
Abstract
Bacground:
The aim of this study was to conduct a meta-analysis to compare the overall intraocular pressure (IOP)-lowering effect of iStent or CyPass as isolated procedures or in combination with cataract extraction.
Materials and methods:
Cochrane review manager 5.3 software (RevMan® 5.3) was used for a meta-analysis of IOPs and the number of antiglaucoma medications in six groups according to the type and number of stents and whether the procedure was isolated or in combination with cataract extraction.
Main results:
A total of 33 out of 446 publications retrieved have been enrolled. The mean changes in IOP in the groups with one iStent and more than two iStents with concurrent cataract extraction were −3.78 ± 0.53 mmHg and −3.89 ± 0.73 mmHg, respectively. The mean differences in IOP in the groups with one iStent and more than two iStents without concurrent cataract extraction were −3.96 ± 0.25 mmHg and −7.48 ± 0.55 mmHg, respectively. The mean changes in IOP in the groups with CyPass implantation with and without concurrent cataract extraction were −4.97 ± 1.38 mmHg and −8.96 ± 0.16 mmHg, respectively.
Conclusions:
Both iStent and CyPass either in combination with cataract extraction or as isolated procedures effectively decrease IOP. This effect is greatest with isolated implantation of CyPass followed by multiple iStents and then single iStent implantation and lasts up to 2 years.
Introduction
Glaucoma is a progressive neuropathy of the optic nerve affecting more than 60 million people in the world1,2 and is projected to affect 80 million by 2020. 3 Glaucoma constitutes a significant burden on public health and economy. The annual cost of glaucoma in the United States (US) is US$2.86 billion. 4 Moreover, glaucoma contributes to additional adverse health outcomes including increased risk of depression, 5 hip fracture, 6 and death. 7
Reducing intraocular pressure (IOP) is currently the primary means for halting the progression of glaucomatous damage. Initial therapy focuses on the use of topical medications. Unfortunately, up to 40% of patients with glaucoma in the US need more than one medication to control IOP. 8 As the number of medications necessary for controlling IOP increases, patient compliance decreases.8–10 Only 67% of patients with glaucoma fully execute their prescribed medication regimens. 11 The most common causes of poor compliance are the side effects including erythema, transient visual changes, pruritus, local irritation and ocular surface toxicity.12,13
Patients in whom glaucoma is not controlled with topical medications may undergo surgical instrumentation such as laser therapy, incisional surgery, or implantation of glaucoma drainage devices (GDDs). Although these procedures can effectively reduce IOP, they do carry a risk of potentially significant complications 14 that may lead to visual loss. Minimally invasive glaucoma surgeries (MIGSs) have been introduced to improve the safety profile. 1 iStent® (Glaukos, Laguna Hills, CA, USA) and CyPass® (Transcend Medical Inc., Menlo Park, CA, USA) are the main two devices currently used for MIGSs. Also known as a trabecular micro bypass stent, an iStent with dimensions of 1 mm length and 0.3 mm height is placed in the Schlem’s canal via an ab interno approach. 15 CyPass is also implanted by an ab interno approach into the supraciliary space. 16 These devices reduce IOP with a favorable safety profile in comparison with incisional and GDD implant surgery. 17 Either of these devices can be implanted as an isolated procedure or in combination with cataract extraction surgery.
Several studies have demonstrated the IOP-lowering effect of these devices but some of these studies were limited in the number of cases or lack of a control arm. In addition, there are only a few studies that have compared the outcomes of these MIGS devices with or without concurrent cataract extraction surgery. The purpose of this systematic review and meta-analysis was to compare the overall IOP-lowering effect of iStent or CyPass as isolated procedures or in combination with cataract extraction.
Methods
Literature retrieval
We adhered to the preferred item for systematic reviews and meta-analysis (PRISMA) guidelines. We searched PUBMED, Scopus and EMBASE for publications from January 2000 to July 2016 with the keywords ‘iStent’, ‘CyPass’ and ‘minimally invasive glaucoma surgery’. Furthermore, we hand-searched the references of the retrieved articles to find additional relevant papers. We also searched the grey literature and abstracts of ophthalmology congresses: the American Academy of Ophthalmology, European Society of Cataract and Refractive Surgeons, American Society of Cataract and Refractive Surgery (ASCRS), American Glaucoma Society, and the Association for Research in Vision and Ophthalmology.
Inclusion and exclusion criteria
Studies published as journal articles, systematic reviews, meta-analyses, cost-effective analyses, multicenter studies, randomized and nonrandomized clinical trials and case series were included in our analysis. The retrieved studies were manually screened. Duplicate studies and those without conclusive data were excluded from this study. Our analysis included studies with participants
Data extraction
We extracted the following data from eligible studies: demographic characteristics, number of participants, study design, duration of follow up, details of intervention (iStent versus CyPass, number of iStents, concurrent cataract extraction), mean preoperative and postoperative IOP, the numbers of preoperative and postoperative topical glaucoma medications, and surgical complications.
