
Abstract
Introduction:
Mental health issues are on an exponential rise in Kashmir due to varied reasons including political instability, eco fragility, the growing lag in the provision of education and employment, and several other reasons. Impediments such as the overwhelming stigma and the cultural sensitivity associated with mental health issues both sustain and perpetuate mental ill health and also prevent any treatment and rehabilitation. This article describes the protocol of a research project, funded by the Indian Council of Medical Research, which aims to address this issue.
Aim:
To screen the population for mental health issues and to provide community-based intervention for the identified cases also to train community health workers for sustainable mental health support.
Methods:
We will conduct a household survey using the Hopkins Symptom Checklist (HSCL-25) for the identification of the clients. A multi-stage random sampling shall be used to select the villages and the households from the marginalized communities. A sample of 500 respondents shall be screened using HSCL-25. Those who screen positive for mental health issues will be offered cognitive behavioral therapy (CBT) by a qualified clinical psychologist. The research will be able to address the diagnosis of depression and anxiety-related cases and the subsequent intervention. Additionally, we will utilize the facilitator’s manual for Mental Health Training Program for Community Health Workers to build sustainable mental health services in community settings.
Discussion:
The study shall present a roadmap focusing on the indispensability of a comprehensive community-based intervention on mental health utilizing a non-pharmacological method. Assessing and analyzing the dynamics of mental health illness first hand, the study shall move ahead to offer a culturally tailored counseling program at the community level. The study also aims to highlight the role of the indigenous human resource (community health workers) and how its participation leads to a more scientific and sustainable intervention for more effective results, with an increased level of awareness and sensitization in a conventional society like Kashmir.
This article describes the protocol of a research project funded by the Indian Council of Medical Research that aims to address mental health issues in Kashmir. The study will include a household survey to identify clients and need and will provide cognitive behavioral therapy by a clinical psychologist as well as to train Community Health Workers to build sustainable mental health services in community settings.Key Messages:
Mental health is a global concern with a wide range of complexity in terms of its causation, effects, perseverance, and modes of rehabilitation. Mental health is cardinal to human beings both in their individual as well as collective capacity because it is much more than simply the absence of psychological pathology. The World Health Organization (WHO) defines mental health as ‘a state of wellbeing in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and can make a contribution to his or her community. 1
The primary casualty in common mental disorders including (anxiety and depression) are cognition, emotions, feelings, and behavior. Therefore, a mental disorder is an illness that affects people’s emotions, thoughts, or behavior, which is out of keeping with their cultural beliefs and personality and produces a negative effect on their lives or the lives of their families. 2 Though there are various treatment modalities both pharmacological as well as non-pharmacological, their implementation in developing countries is problematic. 3 Due to reasons such as stigma, lack of accessible services, and lack of trained manpower, the treatment gap is huge and may be increasing. Kashmir is one such region, and traditional in nature, that suffers from a large treatment gap.
Kashmir has suffered from political disturbances since 1947, including a series of wars and an ongoing insurgency. Apart from the past episodes of extreme and escalating violence, it has experienced even more in recent years. The ramifications of the political instability in Kashmir have not merely been direct in nature, that is, the casualties in the form of the lives lost, but indirect as well. For example, unemployment has risen overwhelmingly making it the most unemployed state across the whole of India. 4 Lack of private investment has multiplied the economic miseries of the people. Frequent protests and hartals (strikes) have not helped the cause either. Beyond the economic dimension, political instability significantly and adversely affects the education system of the whole valley. Besides the political instability, Kashmir witnessed a series of environmental disasters due to its greater eco-fragility: a massive earthquake in 2005, a massive snowstorm in the same year, and the unprecedented floods of 2014. The unexpected snowfall of November 7, 2019, led to a loss of approximately Rs. 2300 crores to the horticultural sector across the southern and northern districts of the valley. 5 As a result of these community traumas, the sociocultural support system has fractured and rapidly declined.
These and other disasters led to a traumatized population across all the districts of the valley. As per the reports of the Kashmir Mental Health Survey, “nearly 1.8 million adults (45% of the adult population) in the Kashmir Valley experience symptoms of mental distress, with 41% exhibiting signs of probable depression, 26% probable anxiety, and 19% probable Post-Traumatic Stress Disorder (PTSD).” 4 The experience of the individual level trauma has transcended beyond into the greater collective. Society in general has been traumatized and the trauma happens to pass through generations, a phenomenon called transgenerational trauma. 6 On average, “an adult living in Kashmir Valley has witnessed or experienced 7.7 traumatic events during his/her lifetime.” Exposure to multiple traumatic events is positively associated with mental ill-health, more specifically anxiety and depression, reported in several studies.
