
Abstract
Background:
Stigma related to mental illness is a reality among health care providers. This study is an attempt to understand the attitudes of doctors from different specialties toward mental illness and the stigma related to it.
Methods:
We used a concurrent nested mixed-methods approach to understand and identify the various factors of mental-illness-related stigma in medical practitioners. Between November 2018 and March 2019, 100 medical practitioners from South India were administered a self-reporting OMS-HC (Opening Minds Scale for Health Care Providers), followed by in-depth interviews among 25 of the 100 participants selected using purposive sampling. Quantitative surveys were analyzed using SPSSv23. In-depth interviews were transcribed as extended notes, translated, and initially explored using focused coding and the constant comparative method.
Results:
Though findings from quantitative analysis show low to moderate stigma (Mean = 53.52, SD = 7.61), the qualitative study revealed unintended and covert negative attitude toward mental illness.
Conclusion:
As stigma occurs at various levels—structural, institutional, interpersonal, and personal—anti-stigma measures also need to be systematically designed. Qualitative studies give more insight regarding the nature of stigma in medical practitioners toward mental illness
Mental-health-related stigma is a serious public health issue 6 and affects the quality of life of the patient. 7 Undertreatment is another issue related to this stigma. 8 Social marginalization is also prevalent in clinical settings. 9 In the medical community, health care professionals face mental health stigma (when affected) and also stigmatize others within the community (when another medical professional is affected). 10 These covert negative attitudes may be due to the lack of knowledge among doctors during their medical school training.11, 12
