
Abstract
Dengue is an arboviral infection endemic in tropical countries. Neurological sequelae to dengue infection are not uncommon, and psychiatric manifestations are increasingly reported. This narrative review aims to present the varied manifestations, postulated mechanisms, and the available treatment options for psychiatric morbidity associated with dengue. The evidence available from eight observational studies is summarized in this review. Depression and anxiety are noted to be prevalent during both the acute and convalescent stages of the infection. The presence of encephalopathy and other neurological conditions is not a prerequisite for developing psychiatric disorders. However, treatment options to manage such psychiatric manifestations were not specified in the observational studies. Anecdotal evidence from case reports is outlined. Special attention is paid to the role of epigenetic modifications following dengue infections and the role of histone deacetylase inhibitors in the management. DNA methylation inhibitors such as valproic acid play a significant role in reversing stress-, viral-, or drug-induced epigenetic modifications.
Dengue is a viral illness caused by a single-stranded ribonucleic acid (RNA) virus belonging to the Flaviviridae family with four different dengue serotypes (DENV 1–4). It is transmitted by infected Aedes mosquitoes. It is a global epidemic with an incidence of around 96 million apparent infections per year 1 and a significant social and economic burden.2,3 India alone contributes more than one-third of such apparent clinical infections. 1 Dengue is endemic in tropical countries, and the incidence of the infection has been progressively increasing through the last two decades.4,5 The illness usually has an abrupt onset, with a course characterized by fever, critical, and convalescence phases. 5 The World Health Organization classifies the illness into two groups: uncomplicated and severe dengue. 6 In the Indian context, severe dengue has been estimated to be 35% of all dengue cases, with a mortality rate of 2% to 3%. 7 All four serotypes are prevalent in India. 8 The critical period marks the essential phase of the severity of the illness that may ultimately lead to hepatic, cardiac, and neurological consequences. To date, there are no approved antiviral drugs available to treat dengue, and the management is mostly symptomatic and supportive. 6
Dengue’s neurological involvement is increasingly recognized but not well understood. DENV-2 and DENV-3 serotypes are reported to be associated with neurological manifestations. 9 Although the studies on incidence rates of neurological sequelae secondary to dengue infection are limited in the Indian context, 10 neurological manifestations were reported in 7% to 10% of the infected adults11,12 and 28% of the infected children. 13 The prevalence of dengue encephalopathy has been estimated to range from 0.5% to 6% in patients with dengue hemorrhagic fever. 14 Postulated mechanisms include vasculitis with fluid extravasations, brain parenchymal edema, metabolic derangements, vascular hypoperfusion, autoimmune cross-reactivity, and, importantly, direct neurotoxic effects of the dengue virus.5,9,15 Dengue infection leads to a wide range of manifestations from headache, fatigue, motor weakness, Guillain–Barre syndrome, seizures, meningitis, and encephalopathy to coma.7,8 Patients with dengue infection and its associated complications are reported to present with psychiatric disorders such as mood disorders, anxiety disorders, personality changes, and rapid cognitive decline. This narrative review focuses on the various psychiatric manifestations of dengue infection and its sequelae, possible mechanisms, and the management options to address the psychiatric symptoms. A note is also added on the effects of histone deacetylase (HDAC) enzyme with respect to the psychiatric sequelae and the novel HDAC inhibitors that are conceptualized to be neuroprotective.
