
Abstract

The origin of concepts of yoga-based philosophical counselling can be derived from the traditional Vedic and Upanishadic literature from 2700
The word “yoga,” meaning “to yoke,” was first mentioned in the Rig Veda (1500–1200
Various Upanishads (subsections of the Vedas) have descriptions of yogic practices as a means of mastering the mind: Brihadaranyaka Upanishad (c. 900
The classical era saw the emergence of “Sutras” and “Puranas” as a means of documentation of yogic philosophy. Yoga Vasishta, Bhagavad Gita (BG, 500
With the introduction to Hatha Yoga, the post-classical period saw a shift from the philosophical teachings of yoga to the “physical culture” of yoga. 6 Teachings of Sri Krishnamacharya Yoga, regarded as the father of modern yoga, became popular in his school of Vinyasa Krama Yoga. Students of Krishnamacharya played an integral role in popularizing Hatha Yoga in the West. Among his students were BKS Iyengar (Iyengar Yoga), Pattabhi Jois (Ashtanga Vinyasa Yoga), and T Desikachar (Vini Yoga). In an effort to institutionalize yoga in physical training, the Inner London Education Authority (ILEA) had issued instructions to BKS Iyengar to teach only the physical and breathing aspects of yoga while the philosophy of yoga in therapy was ignored. 7 The philosophical component of yoga was eventually overshadowed. The yoga practiced today largely has connotations of intracultural exchange and dissolution of philosophy and is different from the traditional yoga taught as per the Gurukul system in India.
Today, yoga is a thoroughly globalized phenomenon. With increased focus on well-being and increased scientific research in the field of yogic sciences, the modern context views yoga as a complementary and alternative therapy in combating metabolic, psychosomatic, and mental health disorders, by addressing the root stressor. 8
Components of Yoga
Yoga traditionally has eight limbs (Ashtanga Yoga by Patanjali). They are yama (one’s conduct in society), niyama (one’s personal conduct), asana (physical postures), pranayama (methods of increasing energy—prana—predominantly through breathing exercises), prathyahara (withdrawal of the senses), Dharana (concentration), Dhyana (meditation), and Samadhi (self-realization). 9 Further, there are four paths of yoga which are Raja Yoga (path of practice), Bhakti Yoga (path of surrender), Karma Yoga (path of selfless action), and Jnana Yoga (path of knowledge). 10 Each text of yoga, in its vastness, reaches the single objective of transcending the mind, beyond emotions and intellect, to reach a realm of consciousness of complete awareness and oneness (Turiya).11, 3
It is important to understand that yoga here refers to a lifestyle caused by a deeper practice involving subtler components of the mind and is not restricted to asanas or physical health. The practice of yoga should ultimately cause a shift in a person’s outlook and experience of life as the components of mindfulness become prominent in daily activities, which can prevent clinical manifestations and improve well-being. 12
Psychotherapeutic Potential of Yoga Philosophy as per Traditional Texts
In earlier yogic texts, counselling was provided in an individual/group format by the guru/teacher through a systematic and structured explanation of concepts of the mind (manas), intellect (buddhi), ego (ahankara), and consciousness (chitta) to help restructure the perception of individuals to resume their duty. The ultimate goal of an individual was emphasized as beyond the mental and emotional dimensions towards moksha/self-realization.
For example, a traditional text called Yoga Vashishtha describes the dialogue between a person (Rama) suffering from ideas of dejection to the world, hopelessness, helplessness, and suicidal thoughts, with his guru/teacher (Vashishtha). Ultimately, Rama gets clarity of thoughts from his conversation with his teacher Vashishtha and comes out of depression to resume his worldly duties with a sense of detachment (vairagya). 13 In BG, a disciple (Arjuna) suffering from panic, anxiety, and depressive symptoms (Vishada) on facing a stressful situation is addressed by the teacher (Krishna) on methods to cope with such situations using the tool of selfless action (Karma Yoga), acceptance (Bhakti Yoga), self-discipline (Raja Yoga), and knowledge (Jnana Yoga). 14 Similarly, in Taittariya Upanishad, a dialogue between the teacher (Varuna) and student (Brighu) addresses the identity/existential crisis faced by the student, by facilitating an understanding of the five levels of holistic existence (panchakosha) through systematic inquiry. 15
These Vedic texts provide insight into achieving a balanced state of physical, mental, and emotional health and accelerating towards a higher state of consciousness (brahman/moksha). These texts remain largely unexplored for their potential application in a clinical setting.