Few studies had addressed stigma related to mental illness among medical practitioners. Especially, studies among Indian medical practitioners are lacking. This suggests a need to systematically and accurately measure the attitudes of the medical practitioners. To understand the true nature of this stigma, it is necessary to do an exploratory study to identify various factors of mental-illness-related stigma in medical practitioners.
In this study, we used a concurrent nested mixed-methods approach to understand and identify the various factors of mental-illness-related stigma in medical practitioners. The study was designed to understand the attitudes of doctors from different specialties toward mental illness and to deconstruct and analyze the various components of stigma related to it.
Materials and Methods
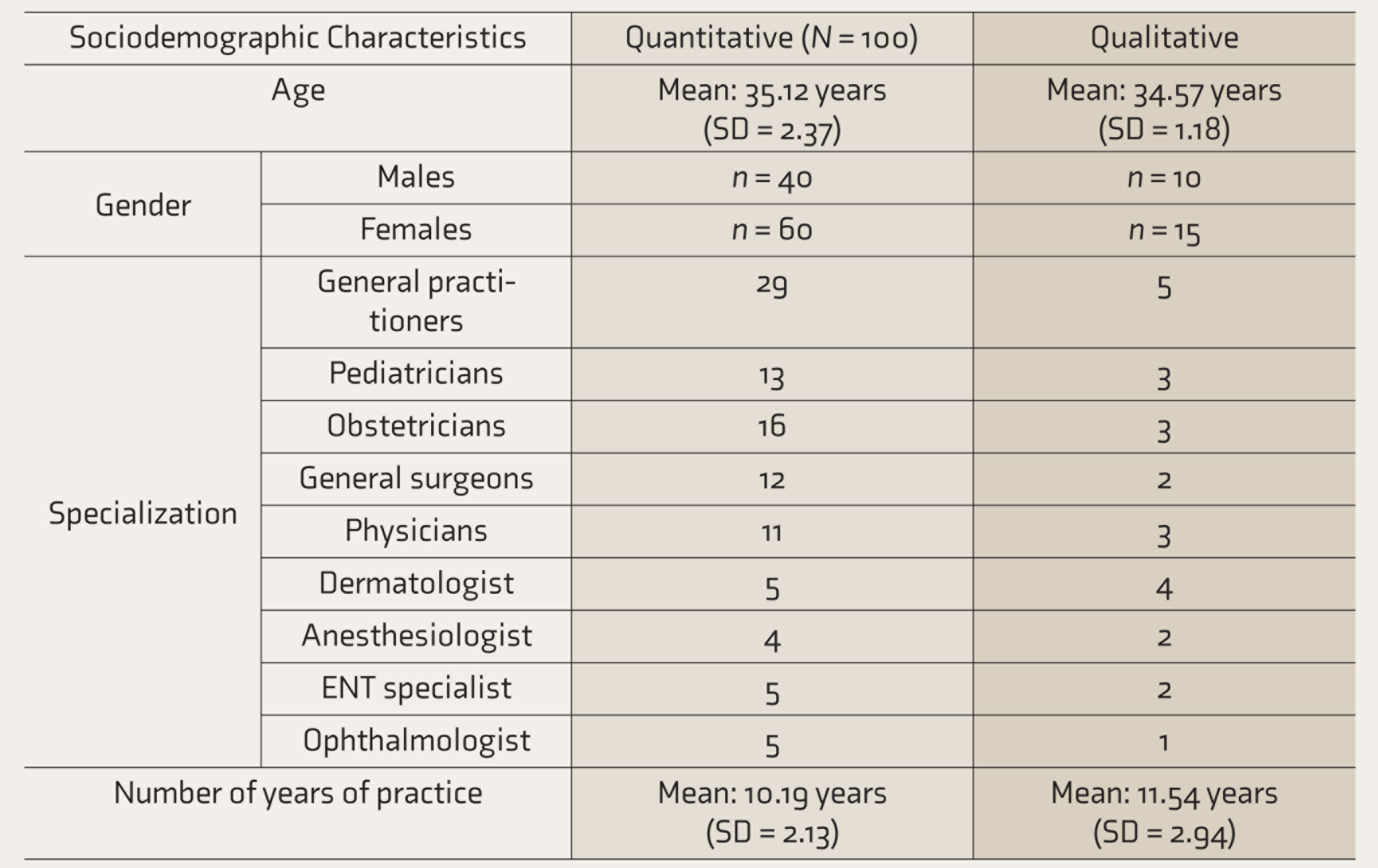
This was a mixed-methods study. It was approved by the Institutional Ethical Committee. The quantitative component used random sampling, while the qualitative component used purposive sampling. Between November 2018 and March 2019, 100 medical practitioners, across various specialties, working at different health care levels in South India were randomly chosen using the lottery method. The methodology for choosing the participants is as follows.
Five states of South India and their respective capitals were chosen, namely
Tamil Nadu, Chennai Andhra Pradesh, Vijayawada Karnataka, Bangalore Kerala, Trivandrum Telangana, Hyderabad
Premier tertiary care centers from these cities were chosen. Five doctors from each of the following specialties were randomly chosen to be contacted for the study: pediatrics, obstetrics, general surgery, general medicine, dermatology, anesthesiology, ENT, and ophthalmology. Five general practitioners belonging to the same geographic location too were randomly chosen using online directories. Overall, 225 doctors were contacted through phone initially and explained about the study, and their email addresses were obtained. A questionnaire about sociodemographic details (age, gender, specialization, and years of practice) and OMS-HC (Opening Minds Scale for Health Care Providers) was emailed to them.