Search Strategy
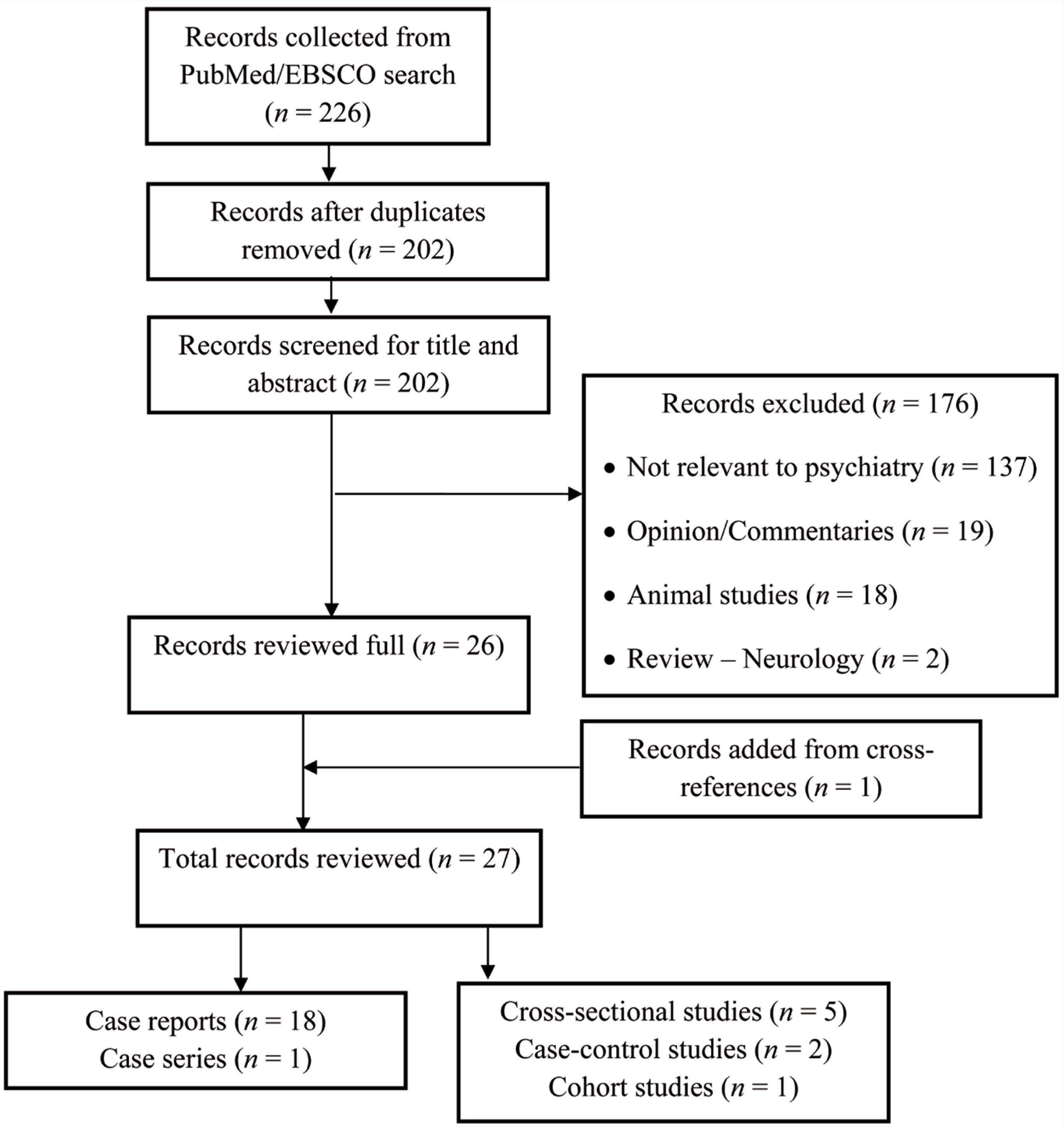
The authors (DD and VS) searched PubMed and EBSCO independently with the following search terms: “Dengue,” “Psychiatry,” “Psychosis,” “Mania,” “Catatonia,” “Schizophrenia,” “Depression,” “Bipolar,” “Anxiety,” “Obsessive-compulsive disorder,” “psychology,” “Neuropsychiatry,” “Dementia,” and “Histone deacetylase.” We identified 226 manuscripts. The search was restricted neither to languages nor time. Manuscripts (case reports, case series, and observational studies) describing the psychiatric manifestations, in all the age groups, during the acute and convalescent phases of dengue viral infection, and their management were included for the review. The outcome of the search strategy is depicted in Figure 1. The total number of unique manuscripts identified for the final review was 27. This included 18 case reports, one case series, and eight observational studies. A detailed review of the eight observational studies16–23 (five cross-sectional, two case-control, and one cohort study) is provided below and summarized in Table 1.
