
Abstract
Background:
Banning smoking in public places has considerably reduced the number of smokers. However, the sale of loose tobacco encourages tobacco use. There is limited data on compliance with section 7(2) of the Cigarettes and Other Tobacco Products Act (COTPA), 2003, concerning the ban on loose tobacco sales in India. The aim of this study is to assess the compliance of section 7(2) of COTPA concerning the ban on loose tobacco sales in four selected cities of Karnataka.
Methods:
This community-based study used a cross-sectional design. Two neighboring cities, that is, district headquarter from North (Bidar and Vijayapura) and South (Mandya and Chikkamagaluru) Karnataka were considered for the study. A total of 207 vendors and 204 smokers were selected using time-cluster sampling. Data was collected using observation and interview methods. Semi-structured interview schedules were administered to smokers and vendors. Percentages and frequencies were used to describe the data.
Results:
Most tobacco vendors (92%) and smokers (91%) were unaware of the loose tobacco ban. Most smokers (76%) perceive that buying cigarettes in packets would increase smoking. Most smokers (96%) prefer to buy cigarettes in loose. The sale of loose tobacco was widely prevalent (94%) in the four surveyed cities. Point of sale of loose tobacco includes tea shops (38%), petty shops (31%), pan shops (25%), and bakeries (6%).
Conclusion:
There is a high degree of noncompliance with Section 7 (2) of COTPA, 2003 regarding ban on selling loose tobacco.
There is a high degree of noncompliance with Section 7(2) of COTPA in Karnataka due to poor awareness among smokers and vendors about the ban on loose tobacco sales. Most consumers prefer to buy loose cigarettes as they smoke less and because of the lower cost. Most vendors prefer to sell loose cigarettes based on smokers’ demand.Key Messages:
Tobacco use is a serious public health threat worldwide and in India. The prevalence of tobacco use shows a decreasing trend among males (42.4%) and females (14.2%). In India, tobacco use declined overall by 6%, from 34.6% in 2010 to 28.6% in 2017. 1 In Karnataka, it reduced by 3% during the same period. Tobacco use among adolescents (aged 15–17 years) has also decreased from 10% to 4%. 1
Cigarettes and other Tobacco Products Act (COTPA), 2003, prohibits smoking in public places, regulates tobacco products’ sales and advertisements, and bans selling loose tobacco (LT). As per Section 7 (2) of COTPA, “No person shall carry on trade or commerce in cigarettes or any other tobacco products unless every cigarette or any other tobacco products sold, supplied or distributed bears thereon, or on its label, the specified warning.” 2 Individual cigarettes and bidis do not carry a statutory health warning. Hence, the sale of LT (individual or small units) would be in non-compliance with COTPA Section 7 (2). Therefore, selling cigarettes and other tobacco products without a packet is prohibited.
Rationale for the study: The purpose of any health warning gets defeated when the smoked or smokeless product does not carry any health warning. Worldwide, limited data exists on health warnings over LT. In September 2017, Karnataka became the 17th state in India to ban loose cigarette sales.3, 4, 5 Later, the Karnataka state anti-tobacco cell was interested in knowing the extent of this ban. Secondly, it is mandatory to carry out a periodical evaluation of the progress made in implementing the National Tobacco Control Programme. Hence, the present study examined the extent of the LT ban in four cities (district headquarters) of Karnataka.
Methods
This community-based study used a cross-sectional design to assess the awareness of and compliance with the ban on LT sale. The study was conducted in two neighboring cities, each of North and South Karnataka, Bidar and Vijayapura (North) and Mandya and Chikkamagaluru (South), in November 2019. Rationale for selecting two districts from north Karnataka was, as both districts were economically backward and far away from Bangalore. The other two southern districts were economically developed and near Bangalore. Compliance refers to the degree to which law is obeyed. LT refers to one or more unpackaged cigarettes, bidi, and rolls of tobacco leaf (chuttu/cigar). LT ban refers to the prohibition of selling one or more cigarette(s), bidi(s), and other tobacco products without a pack containing the statutory health warning. Tobacco vendors are those who sell cigarettes/bidis in pan shops, tea stalls, bakeries, and other general stores.