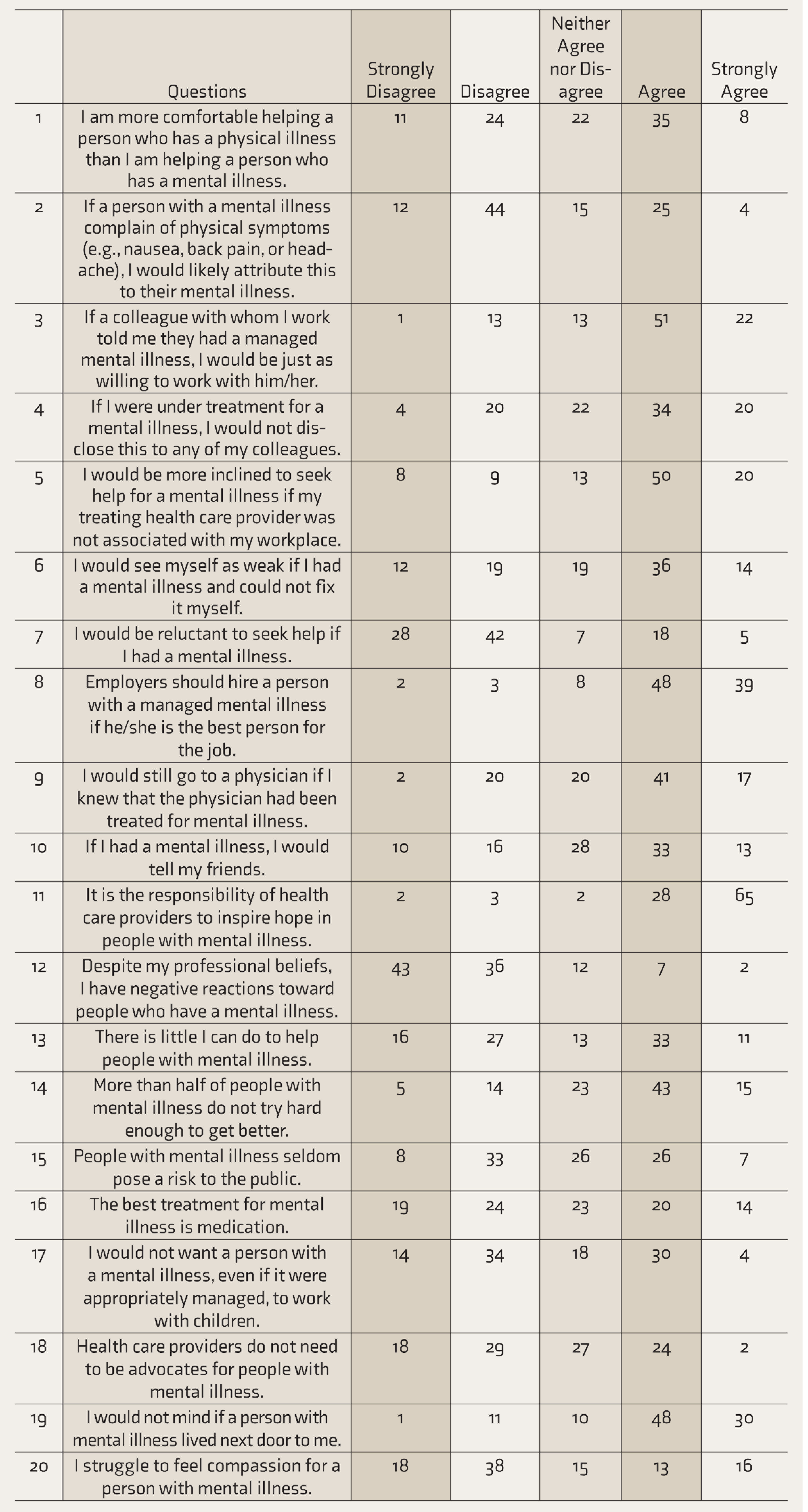
The OMS-HC is a 20-item self-report questionnaire on a 5-point scale, organized under three major sub-headings: Attitudes of health care providers toward people with mental illness; disclosure/help-seeking; and social distance. Seven items (3, 8, 9, 10, 11, 15, and 19) are reverse coded. The minimum score is 20, and the maximum score is 100. Higher scores correlate with higher stigma. The scale has Cronbach’s α of 0.77. 13
The participants were followed up for their responses. The responses were obtained as a separate Word document attached in the mail. Reminders were given after a couple of weeks. No personal identifiers were collected from the respondents.
Out of the 225 doctors, 67 did not respond to the email. Out of the 158 responses received, only 100 cleared the checks for completeness and consistency. Out of these 100 doctors with complete responses, 25 were purposively chosen for in-depth interviewing. The choice of doctors was done based on representativeness from the five cities and also the specialties that were approached for the quantitative survey. After procuring permission, AK met them in person at their places of work and interviewed them. The findings were taken as field notes. The author who conducted the interview in person (AK) is a trained qualitative researcher with over ten years of experience in qualitative research. The following interview guide was used for the in-depth interviewing:
As a doctor, what are the challenges you face in dealing with mentally ill patients? (In diagnosing, treating, explaining, referring, and other issues.) In case of your own mental health issues, what aspects would you consider in seeking help? (Modality of treatment, place, timing, trials, disclosure.) How do you deal with your family members’/relatives’ mental health issues? (Issues addressed in questions 1 and 2.) As an administrator, what are the aspects you would consider in the placement of a person whose mental illness has improved? (Nature of job, disclosure, timings.) How interested are you in communicating with a psychiatrist and how often do you interact with the psychiatrist in your workplace in discussing about patients? (Referral, follow-ups, doubts and clarifications, liaison issues.)