Syed Amin’s 2009 study reported depression to be the major psychological morbidity in Kashmir, with the clinicians prescribing more antidepressant medications now than in the past. 7 A study conducted by the Médecins Sans Frontières (MSF) reported that one out of every two adults is mentally disturbed in Kashmir Valley; the report said that depression is the most prevalent disorder in the valley with 41% adults showing its symptoms. 8 “Nearly 1 in 5 adults (19%) in the Kashmir Valley are living with significant PTSD symptoms, representing 771,000 individuals. 9 Besides, women experience greater psychological morbidity than males.” 9 The number of suicide cases also increased in the valley. 3
Despite a multifold increase in mental symptoms of mental ill-health, not much attention is being paid to expand and modernize the present mental health infrastructure. 7 The only psychiatric hospital in the valley has seen a tremendous increase in the inflow of the patients in the past two decades and is in no way sufficient to meet the need and demand of the ever-growing cases of mental health. Under such conditions, there is an urgent need for the mental health services at the micro, meso, and macro levels. Unfortunately, the District Mental Health Program is still in its infancy in the region. Given the high magnitude of the mental health issues, lack of both pharmacological as well as nonpharmacological interventions, and inadequate community-based intervention, there is an urgent need to address this serious problem.
Therefore, the present project aims to intervene at the community level by providing counseling services to a selected area where a community counseling center will be established and by imparting mental health training to the community health workers. Kashmiri society in general does not prefer counseling services nor are they easily available. Therefore, there is an urgent need to train community health workers and general physicians on the detection and the treatment available for mental ill-health.
Objectives
Following are the objectives of the study:
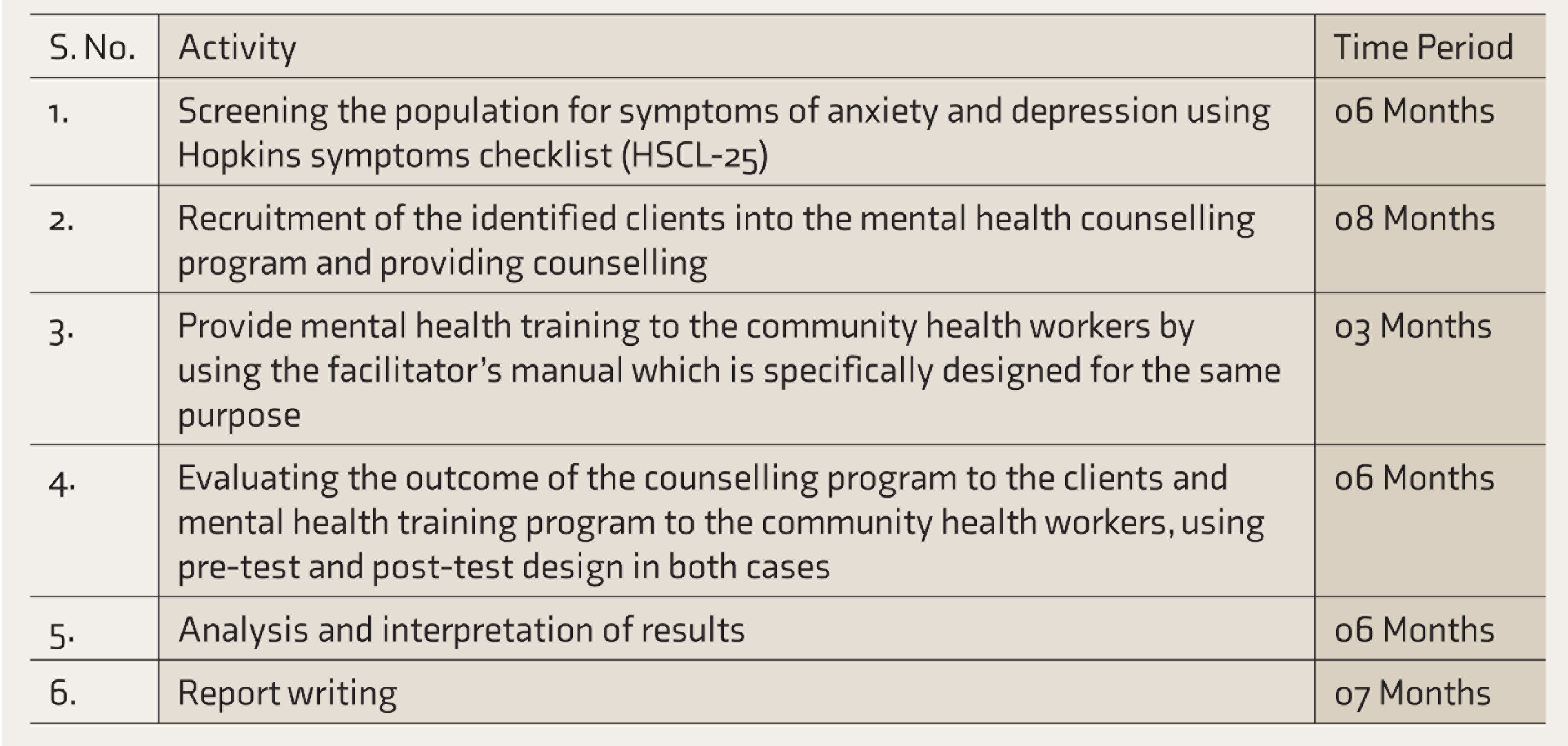
