
Abstract
Background:
Depression has emerged as one of the prime morbidities affecting professional and personal lives worldwide. Antidepressants are one of the mainstays of management of depressive episodes. Although antidepressants are considered a safe class of drugs, the studies examining the effects of antidepressant prescription on intraocular pressure (IOP) have shown a propensity to increase IOP, but not consistently. This study aimed to compare the changes in IOP and iridocorneal angle in drug-naïve patients with depressive episodes prescribed escitalopram or amitriptyline.
Methods:
Overall, 109 patients were recruited, of which 53 were prescribed amitriptyline and 56, escitalopram. A comparison of IOP and the iridocorneal angle at weeks 0, 4, and 8 was done using a two-way repeated-measures analysis of variance (two-way RM analysis of variance).
Results:
Patients initiated on escitalopram tended to show a higher rise in the IOP (left eye–[
Conclusions:
Escitalopram use had an association with an increase in IOP. While initiating patients on antidepressants, clinicians should be aware of this possibility, which can lead to ocular emergencies, and obtain a proper history of ocular morbidities.
Drug-naïve patients with depressive episodes who started on escitalopram tended to show a higher rise in the intraocular pressure than patients who started on amitriptyline. No difference was seen in the iridocorneal angles in the two groups.Key Messages:
Depression is one of the most common disorders worldwide and a leading cause of disability. 1 However, a significant treatment gap exists in the management of this disorder. 2 Inadequate management of depression can lead to significant morbidity in the lives of the patients and, in more unfortunate cases, to mortality too. Pharmacotherapy is one of the mainstays of the management of depression. Common agents for the management of depression include selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs).
Although, in general, antidepressants are considered a safe class of drugs, current literature speculates that antidepressants can affect intraocular pressure (IOP). Changes in the IOP can lead to glaucoma, the second leading cause of blindness worldwide. 3 TCAs are often associated with adverse effects like mydriasis or cycloplegia. TCAs can also block noradrenalin uptake and alpha-adrenergic receptors. All these can lead to an increase in the IOP. Similarly, SSRIs are also associated with increased IOP mediated via serotonergic effects on ciliary body muscle activation and pupil dilation. 4
The interest in this topic started around 2001 when the Australian Adverse Drug Reactions Advisory Committee compiled instances of raised IOP following exposure to SSRIs. 5 Subsequently, a study was published where 1465 recently diagnosed patients with acute angle-closure glaucoma were compared with 5712 persons without glaucoma, and the effect of recent initiation of SSRI was examined. After adjusting for confounding factors, the study reported a 5.8 times higher risk of acute angle-closure glaucoma after being started on SSRIs. 6 On the contrary, at least one another study studied the effects of SSRI on a long-term basis and failed to find any elevated risk of angle-closure glaucoma. 7 However, a subsequent population-based, nested case-control study on a Taiwanese registry-based sample found that SSRI had a weak association with the risk of developing glaucoma. 8 This debate gradually garnered interest, and a meta-analysis on this topic was conducted consisting of six case-control and one cohort study (N = 801,754). It concluded that exposure to serotonergic antidepressants lacked a robust association with a higher risk of glaucoma. 9
A similar approach has also been adopted for the effects of antidepressants with anticholinergic properties, like TCAs. A study followed up four patients with narrow angles on imipramine and found a rise in the IOP. 10 Similar case reports depicted a rise in IOP in patients on amitriptyline 11 and clomipramine. 12 Seitz et al. 13 observed 6470 patients aged 66 years and above to see the effects of intermittent antidepressant exposure on their IOP. It was found that all antidepressant exposure was associated with a modest increase in the risk of raised IOP. The intraclass comparison showed that antidepressants with serotonergic actions had a higher propensity than antidepressants with anticholinergic actions.
In such a background, our study was planned with the aim of (a) finding the changes occurring in IOP and iridocorneal angle in drug-naïve patients with depressive episodes using escitalopram or amitriptyline and (b) comparing the outcomes between escitalopram and amitriptyline groups. This study intends to fill the knowledge gap in this field because there is no data regarding this topic from the Indian subcontinent and a comparative approach between the two drugs has not been used. Escitalopram and amitriptyline were chosen as representatives of SSRIs and TCAs because they are arguably the most commonly prescribed drugs of the two groups.
