
Abstract
Background:
Well-being and locus of control have been important areas of research over the last few years. However, limited information is available about the same from India, due to the lack of validated instruments in regional languages for the same.This research aimed to translate, adapt, and validate the Warwick-Edinburgh Mental Well-being Scale (WEMWBS), Spiritual Well-being Scale (SWBS), and Multidimensional Health Locus of Control (MHLC) Scale in Hindi.
Methods:
The scales were translated into Hindi by following the translation–back-translation methodology as specified by the World Health Organization. Next, the Hindi versions of the scales were completed by 102 participants, and then, the participants completed either the Hindi or the English version of the scales after 3–7 days.
Results:
The Hindi versions of WEMWBS, MHLC, and SWBS have high cross-language equivalence with the English version of the scale, both at the level of the individual items and the various dimensions in all three scales, which was significant (P < 0.001). Cronbach’s alpha for the Hindi version of WEMWBS, SWBS, and MHLC scales was 0.92, 0.83, and 0.77, respectively. The Spearman–Brown coefficient was 0.82, 0.63, and 0.63 for WEMWBS, SWBS, and MHLC, respectively. As measured on the Centrality of Religiosity Scale (CRS), higher religiosity was associated with greater religious and existential well-being.
Conclusion:
The Hindi versions of WEMWBS, SWBS, and MHLC have good cross-language equivalence, internal consistency, and test–retest reliability. It is expected that these validated scales will stimulate more research in this area, focusing on evaluating the association of clinical parameters along with well-being and locus of control.
The Hindi versions of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS), Spiritual Well-being Scale (SWBS), and Multidimensional Health Locus of Control (MHLC) Scale have good cross-language equivalence with the English version. The test–retest reliability of all the three scales is high. Cronbach’s alpha for the Hindi version of all the three scales is 0.92, 0.83, and 0.76 for WEMWBS, SWBS, and MHLC, respectively.Key Messages:
Many efforts have been made to define subjective well-being (SWB). Diener et al. 2 defined it as “a person’s cognitive and affective evaluations of his or her life.” It is considered to have three components, that is, life satisfaction, positive effect, and negative effect. 3 A person is considered to have positive SWB if they have high positive effect and life satisfaction, with low negative effect. On the other hand, if the person experiences a low level of happiness, has little satisfaction with life, and experiences a high level of negative emotions such as anger, anxiety, and low mood, they are considered to have negative SWB. 4 However, experts have emphasized that high SWB should not be considered as synonymous with mental and psychological health, as the absence of psychopathology is not an indicator of positive SWB 5 and a person with mental illness can have positive SWB in the presence of psychopathology. 5
In terms of various determinants of SWB, literature suggests that positive SWB is associated with positive mental health, positive relationships, certain personality and temperament traits, good social relations, genetic factors, environmental factors, employment, marriage, age, culture, etc. 6
Besides SWB, researchers have also described the concept of spiritual well-being and described it to have two components, that is, religious well-being (RWB) and existential well-being (EWB). The RWB evaluates one’s relationship with God, while the EWB evaluates one’s sense of life purpose and life satisfaction.7, 8
The concept of locus of control refers to the person’s belief about the extent to which they have control over things that happen to them. The two overarching domains of locus of control include internal and external locus of control. An additional component of locus of control, which has been described/defined in some of the scales, includes “chance factors.” 9
Research on the concept of SWB is lacking, and there is limited research on the locus of control in the Indian context.10, 11 When someone looks at the concept of SWB in the Indian context, it can be said that how people interpret their health and the factors they attribute their health status to are very important. In India, many patients with physical and psychological illnesses attribute their illness to fate, karma, black magic, etc.12–15 Hence, there is a need to understand the determinants of SWB in the Indian context.
One of the major reasons for lack of research from India may be the unavailability of validated scales for assessment of these concepts in the Indian context. Accordingly, this research focused to translate, adapt, and validate the WEMWBS, SWBS, and Multidimensional Health Locus of Control (MHLC) Scale in Hindi. An additional focus of this investigation was to evaluate the association of SWB, spiritual well-being, and locus of control with the level of religiosity, assessed by using the Centrality of Religiosity Scale (CRS).