Tobacco vendors and smokers were selected using time-cluster sampling (a sampling method utilized when the variables to be studied are likely to vary at different points of time in a day). Data were collected at two different points of time; 11.00 am–2.00 pm and 4.00 pm–6.00 pm in a day at different clusters (different study locations), assuming that smokers will be available during the peak hours (morning tea break, lunch break, evening tea break, and after work hours). Ten clusters (bus stops, market and shopping areas, hotels, religious and tourist places, banks, educational institutions, railway stations, playgrounds, and hospitals) were surveyed in each city.
The sample size was calculated assuming 50% compliance with the ban on the sale of LT, with a margin error of 6%, using the formula n = pqZ 2 /d 2 , where ‘n’ is the minimum sample size, ‘p’ is the estimated proportion of the population (0.5), ‘q’ is variance of population (0.5), ‘Z’ is the value from the normal distribution for α = 0.05 [(confidence level at 95%), standard value (1.96)], ‘d’ is the allowable error (6%). n = (0.5 × 0.5) × 1.96 2 /0.06 2 , n = 0.96/0.0036. Thus, the estimated minimum required sample size was 267. Considering other factors, such as the number of items in the questionnaire for tobacco vendors and smokers, it was decided to select 100 samples in each city (50 vendors and 50 smokers). Two separate semi-structured interview schedules were administered to smokers and vendors. An interview schedule was drafted with the help of subject experts (mental health professionals working in addiction medicine) and validated by field experts (from the state antitobacco cell). The study used a standard proforma (for compliance studies); items were selected from questionnaires used by the John Hopkins Bloomberg School of Public Health, International Union against Tuberculosis and Lung Disease, and Campaign for Tobacco-Free Kids. 6 A few items were modified to suit the topic of compliance with the ban on LT sales. The interview schedule (available as an online-only supplementary file) had 14 items for smokers and 11 items for vendors, such as city name, nature of study location, neighborhood description, date and time of visit, age, education, awareness about the prohibition on LT sales, mode of preference of purchasing/selling tobacco, reasons for buying LT, difficulties in purchasing cigarettes in full pack, and perception and their opinion of the same. Interview and observation methods were used for data collection. Observation was used to assess the compliance on ban of LT sale (LT was sold or not at point of sale). Percentages and frequencies were used to describe the data. The primary parameter of the study was whether the sale of LT was observed in a particular location or not. Ethical clearance was obtained from the Institute Ethics Committee (Ref: NIMHANS/ EC(Beh.Sc.Div)/19th Meeting/2019).
Procedure for Data Collection
Two research assistants, postgraduates in Social Work with previous work experience in community research, carried out the study. They were trained in COTPA 2003 (with a special focus on sections 4 to 7), data collection procedures, as well as study design and sampling procedure for compliance studies. Before proceeding to the four cities for data collection, they conducted a pilot study for 15 days under supervision in certain locations (Bruhat Bengaluru Mahanagara Palike). The pilot study was conducted to pre-test the predesigned data collection tools. Google forms were created to enter the responses from the interview schedule. The study followed the guidelines prescribed for the best practices concerning compliance studies. 6
Results
A total of 207 tobacco vendors and 204 smokers were interviewed for the study across the four cities. About 120 smokers and 60 vendors refused consent to participate in all four cities.
Table 1 has details of the study locations where the sale of LT was observed. The most studied locations were market and shopping areas, hotels, restaurants, tourist places, and bus stops. Smokers and vendors were interviewed about awareness of the prohibition of LT sale.
Observations of Locations of Tobacco Sale.