Materials and Methods
This study was conducted in a tertiary center in Eastern India. The study obtained ethical clearance from the Institute Ethics Committee. The data were collected between May 2019 and October 2020.
Patients were recruited if they fulfilled all the following criteria: (a) diagnosed with depressive episode according to the International Classification of Disease-10th Edition (ICD-10), 14 (b) are drug-naïve, (c) aged 15 to 55 years, (d) willing to provide written informed consent, and (e) with IOP and iridocorneal angles within the normal limit as revealed by applanation tonometry and gonioscopy in the initial assessment. Patients were excluded if they had any one of the following conditions: (a) diabetes mellitus, that is, random blood sugar levels >200 mg%, fasting blood sugar >126 mg%, postprandial blood sugar >200 mg%, or glycosylated hemoglobin levels >6.5%15; (b) hypertension (systolic blood pressure >150 mm of Hg or diastolic blood pressure >90 mm of Hg); (c) glaucoma, eye trauma, receiving steroids, chronic uveitis, long-standing corneal ulcer, or advanced cataract; or (d) any psychotic symptoms.
Patients who met the inclusion and exclusion criteria were allotted treatment with either escitalopram or amitriptyline. The allocation to either of the drugs was nonrandomized. Patients were preferentially allocated to amitriptyline if they had somatic symptoms or decreased sleep. Attempts were made to match the allotment in the two groups in terms of age and gender. Subsequently, they were managed according to the clinical practice guidelines for the management of depression published by the Indian Psychiatric Society. 16 This meant that the patients were coadministered clonazepam if necessary for seven to 14 days.
On being recruited, the sociodemographic and clinical details, including blood pressure and blood sugar levels, were documented. The IOP changes were measured using applanation tonometry, and the iridocorneal angles were measured using gonioscopy and graded according to Shaffer’s system (week 0). The readings on applanation tonometry and gonioscopy were repeated on weeks 4 and 8. All the ophthalmological examinations were supervised by a single senior faculty member from Ophthalmology, who was blinded to the pharmacological therapy of the patient.
Sample size calculation was done for only one of the two primary objectives. We could not access any record citing the prevalence of escitalopram or amitriptyline-induced rise in IOP or narrowing of the iridocorneal angle. So, for sample size calculation, the standard deviation of IOP in patients who were initiated on SSRI was used. This standard deviation in a previous study was 2.17.17 Taking that into consideration, for a 99% confidence interval, and allowing 1% as an error margin, the sample size calculated was 32.
The statistical analysis was done using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA). The descriptive statistics were expressed in terms of ratio, percentage, frequency, and proportion (for categorical data) and mean with standard deviation, median, or range (for continuous data). The comparison of the measures of applanation tonometry and gonioscopy was done using a two-way repeated-measures analysis of variance (two-way RM analysis of variance [ANOVA]). Post hoc tests were conducted using Bonferroni correction.
Results
Overall, 109 patients were recruited, of whom 53 were prescribed amitriptyline and 56 were prescribed escitalopram. There were no dropouts. All the patients tolerated the prescribed medications and showed good medication adherence as assessed by a single question on follow-up. The two groups were comparable in terms of sociodemographic parameters (Table 1). The two groups also did not significantly differ in cumulative exposure to benzodiazepines (calculated in terms of total daily dose multiplied by the number of days prescribed, Table 1).
