
Abstract

Several antitubercular medications are known to cause neuropsychiatric adverse reactions (ADR), including delirium, depression, mania, psychosis, and seizure disorder.1–4 Neuropsychiatric ADR usually appears during the initiation of treatment or while changing from a previously prescribed regimen. The development of psychiatric ADR is rare during the continuation phase (CP), especially after a patient has been on a stable treatment regimen for several months.4–6 We herein report a case of antitubercular treatment (ATT) induced acute psychosis in a young female after 21 months of regular supervised treatment for extrapulmonary multidrug-resistant tuberculosis (MDR-TB).
Case Description
A 23-year-old unmarried female presented in January 2019 with a history of abrupt onset behavioral change for the last two days, characterized by suspiciousness, muttering-and-smiling to self, episodes of inappropriate laughter-and-cry, disturbed sleep, and diminished appetite. History also revealed “delusion of reference” and “delusion of persecution.” The patient was diagnosed with MDR tubercular chest wall abscess (right lower back) in May 2017 and was started on the MDR-ATT regimen. Since January 2018, she has been receiving standard treatment of CP, with tablet cycloserine 750 mg/day, ethionamide 750 mg/day, levofloxacin 750 mg/day, and ethambutol 1200 mg/day, as per the Revised National Tuberculosis Control Programme (RNTCP) regimen. 7
There was no history of fever, head trauma, loss of consciousness, substance use, or any medication overdose. There was no past or family history of any psychiatric illness. There was no history of acute life stressors. Treatment history did not reveal the use of any cytochrome P450 enzyme inhibitor drugs.
During the examination, the patient was oriented to time, place, and person. Pulse rate was 90/min, and blood pressure 128/88 mmHg. Other general and systemic examination findings were within normal limits.
Mental state examination revealed poor rapport, fearful affect, delusions of reference and persecution, impaired judgment, and absent insight. At the time of hospitalization, her Brief Psychiatric Rating Scale (BPRS) 8 score was 52.
Differential diagnoses of neurotuberculosis, immune-reconstitution-inflammatory syndrome (IRIS), and drug-induced psychosis were kept. After hospitalization, all ATT medications were withheld after pulmonary medicine consultation. The patient was started on T. risperidone 2 mg/day and T. lorazepam 2 mg/day. All blood investigations and neuroimaging were within normal limits (Table 1). Within 48 h, the patient started showing improvement, and within 4 days, she was completely free of her positive psychotic symptoms. Her BPRS score improved to 28. Risperidone was tapered and stopped on the seventh day. There was no recurrence of psychiatric symptoms, and the patient was discharged after 10 days. After 1 month, during her routine follow-up, she was maintaining well (BPRS score 19). Naranjo Adverse Drug Reaction Probability Scale 9 score of 6 suggested a probable association.
Discussion
Neuropsychiatric ADR of antitubercular drugs are not uncommon. 4 Psychiatric ADR pose an important challenge in the management of tuberculosis and significantly lower the quality of life of an individual on ATT. Isoniazid (first-line) and cycloserine (second-line) are the two most common anti-TB drugs associated with psychiatric ADR. However, ethambutol, ethionamide, and fluoroquinolones have also been reported to be associated with neuropsychiatric ADR.3,4,10 Several authors have suggested a higher initial dose of medication, hepatic insufficiency, extremes of age, and family history of psychosis as possible risk factors for developing drug-induced psychosis.3,6 The outcome of ATT-induced psychosis has varied from complete recovery to suicide.2,5
In this case, the patient was on cycloserine, levofloxacin, ethionamide, and ethambutol – all of which are reported to be associated with druginduced psychosis, but usually during an early course of the treatment.3–6 Yang et al. did a retrospective study on MDR-TB patients (N = 256) in South Korea and reported the incidence of psychiatric side effects to be 5.5%. After 6.5 months (on an average) of commencing ATT, cycloserine (one of the most common offending agent) was withdrawn in 3.9% of the patients . 4 However, the development of ATT-induced psychosis nearly 2 years after a continuous treatment is rare.5,6 It was, therefore, unique of this case to present with psychosis so late in the course of a stable ATT regimen (in the continuation phase).
A limitation of this report was that we did not obtain serum levels of individual ATT agents. Also, rechallenging with individual drugs was not possible because of ethical concerns. The consulting team of pulmonologists suggested discontinuing ATT, considering 21 months of supervised treatment, resolution of symptoms, and ultrasonographic findings. However, we were able to establish a temporal relationship as the discontinuation of ATT ameliorated the symptoms rapidly, and the improvement persisted even after stopping anti-psychotic medication (risperidone). Furthermore, in the absence of fever, delirium, electrolyte imbalance, neurotuberculosis, HIV, medication overdose, or substance use, the rapid onset and resolution of symptoms point toward drug (ATT) induced psychosis.