Quantitative survey was analyzed using SPSSv23. The in-depth interviews were transcribed as extended notes, translated, and initially explored using focused coding and constant comparative method.14, 15 A few emergent codes and categories were identified from the text and added to the existing codes gained from observational studies. Axial coding was done to develop connections between the categories derived from all the data. Themes were identified by looking for similarities, differences, and relationships between categories. 16
Results
Participant Characteristics
Sociodemographic Characteristics of the Participants
Responses to the Opening Minds Scale for Health Care Providers (OMS-HC)
Findings from the Qualitative Research
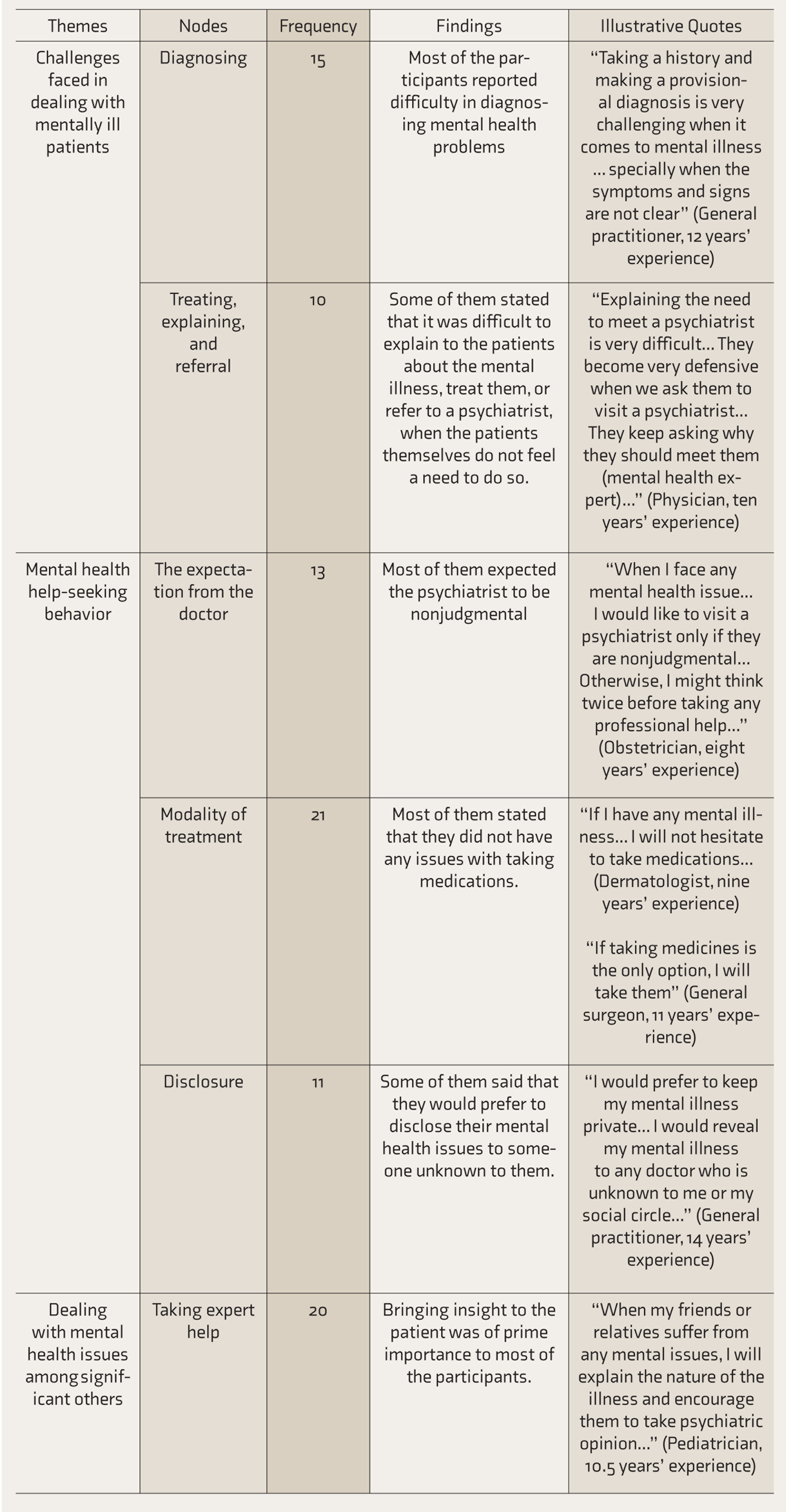
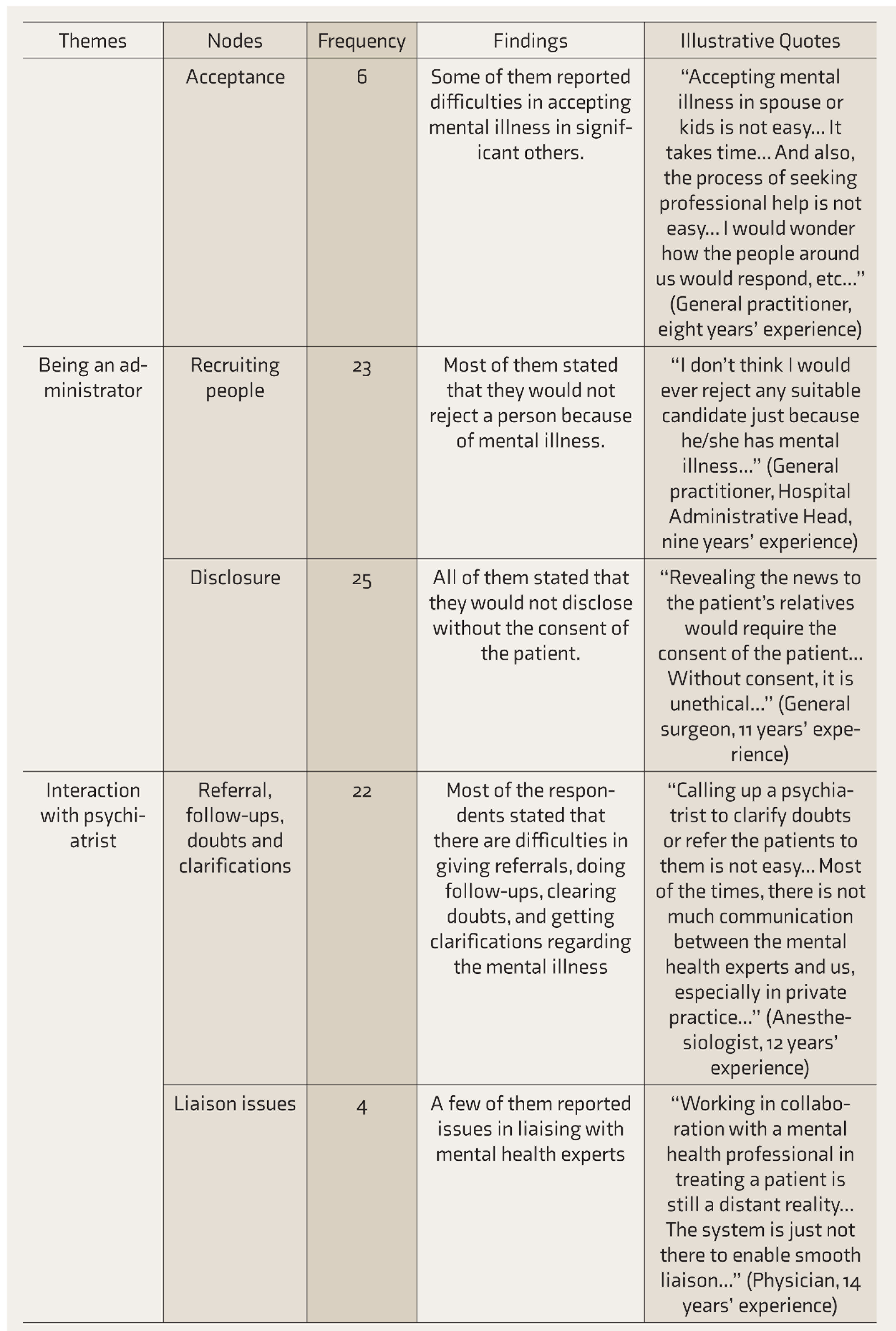
The qualitative analysis using grounded theory approach revealed various nodes that were organized into themes, and relevant illustrative quotes were selected. Table 3 shows the findings from qualitative research. They can be broadly classified as personal and interpersonal factors.