Sociodemographic Variables of Recruited Subjects
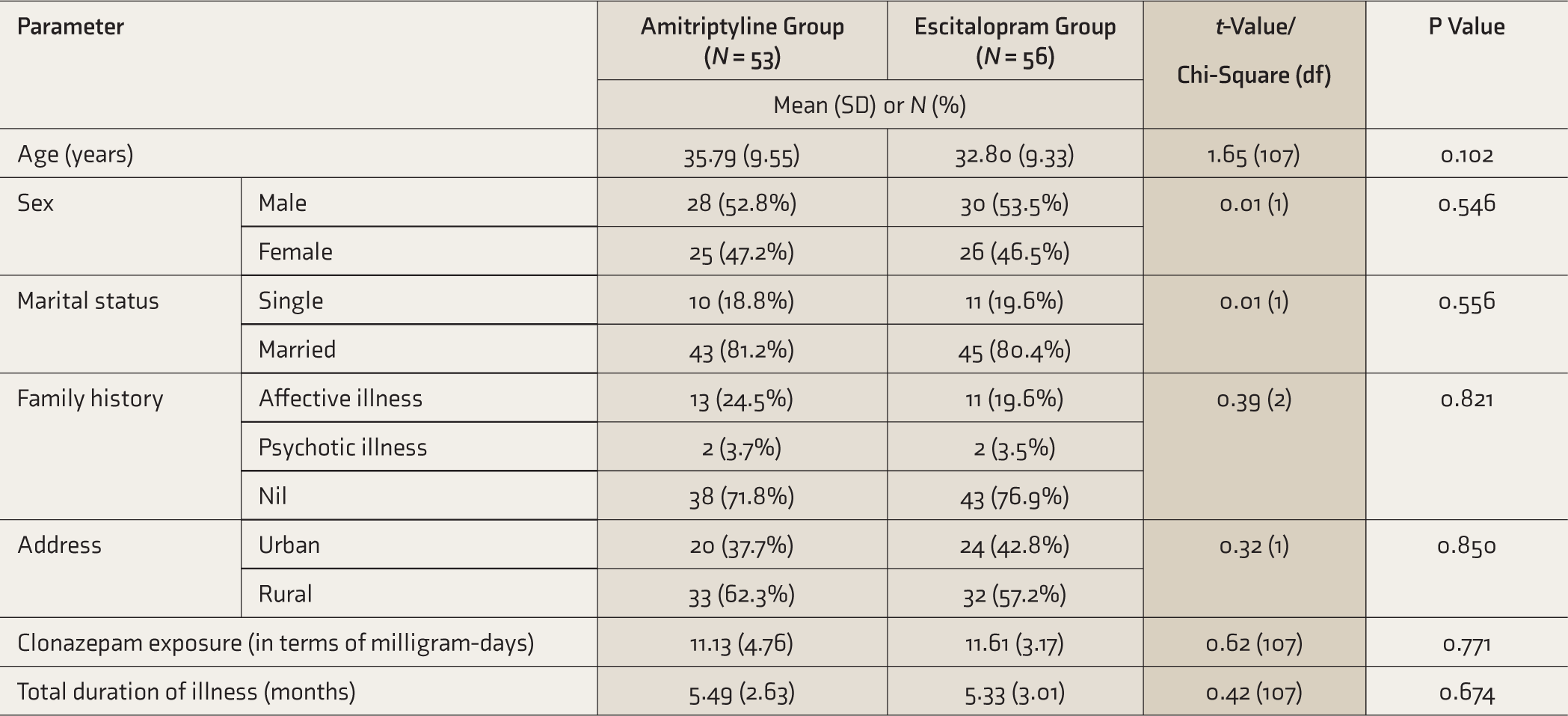
SD, standard deviation.
The measures of applanation tonometry were compared at baseline and then after four and eight weeks.
Comparison of Scores of Applanation Tonometry of Both Eyes in the Two Groups Across Weeks 0, 4, and 8
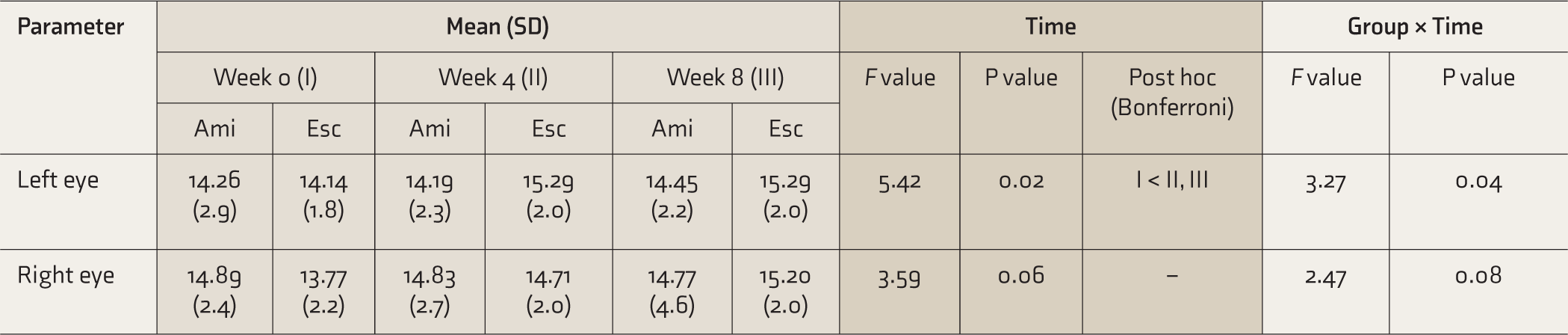
Ami, amitriptyline; Esc, escitalopram; SD, standard deviation.
