbances, treatment of psychopathology, as well as prevention of sexual recidivism in future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.