To screen the population for the symptoms of anxiety and depression using the Hopkins Symptom Checklist (HSCL-25). To admit the identified clients into the counseling program. To provide mental health training to the community health workers by using the facilitator’s manual which is specifically designed for the same purpose. To evaluate the outcome of the counseling program and mental health training program using pre-test–post-test design.
Research Design (Intervening Modalities)
The project will be implemented in the following phases.
Phase I: Identification of clients with anxiety and depression.
Phase II: Recruitment of clients for cognitive behavioral therapy (CBT).
Phase III: Imparting CBT.
Phase IV: Training and educating the community-based health workers.
Phase V: Evaluation.
Phase VI: Referral and registration. Refer to Table 1.
Place of Intervention
District Budgam shall be the area of intervention. The total population of the district is approximately 753,745 (Census 2011) with a sex ratio of 833/1000. 10 It is the second most dominant Shia district after Kargil. Even though geographically close to the city, it lacks in many developmental areas. Budgam is known for its great historical legacy and rich heritage in terms of both infrastructures as well as religion. It was chosen for the study due to the significant prevalence of mental health issues. As per the study conducted by MSF in 2015, district Budgam has the second highest prevalence of mental distress of all the districts. 7 Furthermore, depression is much higher in rural areas (84.73%) as compared to urban areas (15.26%) with Budgam being a predominantly rural district. 7 In terms of the prevalence of anxiety and depression, “the proportion of the population in Budgam suffering from symptoms of probable depression in 2015 was 54%, representing 210,000 adults. 7 The proportion showing signs of a probable anxiety disorder was 36%, representing 75,000 adults.” District Budgam has a significantly higher proportion of women (66%) who were classified with a probable mental disorder compared to men (55%). 4
Activity Timeline
Materials and Methods
Study Design
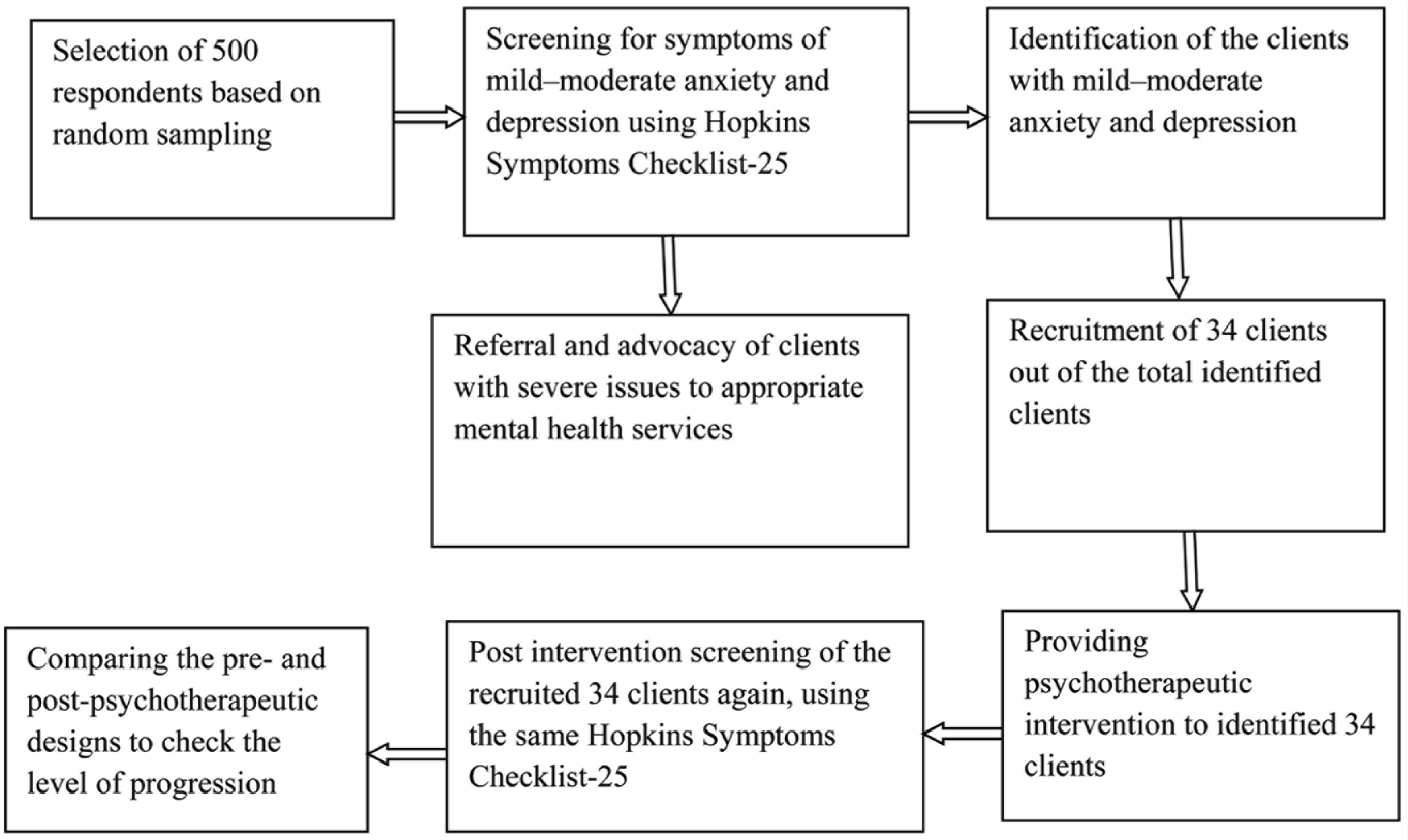