Materials and Methods
This study was conducted at a tertiary care centre, after due approval from the Institutional Ethics Committee. A cross-sectional study design was followed, and the study included 102 participants selected by convenient sampling. The study participants were enrolled during the period of April 2017 after seeking their written informed consent. They included healthy subjects who agreed to complete the different versions (Hindi/English) of the scales on two occasions within a span of 3–7 days.
Only those subjects who reported to be free from any diagnosed mental illness and any diagnosed chronic physical disease were included.
The sample size was calculated based upon the longest scale (SWBS), which consists of 20 items. Although a factor analysis was not carried out, a sample size of five times the number of items in the scale with the highest number of items was considered.
The instruments that were translated and adapted were the WEMWBS, SWBS, and the Multi-Dimensional Health Locus of Control Scale. Additionally, the CRS, which has been validated in India 16 was used for evaluating concurrent validity.
Process of Translation and Adaptation
Translation of the scales was done by mental health professionals with proficiency in both the languages, that is, Hindi and English, as per the methodology suggested by the World Health Organization. 19 Initially, each of these scales was translated to Hindi by three mental health professionals. Then these were reviewed by another panel of three mental health professionals, who compared the three available Hindi versions and the English version of the scales. During the process of review of the Hindi versions, the translation that retained the original meaning and was able to express the meaning in the simplest way, was retained. If the experts felt that the translations did not meet the required criteria, they gave their inputs and translated the item. The items that required adaptation, in view of the Indian culture, were suitably modified. During the process of translation, an effort was made to keep the language simple, without changing the meaning of the “stem/item” of the scales. Additionally, an effort was made to address the issues related to semantics and cultural factors. Based on these inputs, a draft Hindi version of the scale was developed. The draft Hindi version was given to 10 healthcare workers, five patients with mental illnesses, and five of their caregivers, who were proficient in Hindi, to evaluate the language and cultural appropriateness and to give suggestions to improve the scale further. These inputs helped to refine the Hindi translation further. This Hindi version was back-translated to English by bilingual mental health professionals who were not familiar with these scales. The back-translations were compared with the original English version in terms of the meaning conveyed. The back-translated versions were also sent to the authors of the original scales for their view. Based on all the inputs, if any of the items was not appropriate, the Hindi translation was further modified and a final version was developed.
Process of Evaluation of Psychometric Properties
First, the Hindi version, so developed, was handed over to 102 healthy subjects selected by convenient sampling. They were requested to answer the questionnaires as per the requirement. The participants were again approached after a time frame of 4–7 days, and they were asked to complete either the Hindi version again (n = 61) or the English version (n = 41) of all three scales.
Statistical Analysis
Statistical Package for the Social Sciences, 20th version (SPSS-20, IBM) was used to analyse the data. Simple descriptive statistics involved the calculation of mean and standard deviation for continuous variables and frequency along with percentages for the categorical variables. Cronbach’s alpha was used to assess the internal consistency of the Hindi version of the scales and the Spearman–Brown coefficient was used to estimate the split-half reliability of the Hindi versions of the scale. Test–retest reliability of the Hindi–Hindi version and cross-language agreement between Hindi–English versions were assessed by using the intraclass correlation coefficient (ICC) and Pearson’s correlation coefficient.
Results
The study sample comprised 102 participants, with a mean age of 33 (SD: 8.49) years and mean duration of education of 15.1 (SD: 2.72) years. There was nearly equal representation of males (51%) and females (49%). The majority of the participants were married (61.8%), from nuclear families (56.9%), and urban locality (92.2%). In terms of religion, 55.9% were Hindus, 37.3% were Sikhs, and small proportions were following Islam (3.9%) and Christianity (2.9%).