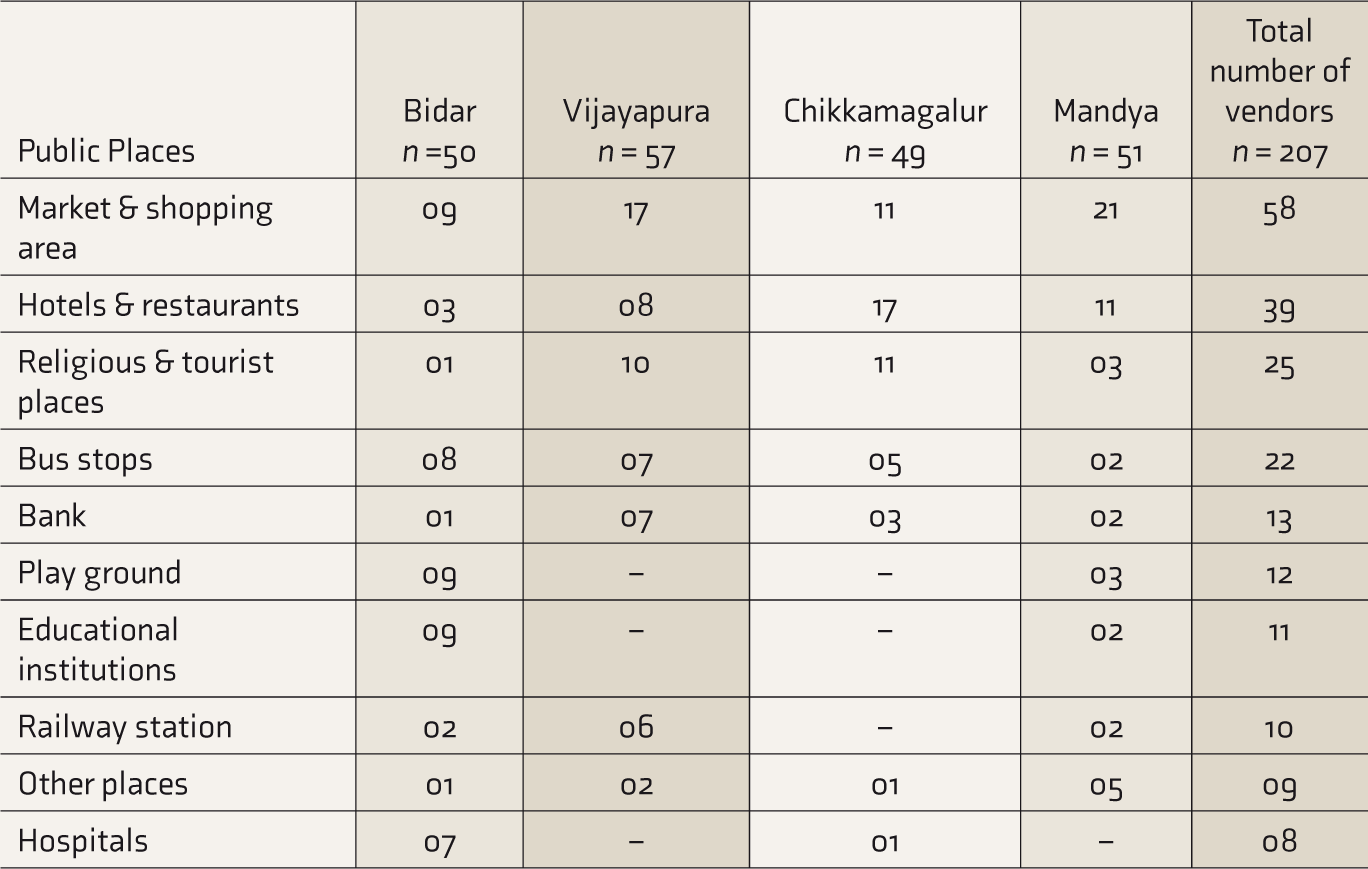
Table 2 shows that most tobacco vendors were males (96%). Four minor male children were selling tobacco. Almost all smokers available during the interview were males. About half of the users (46%) and vendors (47%) had studied up to 10th or below. Most smokers (55%) belonged to the younger age group of 20–39 years, and 51% of vendors belonged to the middle-age group of 30–49 years.
Demographic Profile of the Tobacco Users and Vendors.