Table 3 shows the results of the two-way RM ANOVA of the scores of gonioscopy of both eyes in the two groups across weeks 0, 4, and 8. The comparison was made across the four quadrants of both eyes. The measures did not vary significantly across any quadrants of either eye between the two groups.
Comparison of Scores of Gonioscopy of Both Eyes in the Two Groups Across Weeks 0, 4, and 8 (Graded According to the Shaffer’s System)
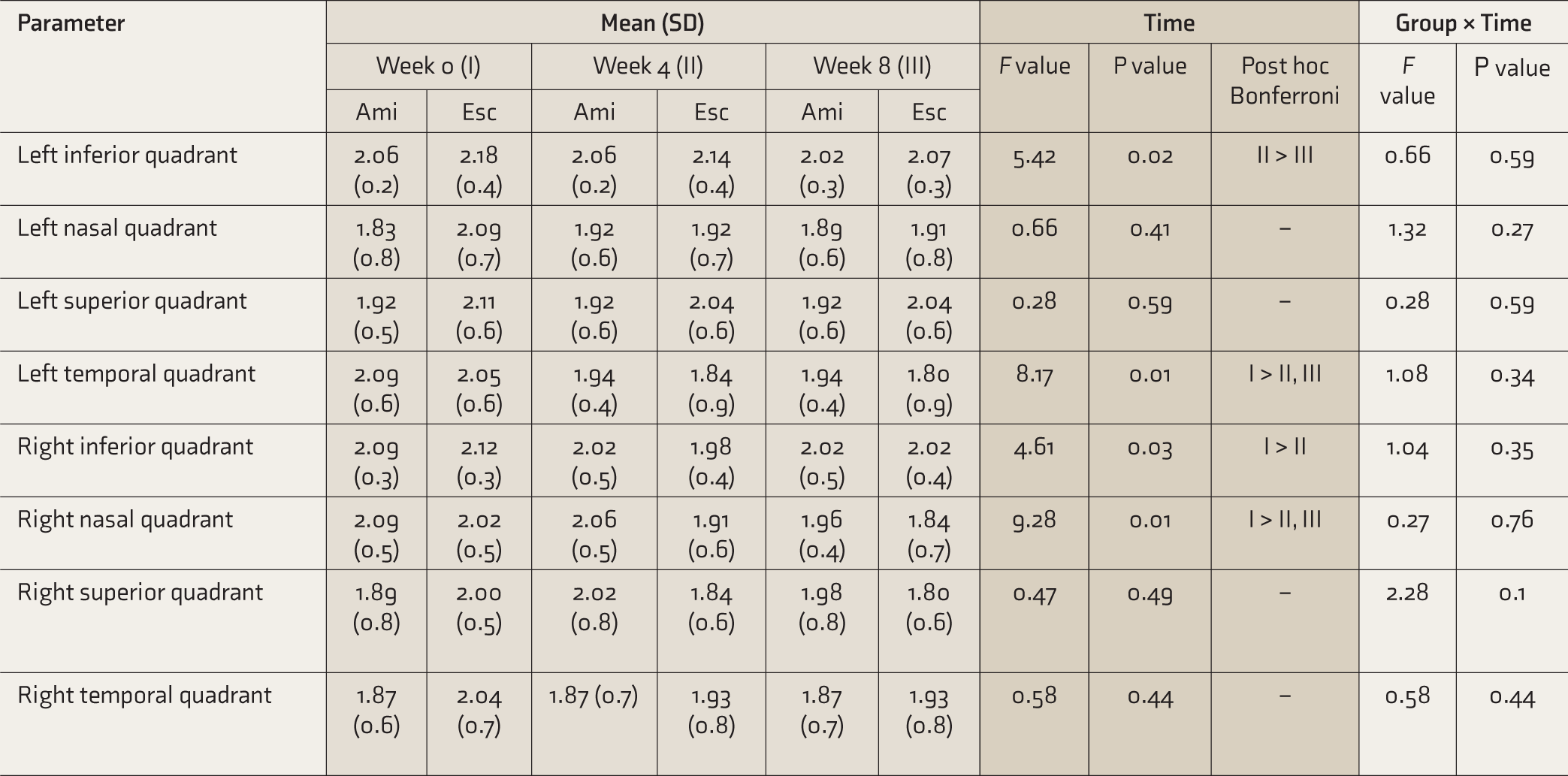
Ami, amitriptyline; Esc, escitalopram; SD, standard deviation.