Psychometric Properties
Concurrence Between Hindi and English Versions
As shown in
Psychometric Properties of the Warwick-Edinburgh Mental Well-Being Scale
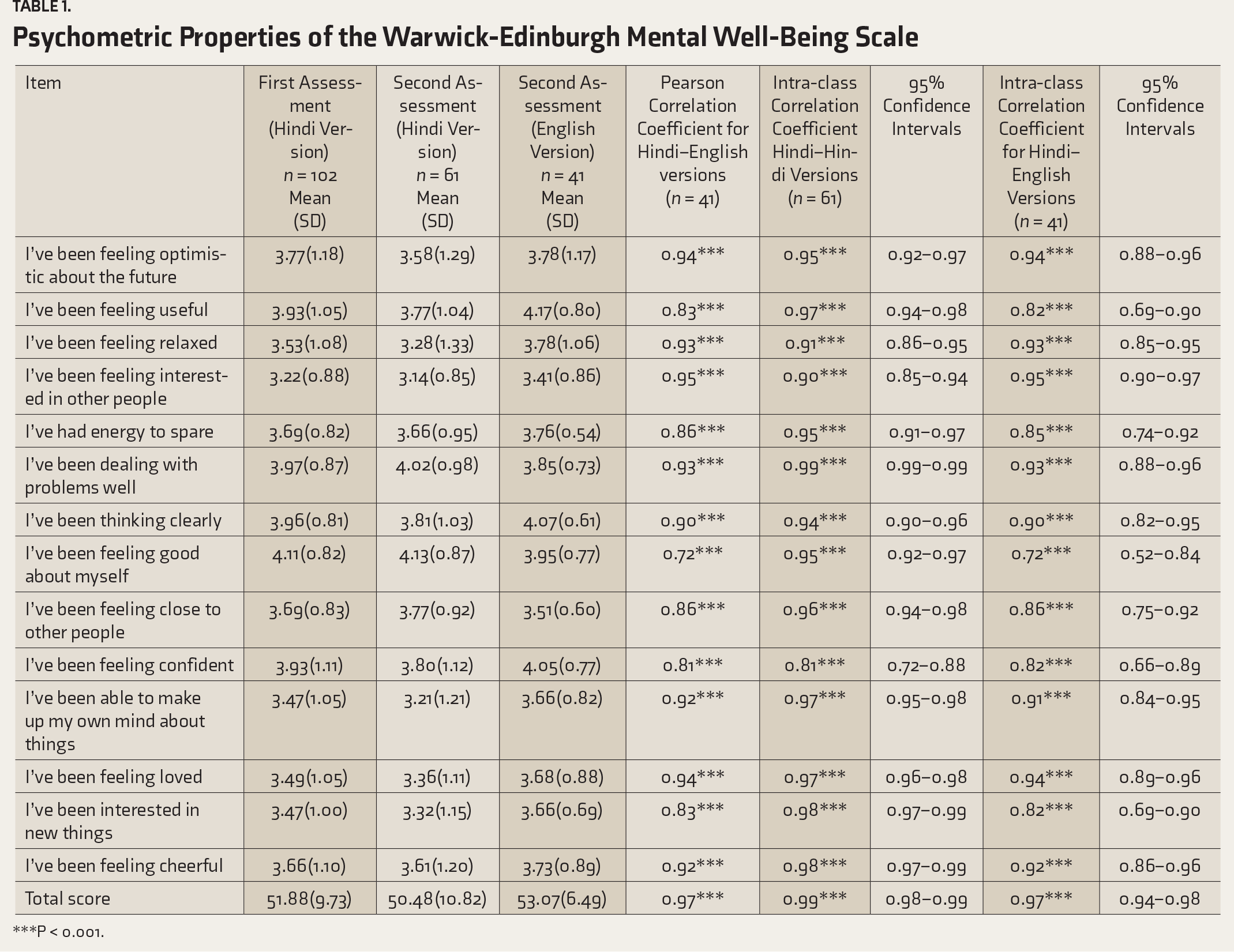
***P < 0.001.
Psychometric Properties of Spiritual Well-being Scale