Outcome of the Literature Review
Psychiatric Manifestations in Dengue Infection
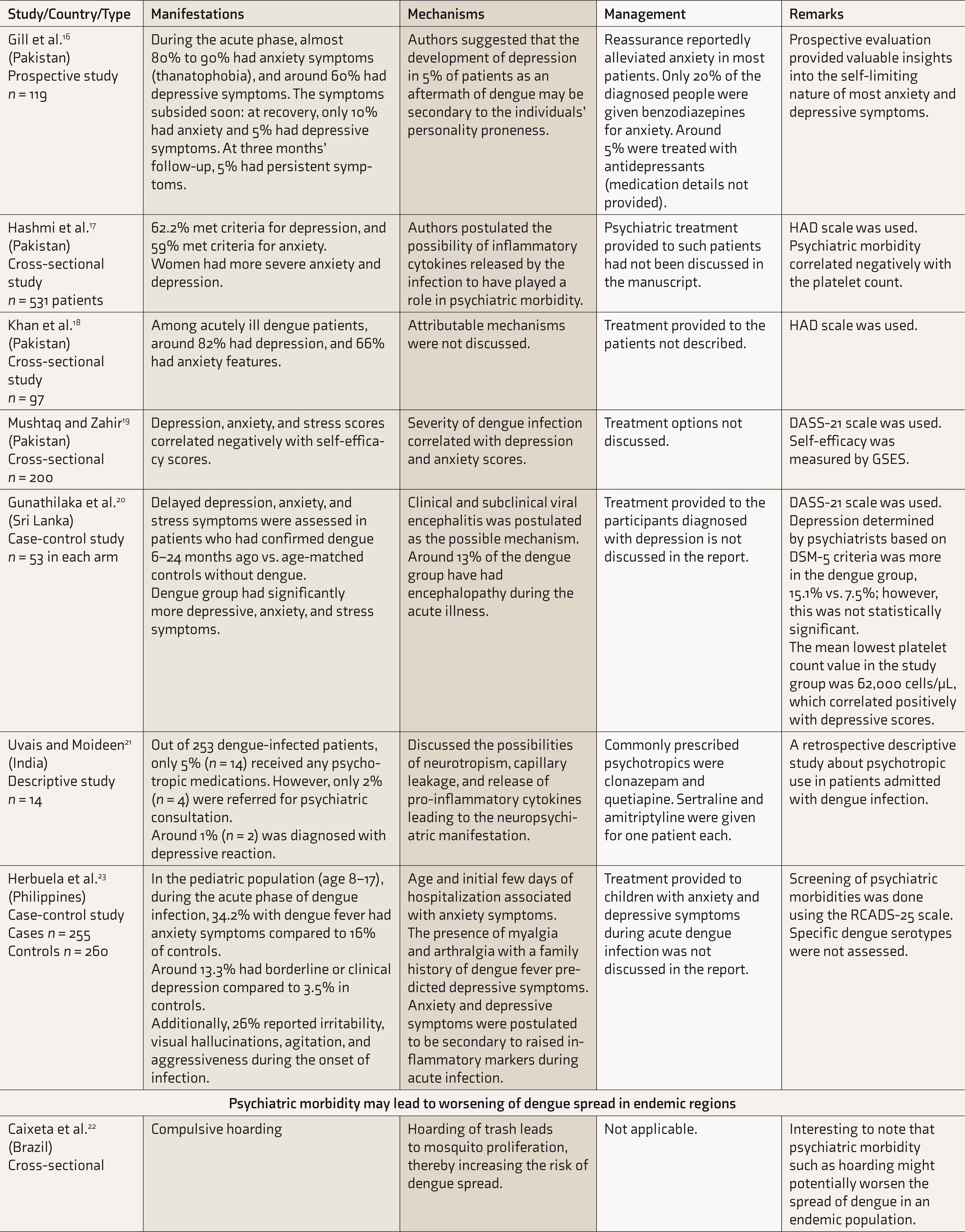
DASS, depression anxiety stress scale; DSM, diagnostic statistical manual; GSES, general self-efficacy scale; HAD, hospital anxiety and depression scale; RCADS-25, revised child anxiety and depression scale-25 items.