Adaptation of Yogic Philosophy in Western Psychology
The popularity of the philosophy of yoga in the West started as early as the 19th century. Further, yogis such as Swami Vivekananda, Swami Rama, and Maharshi Mahesh Yogi carried the philosophical and spiritual essence of yoga to Western countries of Europe and the United States. The psychotherapeutic impact of yogic philosophy was translated and studied by modern psychologists and orientalists in the early 1800s. Various Vedic literature was translated to Latin, Greek, and German in an effort to understand the mind according to Hindu philosophy. Academicians, Indologists, and psychologists worldwide made efforts to study these philosophical texts, including Carl Jung, Sir John Woodroffe, Griffith, and John Muir. Prominent psychologists Carl Jung and Arthur Schopenhauer had extensively studied the Upanishads and Yoga Sutras. 16
Jung (2021[1939]) 17 had acknowledged Patanjali, the father of yoga, for drawing a relationship with philosophy and applied psychology. While he acknowledged Patanjali’s work on understanding the mind “chitta” and the process of training the mind, the higher components of yoga, which talk about the union with universal consciousness, were left out. 18 A few components of yogic philosophy that Jung adapted into Western psychotherapy include the concepts of Karma and Kleshas (developed further by Jung as unconscious mental obstructions), self, archetype (as samskaras), and psyche (as chitta). 16 Practices such as Swadhyaya (introspection), meditation, and mindfulness-based techniques are also adaptations from the Indian philosophy. Recent developments in the field of health and positive psychology resemble concepts from the Indian system. Concepts such as eudaimonia and well-being corelate to the aspect of “sattva” in the yogic philosophy and the humanistic paradigm of Maslow correlates with the Purushartha theory in the Vedas. 19
Thus, we see the adaptation of traditional yoga philosophy into the theoretical framework of modern psychology.
Western Models of Psychotherapy vs Yoga-Based Counselling Program: Similarities and Differences
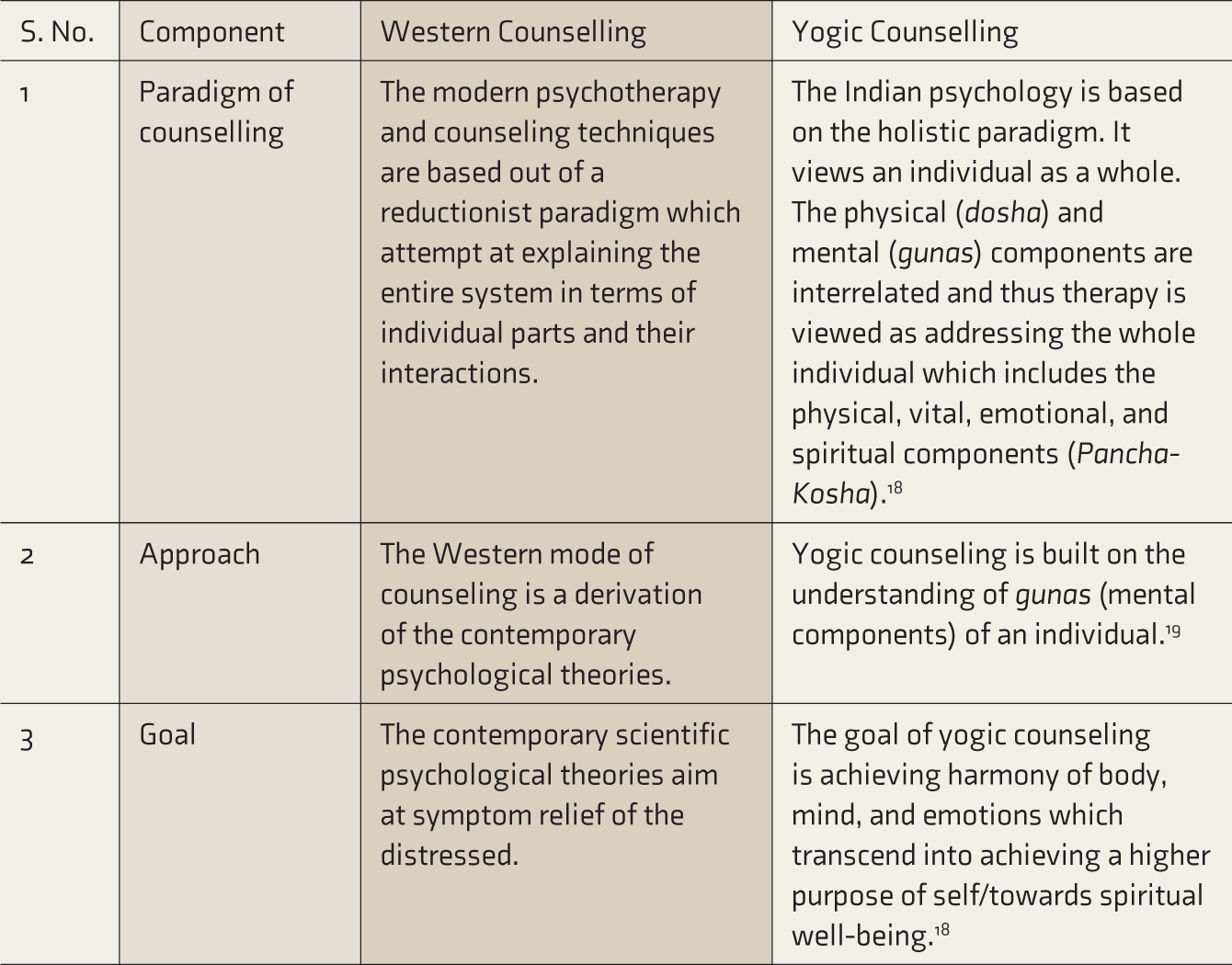
While the goal of counselling in both the Eastern and Western models of counselling remains the same, which is to cause a behavioral change in an individual based on a cognitive shift of perspective, there are some differences in the process of counselling (Table 1).20, 21
Differences in Yoga-Based Counselling and Western Models of Counselling
Limitations of Modern Psychotherapy in India
The Western psychotherapy models largely applied in India to treat common mental disorders (CMD) include Cognitive Behavioural Therapy, psychoanalysis, and psychodynamic psychotherapy. Although there are studies that have demonstrated effectiveness of Western psychotherapies in the Indian population,22, 23 according to the Global Burden of Disease Study (2017), 24 there are significant challenges that hinder its application to a vast majority of population which requires psychosocial support, especially in rural India. These include mental health treatment gap, the need for community based interventions, and the need for cultural adaptations. As the majority of the Indian population is not urbanized or literate, understanding the theoretical framework of these Westernized therapies is challenging for them. 25 Further, social psychology denotes how culture plays an integral part in an individual’s idea about self, community, structure, and social relationships. The basic nature of the Indian population, which is psychological dependence, need for societal validation, and strong religious beliefs in concepts such as rebirth, karma, etc., makes it difficult to adapt to Western therapy. 26