Statistical analysis
We used review manager 5.3 software (RevMan® 5.3, The Cochrane Collaboration; Copenhagen, Denmark) for analyzing the data. Risk of bias in each study was calculated using RevMan® software. Numerical data entered into the software included mean and standard deviation of preoperative and postoperative IOPs and number of medications. Available confidence interval values from the original data were used to calculate the respective values for standard deviation (SD). For studies lacking tabular data, they were derived from the manuscript graphs.
Heterogeneity of the groups was evaluated with the I2 value. In cases of high heterogeneity, we used a random effect mode, otherwise we used a fixed effect mode for each group. We subdivided the extracted data into six subgroups for comparison of changes in IOP and number of medications:
Group 1: One iStent implantation as an isolated procedure
Group 2: One iStent implantation with concomitant cataract extraction
Group 3: Two or more iStents implantation as an isolated procedure
Group 4: Two or more iStents implantation with concomitant cataract extraction
Group 5: CyPass implantation as an isolated procedure
Group 6: CyPass implantation with concomitant cataract extraction
After entering data in the relevant subgroups and analyzing them with the RevMan® software, we compared the output in three ways with Student’s t tests:
We compared the mean change of IOP to their respective preoperative values between all six subgroups to evaluate the overall effect on IOP from 6 to 60 months of follow up.
To determine the effect of cataract surgery on MIGS device function, we compared the mean IOP change at 12 months and 24 months follow up between group 1 and 3, group 2 and 4, group 5 and 6.
Finally, we compared the effect of MIGS devices on mean number of topical medications within all subgroups during 6 to 60 months of follow up.
A p value ⩽0.05 was considered as statistically significant.
Results
Publications retrieved
We retrieved 446 papers from the database and grey literature search. Duplicate publications, studies without conclusive data, review articles, and case reports were excluded. After screening and full article review, a total of 33 studies including 26 full-text publications18–43 and 7 abstracts44–50 which enrolled 1745 patients altogether were examined in this meta-analysis (Figure 1). From the identified literature, we extracted data including study design, initial and final number of patients, type of surgical intervention, mean age of study patients, type of glaucoma, mean preoperative and postoperative IOP values and number of medications, as well as the duration of follow up (Table 1). No study reported any device or procedure related major complication. To evaluate for publication bias, we examined the symmetry of the funnel plot depicting mean changes in IOP against the standard errors of mean that revealed no apparent asymmetry (Figure 2).
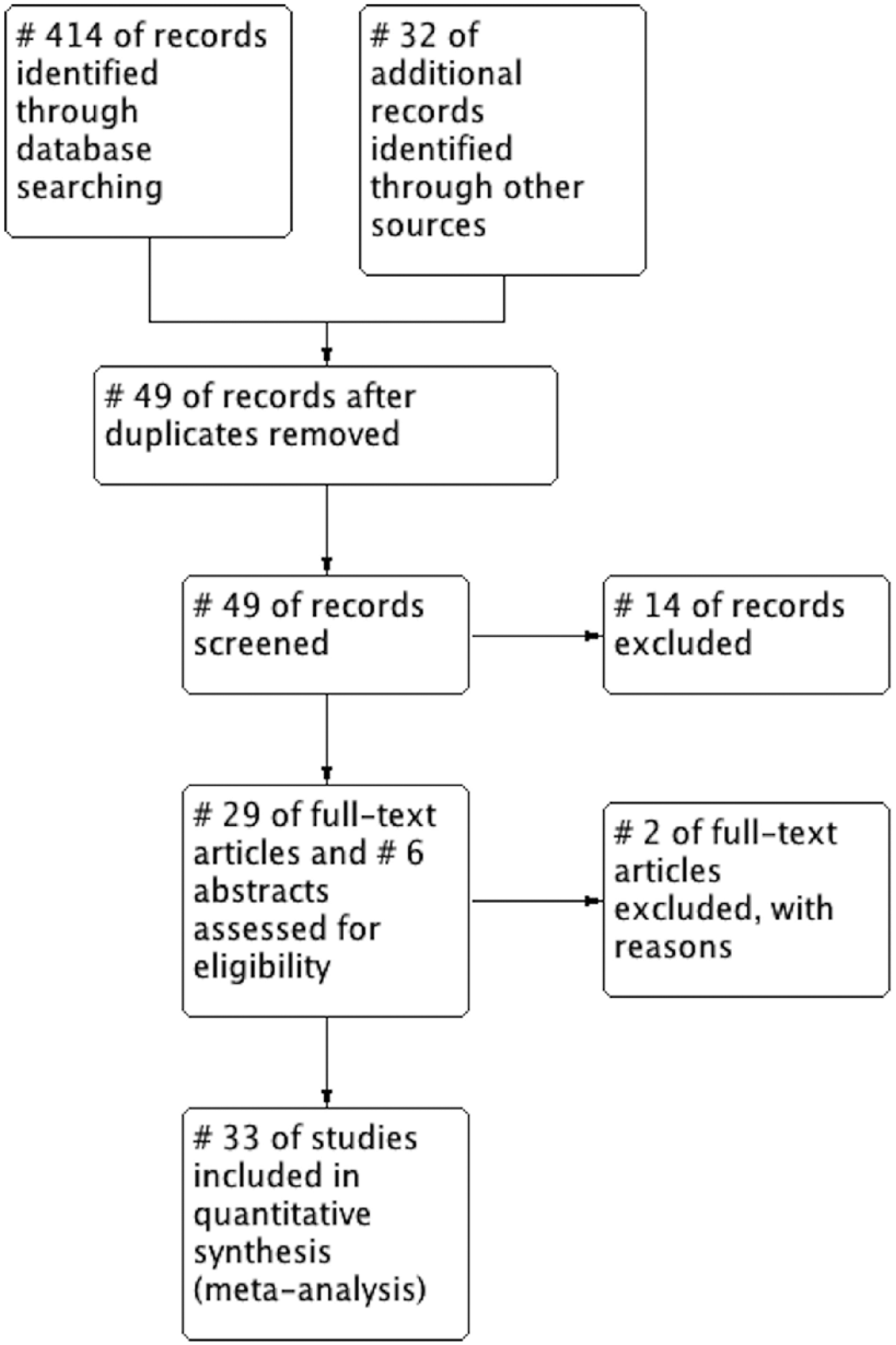
PRISMA flow diagram demonstrating literature search and data extraction.