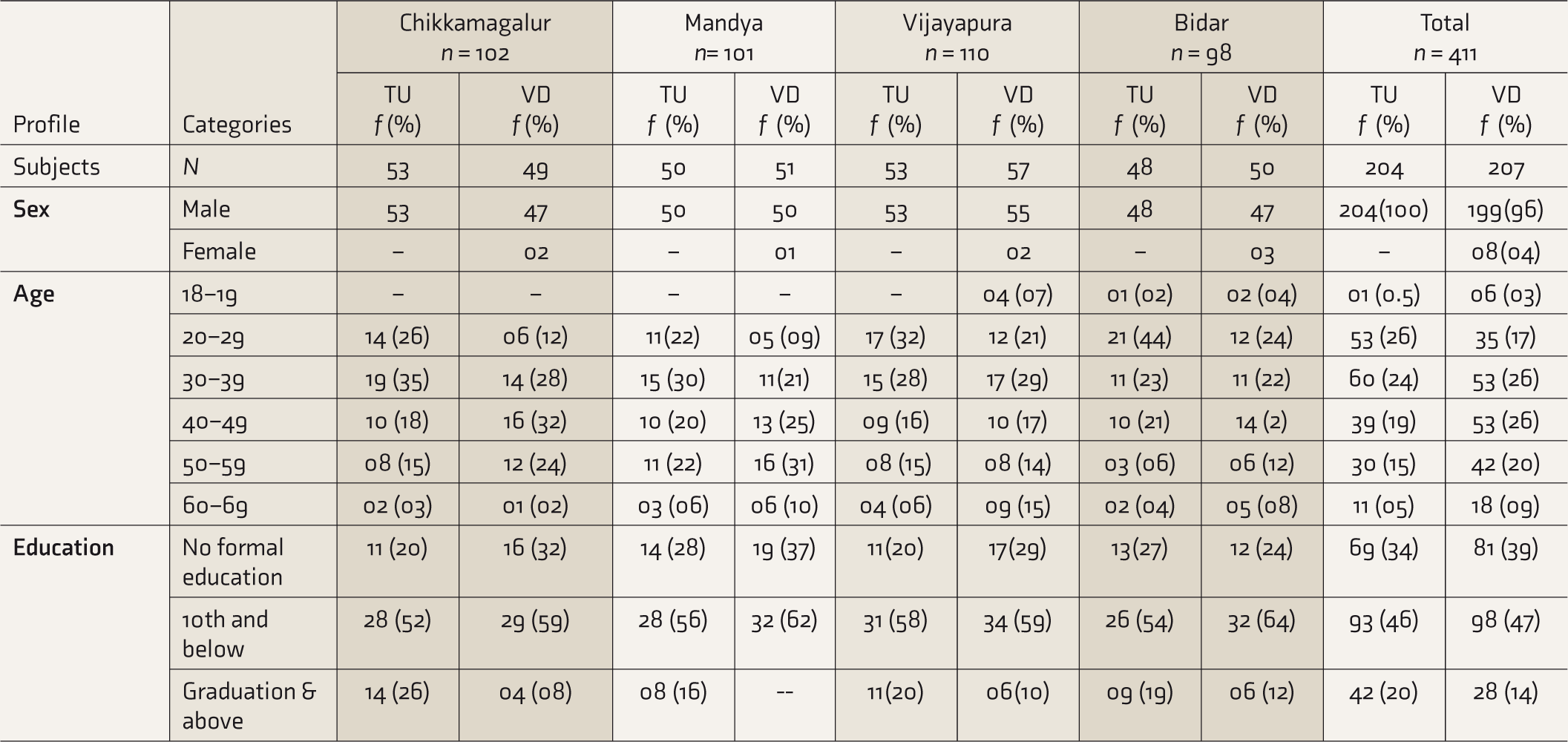
F: frequency, TU: tobacco users, VD: vendors.
Most tobacco vendors (92%) and smokers (92%) were unaware of the ban on the sale of LT (Table 3). Awareness was better among vendors in Chikkamagaluru (21%) than the other three cities. Awareness among smokers was comparatively more in Mandya (20%) than the other three cities (<10%).
Compliance with Loose Tobacco Ban (TU = 204, VD = 207).