Research in cultural competence and cross-cultural interventions has demonstrated the need for an individualized culturally modified adaptation of therapeutic models in counselling. A culturally acceptable model for counselling is essential not just in the treatment paradigm of intervention but also in diagnosing and understanding the emotional problems of the individual.
In this context, Yoga-based Counselling Program (YBCP) could explore the traditional Indian methods described in the yogic texts, especially the PYS, Vedas and Upanishads, BG, etc., to understand and conceptualize a framework of counselling for persons with CMD in India.
Need for YBCP in CMD
CMD are a group of distress states generally encountered in community and primary care settings. They manifest with anxiety, depressive, and unexplained somatic symptoms. 27 Among the CMD, with regard to depressive disorders, yoga improves psychopathology, and quality of life in most CMD. 28 Yoga reduces acute stress and anxiety in case of psychiatric disorders. 29 A single session of 60-minute yoga practice demonstrated an increase of 27% of brain GABA levels from the baseline (effect size = 0.49), whereas there was no change in the GABA levels after the reading session. 30 In a meta-analysis of 12 Randomized Controlled Trials (RCT) on the short-term effect of yoga for depression, with 619 participants, moderate evidence for yoga was demonstrated over usual care and aerobic exercises. Yoga was compared to usual care (standardized mean difference: −0.69; 95% CI: −0.99 to −0.39; P < 0.001; heterogeneity: I 2 = 86%; χ2 = 28.81; P < 0.001) and aerobic exercise (SMD = −0.59; 95% CI −0.99 to −0.18; P = 0.004; heterogeneity: I 2 = 68%; χ 2 = 3.08; P = 0.08). The subgroup analysis of intervention models for these RCTs showed that breathing/meditation-based yoga interventions, along with a component of lifestyle advice/yoga theory, was superior to exercise-based yoga interventions. 31 Yoga elevated the levels of oxytocin (a hormone related to the feeling of well-being). 32 The change in psychophysiological parameters (biomarkers) of depression, anxiety, and somatoform disorders by yoga intervention have been established in the studies above. This corresponds to the yogic philosophical concept of “Panchakosha theory,” which states that alterations in the subtler sheaths of existence can influence the grosser sheaths. While most of these studies focused on asanas, pranayama, and mediation techniques, the philosophical component of yoga was not utilized. Considering the huge gap in demand and human resource availability in a large country like India to meet mental health needs through conventional psychotherapeutic approaches, it is important that more indigenous and culture-sensitive psychotherapy options are explored. Yoga, with its rich philosophy, has been utilized for achieving calmness of mind in India and other South Asian countries for centuries. In fact, there is a recognized separate stream of yoga called Jnyana Yoga (yoga of knowledge) that focusses on using perception, cognition, and introspection to resolve psychological conflicts and achieve spiritual growth. 33 Thus, the benefits of the yoga practice in mental health disorders may be enhanced further by enriching it with philosophy-based counselling.
What Is YBCP?