Psychiatric Manifestations
Most reported patients are from Asian countries or involved travelers returning from dengue-endemic regions. Depressive disorders were the most common psychiatric presentations. During the acute phase, most (60% to 90%) patients had both anxiety and depression symptoms,16,17 and syndromal depression was prevalent in 5% to 15% of patients in convalescence. 20 High rates (80% to 90%) of anxiety symptoms (thanatophobia) noted during the acute phase subsided during convalescence, and only 5% had persistent symptoms at three months’ follow-up.16,18 In another study, 62% and 59% met the criteria for depression and anxiety during the acute phase. Women had more severe depressive symptoms than men. 17 Severity of depression, anxiety, and stress correlated negatively with the self-efficacy scores during acute infection. 19 A case-control study involving pediatric population observed the prevalence of depression (13.3%) and anxiety symptoms (34.2%) during acute dengue infection to be significantly higher than matched controls. 23 Further, around 25% of the admitted children exhibited agitation, aggression, irritability, and visual hallucinations. Delayed psychiatric manifestations of dengue infection were reported to be predominantly depression and anxiety. At 6–24 months’ follow-up after dengue infection, the rates of depression were 15%. 20 There are multiple case reports of manic presentation,24–31 acute polymorphic psychosis,32–39 prolonged depression, 40 and catatonia29,41 and one on rapid cognitive decline. 42 However, the evidence for a psychotic, manic, or catatonic presentation from observational studies is lacking. It is also interesting to note that psychiatric presentations such as compulsive hoarding lead to the accumulation of trash, thereby endangering the proliferation of the Aedes mosquito and the increased spread of dengue. Such a possible relationship is observed in a cross-sectional study from Brazil. 22 Only a few studies used standard diagnostic criteria and structured psychopathology and cognition rating scales to quantify the presentation.17,18,25,26,29 Most studies had little/no information on follow-up details, and retrospective studies had suggested predominant anxiety and depressive symptoms as chronic consequences. However, the persistence of these symptoms and the need for prolonged treatment for secondary psychiatric manifestations are not specifically described in the available studies.16,20
Postulated Mechanisms
Although there was an argument that psychiatric presentations such as mania were mere coincidental findings during dengue fever,43,44 with a rising incidence of dengue infections and growing reports of such presentations in the existing literature, it is essential to review the probable postulated mechanisms underlying psychiatric morbidity in dengue. Available observational or longitudinal studies did not elicit the etiopathogenetic mechanisms underlying psychiatric manifestations. The mechanisms postulated are largely from case reports/series and hence are anecdotal.
Interestingly, only a few reported patients with psychiatric symptoms had additional neurological manifestations such as confusion, seizures, cognitive decline, delirium, and gait disturbances.36,39,42 Cerebrospinal fluid analysis showed increased protein levels and lymphocyte cells in two reports.36,39 But, the analysis was considered normal in the other two reports.27,42 Brain imaging studies such as computed tomography25–27,34,35,41 and magnetic resonance imaging32,33,36,38 in most reports were normal. Metabolic derangements, including elevated liver enzymes,24,25 electrolyte abnormalities, 27 vasculitis with capillary leak, and fluid extravasations, were postulated. 5 Platelet counts ranged from 20,000 to 2,00,000 cells/µL,24,35 and there were inconsistent correlations between platelet count and psychiatric morbidity.17,20 Only four studies reported the dengue virus serotypes. DENV-2 was identified in two reports,38,39 while DENV-1 40 and DENV-4 39 were associated in one report each. Direct neuronal invasion by the dengue virus was doubted for long but has been reported to be possible.26,28,45 Recently, the role of secondary immune activation and epigenetic modifications in dengue-related neuropsychiatric complications has been increasingly studied. 5 Encephalopathy alone was not the prerequisite to psychiatric presentations, and in fact, most patients exhibited clear sensorium during manic/psychotic breakdown, making a case for other etiological possibilities. 34 Further systematic studies are necessary in identifying the underlying mechanisms better.