Characteristics of the studies included in the analysis.
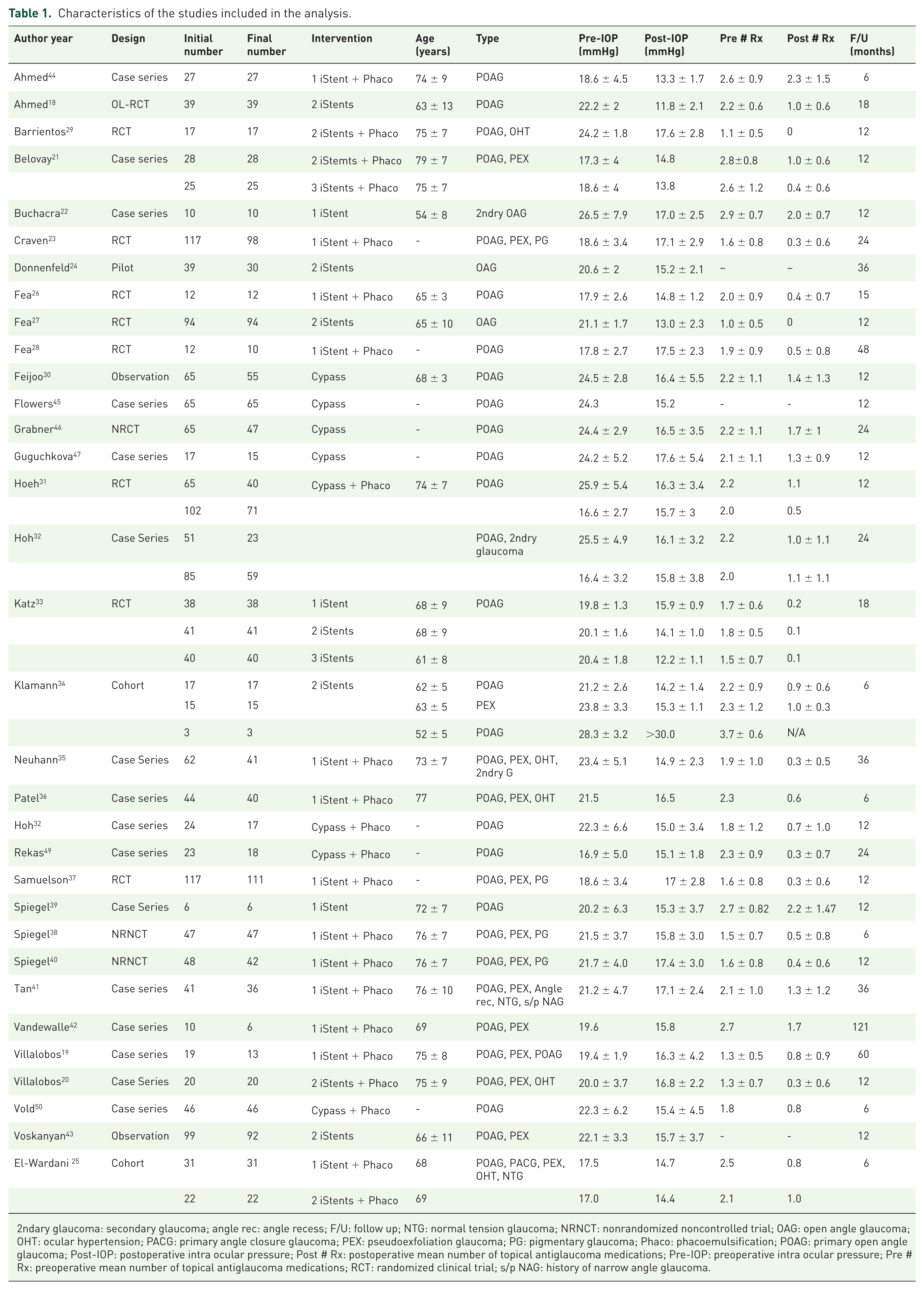
2ndary glaucoma: secondary glaucoma; angle rec: angle recess; F/U: follow up; NTG: normal tension glaucoma; NRNCT: nonrandomized noncontrolled trial; OAG: open angle glaucoma; OHT: ocular hypertension; PACG: primary angle closure glaucoma; PEX: pseudoexfoliation glaucoma; PG: pigmentary glaucoma; Phaco: phacoemulsification; POAG: primary open angle glaucoma; Post-IOP: postoperative intra ocular pressure; Post # Rx: postoperative mean number of topical antiglaucoma medications; Pre-IOP: preoperative intra ocular pressure; Pre # Rx: preoperative mean number of topical antiglaucoma medications; RCT: randomized clinical trial; s/p NAG: history of narrow angle glaucoma.