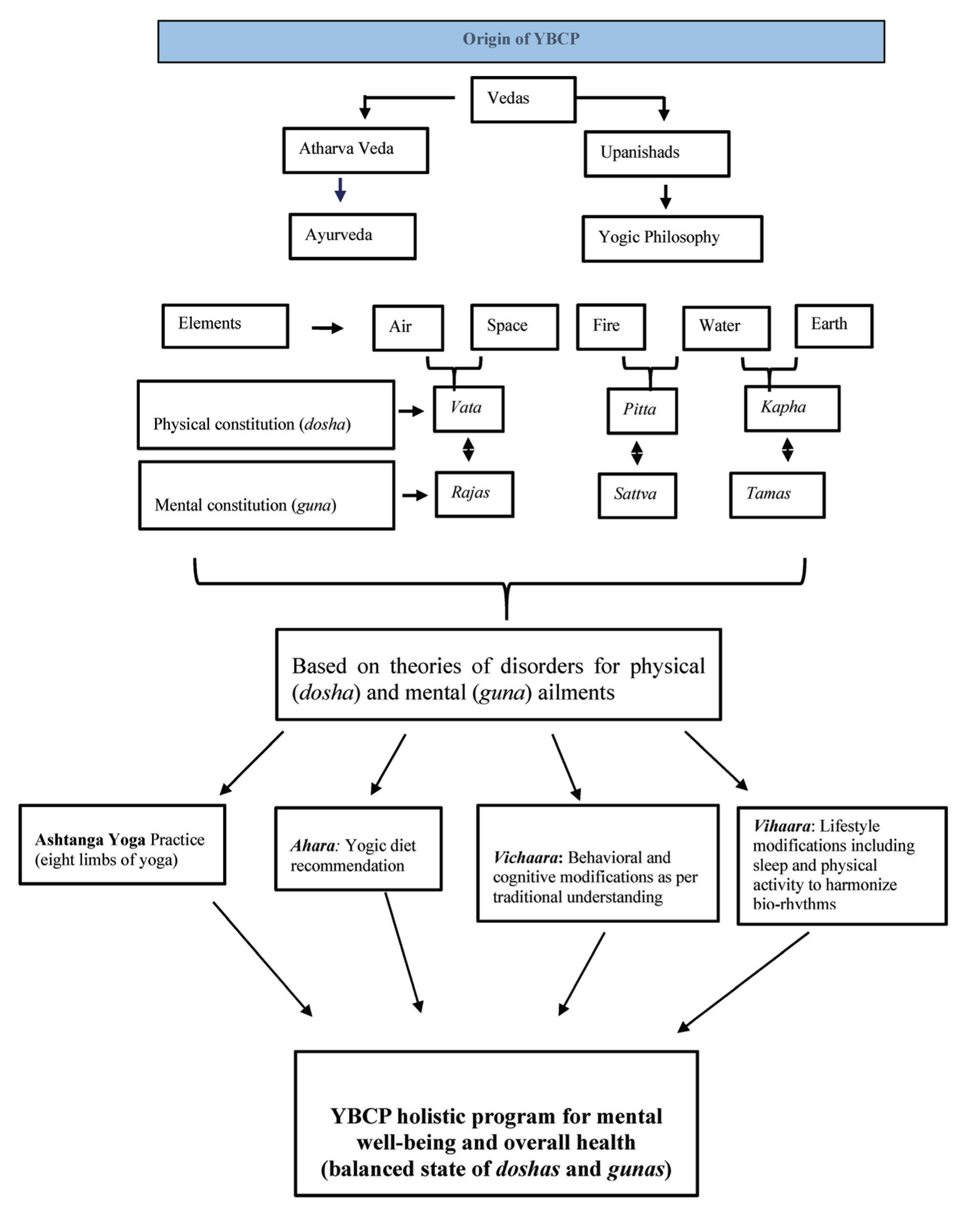
YBCP refers to the psychotherapeutic relationship aiming to cause cognitive and behavioural changes in an individual by yogic counselling and recommending lifestyle modification based on the traditional Indian yoga texts. 8 The stress-vulnerability model demonstrates the aetiology of CMD as a combination of many factors including biological triggers, personality traits and environmental factors including social triggers that can cause distress. 34 YBCP is a psychophysiological therapy that integrates both physical and psychological aspects of therapy, yoga and Ayurveda are interrelated systems that conceptualize the integration of the five elements (Pancha Bhootas) into “guna” as the evolving trait of personality and “dosha” as the corresponding physical constitution. They bring out the essence of balance in the physical (dosha) and mental constitution (guna) of an individual, leading to health. In contrast, an imbalance in either of the two leads to disease (Figure 1). This forms the fundamental basis of YBCP.
The principal components of the YBCP include the following.