Discussion
Our study found that drug-naïve patients of depression initiated on escitalopram tended to show a higher rise in the IOP than those initiated on amitriptyline. From a statistical point of view, this was significant in the results obtained from the left eye but not in the results obtained from the right eye. Nonetheless, a trend evolved from our study that escitalopram was associated with a higher rise in IOP. Our results are, to some extent, supported by the results obtained by Seitz et al. 13 that serotonergic antidepressants (like escitalopram) are likely to cause a higher rise in IOP as compared to antidepressants with anticholinergic properties (like amitriptyline). Our study also falls in line with the substantial volume of studies that concluded that serotonergic drugs (like SSRI) can lead to a rise in IOP.6,8
Our study also showed that the rise in IOP was more prominent for escitalopram in the first four weeks than in the period between four and eight weeks. This trend is also supported by various studies that found that the rise in IOP was higher in the immediate aftermath of the initiation of the drug. Chen et al. 6 found that the elevated risk of developing glaucoma was more prominent within seven days of initiation of the drugs. Similarly, Seitz et al. 13 also reported the risk to be higher immediately after initiation of the drugs.
Our study found no intergroup difference in the iridocorneal angles in any of the four quadrants across both eyes. This finding is a noticeable departure from most previous studies that cite changes in the iridocorneal angles after being initiated on either of the drugs. A substantial amount of evidence shows that various SSRIs are associated with the precipitation of acute angle-closure glaucoma. 18 – 20 Similar evidence also supports various TCAs causing acute angle-closure glaucoma. 10 – 12 A possible reason for this disparity could be that most of the mentioned research were case reports.
The IOP depends on the amount of aqueous humor in the anterior chamber. This is maintained by a fine balance between its formation and absorption (via the trabecular meshwork and uveoscleral outflow). No evidence suggests any action of escitalopram on the uveoscleral outflow. So, the results of our study do require an alternative explanation for this IOP raise. Aqueous humor formation occurs from the ciliary epithelium. This epithelium is a tissue that shares the same embryonic source as many other brain structures, like the retina and the pineal gland. A significant amount of serotonin metabolism occurs in the pineal gland and retinal epithelium. Moreover, it is noteworthy that this metabolism of serotonin has a cyclical pattern tuned to the circadian rhythm. 21 As SSRIs and TCAs cause an increase in the serotonin levels for the necessary actions on mood, a similar increase of serotonin in aqueous humor can be a reason behind this discordant finding. However, decisive results can only be inferred after meticulous aqueous humor studies.
The main strengths of our study were the use of a prospective design, inclusion of drug-naïve patients, and use of a head-to-head comparison approach with age and gender matching across the two groups. However, there were a few very important limitations to our study. We did our best to calculate the appropriate sample size using proxy markers. But, despite that, our sample size was small, and probably a few results did not achieve statistical significance because of this. Our follow-up duration was also relatively small. As a result, we could not observe the long-term effects of the prescribed drugs on IOP. Future studies should examine the reason behind the rise of IOP after being initiated in SSRIs. The effects of SSRIs on the serotonin levels in the aqueous humor could be one promising area to study.
To conclude, we found that escitalopram use was associated with an increase in IOP, which is partially in support of the existing literature. However, unlike most previous literature, our study found no change in the iridocorneal angle being precipitated with escitalopram and amitriptyline use. Clinicians should be aware of the possibility of a rise in IOP leading to ocular emergencies. We stress the practice of obtaining a proper history of ocular morbidities and remaining vigilant about raised IOP during follow-up of patients who are being prescribed escitalopram or amitriptyline.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
The authors received no financial support for the research, authorship, and publication of this article.