Findings from Qualitative Research
Personal Factors
Lack of awareness about mental illness and the resultant unconscious biases are the major reasons why doctors express stigma-related behavior toward a patient. This lack of awareness, coupled with a lack of adequate training and skills, leads to a failure to recognize and diagnose mental health problems. Even if identified, doctors felt that it was difficult to explain, treat, and refer patients to a psychiatrist when the patients themselves did not feel a need to do so. All this affects the patient–provider interactions and the quality of the care.
The acceptance of mental illness in significant others is debatable and differs from doctor to doctor though treating the illness has always been emphasized. When the doctors themselves are affected, they prefer nonjudgmental psychiatrists and preferred disclosure to mental health professionals who are mostly unknown to them. However, they felt no discomfort in taking treatment for their mental illness. When it comes to the workplace culture, the doctors respected the privacy of the patients. They invariably stated that they prefer nondisclosure policies and felt that mentally ill patients have the right to pursue their vocation, provided the illness does not interfere with productivity.
Interpersonal Factors
Doctors, when faced with challenges in identifying/diagnosing mental health issues, felt that liaising with mental health experts is an issue to be addressed. Also, there are difficulties in referrals, follow-ups, doubts, and clarifications, which affect holistic patient care.
Discussion
Stigma is a combination of several independent and interrelated factors. 2 Studies have reported a commixture of emotional, behavioral, and cognitive components leading to a cascade of labeling, othering, devaluation, and discrimination. 17 The process of stigmatization and its consequences happen in tandem at various levels: personal, interpersonal, and structural. 18 Stigma fosters fear, apprehension, and distorted views of mental illness and psychiatry. 19
Though OMS-HC indicated low to moderate stigma and a positive attitude and approach to mental illness among doctors, the interviews revealed many unintentional discriminatory behaviors, which they were unaware of. This reflected a tendency to “see the illness ahead of the person” and could contribute to dismissive behaviors such as addressing mentally ill persons as “difficult” and “manipulative.” Also, they held pessimistic views about the course of illness, treatment duration, and treatment outcome, which may affect the mental health seeking behavior of the doctors. This resonates with previous studies that mention mental-illness-related stigma in health care as a barrier to access and care. 20
In the present study, the challenges doctors face in dealing with mentally ill patients fell under “what and how to say and do” categories of problems. Though many had little or no difficulty in identifying psychiatric issues in their patients, they felt that they are ill-equipped to persuade the patient for a psychiatric referral. Similar studies have shown that there is a long-standing difference of opinion among the nonpsychiatric doctors about the appropriateness of psychiatric referrals. 21 The doctors, during the in-depth interviews, were more concerned about the side-effects of psychotropics and the duration of treatment. Studies from Swedish primary care also reported similar findings of skepticism related to medications. 22 Some practitioners, in our study, reported that they start a few patients on benzodiazepines as sedatives and anti-anxiety agents, albeit for a short term, without consulting a psychiatrist. The reasons cited were difficulty in convincing the patients to consult a psychiatrist, the perceived stigma of mental illness, and poor communication and rapport the doctors had with the psychiatrist. Similar problems of lack of rapport between nonpsychiatric doctors and psychiatrists have been reported in the literature, and this has been known to affect the delivery of quality care. 23
On the other hand, when dealing with psychiatric patients referred to them, the nonpsychiatric doctors find difficulty in eliciting the history, delineating the symptoms, and discussing the treatment with the patient. The majority accept social distancing and attribute it to the nature of the mental illness. Many expected the psychiatrist to play an active role in sensitizing the fellow doctors and to participate actively in general case conferences and academic meets. Academic literature cites similar suggestions from nonpsychiatric doctors who stated the need for sensitization by psychiatrists. 24