Panchakosha Model and Understanding Mental Disorders from Yogic Perspective
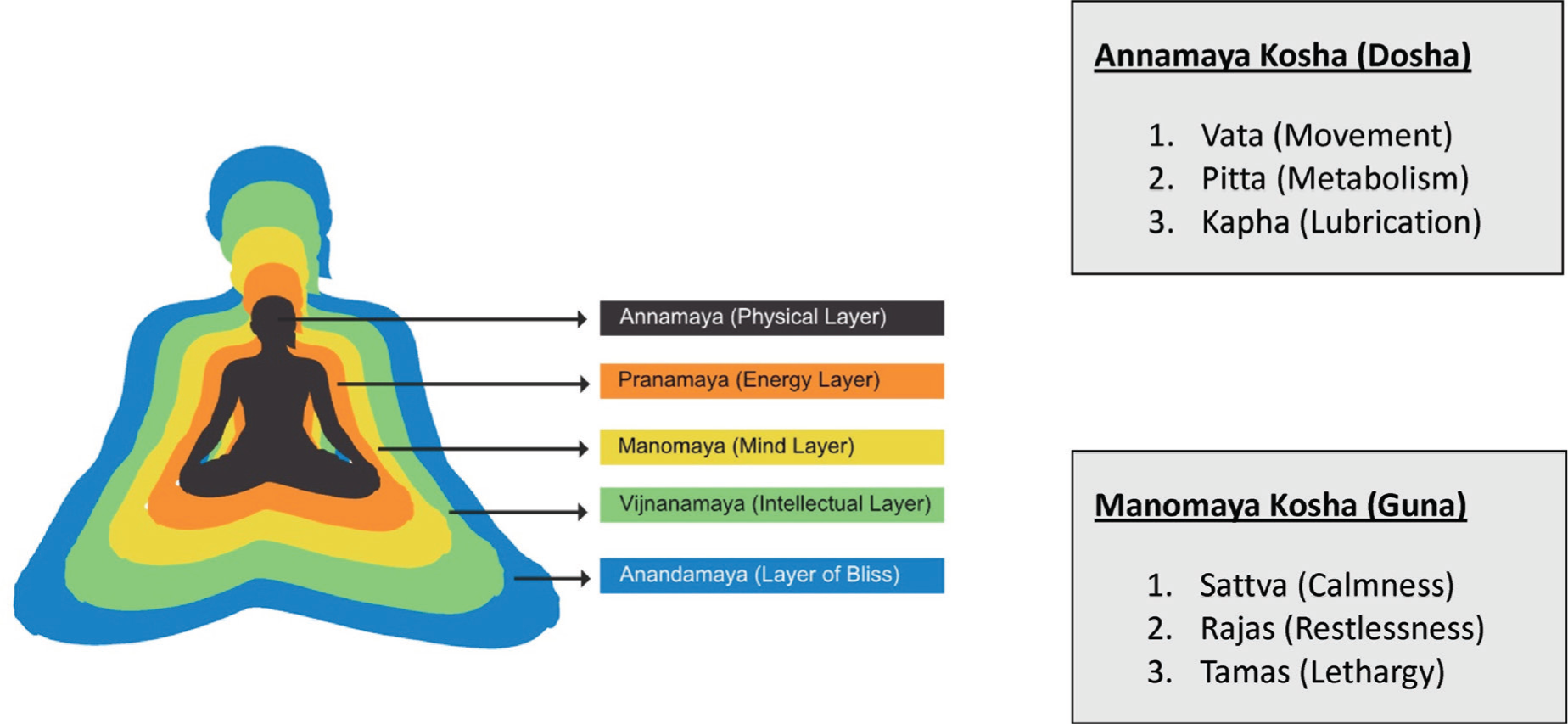
The Integrated Approach of Yoga Therapy (IAYT) for mental health disorders describes the cause for psychological disturbances as the deep-rooted emotional conflicts that lead to psychological stress. 8 Stress, according to yoga, is attributed to the speed (Vega) of repetitive thoughts/ideas, which lead to imbalances in the mind, leading to agitation or negative emotional states. This state of unrest at the mental level (Manomaya Kosha) would lead to an imbalance in the other levels of existence. At the physical and energy levels (Annamaya Kosa and Pranamaya Kosa), excessive speed and demanding situations create stress; at the emotional level (Manomaya Kosa), imbalances are caused by strong likes and dislikes; and at the psychological level (Vijnanamaya Kosa), conflicts and egocentric behavior are responsible for imbalances found at the gross level.
YBCP aims at the holistic treatment of an individual through the incorporation of specific tools of yoga addressing each of the five levels based on the individual’s physical (dosha) and mental (guna) constitution (Figure 1). Practices specific to each sheath would be suggested to an individual, which includes components of the diet, asana, pranayama, cognitive and behavioural practices emphasizing self-reflection, mindfulness, and other philosophical thoughts based on yoga philosophy.
