
Abstract

The Context: NITI Aayog
Since independence, the Planning Commission of India had been estimating the country’s physical, capital, and human resources, making a staged plan, and allocating these resources. With the shift in political power in 2014, in 2015 it was replaced by the National Institution for Transforming India (NITI) Aayog. NITI Aayog acts only as a “think tank” to the central and state governments on policy matters, presumably to overcome slow policy implementation by encouraging improved interministry and center–state coordination. The overall purpose is strategic input for the development process of India, while the powers of allocation of funds (especially to the annual plans of the states), unlike the Planning Commission, are next to none.
As a part of this mandate, health and family welfare is one of the many verticles. Each vehicle is responsible for sector-specific issues for development and growth. One of the approaches of the NITI Aayog is its mix of cooperative and competitive federalism. The former implying “a joint focus on the National Development Agenda by the Centre and States, and advocacy of concerns and issues of States and Union Territories with Central Ministries.” 1 On the other hand, competitive federalism fosters a spirit of competition among the states for scarce resources that the center allocates as per performance. And for the latter purpose, various indices have been/are being developed for the states for a dynamic annual ranking. Of the 11 indices, two concern with health: the state health index and the district hospital index (presently in preparation).
The NITI Aayog’s Health Index: A Critique
The said index, developed with inputs from the ministry of health and family welfare (MoHFW) and world bank, is a composite of health outcomes, governance and information, and key inputs and processes (weightage of 70:12:18, respectively). 2 A performance measurement instrument for health systems has two primary purposes: improve performance and encourage accountability, besides allowing judicious health system decision making. 3 While choosing a measure that eventually contributes to a composite index, a few crucial elements that need consideration are defining priority areas, avoiding positively correlated measures (as it may lead to “double counting),” 3 and data that are robust and part of a routine process. Health outcome measures such as under-five mortality rate or suicide rate are dependent not only on the health service system but also on an extraneous complex of social, cultural, environmental, and political factors. For example, the suicide rate is also determined by employment and livelihood issues, religious beliefs, gender, socioeconomic status, rural–urban differences, etc. 4 However, health systems, too, are part of the latter complex. In contrast, inputs and process indicators are contingent on the functioning of the health service system a and are sensitive to change.
Thus, for NITI Aayog’s composite index, the excessive weightage on outcome measures for annual comparison seems arbitrary, although acknowledged as the primary focus of performance, and rightly so as long-term targets. Moreover, among the outcome indicators, infant mortality rate, anemia among women (15–49 years), children (under six months of age) exclusively breastfed, 5 or the maternal mortality ratio are conspicuously absent. At the same time, they are considered global reference indicators by the World Health Organization. 6 It has been suggested that choosing individual indicators for a composite index is as much technical as it is political (depending on the interest groups involved) that can bring down the latter’s credibility. 3 Take the example of the index “Proportion of districts with functional Cardiac Care Units” (in district hospitals). Remarkably, on this indicator, Rajasthan jumps from 2.9 in the base year (2014–2015) to 70.6 in 2015–2016, and is then down to 24.2 in 2017–2018, which sets the alarm bells ringing.
On the other hand, inputs and process indicators include domains such as vacancies at various health provider positions, the proportion of 24×7 functioning primary health centers and quality-assured public health centers, registration of births and pregnant mothers, aspects of the functioning of a health information system and ease of finance flow from center to the periphery.
Mental Health Indicators
NITI Aayog accepts the absence of mental health (MH) indicators besides critical areas of noncommunicable diseases (NCDs), infectious diseases, and financial risk protection in the composite state health index because of the nonavailability of quality data annually.
On the other hand, reported under sustainable development goals and available with National Crime Records Bureau, suicide data are not included in the state health index. Thus, NITI Aayog’s rationale for the unavailability of reliable MH data stands invalid.
It is also acknowledged that data on the availability of specialists, including psychiatrists in district hospitals, is also part of the process indicator.
