
Abstract
Background:
Gambling disorder is rarely diagnosed in Nigeria. The prevalence and factors associated with gambling disorder in many parts of Nigeria are not known. Our study aimed to evaluate psychometric properties of the Diagnostic and Statistical Manual (DSM)-5 for use as a self-report screening instrument for large-scale studies in Nigeria.
Methods:
Cross-sectional surveys were done involving two independent sampled populations from a hospital setting and the surrounding community. Instruments administered included a semistructured sociodemographic questionnaire, South Oaks Gambling Screen (SOGS), International Classification of Diseases (ICD) 11 criteria, and a screening questionnaire based on Diagnostic Statistical Manual (DSM-5), which was designed as a self-report measure (Sports betting).
Results:
The prevalence rate for gambling disorder was 30.5%. The diagnostic accuracy of DSM-5 and ICD-11, and SOGS were comparably similar. Factors associated with gambling disorder (sports betting) were low educational level and poor employment status.
Conclusion:
The DSM-5-based screening questionnaire showed good psychometric properties, with sensitivity and specificity comparable to that of ICD-11 criteria and SOGS. The study also found a high prevalence of gambling disorder. There is a need to address educational and employment opportunities.
As a self-report screening tool, the DSM-5-based screening questionnaire showed good psychometric properties comparable to those of SOGS and ICD. There is a high prevalence of gambling disorder in the community, and the associated factors were low educational status and employment status.Key Messages:
From antiquity, gambling has always had an attractive social appeal.1,2 For many persons, gambling is a form of recreation and rewarding entertainment. However, for some subsets of the gambling population, significant problems affecting behavior have been documented. 5
The Diagnostic Statistical Manual (DSM-III) defined pathological gambling as a progressive loss of control of gambling impulses. 3 The DSM-IIV adopted a criterion-based diagnostic approach: with a minimum of five positive items for diagnosis. In the DSM-5, the illegal act criterion was excluded and a minimum of four positive items were required.4,5 Also, in DSM-5, further development in the understanding of apparent neurobiological correlates and similarity to addictive behaviors necessitated a subclassification under substance-related disorder.6,7
Clinical studies have focused more on prevalence rates based on the five-item criteria in DSM-IV and available generic gambling instruments. Reported prevalence rates of gambling disorder differ across countries and continents. In a countrywide study of over 4,000 adults in New Zealand, 2.7% of those sampled met the diagnostic criteria for probable pathological gamblers, while 4.7% met the criteria for problem gambling. 8 Another survey in Seville, Spain, diagnosed 1.7% of the population as probable pathological gamblers and 5.2% as problem gamblers. 9 There are very few prevalence studies in Africa. 10 Reported prevalence rates of pathological gambling in Africa have been limited to defined local groups.
The most common form of gambling among young adults in Nigeria is sports (soccer) bets. Conservative estimates put the number of Nigerians engaged in soccer bets as above 60 million. Every 4 in 10 Nigerian play some type of sports bet. 11 The southwestern part of the country is reputed to have the largest number of sports betting stalls than any other part of the country. 12 Regardless of these anecdotal statistics, the prevalence rate of gambling disorders is not known. The problem is partly due to limited instruments for large scale studies.
In many Nigerian clinic settings, the International Classification of Diseases (ICD) is the principal diagnostic instrument used. Prevalence estimates have been difficult due to lack of screening instruments that are simple and easy to use. Further, the criteria in DSM-5 have not been compared with the diagnostic criteria of ICD-11. Our objectives were to estimate the prevalence rate and associated factors of gambling disorder in the Sagamu community, a major southwest community in Nigeria. We also aimed to compare ICD-11 criteria with DSM-5 criteria and to compare the diagnostic accuracy of DSM-5 criteria with ICD-11 criteria in a clinical setting and with the South Oaks Gambling Screen (SOGS) in a community sample.
Materials and Methods
Setting
Sagamu is a major commercial center and transportation hub in Nigeria. It consists of 15 wards. It is one of the largest and densely populated semiurban towns in the southwest region of the country. It has an estimated population of 255,885 at the last population census.13,14 It hosts several diverse populations, and sports-betting shops and stalls can be found on almost every street in Sagamu. The community is semiurban, and the majority of the people are traders and farmers. The Teaching Hospital caters to the tertiary health needs of the community.
Design and Participants Recruitment
The cross-sectional surveys were conducted between March 2019 and February 2020. Participants were recruited from the clinic attendees and the various wards in the community. The recruitment was done in phases. Phase 1 involved recruitment of clinic attendees from the General Outpatient Unit of the Teaching Hospital in Sagamu. Phase 2 involved the recruitment of participants from the community. Inclusion criteria included participants who gave informed consent (verbal and written) and played or ever played sports bet. We excluded respondents with a history of mental illness or cognitive disorders and those below 18 years of age.