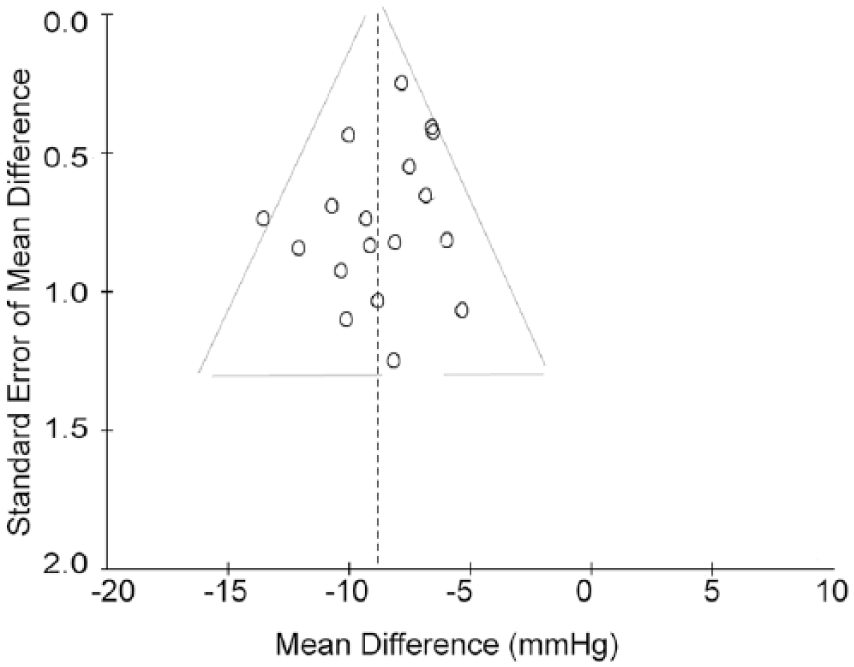
Funnel plot presenting studies on the changes in intraocular pressure before and after stent implantation.
Implantation of iStent without cataract extraction
We analyzed the effect of implanting 1 or ⩾2 iStents (group #1 and #3 respectively) without concurrent cataract extraction on changes in IOP. Group #1 included 54 patients with a mean change in IOP of −3.96 ± 0.25 mmHg during a follow-up period of 12 to 18 months [Figure 3(a)]. Group #3 included 368 patients (who completed follow-up assessment from the initial 384 patients) with a mean change in IOP of −7.48 ± 0.55 mmHg during a follow-up period of 6-24 months [Figure 3(b)]. We further analyzed the data for groups #1 and #3 based on the length of follow-up period. The mean change in IOP for group #1 was −7.50 ± 1.93 mmHg in 16 patients after 12 months and −3.90 ± 0.25 mmHg among 38 patients after 24 months (p
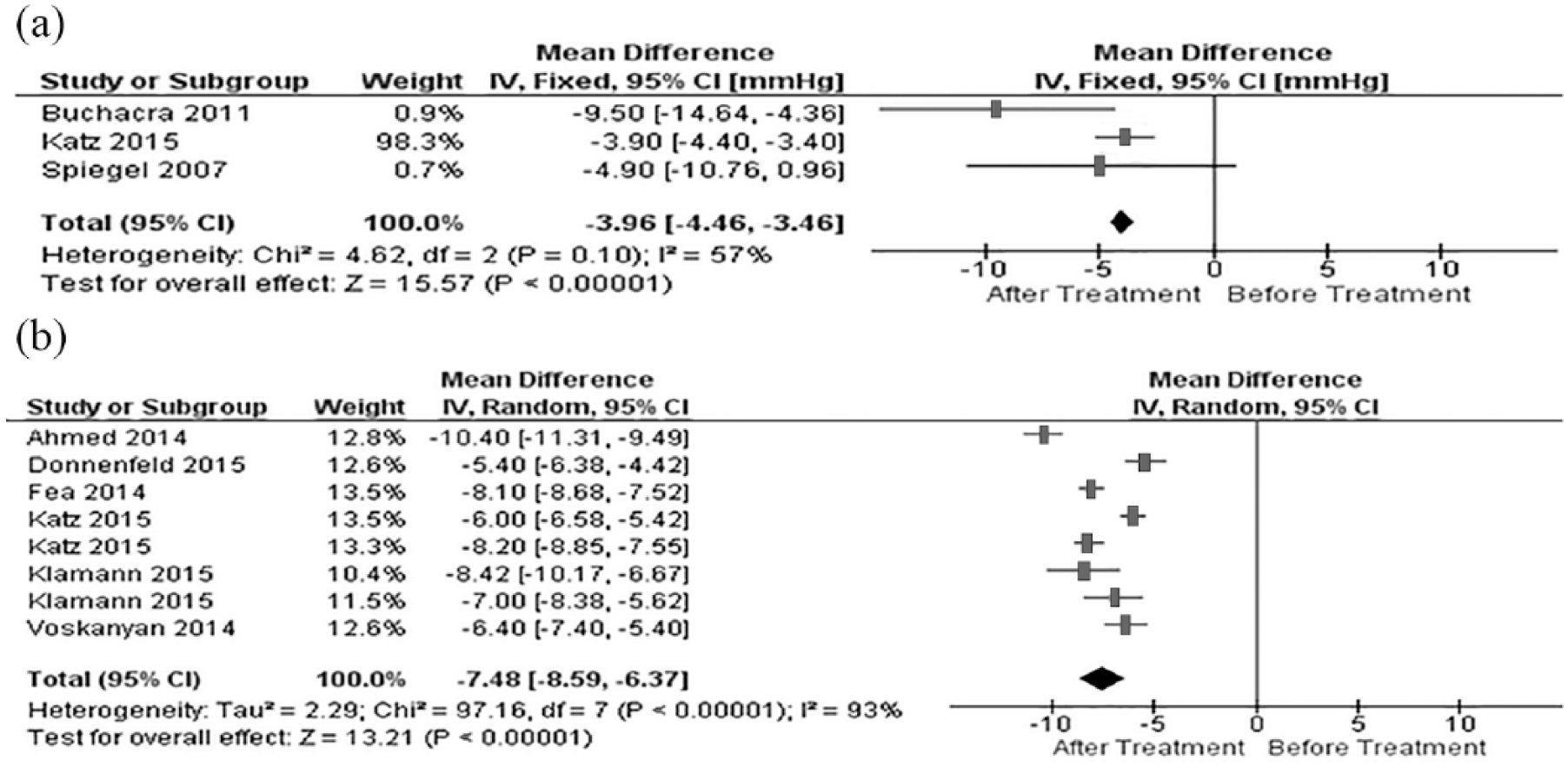
Forest plots depicting the changes in intraocular pressure following isolated implantation a single iStent (group #1) or implanting ⩾2 iStents (group #3) without concomitant cataract extraction. (a) The IOP-lowering effect in group #1. (b). The IOP changes in group #3.
Mean changes in intraocular pressure in various time points in each study group.

IOP, intraocular pressure; N/A, not available.
Effects of iStent implantation on IOP with cataract extraction
We analyzed the IOP-lowering effect of implanting 1 and ⩾2 iStents (group #2 and #4, respectively) with concurrent cataract extraction. In group #2514 out of 587 patients completed the follow-up IOP measurements. The mean change in IOP of −3.78 ± 0.53 mmHg in group #2 during a follow-up period of 6 to 60 months [Figure 4(a)]. Group #4 included 112 patients with a mean change in IOP of −3.89 ± 0.73 mmHg during a follow-up period of 6−12 months [Figure 4(b)]. We further analyzed the data for groups #2 and #4 based on the length of follow up. For group #2, 12 months and 24 months after the time of the surgery, the mean change in IOP was −3.99 ± 0.59 mmHg (304 patients) and −2.14 ± 0.76 mmHg (110 patients), respectively (p