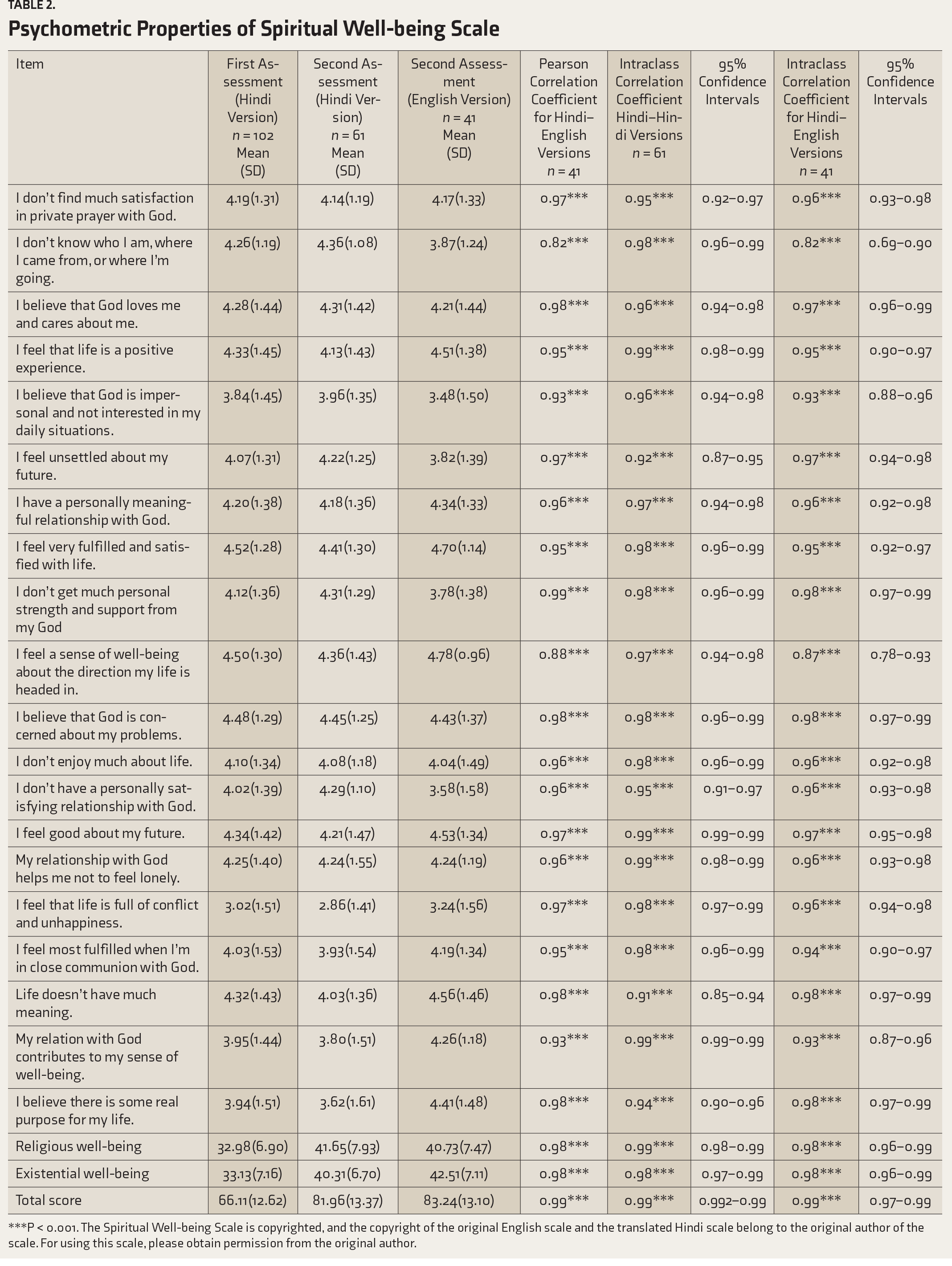
***P < 0.001. The Spiritual Well-being Scale is copyrighted, and the copyright of the original English scale and the translated Hindi scale belong to the original author of the scale. For using this scale, please obtain permission from the original author.