Procedure
The first sampled population was recruited from patients presenting at the General Outpatient Unit. A survey form was used to recruit participants who play sports bet, from clinic attendees from all clinic days and units, for further interviews with the investigators. The diagnosis was made based on the ICD version 11 criteria for pathological gambling. 15 Fifty-three persons who play sports betting regularly were recruited for the clinical survey.
The phase 2 recruitment commenced after the completion of phase 1. It involved recruiting participants from the Sagamu community. The sample size was determined using Yamane’s formula, which pinpoints accuracy when the population is finite and the desired accuracy is greater than 5%. 16 The sample size calculated via this formula was 400.
Multistage random sampling method was adopted. The more populated wards were ranked in terms of population size in descending order. A greater number of participants were recruited from the heavily populated wards. House to house visits were done in streets that were randomly selected, to recruit residents within each ward.
Investigators were organized into cells headed by psychiatrists. Each cell was made up of three members. The instruments were used in the English language. Research assistants were taught how to use the various instruments and to communicate effectively in the local language if the wordings were not well understood.
Instruments
A battery of instruments and questionnaires were used.
Sociodemographic details
A sociodemographic information questionnaire was used to obtain sociodemographic details such as age, sex, employment status, and level of education.
The SOGS
The SOGS, developed by Lesieur and Blume, is a 20-item gambling screen based on the DSM-III criteria for pathological gambling. 17 It can often be self-administered with interviewer guidance. Not all items are scored. It is a validated, reliable screening tool that can be used for large-scale community studies. It has been widely used and reported to have good reliability in separate surveys, with coefficient alphas of 0.69 and 0.86 respectively, indicating good internal consistency and reliability. 18 It was intended to screen for individuals with pathological gambling problems. In Nigeria, the reliability was reported to be between 0.75 and 0.78. 19 Further, the SOGS has been reported to have good psychometric properties with DSM-5 criteria. 20 The cutoff criteria of ≥5 for individuals with probable gambling disorder, 1–4 for problem gambling, and 0 for No gambling problem were adopted for scoring in both the study samples. We trained the research assistants to use the English version and to adequately and appropriately interpret the items to the participants.
The DSM-5 betting questionnaire
The questionnaire was developed by the authors. The questionnaire items are based on the 9-items in the DSM-5 criteria for gambling disorder.20,21 We simplified the wordings in keeping with the local setting, and we designed it to be self-administered. We aimed at making it easier for our participants in our social context to understand and relate it to their local betting activities. It was scored on a binary scale with “yes” responses scoring 1 and “no” responses scoring 0, similar to scoring points adopted by Stinchfield et al. 12 A cutoff score of ≥4 was decided. Three pilot surveys were done to pretest the DSM-5 questionnaire and assess the understanding of its items. Its test–retest reliability was done within two weeks. Internal reliability was assessed using Cronbach’s alpha. Confirmatory factor analysis was done to test the underlying latent assumption as a measure of its construct validity. Sensitivity and specificity were examined by comparing the diagnostic correlation with the ICD-11 diagnosis by Consultant Psychiatrists. The convergent validity was measured by a comparison of correlation coefficients with scores of the SOGS. Discriminant validity was measured by comparing correlations and mean differences with independent demographic variables such as age, sex, and education. The clinical sample was used to determine classification accuracy, sensitivity, specificity, hit rate, precision rate, receiver operating curve (ROC), and area under the curve (AUC).
ICD 11th edition
Produced by the World Health Organization, 15 this manual provides a basis for the classification of psychiatric disorders. The criteria for gambling disorder are based on a one-year pattern or significant pattern of misbehavior related to gambling. 15 A major limitation is the difficulty in the utility of the diagnostic guideline in large-scale community studies and it is more adaptable to clinical settings.
Statistical Analyses
The data were analyzed in stages. In the first stage, we calculated the total scores on the DSM-5 Betting Questionnaire and compared them with the ICD-11 diagnosis. The ROC curve and AUC curve were computed to determine the best cut off criteria for the DSM-5 in comparison to the ICD-11 diagnoses in our clinical sample. The ROC analysis classification accuracy was also computed. We calculated the sensitivity and specificity and other related measures such as hit rate and precision rate, negative rates as important constructs related to sensitivity. Missing data were handled using list-wise deletion.