Forest plots depicting the changes in intraocular pressure following implanting 1 iStent (group #2) and ⩾2 iStents (group #4) with concomitant cataract extraction. (a). The IOP-lowering effect in group #2. (b) The IOP changes in group #4.
Comparison of all iStent groups
In overall comparison of all iStent groups, the differences among the groups were statistically significant (p
CyPass implantation
We analyzed the effect of CyPass implantation without (group #5) and with (group #6) concomitant cataract extraction. In group #5, the mean change was −8.96 ± 0.16 mmHg for 212 patients after 12 to 24 months of follow up [Figure 5(a)]. However, in group #6 the mean change in IOP was −4.97 ± 1.38 mmHg for 396 patients after 6 to 24 months follow up [Figure 5(b)]. We further analyzed the data for both groups based on the length of follow-up period. For group #5 at 12 and 24 months of follow up, the mean change in IOP was −9.04 ± 0.16 mmHg (135 patients) and −7.90 ± 0.61 mmHg (47 patients), respectively (p

Forest plots depicting changes in intraocular pressure before and after single CyPass implantation in isolated form (a) or with concomitant cataract extraction (b).
iStent versus CyPass
CyPass had a greater effect on decreasing IOP at all time points compared with iStent implantation except at 24 months for those implanted with multiple iStents without cataract extraction (group #4). In all remaining comparisons, the observed differences between the iStent and CyPass groups were statistically significant. Figure 6 demonstrates and compares the IOP-lowering effects of all iStent groups and CyPass groups at various time points after surgery.