Psychometric Properties of Multi-Dimensional Health Locus of Control Scale
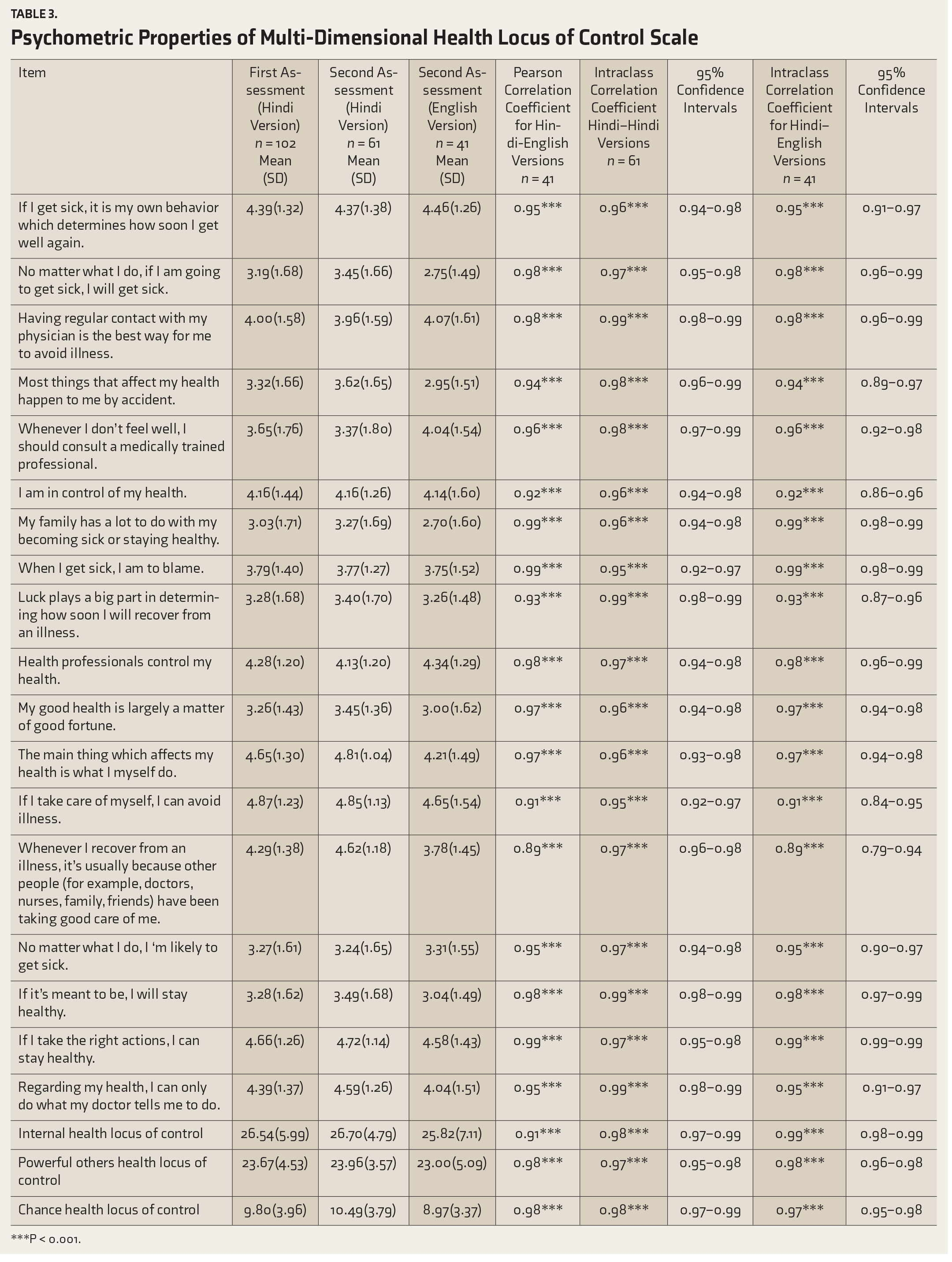
***P < 0.001.
Test–Retest Reliability
In terms of test–retest reliability for the total score for the Hindi version, ICC value for WEMWBS was 0.995 (P < 0.001), SWBS was 0.946 (P < 0.001) and that for three domains of MHLC were 0.969–0.984 (P < 0.001). Similar ICC values were also noted for the individual items of the scales (