The absence of an MH information system is one of the significant drawbacks of our MH system. Thus, data on such is essential, and a robust health information system is necessary. While it may seem to some that with the already available data on MH services, NITI Aayog should include specific MH indicators immediately. We, on the other hand, argue otherwise in the following sections.
Mental Health System of India: The National Mental Health Survey
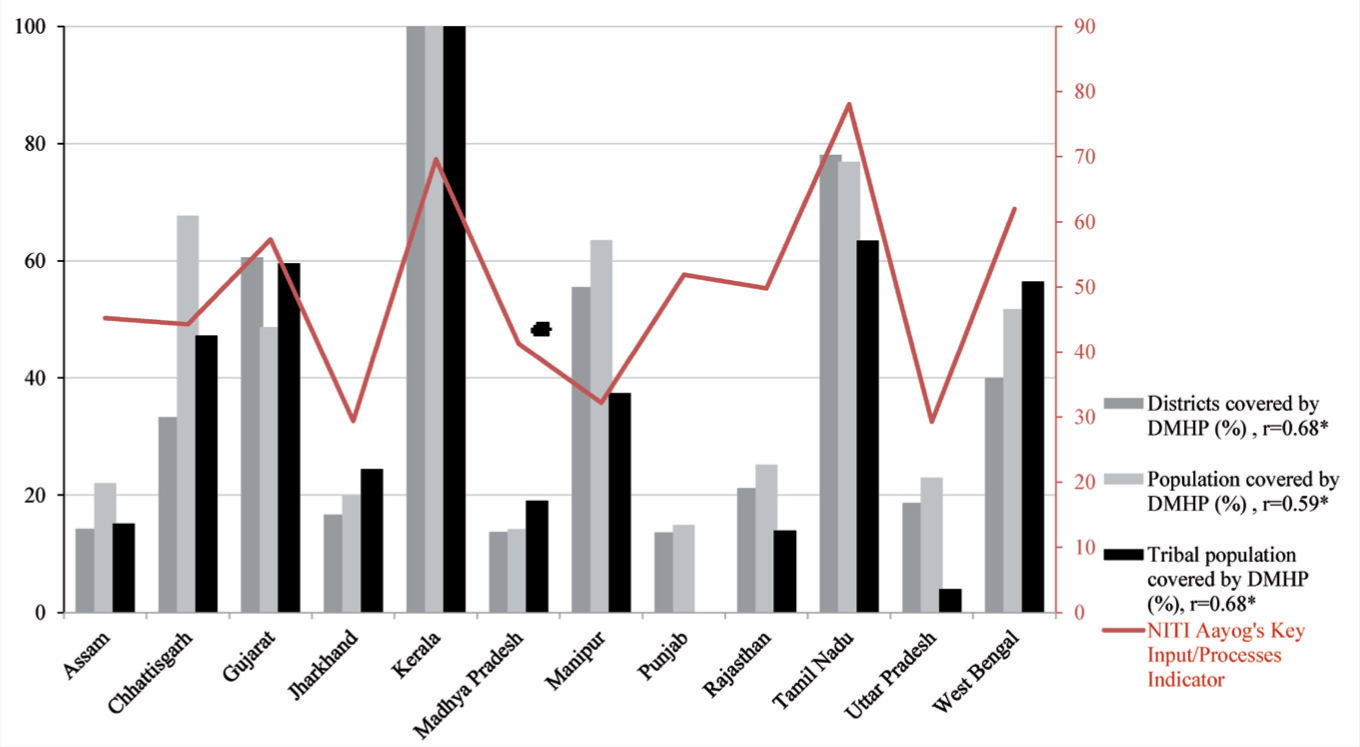
In 2015–2016, massive data collection by the National MH Survey (NMHS) 7 included not only the prevalence and burden of mental disorders but also the treatment gap, patterns of health care-seeking, service utilization, impact, and disability of mental disorders. 8 However, it included only 12 states, representing each region of India. The NMHS developed a composite score for the MH system coverage in each state based on the availability of MH care facilities, human resources (and their training in MH), drugs, action plan for the implementation of MH policy and legislation, funding, engagement with other service sectors (e.g., welfare programs) and civil society, and monitoring and evaluation activities. Among other parameters, the NMHS also reported the district MH program (DMHP) coverage by districts, population, and tribal population of each of the 12 states. We premise that an essential part of the future public MH service system is the MH program (or the community-oriented services) that has a wider reach for a vast country like India. My argument becomes even more critical, particularly in the context of the 12th five-year plan of the Government of India, whereby the DMHP is mandated to run a 10-bedded inpatient facility at the district hospital, a daycare psychiatric rehabilitation facility, and a residential/long-term continuing care center 9 . Therefore, the program is also a vital conduit for realizing the MH Policy of India and the MH Care Act, 2017.