Reports suggest N-methyl-D-aspartate (NMDA) receptor antagonism, partial agonism at the NMDA receptor-associated glycine site, and gamma-aminobutyric acid receptor antagonism as possible mechanisms of ATT-induced psychosis. A combination of drugs with a similar mechanism (e.g., cycloserine, ethambutol, and levofloxacin) is more likely to exert an additive effect in the causation of ADR.1,3,6,10 The exact mechanism of delayed-onset ATT-induced psychosis and how it differs from acute onset psychosis need to be explored in future studies.
Investigation Findings
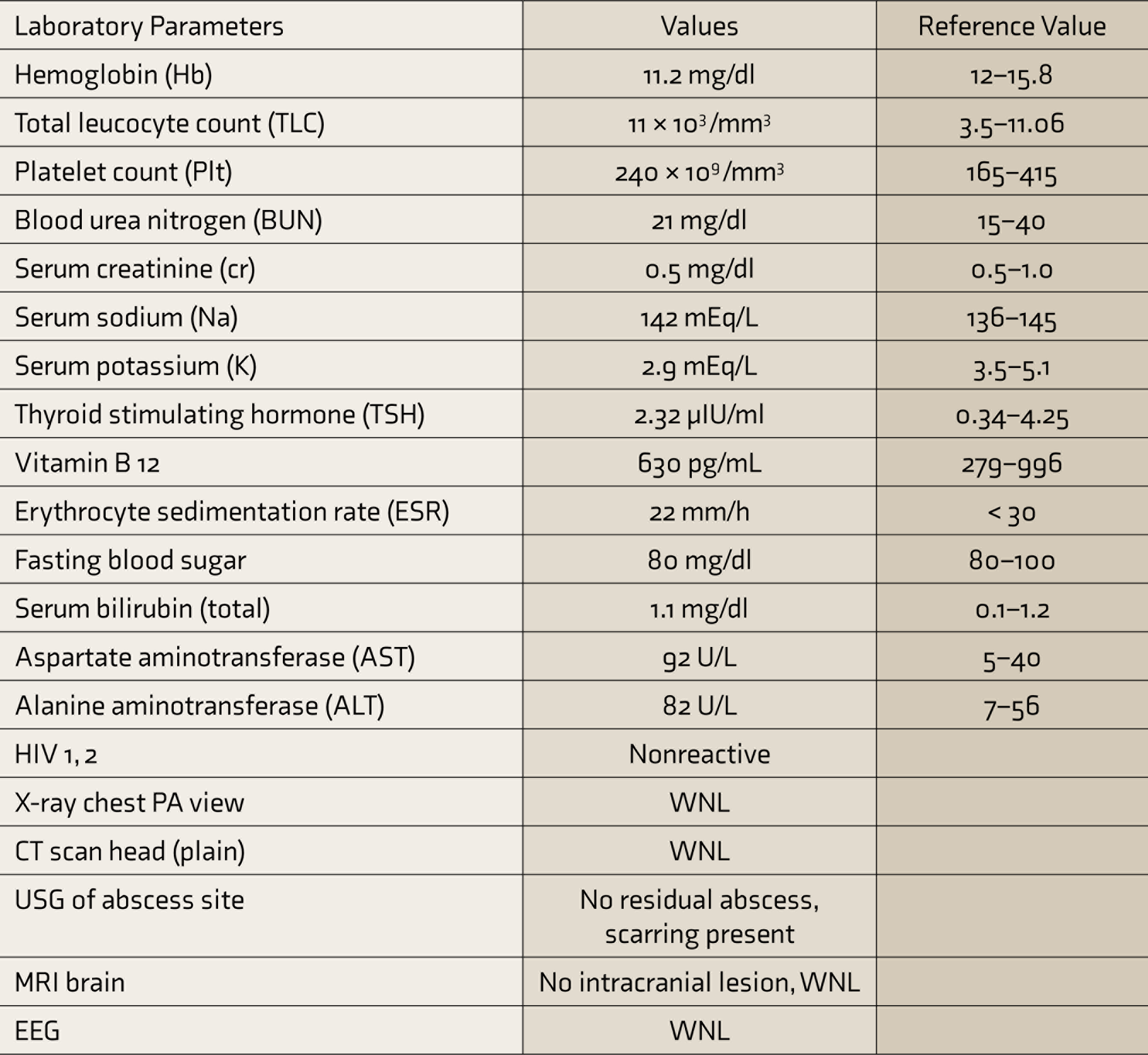
CT: computed tomography, EEG: electroencephalogram, HIV: human immunodeficiency virus, MRI: magnetic resonance imaging, PA: posterior–anterior, USG: ultrasonography, WNL: within normal limits.
To conclude, the current case highlights a relatively rare occurrence of late-onset ATT-induced psychosis that rapidly reversed on discontinuation of the drugs. We recommend that the clinicians should be watchful for psychiatric manifestations not only at the start of ATT but during the late course of treatment as well.
Footnotes
Acknowledgements
The authors would like to acknowledge the Department of Pulmonology and Department of Neurology for their expert opinion in managing the case.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed..
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.