Management Options
Management options for the primary dengue infection are beyond the scope of the current review, and detailed reviews on the topic are available.46–48 The supportive management for dengue fever primarily involves anti-inflammatory agents and corticosteroids. But, studies on psychiatric manifestations either completely neglected to report the management details of primary dengue infection17–20,23,38 or did not clearly specify the agents and the doses used.16,21 The literature exploring psychiatric manifestations in relation to these agents used to treat dengue is more important given the well-known association of some of them in precipitating behavioral and mood symptoms.
Only limited information is available about the management of secondary anxiety and depression symptoms. Most observational studies that aimed at understanding acute and delayed psychiatric morbidity in dengue patients did not report the treatment provided for the identified patients.17,19,20 Successful management of agoraphobic symptoms with oral sertraline (dose not available) 39 and prolonged depression with duloxetine (dose 40 mg/day) 40 was reported. Mania in dengue patients was managed with antipsychotic/benzodiazepines or a combination of mood stabilizers and antipsychotic/benzodiazepines.24,26–29 For psychotic presentations, a good response was achieved with oral antipsychotic agents, mostly in low doses.32–37,39 Catatonic presentation responded well to intravenous lorazepam 4 mg/day, which was tapered and stopped over four weeks. 41
It was noted that clonazepam and low-dose quetiapine were started for dengue patients with psychiatric comorbidity without an appropriate specialist referral. Only less than 2% of the patients with psychiatric morbidity were usually referred for formal assessment. 21 There is a lack of evidence on the preference of any specific psychotropics in managing psychiatric symptoms, and the chosen treatment seems to be in line with their conventional use in general psychiatric practice.
Histone Deacetylase (HDAC) Enzyme and Epigenetic Modifications
Histone proteins are implicated in organizing the DNA structure. Acetylation of histone proteins favors the binding of relevant transcription factors to the DNA. 49 Histone deacetylase (HDAC) removes histone acetylation and condense the chromatin, leading to a slowing of gene transcription.50,51 After the recruitment of HDAC by factors such as DNA methyltransferase (DNMT), the silencing of promoter genes is ensured through DNA methylation. 52 The inactivation of genes with increased HDAC and DNMT activity has been implicated in the manifestation of psychiatric conditions. 53
HDAC enzymes are classified into two families, four groups, and 18 isoforms (HDAC 1–11 and silent information regulator-2 related proteins 1–7).49,54 Virus-mediated gene transduction was shown to result in altered HDAC activity, impairing neuroplasticity and cognition. 55 Dengue infection, especially hemorrhagic fever, was reported to result in a “cytokine storm” characterized by elevated levels of circulating cytokines and chemokines. 5 Cytokine storm following dengue infection may lead to oxidative stress, which promotes the HDAC activity.56,57 (Inflammatory mechanisms were postulated in the etiopathogenesis of bipolar disorder in animal models. 58 HDAC overexpression in adult mouse hippocampus was reported to result in decreased prepulse inhibition. This aberration was described in both human and animal models of schizophrenia.59,60 Such epigenetic modifications play a crucial role in understanding the etiopathogenesis of most psychiatric disorders.)