Regarding the MH service systems of India, it can be counterargued that the larger share is of the General Hospital Psychiatry Units and mental hospitals, and not DMHP. We argue that the ideal MH service system is likely a community-oriented MH system as seen in certain world regions such as Australia, Canada, or Nordic countries. Thus, places with successful DMHPs/community-oriented MH services indicate progressing toward an ideal MH service system in India.
In the absence of robust data on MH across the country, using MH data from the 12 districts surveyed under NMHS, we could evaluate if the general health system processes measure correlate with the coverage of DMHP. The choice to retain only the process indicator, as elaborated earlier, is because of its sensitivity to changes in the organization of health services. The theoretical background to this premise lies in the general conceptualization of how the National MH Program (NMHP) was conceived in the first place. We presume that the success of NMHP is contingent on the successful organization of the general health care services. Moreover, if health service process indicators are correlated, it may also be partly redundant to include the currently available MH data into the State Health Index (to avoid double-counting).
Figure 1 shows the correlation between the coverage of DMHP (in 2015–2016) with NITI Aayog’s inputs and process indicators (for the year 2015–2016), and we find a significant (P = 0.014) correlation coefficient of 0.68. This more than modest correlation thus suggests that partly the DMHP’s success rests much on the available health services system, a logical strategy for MH services. The logic is that NMHP is a horizontal program. There is widespread comorbidity of mental illness with NCDs and infectious diseases (e.g., HIV, TB). Moreover, the skill sets of primary health care workers required to manage MH conditions and NCDs or chronic infectious diseases are similar. 9
Mental Health Performance Indicators and NITI Aayog’s Health Index