This study aims to evaluate the outcome of a culturally tailored eclectic counseling approach in reducing the symptoms of depression and anxiety in a community counseling center which is to be established in the Budgam area of Kashmir (the selection of the area is based on reports of a high prevalence of mental disorders as documented by MSF report, 2015); it also aims to evaluate the outcome of a 5-day long Mental Health Training Program for the community health workers. Both evaluations will be done by using a pre-test and post-test design. For documenting the outcome of the counseling module, the HSCL-25 will be administered to the counselees before and after the counseling program; and for evaluating the outcome of a mental health training program for the community health workers, the Mental Health Literacy (MHL) assessment will be administered to the trainees before and after the training. The design of the study is illustrated in Figure 1.
Sample Size and Selection
A mixed-methods design will be adopted including a household survey and focused group discussion. We will randomly select 10 villages/towns of the district Budgam, corresponding to economically marginalized areas having a lower economic index. Probability sampling shall be used to randomly select respondents; we estimate that it is feasible to select 500 respondents based on approachability and availability of the select population. The respondents will be interviewed about their daily life routines, personal as well as professional life, the family composition and economic background, and will be screened for depression and anxiety using HSCL-25. Out of the 500 respondents, consenting clients who have mild–moderate anxiety and depression will be asked to participate in the next phase. The final number of clients to be recruited into the counseling program for final intervention shall be calculated/determined by using McNemar’s Test (approximately 34). These clients will be the individuals screened for anxiety and depression from the general population in the selected area. Likewise, to select an appropriate sample size for evaluating the outcome of a mental health training program for the community health workers, the effect size was taken to be as 0.5, with alpha to be 0.05, and the statistical power to be 0.9, with a repeated-measures t-test; with these figures, the total of 44 community health workers will be selected from the list of health workers that will be obtained from the office of the Director of Health Services Kashmir and Director of Social Welfare.