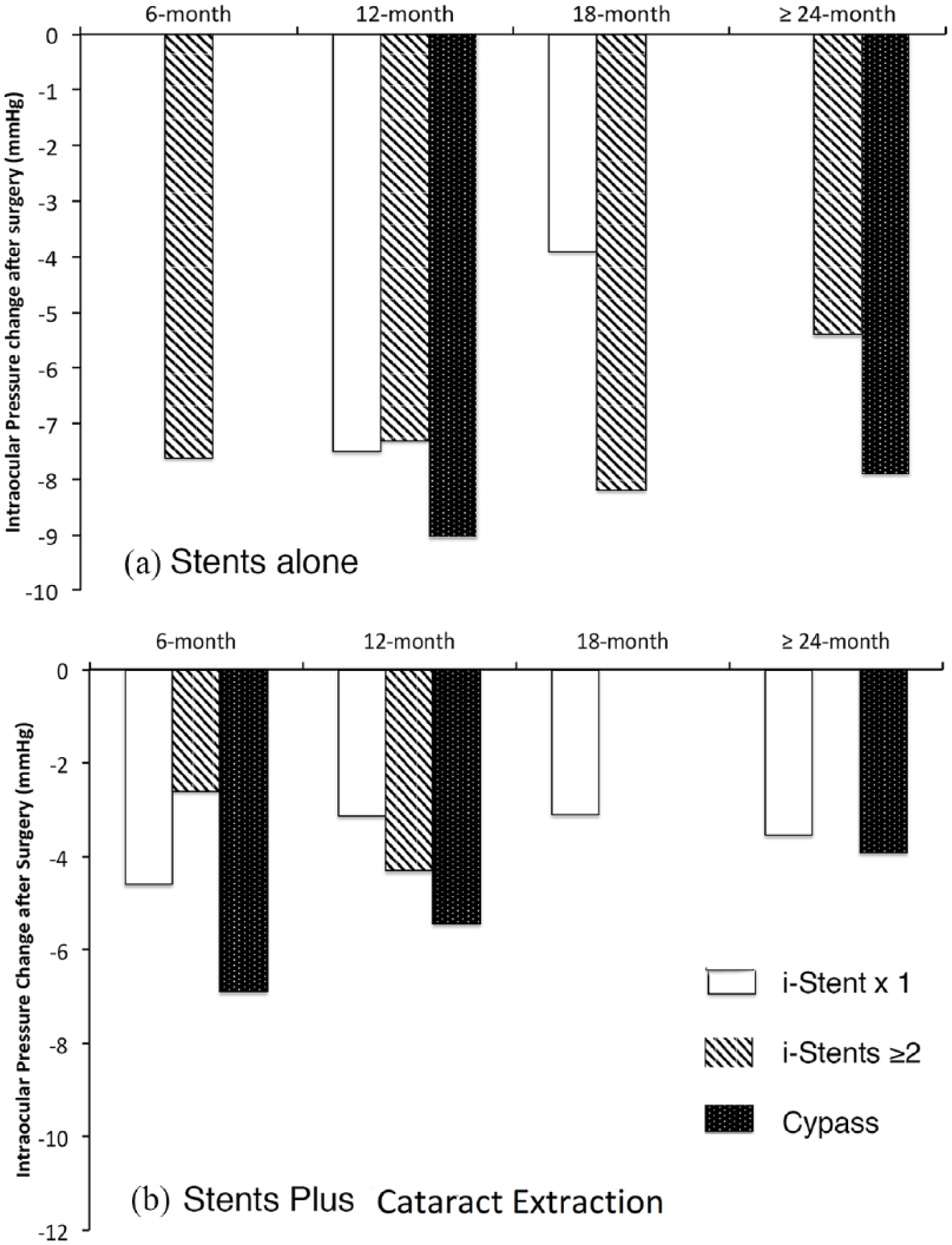
Bar graphs demonstrating the changes in intraocular pressure before and after isolated stent implantation (a) and with concomitant cataract extraction (b) through a 6 to 24 month follow-up period.
Effect on number of antiglaucoma medications
The number of medications decreased significantly following implantation of either type of stent (Table 3). The mean reduction in the number of topical antiglaucoma medications was similar among groups of the patients who were treated with implantation iStents/CyPass; −1.23 ± 0.10 in groups #2; −1.43 ± 0.22 in group #4 and −1.24 ± 0.14 group #6, where concomitant extraction of the cataract was performed (Figure 7). The net effect on changes in the number of antiglaucoma medications was similar between CyPass and iStent implantation combined with cataract extraction (p = 0.22). Similarly, the difference in the number of medications was not significant between the patients who received an isolated implantation of a single iStent (group #1); patients in group #3 who were implanted with multiple iStents and group #5 who were implanted with CyPass without concomitant extraction of cataract (Figure 8).
Mean changes in the number of antiglaucoma medications in each study group.