Reliability was measured by the test–retest method and computing the internal consistency using Cronbach’s alpha. For good reliability, the two measures should have a correlation coefficient greater than 0.70.22–24
The second stage involved computation of the confirmatory factor analysis to measure the construct validity and to determine the factor loadings on a single factor (gambling addiction) using the community sample. The confirmatory factor analysis was done, using Mplus, to confirm the prior hypothesis underlying the construct. The weighted least-square means and adjusted variance approach was used due to the nominal nature of the measure, and the technique is also favored for analysis of ordinal variables. 25
The three indices used were the chi-square goodness of fit (χ2), Standardized Root Mean Square Residual (SRMR), and small standardized residuals correlations. These fit indices were used to predict the model fit by Asparouhov and Muthen. 26 Exact model fit will produce a (χ2), P > 0.05. Otherwise, approximate fit models will produce a χ2 that is significant, that is, P < 0.05, SRMR of ≤0.8, and small residual correlations defined as correlation coefficient r < 0.1.27,28 However, notably, the chi-square model fit (χ2) is known to vary with sample size.
The third stage involved examining convergent validity by correlations of SOGS total scores with the total scores on the DSM-5 betting Questionnaire. Convergent validity was established with r > 0.30. Discriminant validity was examined by comparison of DSM diagnosis with independent variables such as age, sex, and personal income.
Discriminant validity is evident if the coefficients of correlation (r) are <0.1. 29 Ordinal regression analyses of prevalence rates across demographics and prediction of models using binary logistic regression were done. Chi-square tests were used to compare nominal variables with DSM-5 diagnosis. The data were tested for normality using the Shapiro–Wilk test, which (P < 0.001) indicated a skewed distribution using the Mann–Whitney U test of independence and hence we used the Kruskal–Wallis H Test and Analysis of Variance to compare means with the total scores on DSM. Effect sizes were also computed. Factor analyses were computed using Mplus software version 6.4. 26
Ethical Considerations
The ethical committee of the Olabisi Onabanjo University Teaching Hospital approved the study protocol (OOUTH/HREC/273/2019AP). Voluntary and informed consent was obtained from every respondent. Responders were adequately briefed and informed before administration of the instruments.
Results
Demographics
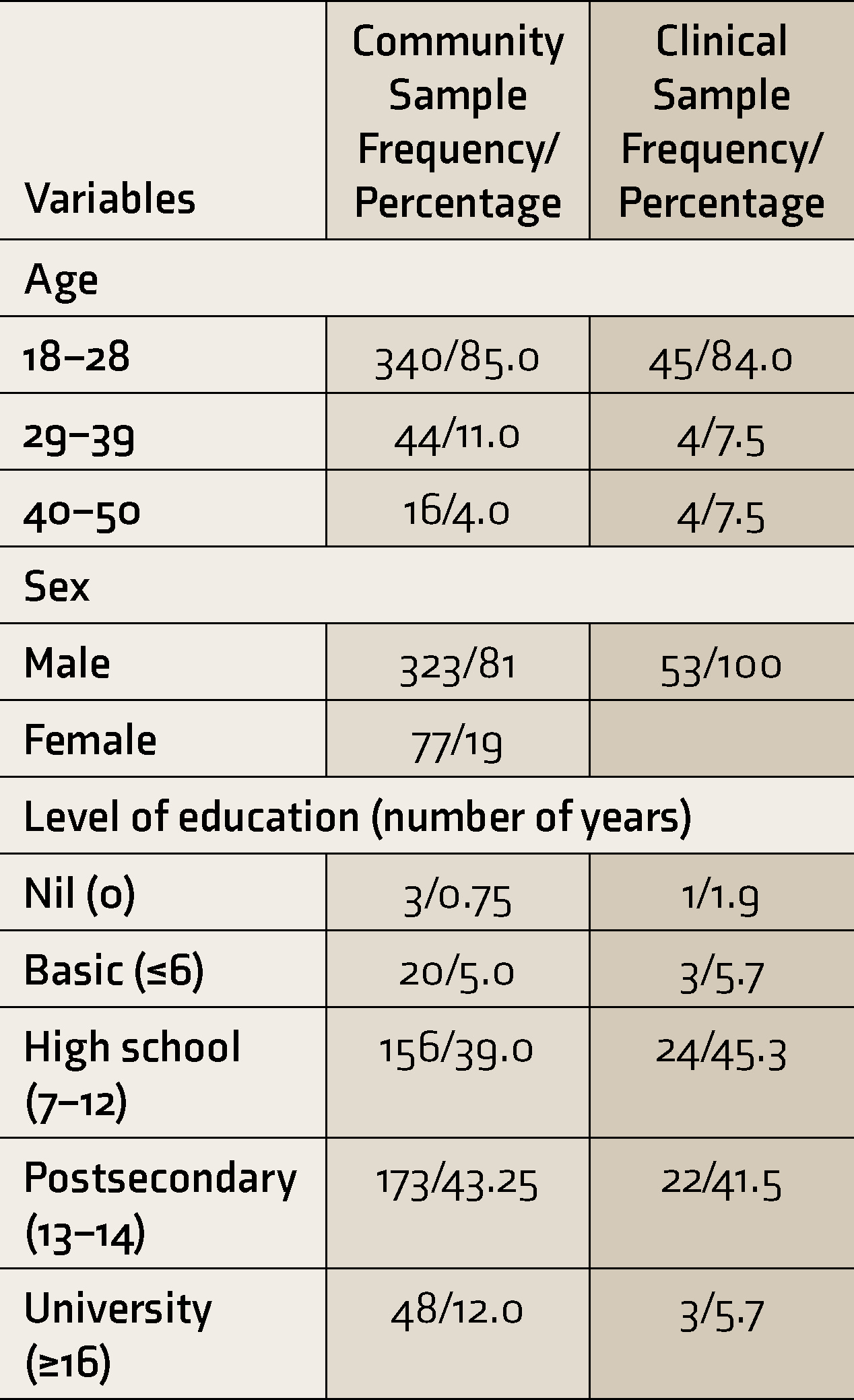