Diagrammatic Representation of Origin and the Holistic Components of YBCP for Mental Well-Being
Concept of Gunas to Achieve Mental Balance
Yogic texts classify attributes of an individual arising from the mental level of existence (Manomaya Kosha) into three fundamental types: sattva (flexibility), rajas (excitation), or Tamas (inertia/rigidness). 23 Scientific literature shows that different psychiatric disorders are characterized by the dominance of different gunas.35, 36 Vedic Personality Inventory (VPI) is a validated instrument 37 that provides an objective measure for each guna in an individual.
Yogic texts also prescribe a detailed lifestyle management guideline to bring balance at the level of gunas. It is considered that in the process of emotional and spiritual development, the mind should progress from tamas to rajas, rajas to sattva, and sattva to gunatita (transcending gunas). A study correlating the VPI with well-being demonstrated that sattva was positively correlated with well-being, while rajas and tamas were negatively correlated. 36 An assessment of the gunas in a clinical population, comparing persons with depression (n = 20) with heathy controls (n = 20), demonstrated that the clinical sample was predominantly rajasik compared to the healthy sample who showed sattvik disposition. 35 In another study that included persons with anxiety disorder, the clinical sample demonstrated high rajasic and tamasic factors, which were associated with impaired quality of life. 36 Previous studies have also demonstrated a correlation of the VPI scores and psychological construct and mental health conditions, indicating the similarity of the five-factor model of personality traits with the guna-based assessments. 38
According to the BG, the modification of personality (guna) can be made by strengthening the dormant gunas in a person instead of focusing on the dominant guna 10 (Shloka 9.15-17). This principle is being applied in YBCP.
Concept of Doshas to Achieve Physical Balance
According to traditional Indian systems of medicine, that is, yoga and Ayurveda, the gunas (sattva, rajas, and tamas) are said to be the psychological correlates of the three doshas (Vata, Pitta, and Kapha), which determine the physical constitution. 39 According to Vedas, the three doshas, when in equilibrium, contribute to health and wellness. If any of the three doshas are aggravated or depleted, it leads to a state of disease. While the doshas affect the body, the gunas take effect on the psyche. 40 However, doshas have also been linked to psychiatric illnesses. For example, vata dosha was higher in paranoid illness. 41 For the management of mental disorders, Vedic philosophy provides prescription of diet (aahara), lifestyle modification (vihaara), and psychotherapeutic management (vichara; yogic asana, pranayama, meditation) in various permutations and combinations according to the individual’s physical and mental constitution.
In summary, according to the Vedic concept, well-being is influenced by three subtle energies of the psyche (sattva, rajas, and tamas), which are also influenced by the three doshas of the gross body (vata, pitta, and kapha). 42
The association of the gunas, tridoshas, and five basic elements can be seen as follows:
Kapha–Tamas—Water and Earth Vata–Rajas—Air and Space Pitta–Sattva—Fire and Water
Well-being is achieved by a balance in the physical and mental constitutions.
The Panchakosha Model with Correlation of Dosha and Guna
Concept of Vritti to Understand Mental Modifications
Patanjali describes the vrittis as the modifications of the mind. The five vrittis described in the PYS are: (a) pramana (wakefulness/being in the present), (b) viparyaya (wrong knowledge/ assumptions), (c) vikalpa (imagination), (d) nidra (sleep), and (e) smriti (memories). Patanjali states that throughout the day, each person operates from one of these modifications of the mind and that each of these could either be helpful in our evolution or an impediment (klishta -aklishta). 8 Operating from the state of vrittis for selfish motives could lead to mental afflictions, while operating from these states at the backdrop of mental discipline and detachment (abhyasa, vairagya) could lead to a sense of contentment and well-being. Throughout the day, one can mindfully assess the various states of mind he/she operates from (vritti). Vrittis are different modes of functioning of the mind such as mindfulness of the present moment (pramana), misinterpretation of the facts (viparyaya), day-dreaming (vikalpa), deep sleep (nidra), and flashbacks of memory (smriti).
This provides an insight to plan a suitable intervention to bring balance into the different modes of the functioning of the mind.