The need for MH performance indicators in the Health Index on its face is appealing; on the other hand, it requires a more nuanced understanding. To suggest indicators, one needs to consider the proposed measures’ rationale, validity, sensitivity, predictive validity, and feasibility, besides the political and organizational context within which the data are collected and disseminated. 3 Although a composite index is convenient because of its simplicity, it should be inferred with caution. Instead, a robust health information system that routinely collects MH data is a more critical agenda for MH advocacy.
Future Direction
The health management information system (HMIS) (
Proposed Mental Health Indicators to Support Mental Health Information System
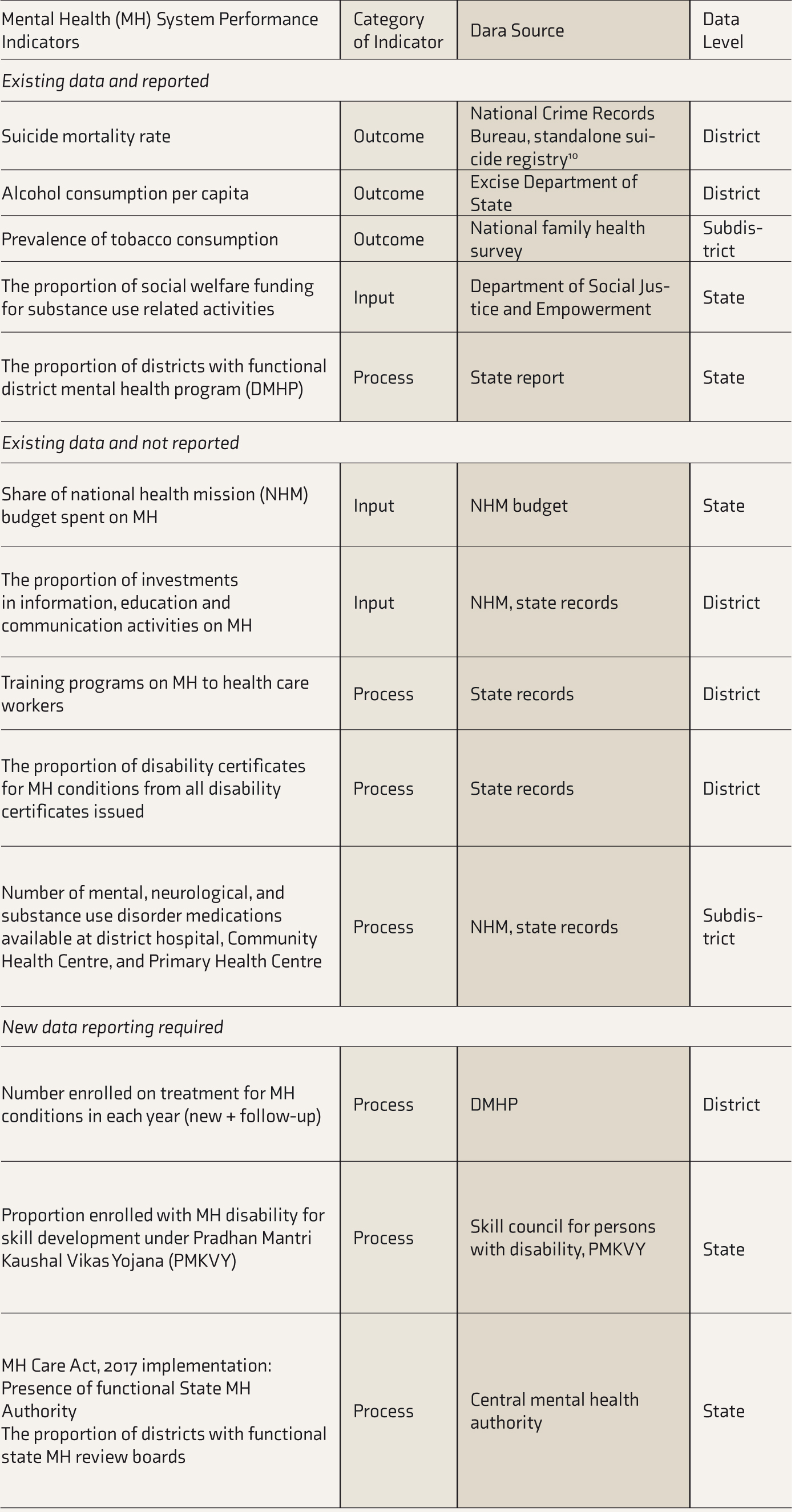
NHM, national health mission; DMHP, district mental health program.
While choosing performance measures for health systems, the right balance of promotive, preventive, and curative dimensions must be considered. Data for a few indicators are already present—some reported and others collected but not reported (are indicated in Table 1)—while a few need new efforts for data collection. Without any routine reporting of NCDs, DMHP will be the only data source on the number enrolled on treatment for MH conditions each year. Some indicators such as the proportion of districts with MH Review Boards (MHRBs) in the present stage may give way to the average number of grievances processed by MHRBs in each state later.
Conclusion
My proposal for HIMS that includes MH looks forward to an agenda of MH monitoring and evaluation, given the current trends in performance evaluation. However, we propose MH not to be part of the NITI Aayog’s Health Index without a robust data collection system in place. With the expectation of more investments in health in the future, and various developments around MH in the past decade, an MH information system will be crucial for MH system development, feedback, and decision making. A list of MH information feeding the HIMS, grounded on data availability and a comprehensive understanding of the public MH system, is needed.
The suggested list of MH indicators is tentative and a teaser to engage the community of public (mental) health specialists. It is acknowledged that building health indicators is a complex task and brings up much debate. Because of the uniqueness of each country’s health system, concerted effort from multiple experts is necessary to develop a sound health information system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.