Role of HDAC Inhibitors in Treatment
Numerous preclinical studies reported the antimanic effects of HDAC inhibitors. Valproate is a potent inhibitor of HDAC and has been used as a mood stabilizer for decades.49,61 Carbamazepine and topiramate are also reported to inhibit HDAC to some extent, while other antiepileptics such as levetiracetam, phenobarbitone, or gabapentin did not inhibit HDAC.62–64 The ability of lithium to inhibit HDAC has not been elucidated. 65 However, lithium plays a role in gene transcription regulation through glycogen synthase kinase-3 inhibition. 66
Interestingly, chronic exposure to second-generation antipsychotic drugs has been reported to result in overexpression of HDAC2 and thereby proposed to result in cognitive dysfunction.55,67 Quetiapine was shown to reduce DNMT, a close associate of HDAC, in the hippocampus and nucleus accumbens, thereby reducing DNA methylation in animal models and also promoting hippocampal neurogenesis.63,68,69 The HDAC/DNMT inhibitors reactivate the suppressed genes, which ultimately results in clinical improvement 53 (see Figure 2).
Inhibition of Class I and Class III HDACs was reported to promote antidepressant action of fluoxetine, while additional inhibition of Class II HDACs was required to promote anti-anxiety action of the molecule. 70 In animal models, high-frequency repetitive transcranial magnetic stimulation was reported to promote histone acetylation and gene expression. 71 Selective HDAC2 isoform inhibitors were reported to ameliorate cognitive deficits in animal models. 72
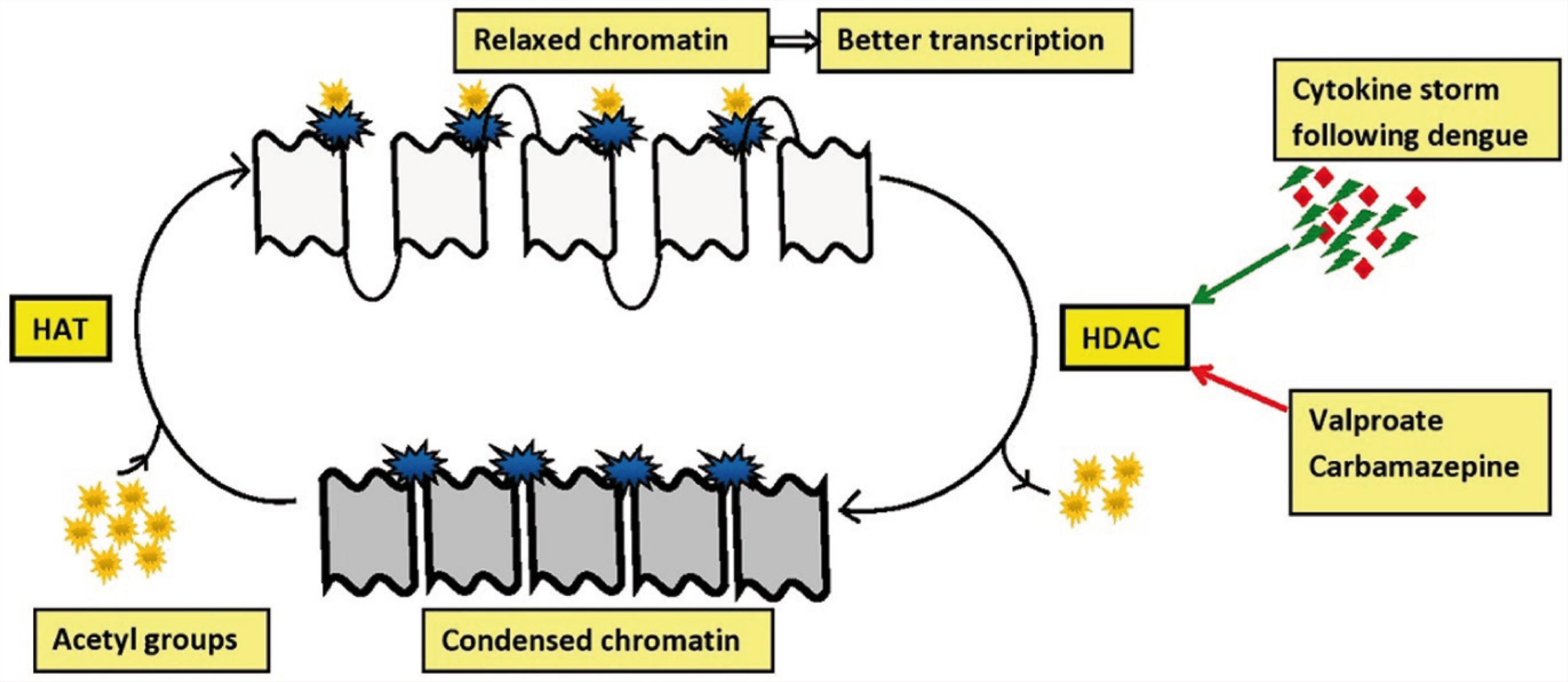
HDAC, histone deacetylase enzyme; HAT, histone acetyltransferase enzyme.