Research on YBCP
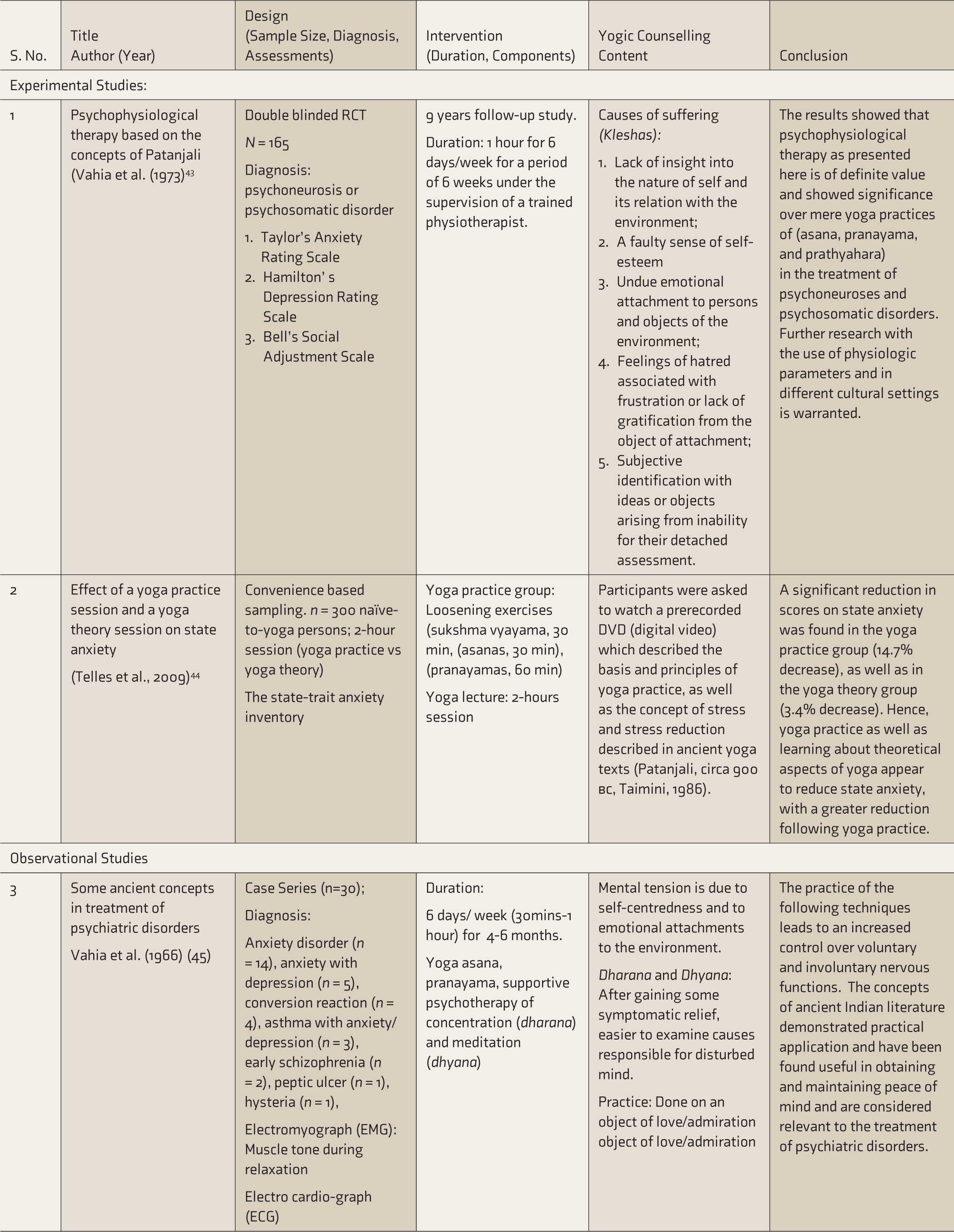
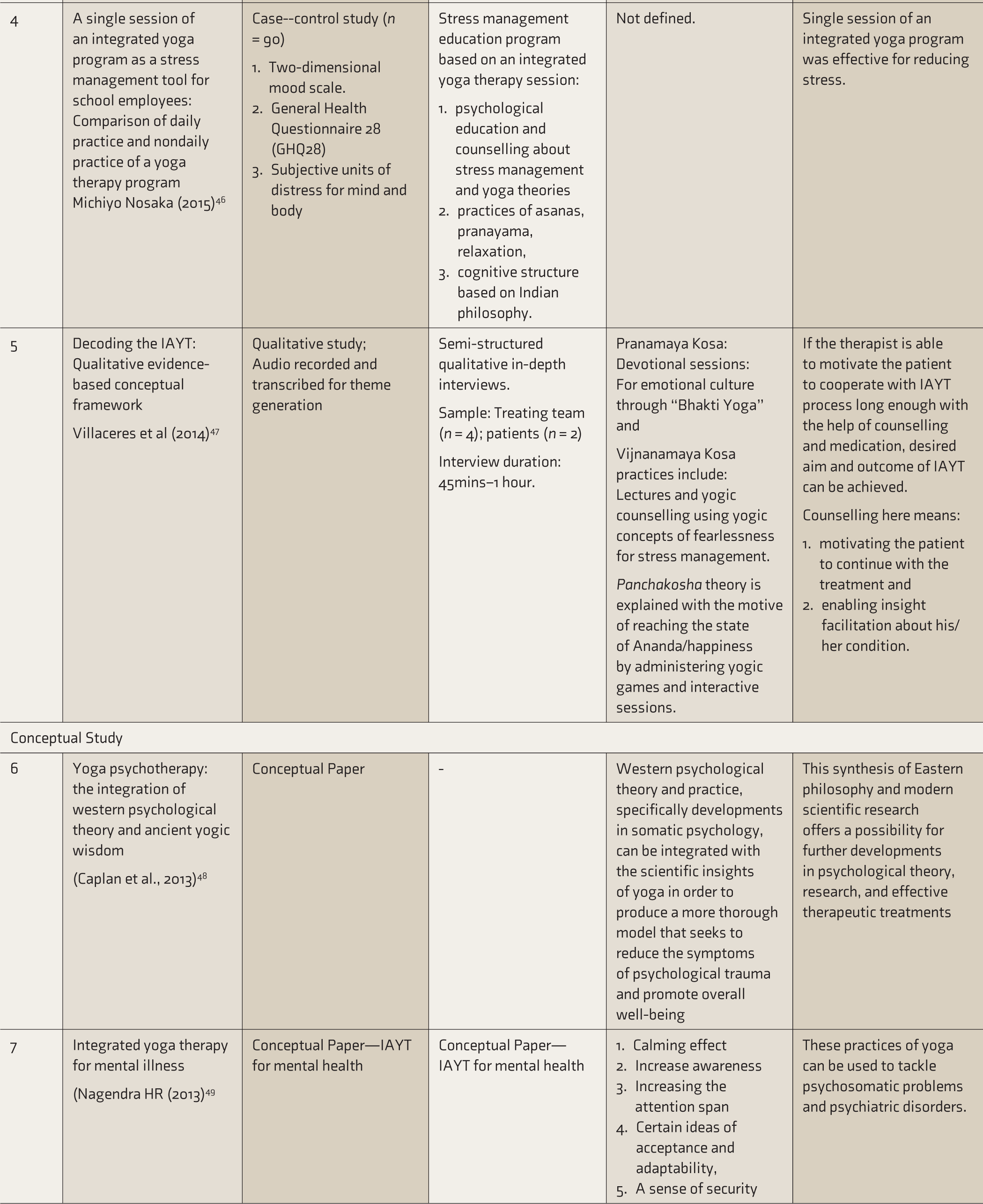
A literature search using keywords “Yogic counselling,” “Yoga-based Counselling,” “Yoga AND counselling,” and “Yoga Philosophy” in search engines of PubMed and Cochrane Library from all timelines yielded a total of 15 research studies of yoga philosophy applicable to mental health conditions (Table 2).43–49 The final list after excluding unpublished work and studies not based on clinical mental health conditions included experimental studies (n = 2),43, 44 observational studies (n = 3),45–47 and conceptual papers (n = 2).48, 49 All of the above studies had a central theme of clinical application of yogic philosophy in psychiatric conditions. These studies give an insight into the implementation of YBCP. The conceptualization of using yogic philosophy in the treatment of psychiatric disorders is seen as early as 1966 by Dr Vahia by using the principle of “vrittis” (modes of mind). 42 This conceptual study also highlighted the importance of symptomatic relief and relaxation as a prerequisite to gaining clarity of the mind to recognize the causes of distress. A few of these studies give an insight into the therapeutic relationship and qualities of an effective therapist47, 49 and the implementation of a yogic educational program in a group setting.44, 46 It is noteworthy that preliminary evidence points towards the usefulness of yogic counseling in reducing CMD symptoms as demonstrated in a double blinded RCT, 43 a case series, 45 and a case-control study 45 patients with depression, anxiety disorder, and psychosomatic and psychoneurotic disorders, respectively (Table 2). The psychotherapeutic implication in traditional texts of BG and Ramayana were also discussed.50, 51 Case vignettes emphasized and encouraged the applicability and exploration of a Vedic counselling in the clinical setting as an IAYT.52,
Evidence Base for Yoga Based Counselling
While the role of yogic philosophy in a clinical setting is explored, these studies lack: (a) uniformity in diagnosis/screening of patients, (b) common yoga counselling concepts applicable in a clinical setting, (c) individualization of yogic counselling, (d) information on session duration and frequency, and (e) details on development process and validation of a structured yogic counselling program.
Further research into yogic texts and systematization of the same can help integrate the traditional wisdom into the modern clinical application of addressing CMD, bridging the gap of yoga seen as a mere physical culture towards a holistic intervention.
Conclusion
Philosophical dimensions of yoga may also have some therapeutic value in CMD, especially in countries like India where culture-sensitive psychotherapy interventions are more acceptable. However, this needs further exploration through systematic, community-based research before drawing any definitive conclusions. Future studies should aim at developing structured and validated YBCP for addressing specific mental health issues. Questions such as the steps involved in the counseling program, the number of sessions, along with duration of each session and frequency, and how to monitor the progress need to be answered through future research. The adjunctive value of the developed programs should subsequently be tested in clinical settings using a robust methodology.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.