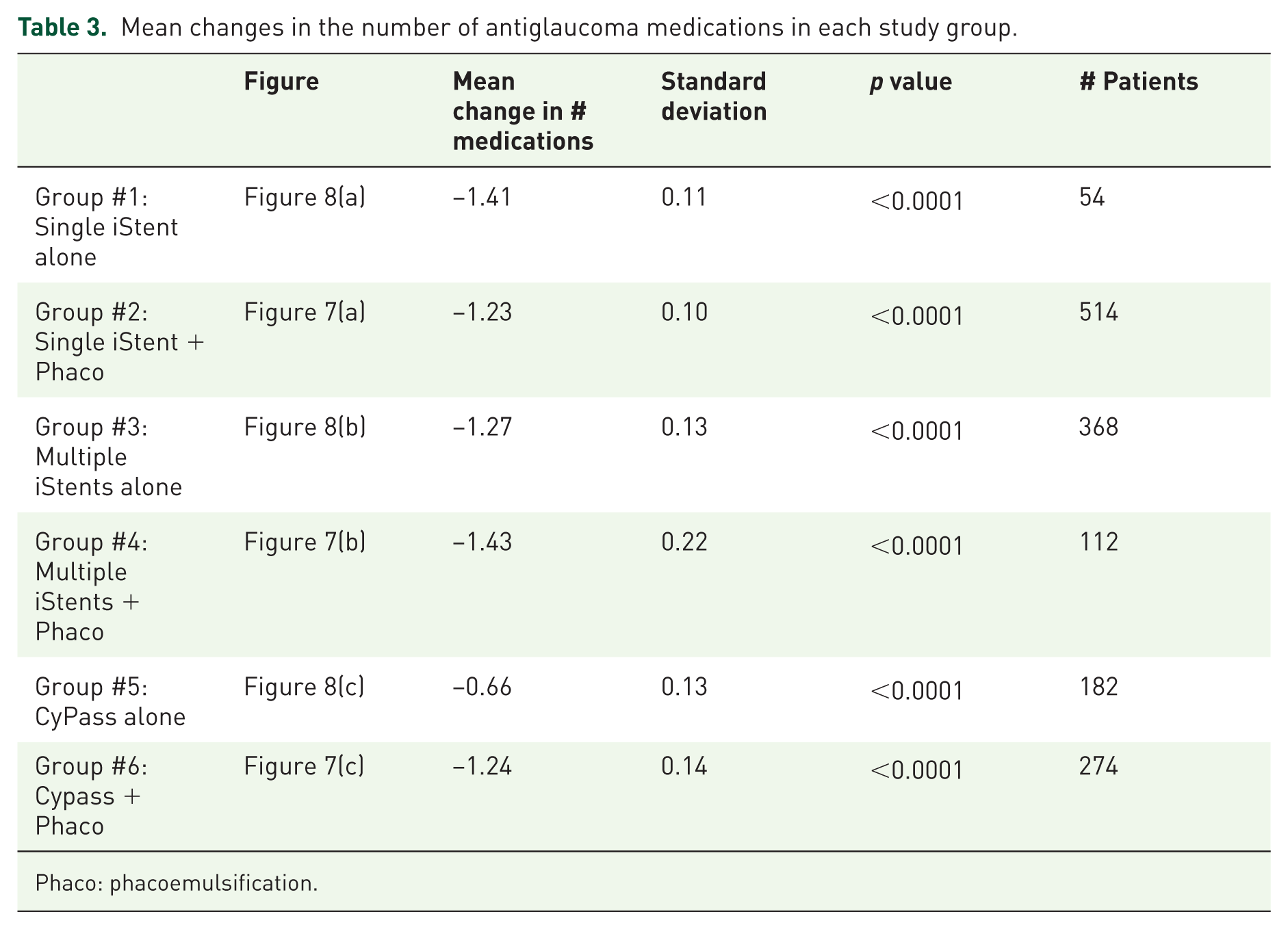
Phaco: phacoemulsification.

Forest plots depicting changes in the number of the medication before and after isolated implantation of a single iStent (a); multiple iStents (b) and or CyPass (c) along with cataract extraction.

Forest plots depicting changes in the number of the medication before and after implantation of a single iStent (a); multiple iStents (b) and or CyPass (c) without concomitant cataract extraction.
Discussion
Our meta-analysis is the first to compare the IOP-lowering effect of iStent versus CyPass with or without concurrent cataract extraction surgery. We find that for both devices, a greater IOP-lowering effect is noted when the implant is performed as an isolated procedure. When comparing devices, the CyPass has a greater IOP-lowering effect than the iStent, especially when only one iStent is implanted. All studies uniformly report a greater effect on IOP reduction with increasing number of iStents implanted. 7 While CyPass decreases IOP to a greater extent, the reduction in number of glaucoma medications is modest compared with iStent.