Internal Consistency and Split-Half Reliability
The internal consistency of the Hindi version was assessed using Cronbach’s alpha. As evident from
Internal Consistency and Split Half Reliability of the Scales
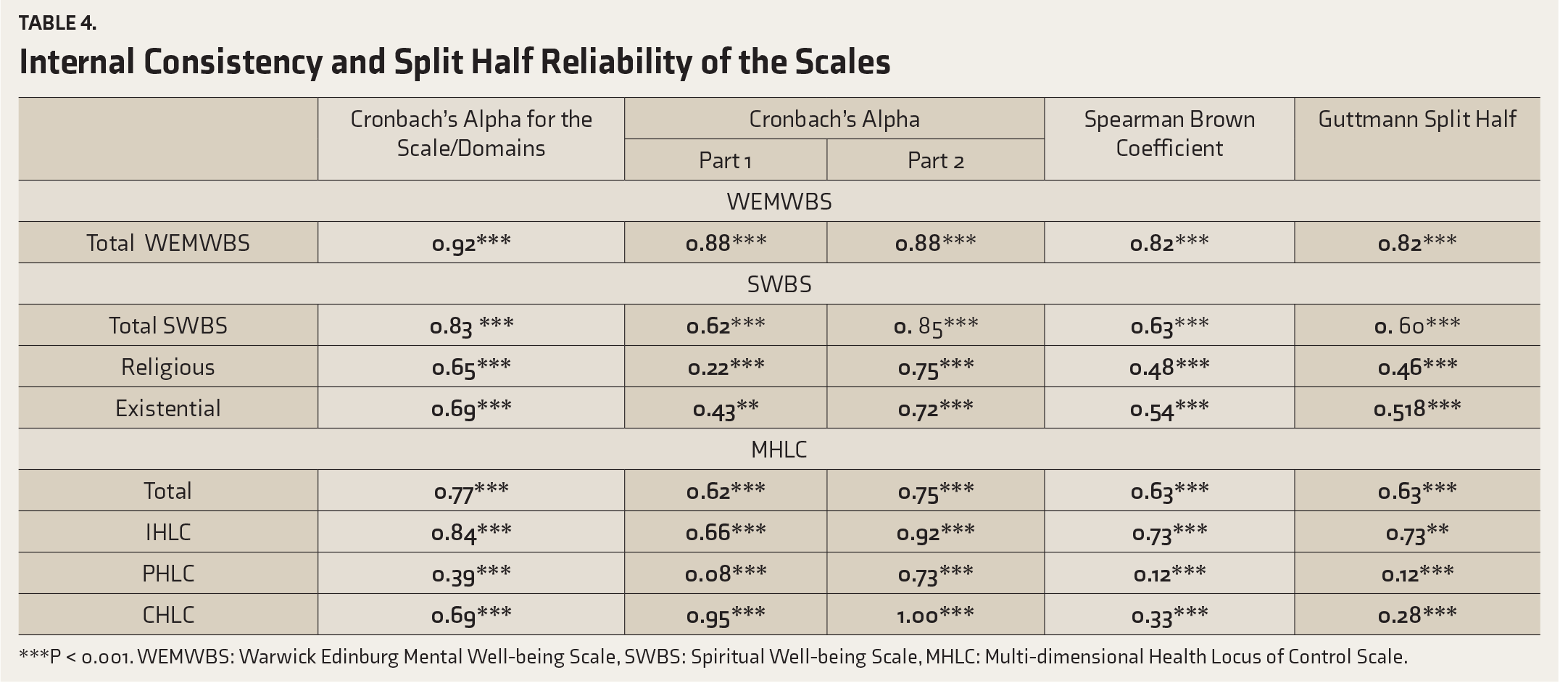
***P < 0.001. WEMWBS: Warwick Edinburg Mental Well-being Scale, SWBS: Spiritual Well-being Scale, MHLC: Multi-dimensional Health Locus of Control Scale.