In our review, generally, the prognosis of psychiatric morbidity following dengue was good. Seven of the reviewed reports utilized any one agent (valproate, quetiapine, or carbamazepine) with HDAC/DNMT inhibition.24–29,31,34 These reports suggested an early and favorable outcome. However, reports utilizing other agents without HDAC/DNMT inhibition also suggested favorable outcomes. Clinicians are recommended to follow appropriate precautions while prescribing HDAC inhibitors such as valproate and carbamazepine to women in the childbearing age group because of high teratogenicity and other side effects. The role of HDAC inhibitors in treatment is limited, owing to the lack of specificity for selective HDAC isoforms and severe side effects such as teratogenicity, cytotoxicity, polycystic ovarian syndrome, etc.73,74
Conclusion and Future Directions
The dengue epidemic is on the rise for two decades. Neurological and especially psychiatric manifestations are increasingly reported in acute as well as convalescent phases of dengue infection. Frank psychiatric manifestations without neurological consequences are also reported, with mood disorders being the commonest. A cytokine storm unleashed by dengue infection potentially leads to significant neuropsychiatric manifestations. Proposed etiopathogenesis involves epigenetic mechanisms such as overexpression of HDAC enzymes. Mood stabilizers such as valproate and second-generation antipsychotics such as quetiapine and clozapine show inhibition of DNA methylation. These agents provide clinical scope and utility to manage post-dengue psychiatric manifestations. However, the specificity of HDAC class and isoforms associated with psychiatric symptoms needs further delineation. The development of HDAC isoform-specific inhibitors might improve the clinical application, with reduced side effects. The authors consider that the following steps are essential in improving the understanding of psychiatric manifestations and management of dengue infection.
Documentation of phenomenological psychiatric presentations.
Delineating neurological consequences (seizures, encephalitis, confusion, etc.).
Reporting the identified dengue serotype involved and other relevant immunological investigations.
Reporting the details of treatment provided and the response.
Following up for longitudinal consequences.
Systematic studies to evaluate the association and effectiveness of psychotropic agents that have properties of modulating specific epigenetic factors in dengue-related psychiatric disorders.
Despite reporting a significant proportion of dengue infections, longitudinal studies describing the neuropsychiatric manifestations and its management are a few from India. Multidisciplinary research is the need of the hour. Clinical suspicion regarding comorbid depression and anxiety, with an appropriate referral for psychiatric consultation, would ultimately result in better outcomes. Longitudinal studies are sparse and, whenever available, are with further limitations such as neuropsychiatric manifestations being assessed without standardized tools, inadequate attention paid to postulating possible mechanisms, and describing the treatment options used. The development and availability of vaccines to prevent dengue infection are in their early stages. Systematically designed prospective studies with the suggested steps might elucidate the pathogenesis of dengue-related psychiatric consequences and probably shed light on novel treatment options.
Footnotes
Acknowledgements
This work is supported by the Department of Science and Technology (Government of India) Research Grant (DST/SJF/LSA-02/2014-15) to GV.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.