Fifty-three participants were recruited for the clinical study, while 400 participants were recruited from Sagamu community (see Table 1), out of the 507 persons approached (79.0% response rate). Mean ± SD ages in years were 26.05 ± 6.89 (clinical sample) and 25.09 ± 5.09, (community sample). Participants in the clinical sample were all males. The majority (45, 84.9%) were within the 18–28 age group, students (29, 54.7%), and in high school (24, 45.2%). Males constituted the majority (212, 85.1%) of the community sample. More than half of the participants within the community had either played sports bets in the past or are currently active players of sports bets. The prevalence of individuals with probable pathological gambling disorder in the community was 152, 38% (n = 152) using the SOGS criteria, while individuals with gambling disorder made up 138, 34.5% (n = 138) using DSM-5 cutoff criteria. In the clinical study, those who met the ICD-11 criteria and DSM-5 criteria were the same percentage, 22, 41.5% (n = 22), while for SOGS was higher, 27, 50.9% (n = 27). Among those diagnosed with gambling disorder, the severity was mild in 40, 9.8% (n = 40), moderate in 48, 11.18% (n = 48), and severe in 50, 12.3% (n = 50). The item with the lowest endorsement was item 8 (lost an opportunity) on the DSM criteria.
Demographics
Mann–Whitney U test indicated that the mean rank of total scores on the DSM-5 based questionnaire for males in the community sample was 126.26, while for females, the mean rank score was 117.20, U = 3633.33, P = 0.40. Kruskal–Wallis H test showed no statistically significant difference in total scores in DSM-5 Betting questionnaire across age groups in the clinical sample. In the clinical sample, with the DSM-5 based betting questionnaire, the mean rank was 26.67 for age groups 18–28, 33.26 for 29–39, and 24.50 for 40–50, χ2(2) = 0.84, P = 0.66. In the community sample, the mean rank of 120.33 for age group 18–28, 147.56 for 29–39 and 147.38 for 40–50 age group, χ2(2) = 4.96, P = 0.08. Across employment status, Kruskal–Wallis H test showed that in the clinical sample, there was a statistically significant difference in total scores on the DSM-5 based Betting questionnaire χ2(3) = 8.87, P = 0.03, effect size=0.17. Mean ranks were 35.22 in the unemployed, 32.25 in employed, 33.21in self-employed, and 21.50 in students. In the population sample, the mean ranks were 178.50(unemployed), 128.05(employed), 170.47(self-employed), and 104.83 (student), χ2(3) = 42.63, P < 0.001, effect size = 0.17. Post Hoc test showed significant differences across all levels. The correlation between total scores on DSM and income per month was not significant (r = 0.05, P = 0.43).
Across levels of education, in the clinical sample, mean ranks were 11.00(nil formal education), 37.33 (primary), 32.60(secondary), 18.36(postsecondary), 40.50(university), χ2(4) = 15.794.30, P < 0.005, effect size = 0.30. In the population sample, the mean ranks were 86.00(nil formal education), 155.74 (primary), 138.75(secondary), 103.86(postsecondary), and 125.29 (university) χ2(4) = 16.39, P = 0.003., effect size = 0.06. There were significant differences between various educational levels in the post hoc tests at P < 0.05. Further, chi-square (χ2) statistics was significant across certain demographics among those who play sports bets (Table 2).