Consultation-Liaison Psychiatry (C-L Psychiatry) is almost nonexistent in India. Studies show that referral rates from other doctors remain very low, and many private super-specialty hospitals and tertiary care centers function without a psychiatry department. 25 Psychiatry has been alienated, ostracized, and side-lined from the mainstream medicine and has been rightly called the “Cinderella” of medicine. 26 It has always been a direct consultation by the patient or relatives when the reasons are obvious and, at times, by doctors when the behavioral disturbances are unmanageable. Many a time, referrals are made only when they are sought for.27, 28
Previous studies showed that in the case of their (doctors) illness, perceived stigma was higher than self-stigma, and also they were not sure about adherence to medication. 29 When it comes to the matter of mental illness among their significant others, doctors were more convinced of the need for treatment in the elderly but found it difficult to persuade them for treatment. 30 On the contrary, for their own children, they were not very convinced for taking any psychiatric consultation for stress-related issues and were highly skeptical about starting psychotropics. 31 Even in this present study, in-depth interviews reflected this skeptical attitude of nonpsychiatric doctors toward psychiatric medications.
Doctors in the study felt that the spectrum of mental illness is vast and could not be categorized under an umbrella term “psychiatric disorders.” In-depth interviews revealed that they saw common psychiatric illnesses differently from serious mental health disorders. Also, the attitudes of the respondents toward mental illness varied widely between manageable mental illnesses that are common and severe psychiatric illnesses that required hospitalization.
The in-depth interviews revealed that doctors had a better understanding of psychotic and neurotic illnesses than substance use and personality disorders. They were not much convinced about the need for referral and the reliability of persons with substance use disorders in case of employment. They were not convinced about referring a patient for psychiatric treatment (even when there were symptoms suggestive of underlying mental illness), an attitude that is commonly encountered in regular clinical practice.27, 28
Alienating, segregating, and ostracizing psychiatry continues, and though public awareness about mental health has improved, health care professionals need to “unlearn” many erroneous concepts about psychiatric issues. But for a few conditions, it has been reported that they hold a nihilistic attitude about recovery from the illness. 32
As stigma occurs at various levels (structural, institutional, interpersonal, and personal), anti-stigma measures also need to target the same. The strategies to be implemented should be integrated both vertically and horizontally. 33
The structural level includes insurance coverage, budget allocation, legislation, and policies, especially encouraging mental health-seeking behavior among health care providers. Institutional, interpersonal, and personal level are closely knit, and “catching them young,” and training medical students, interns, postgraduates, and resident doctors with more emphasis on treating mental illness within the same ontological realm as other illnesses is a key step in achieving “conceptual parity” and integration of psychiatry into mainstream medicine. 33
Sensitizing the nonpsychiatrists about the magnitude of mental health issues, the heterogeneity of the presenting complaints, the impact of psychiatric treatment on the overall improvement and well-being of the patient, and also the increased gratification for themselves for being “holistic” is an important strategy in combating stigma. Positive role models can bring about a change in organizational cultures. 33
Stigma reduction programs should be an ongoing and continuous process focusing on pre-service and in-service training of all cadres of health professionals. De-stigmatizing mental illness should be done through an emphasis on incorporating elements designed to increase knowledge, develop skills, and change the attitude toward mental illness. The programs should target the unintentional, unconscious bias toward mental illness and be a truly myth-bursting and transformative learning experience. 33
The study has the following limitations: lower response rate from the respondents, which affects the generalizability of the findings. The concurrent mixed-method design was chosen to offset the weakness due to <50% responses in the quantitative survey and single interviewer bias in qualitative research. The study was self-funded, which affected the scale of research. Hence, a limited number of respondents were chosen, and the study was limited to South India.
Future research focusing on rigorous evaluation and standardization of anti-stigma measures and testing the designed intervention methods for effectiveness could guide us in the right direction.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.