The split-half reliability for WEMWBS, as assessed by the Spearman–Brown coefficient and Guttmann split-half value, was high (0.82). The split-half reliability for MHLC and SWBS total scores were 0.63 for both the scales (
Correlation between WEMWBS, MHLC, SWBS, and CRS
A higher level of religiosity as assessed by CRS was associated with significantly better well-being as assessed by WEMWBS, RWBS, total score of SWBS scale, and lower chance health locus of control. WEMWBS also had a significant positive correlation with the SWBS and internal locus of control, and negative correlation with chance health locus of control. Both the subscales of SWBS had a significant correlation with each other (
Correlations of Different Scales and with Centrality Religiosity Scale
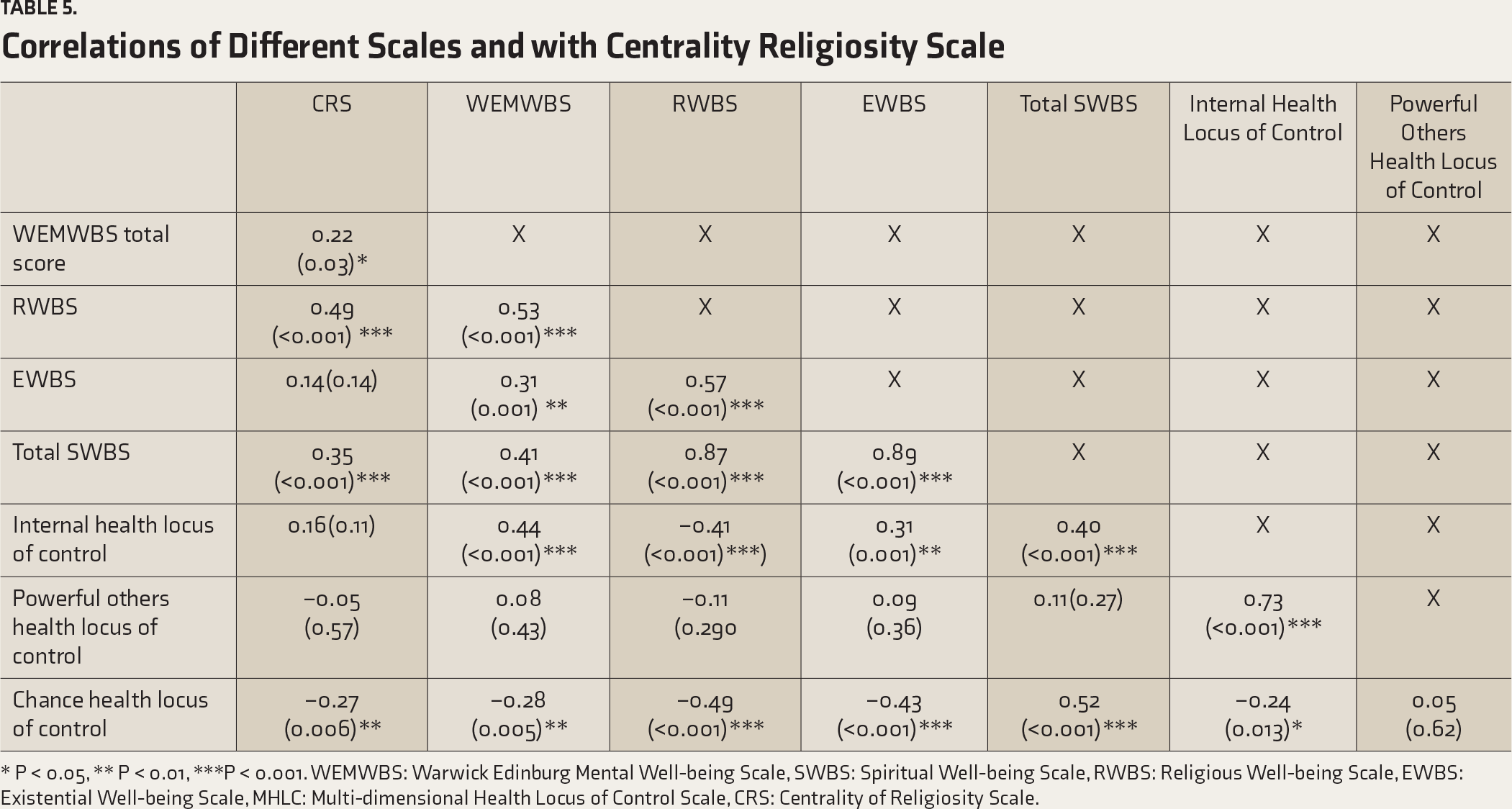
* P < 0.05, ** P < 0.01, ***P < 0.001. WEMWBS: Warwick Edinburg Mental Well-being Scale, SWBS: Spiritual Well-being Scale, RWBS: Religious Well-being Scale, EWBS: Existential Well-being Scale, MHLC: Multi-dimensional Health Locus of Control Scale, CRS: Centrality of Religiosity Scale.