Prevalence of Sport Betting Across Demographics of Participants
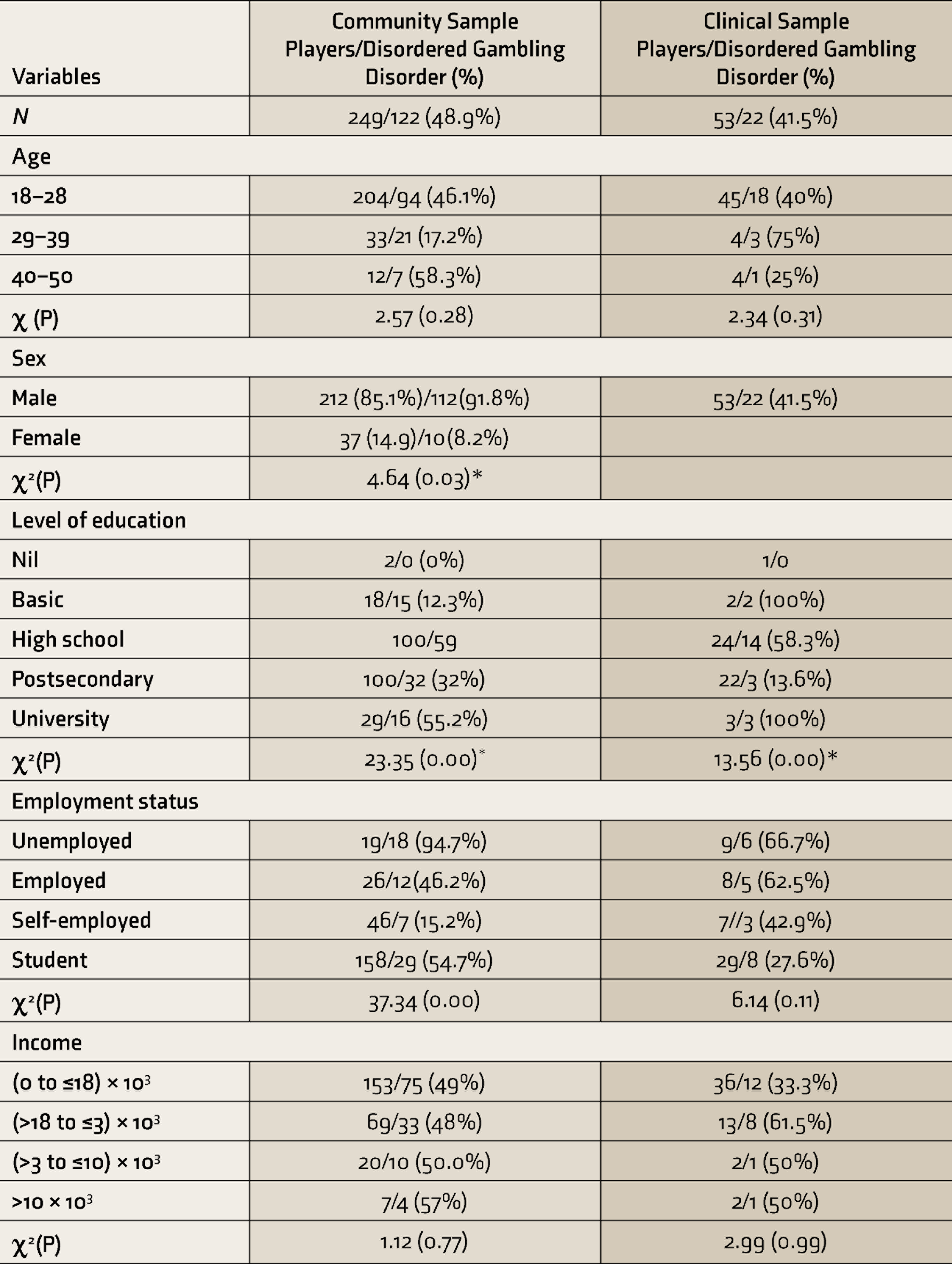
*=# and * means p < 0.05.
Cutoff Point, Sensitivity, Specificity, and Other Predictive Rates of DSM-5 Betting Questionnaire
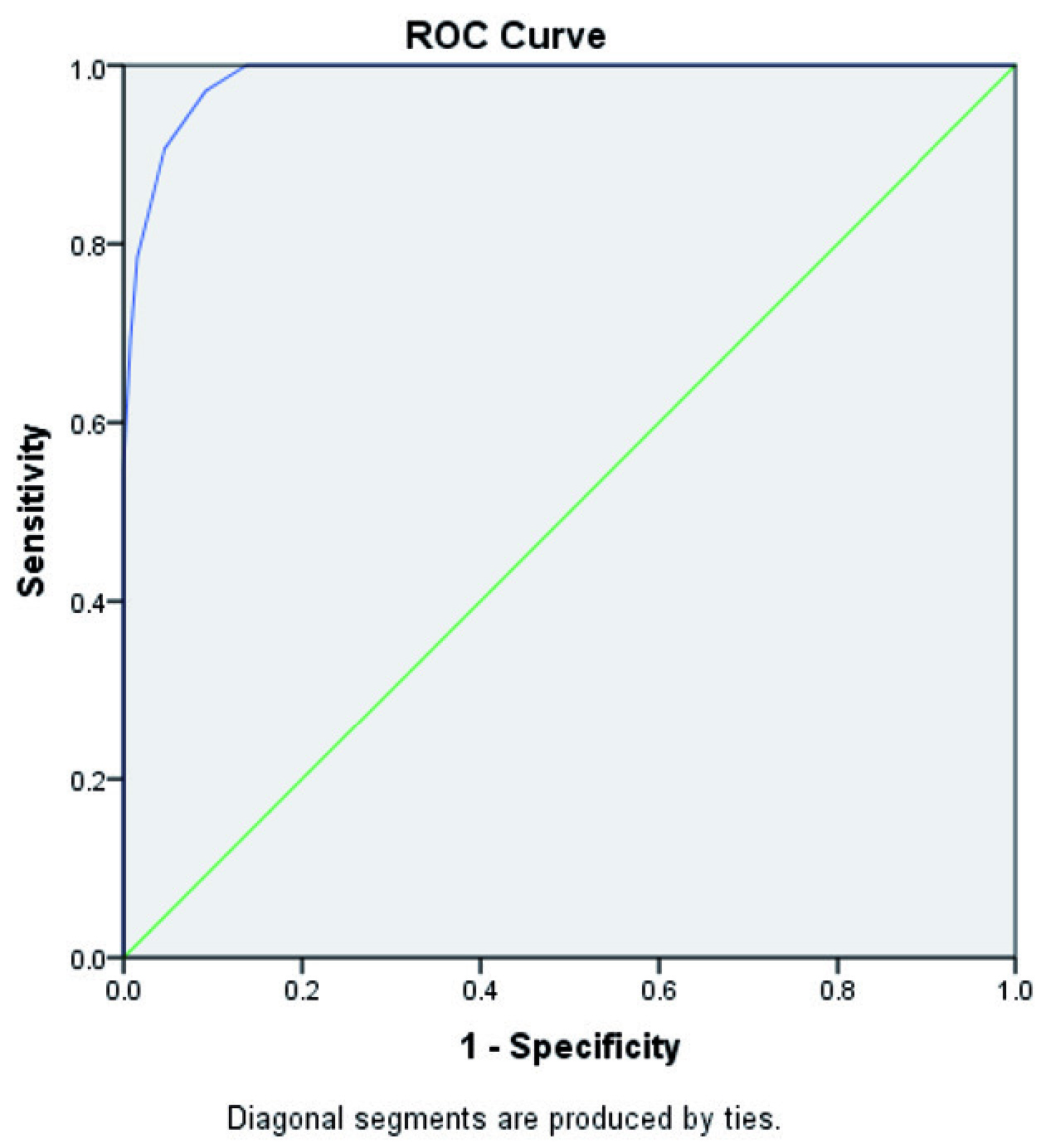
The ROC was used to obtain the best cutoff point for the DSM-5 based questionnaire. The optimal cutoff point score was around 3.5, as shown in Figure 1. The AUC was 0.99 (95% CI 0.98–0.99). Sensitivity was 91.4%, specificity was 94.9%, precision rate was 91.4%, false positive rate was 8.6%, true negative rate was 5.1%, and hit rate was 93.6%. The positive predictive value was 91.4%, while the negative predictive value was 5.1%.
ROC Curve
Reliability Analysis and Confirmatory Factor Indices (CFA)
The test-retest reliability was 0.90. Internal consistency (α) was 0.90 in clinical sample and 0.92 in Community Sample. The CFA was conducted to examine the latent factor (gambling disorder) construct of the 9-item DSM-5 Betting Questionnaire using weighted least means square as the principal estimator. The three parameters of interest used as indicators of model fit were the chi-square goodness of fit χ2(2663.577) = 0.000, the SRMR = 0.07, and standardized residual correlations. These parameters were all small, ranging from 0.57 to 0.18. The majority of the absolute residual variance were <0.10, and only two were <0.10 (0.18 and 0.10). The various factor loadings are as shown in Table 3.