We speculate that the differences in IOP outcome with MIGS device implantation with or without cataract surgery may be secondary to changes in anterior segment anatomy. It is well documented that cataract surgery alone may have an IOP-lowering effect. Structural alteration of the anterior segment angle may in part contribute to this observation.51–54 However, implantation of MIGS devices does not alter angle anatomy.22,55 Additionally, the outcomes of conventional trabeculectomy in aphakic and psuedophakic eyes are not as favorable as phakic eyes, which indicates the importance of the anterior chamber manipulation on the outcomes of aqueous drainages surgeries. We speculate that the angle configuration contributed by the phakic lens provides an optimal environment for function of MIGS devices. This hypothesis is supported by our finding that IOP changes are more prominent in patients after isolated implantation of both types of MIGS devices. More specifically, concurrent cataract extraction reduces the IOP-lowering effects of MIGS devices; we found no difference with the changes in IOP between patients implanted with multiple iStents with cataract extraction and those who received isolated implantation of a single iStent. However, further studies are necessary to shed light on the mechanisms underlying this observation.
Preoperative state of IOP is a significant confounding variable for these findings. In further details and analysis of the aforementioned studies, both Hoeh and colleagues and Hoh and colleagues, who examined the IOP-lowering effects of CyPass insertion plus concurrent cataract extraction, the patients were stratified by baseline IOP ⩾ 21 mmHg and <21 mmHg.31,32 The ‘controlled’ group of eyes with a lower baseline IOP had a lower magnitude of IOP reduction but had less medication dependence, postoperatively. In ‘uncontrolled’ eyes (IOP ⩾ 21 mmHg) with a higher baseline IOP, there was a larger magnitude of IOP reduction, as well as medication reduction. As shown in Table 1, the CyPass-alone subgroup had a mean preoperative IOP of 24.3 mmHg that decreased to 17.0 mmHg, postoperatively. Likewise, in the CyPass + phacoemulsification group, the IOP postoperatively decreased to 16.2 mmHg from their preoperative IOP of 25.7 mmHg. Whereas, in a group of patients with ‘controlled’ glaucoma with IOP < 21 mmHg, after implanting CyPass alone, the IOP decreased from 16.4 mmHg to 15.7 mmHg and it reduced from its preoperative value of 16.6 mmHg to 15.8 mmHg after implanting the CyPass with concurrent extraction of cataract.
The IOP-lowering effect of both MIGS devices decreases from 12 to 24 months (except with isolated implantation of ⩾2 iStents). This is a familiar trend noted in other surgeries that lower IOP. For example, cataract surgery is known to decrease IOP; however, that decrease is transient.56–58 Similarly, argon laser trabeculoplasty lowers IOP, but the effect diminishes over time.59,60
This review suggests that implantation of either the iStent or CyPass devices leads to a reduction in the number of necessary glaucoma medications, however it is more prominent with iStent than CyPass. Additionally, there may be a potential for cost savings as the concurrent lens extraction can be avoided in glaucoma patients who do not present with symptoms and signs of cataracts. Although the decrease in the number of necessary medications may contribute to cost savings, 61 further cost savings may be derived from the increased patient compliance from reduced medication requirements. Better patient compliance may result in improved glaucoma outcomes with a decreased number of clinic visits.
This study further showed that the use of multiple iStents is more effective than implanting a single iStent in reducing IOP. However, in the studies that looked at multiple iStents, some used two or three standard iStents while others used the iStent inject (which comes packaged with two stents). The different versions of stent used, as well as whether single/two standard iStents were comparable to single/two iStent injects might have contributed to a lower homogeneity in our comparison. Both MIGS devices have favorable safety profiles. Complications were noted such as microscopic hyphema, and device malpositioning and occlusion. However, there were no reports of serious complications, such as choroidal effusions, hypotony and bleb-related complications as for conventional trabeculectomy and other ab externo procedures.62–65
Although our meta-analysis was limited by the reliability of data from published studies, in aggregate, our data support the IOP-lowering effect of iStent and CyPass devices. The magnitude of effect is dependent upon concurrent cataract surgery and outcomes vary in their long-term efficacy. Our meta-analysis without separating those with normal and elevated preoperative IOPs might have led to inaccurate conclusion of CyPass alone being more effective than CyPass and cataract extraction. However, the structural and biological changes in the anterior chamber need to be elucidated by more extensive studies on the microarchitecture and cellular and subcellular structures of the anterior chamber following procedures such as cataract extraction surgery. These factors should be taken into consideration when planning MIGS device implantation.
Post-acceptance addendum
For the time period of the studies reviewed for this meta-analysis, both devices had comparable safety profiles. However, the CyPass was recently removed from the market voluntarily by the manufacturer upon noting increased endothelial cell loss with CyPass implantation. 66 In the interests of transparency, the meta-analysis should be interpreted in the context of this market withdrawal. Nevertheless, as multiple MIGS devices are now coming to market, our study highlights the necessity of considering multiple variables such as lens status and number of devices implanted when considering clinical study design and data interpretation with these devices.
Footnotes
Acknowledgements
The opinions expressed herein do not necessarily represent those of the Veterans Administration or the US Government.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SPP is a consultant to Novartis for expertise unrelated to the topic of this manuscript. None of the other authors report a conflict of interest.