Study Design
Scales/Tools to Be Used
HSCL-25 11
HSCL-25 is a symptom inventory that measures the symptoms of anxiety and depression. It consists of 25 items: Part I of the HSCL-25 has 10 items for anxiety symptoms; Part II has 15 items for depression symptoms. The scale for each question includes four categories of responses “Not at all,” “A little,” “Quite a bit,” “Extremely” rated 1 to 4, respectively. Two scores are calculated; the total score is the average of all 25 items, while the depression score is the average of the 15 items. It has been consistently shown in several populations that the total score is highly correlated with the severe emotional distress of unspecified diagnosis and the depression score is correlated with major depression as defined by DSM-IV which is evidence for the scale’s external criterion validity.
Mental Health Literacy (MHL) Survey
MHL is a tool to assess the ability to recognize the mental disorders, to prevent mental disorders, to assess the knowledge about the risk factors or causes of mental disorders, to assess knowledge and beliefs about the self-help interventions, and to assess the knowledge and beliefs about the effectiveness of professional treatment available. This tool has been used in India and Australia.
Facilitator’s manual for Mental Health Training Program For Community Health Workers:
This manual which will be used to train the community health workers consists of four segments: (a) An introduction to mental health and disorders; (b) Mental health first aid; (c) Practice-based skills, and (d) Mental health promotion.
Evaluation
For achieving the objectives of evaluating the outcomes of the counselling program in reducing the symptoms of depression and anxiety, the HSCL-25 will be administered to the screened clients who showed the symptoms of anxiety and depression and their respective scores will be recorded. Thereafter, the identified persons will be admitted to the CBT counseling program of 6-8 sessions. Then these individuals will again be tested by using the same test—HSCL-25, and their respective scores will be recorded. Then each individual’s score on HSCL-25 before the counseling program and after it will be compared. For this purpose, a statistical test, namely, repeated measures t-test will be used. We hypothesize that the CBT intervention will result in significant improvements in postcounseling program scores and precounseling program scores.
Likewise, for evaluating the outcome of a 5-day long Mental Health Training Program for the community health workers, the MHL Survey will be administered on the selected community health workers before their induction into the mental health training program; their respective scores on MHL will be recorded. Then these health workers will be given a 5-day long mental health training. After the training they will again be tested using MHL, then their respective scores on the second administration will also be recorded. Then the scores on the first and second administration will be compared again by using a statistical tool that fits the format of MHL.
Ethics Approval and Information Dissemination
The project has been approved by the Institutional Ethics Committee for the conduct of study. The principle of confidentiality and controlled emotions, non-judgmental attitude will constitute the fundamental components of any intervention. Strict data insulation will be followed in letter and spirit. Findings and the results derived during the course of the whole project will be disseminated through various professional, public as well as private platforms including conferences, seminars, workshops, journals, etc. All options to share the results with institutions that work at policy levels are an imperative priority.
Project Team and Training
Before officially starting the actual data collection (i.e., identification of clients for the symptoms of mild–moderate anxiety and depression), the research team (one senior and two junior research fellows) will practice the use of such tools and techniques under guidance from the principal investigator. All the researchers/fellows shall be trained in psychological first aid as well to professionally and scientifically manage the persons with extreme distress if they come across any such case while screening the clients from the field.
Tentative Results/Findings
The community-based intervention approach is the cardinal paradigm not only for comprehensively understanding the first-hand dynamics about the causality of mental health illness but also for the establishment of a more effective and integrated formulation and implementation mechanisms for mental health services, thereby addressing all the mental health disparities and asymmetries. There are challenges in various phases of intervention, but this approach is the best possible outreach of mental health services into diverse communities that have no or very little access to mental health services.
The community-based intervention leads to an increase in the relevance and outreach of the public health impact of mental health services due to the inclusive participation of the indigenous populace. Such intervention also leads to the mitigation of social stigma associated with mental distress and is also the best intervention in communities with the poor economic condition.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This protocol paper describes the methodology of a research project funded under ‘Capacity Building Task Force for Mental Health Research in India’ funded by the Indian Council of Medical Research vide file number 5/4-4/151/M/2017/NCD-1. International mentors were funded by the training program 'Cross Fertilized Research Training for New Investigators in India and Egypt' funded by FIC, NIH (No. D43 TW009114).