Mean Scores, Frequency, Factor Loadings, and Item-Scale Correlation on the DSM-5 Sports Betting Questionnaire
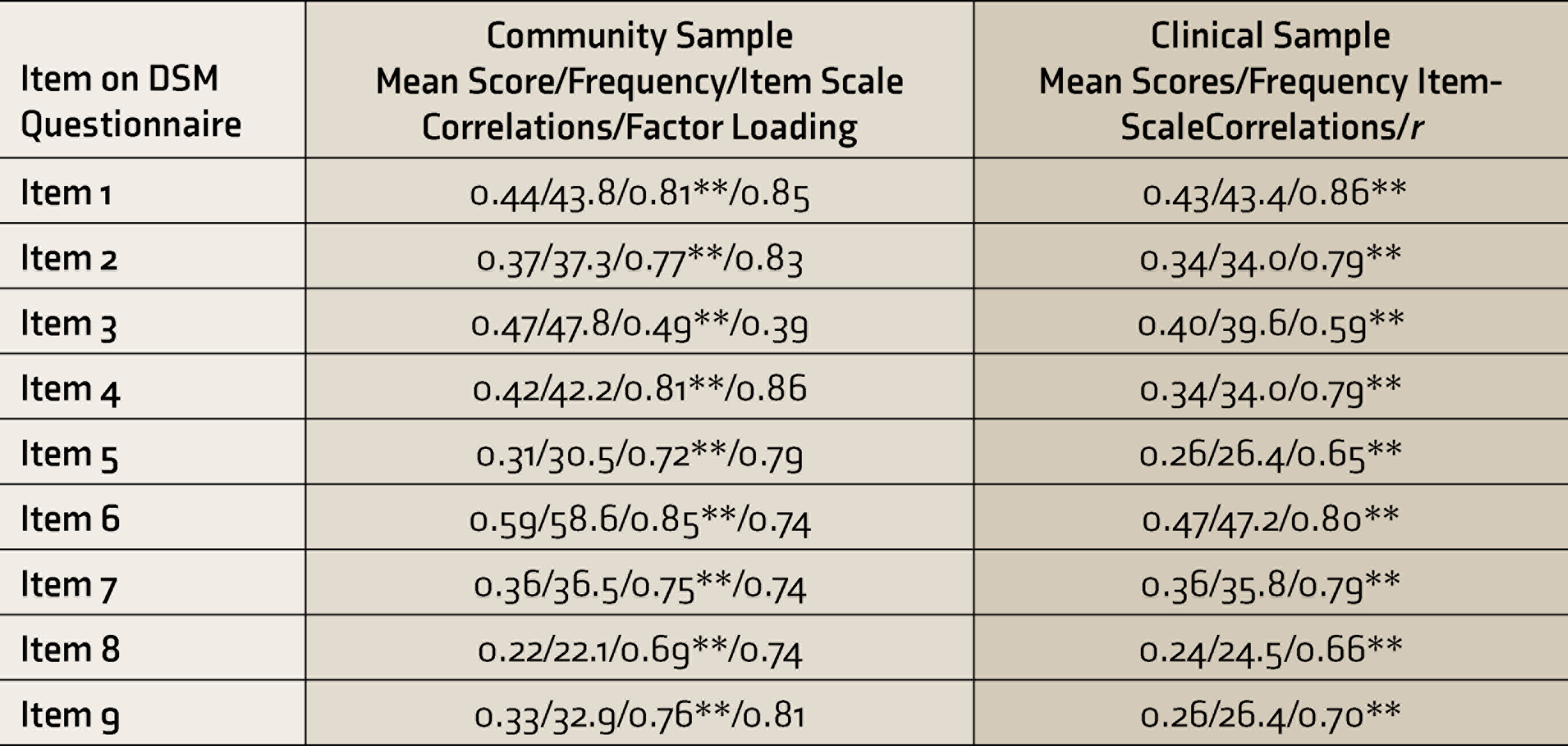
**P < 0.001.
Convergent Validity and Discriminant Validity
The total scores on the DSM-5 Betting questionnaire were correlated with the total scores on the SOGS. Correlations were significant and r were above 0.50 in both the clinical (r = 0.69, P < 0.001) and community (r = 0.74, P < 0.001) samples. Discriminant validity of the DSM-5 Betting questionnaire was established, with low correlations with measures that have no relationship with betting. In the clinical sample, coefficients of correlation with age, gender, education, and employment ranged from r = 0.02 to 0.33. In both clinical and community samples, the majority of correlation coefficient were below r < 0.10.
Factors Associated with of Gambling Disorder on the DSM-5 Self Reporting Betting Questionnaire
Logistic regression was performed to ascertain the effects of age groups, sex, employment status, level of education, and estimated monthly income and the likelihood of participants to be diagnosed with gambling disorder based on DSM-5 Betting questionnaire. The logistic regression model was statistically significant, χ2(5) = 21.42, P < 0.001. The Hosner and Lemeshow test was not significant, P = 0.07, indicating goodness of fit for the model. The model explained 18.4% (Nagelkerke R 2 ) of the variance in gambling disorder and correctly classified 11.7% of cases. Increasing age was not significantly associated with the increasing likelihood of being diagnosed with gambling disorder. Although males were 0.6 times less likely to be diagnosed with gambling disorder than females, it was not significant (P = 0.18). Increasing levels of education were significantly less associated with being diagnosed with gambling disorder (P < 0.005), Increasing monthly income was not significantly associated with individuals being diagnosed with gambling disorder (P = 0.52).
Discussion
Our objectives were twofold. We aimed to compare psychometric properties of the DSM-5 gambling disorder criteria with the ICD-11 gambling criteria and the SOGS. The second objective was to estimate prevalence rates and factors associated with gambling disorder in the Sagamu community using the DSM-5 based sports betting questionnaire.