Discussion
This study attempted to translate and validate the Hindi versions of scales for assessment of well-being and locus of control in a group of people not known to be diagnosed with any mental illness. Additionally, an effort was made to evaluate the association of well-being and locus of control with the level of religiosity. We chose to validate these three scales together because two of these evaluate different aspects of well-being, and the third scale, that is, MHLC, evaluates the locus of control, which can influence the persons’ attitude towards health, illness, well-being, and help-seeking.
We found that the Hindi versions of the WEMWBS, SWBS, and MHLC have an adequate level of psychometric properties in terms of internal consistency, test–retest reliability, and cross-language concurrence with the English version of the scale. The high Pearson correlation coefficient values and ICC between various items of the Hindi and English versions of the scale provide evidence for the cross-language equivalence of various items.
In terms of test–retest reliability, the ICC values for WEMWBS, SWBS, and MHLC total score and various domains of MHLC were more than 0.94, suggesting good to excellent test–retest reliability. For each item of various scales, the test-retest reliability was also very high.
Internal consistency of the various scales, as assessed by Cronbach’s alpha, was ≥0.8 for the total scores, and hence, excellent. However, when the internal consistency was evaluated for various subscales of the scales, it was seen that the Cronbach’s alpha was 0.651 (P < 0.001) for the RWBS and 0.697 (P < 0.001) for the EWBS, which are in the acceptable range. For the MHLC scale, the Cronbach’s alpha for the internal control domain was 0.845, suggestive of good internal consistency, whereas for the chance factor domain, it was very close to 0.7, indicative of an acceptable level of internal consistency. However, for the domain of powerful others, the internal consistency was 0.39, which can be considered as an unacceptable level. The split-half reliability of all the full scales was also in good to excellent range.
All these findings suggest that the Hindi translation of WEMWBS, SWBS, and MHLC have an adequate level of psychometric properties in terms of internal consistency, test–retest reliability, and cross-language concurrence with the English version of the scale. It is hoped that the availability of these validated scales will facilitate further research in this direction.
Additionally, this study also aimed to evaluate the association of WEMWBS, SWBS, and MHLC with the level of religiosity, assessed by using CRS. It was hypothesized that those with high religiosity would have high SWB and high spiritual well-being. In terms of MHLC, it was hypothesized that those with higher religiosity would have a higher chance of health locus of control.
In terms of correlations, this study suggests that SWB, as well as spiritual well-being (both religious and existential), have a positive correlation with the level of religiosity. However, an inverse correlation was observed between the level of religiosity and chance locus of control. This inverse correlation possibly suggests that attribution of control to a higher power is not considered the same as that attributed to luck or chance.
This study has certain limitations. It was limited to a group of healthy subjects selected by purposive sampling. The study was done to evaluate the psychometric properties of these scales, rather than evaluating these concepts among people from India.
To conclude, this study suggests that the Hindi-translated versions of WEMWBS, SWBS, and MHLC have high internal consistency, test–retest reliability, and cross-language concurrence with the English version of the scale. It is hoped that the availability of these scales will further research in this direction in the general population and people with various mental illnesses.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.