In validating the DSM-5, we adapted an earlier measure of pathological gambling based on DSM-IV criteria 18 ; but we removed the illegal criterion (item 8). The responses were scored on a Yes and No option with Yes responses = 1 and No responses = 0. Stinchfield’s measure was reported to have satisfactory reliability, validity, and classification accuracy. 26 Unlike the DSM-IV, the cutoff criteria for DSM-5 was based on four positive responses.
We determined the cutoff points, sensitivity, specificity, and classification accuracy by comparing the diagnosis between the ICD-11 diagnostic criteria and DSM-5 criteria using the self-report questionnaire in the clinical sample. The optimal cutoff point from our study was close to the recommended cutoff criteria in DSM-5. 26 The indices were all satisfactorily similar to ICD-11 criteria, showing good psychometric properties as a diagnostic instrument in clinical settings.
The majority of the factor loadings were highly loaded on a single factor, validating the one-factor construct of the scale, with only an item 8 (loss of opportunity) having low average loadings and lowest mean scores in both the clinical and community sample, due to lower endorsement by participants. Participants in our study probably felt that no major opportunity loss was attributable to playing sports bets.
Reliability analysis was satisfactory, and findings were similar to reliability results reported for the DSM-5 in studies on gambling disorder. 26 Convergent validity of the DSM-5 Betting Questionnaire was demonstrated with significant-high correlations of scores with SOGS scale responses in both clinical and community samples. Our findings were similar to an earlier study that reported correlation results obtained with the comparison of DSM-5 and the SOGS. 20 Equally, discriminant analysis showed that the scale has satisfactory discriminant properties in an unrelated context.
The overall prevalence rates using the DSM-5 Betting Questionnaire were 34.5% in the community and 4.5% in the clinical sample. Similar rates were observed with the ICD11 based criteria. In both the clinical and community samples, higher prevalence rates were observed using the SOGS criteria and a cutoff of 5 and above for Pathological Gambling Disorder.
Our study showed a high proportion of persons who had played sports bets. This supports previous research that showed that sports betting is the most common form of gambling in Nigeria. 27 In both samples, more than a third were diagnosed with pathological gambling concerning sports (football) betting. There are no comparable studies in Nigeria; however, the prevalence rate we found is much higher than those reported in many communities with a prevalent gambling culture.28,30.
Unlike previous research, our findings show that the most prevalent age groups engaged in sports betting are those above 28 and less than 40 years. 12 Expectedly, these age groups form the major workforce in such communities and have the means, coupled with relative independence from social constraints or parental authority. They also form the bulk of those who are active sports fans, who embrace technology more readily. More recently, as earlier noted, the high unemployment rate in Nigeria may also be a factor. Consistent with most studies on gambling, males and the unemployed form the bulk of gamblers and of those who meet the criteria for gambling disorder. 31 Noticeably, the population studied was skewed with a higher percentage of males; this is due to the higher recruitment of males probably due to the higher likelihood of males who play sports betting in comparison to females. It is relatively rare for females in our Nigerian context to own up publicly to playing sports bets or any other gambling activity. Our study’s overall demographic pattern showed that many of those who met the diagnosis for gambling disorder were less than 40, unemployed, and with secondary education. The majority were in the low social class, similar to reports from other countries. 31 Further, we found significant differences across sex, employment status, and educational level when cross-tabulated with respects to the presence and absence of gambling disorder. As a social behavior, gambling reflects socio-demographic influences within the socio-cultural environment. 32 Sports’ betting in Nigeria require very little monetary investment and is hence easily affordable; this low investment cost fuels the popularity even among the unemployed. In our findings, there was no significant correlation between income and gambling, which may support earlier reports that that income is not a strong factor associated with gambling behavior. Cognitive distortions have been reported to underlie income spending, with the poor spending a greater percentage of income on gambling. 33 Interestingly, the highest endorsement on the DSM-5 scale in our study was for item 1, which measured increasing amounts spent on gambling to achieve the desired excitement.
Our model, involving age groups, sex, level of education, and employment status, explained less than 20% of the variability of gambling disorder as measured on DSM-5 criteria. Our study showed that among individuals who met the criteria for gambling disorder, those diagnosed as having severe illness were greater in proportion, relative to the milder and moderate forms, highlighting a potentially large population of individuals with gambling disorder who are not captured by the health system with no proper referral network within the community. 34
Limitation
A major limitation of our study is the small sample size, especially in phase 1 clinical recruitment, and the skewed sampling. Also, the ICD 11 diagnostic criteria was not used in the community survey. Our study focused on sports betting as typical of gambling behavior and cannot be generalized to include all forms of gambling.
Conclusion
The prevalence of gambling disorder is high in Nigeria. The main associated factors of gambling disorder are lower employment status and low educational status. The self-report DSM-5 Betting Questionnaire showed good psychometric properties comparable to SOGS and ICD-11 criteria and can be used in large population surveys.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.