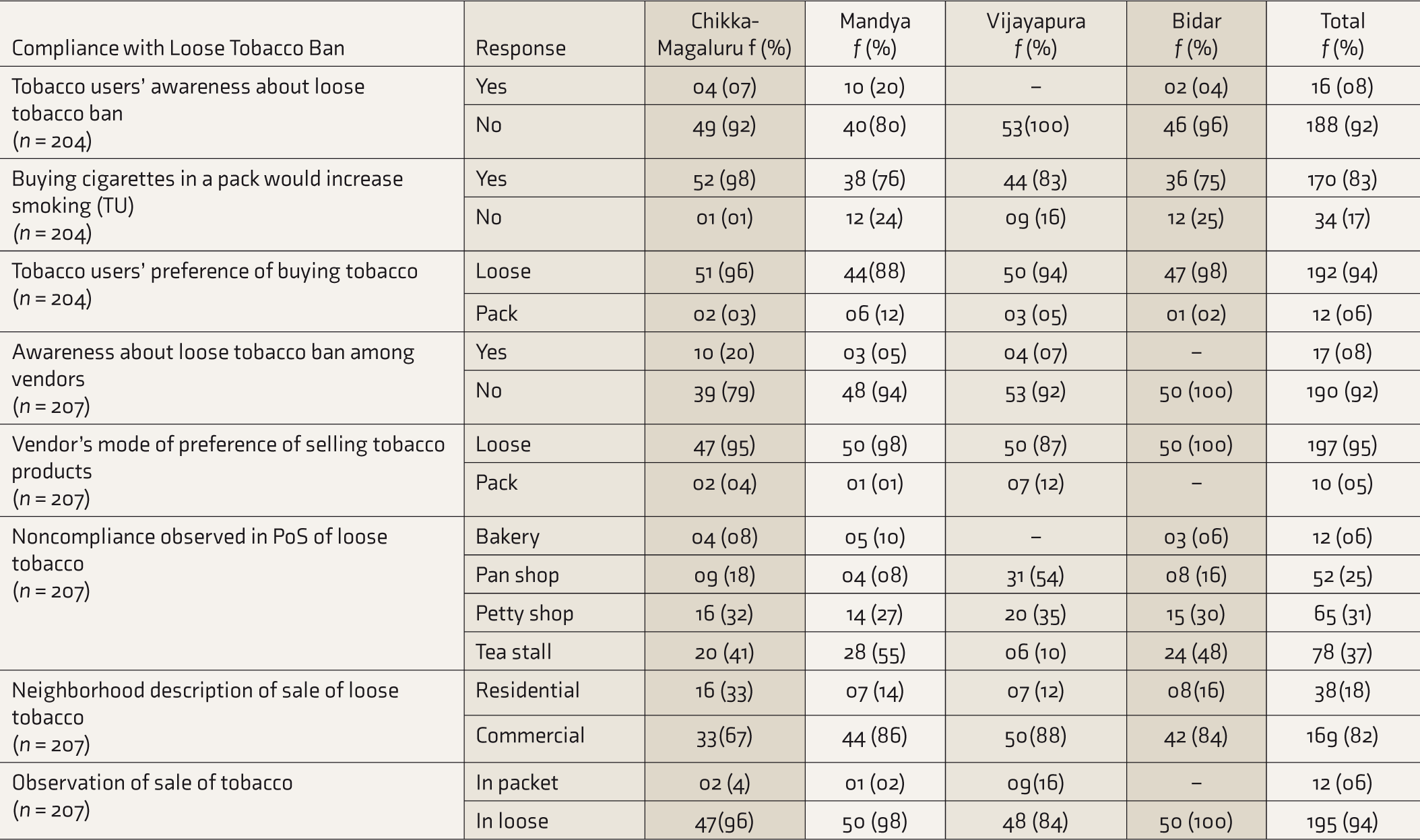
PoS: point of sale, TU: tobacco users, VD: tobacco vendors.
Most smokers (94%) preferred to buy loose cigarettes, and most vendors (95.2%) preferred to sell LT. Preference for buying cigarettes packets was relatively more among smokers in Mandya (12%) than the other three cities (<5%). Most smokers (83%) perceived that buying cigarettes in a pack would increase smoking. The most common point of sale of LT was tea shops (38%), followed by petty shops (31%), pan shops (25%), and bakery cum tea stalls (6%). These were the most common places that were noncompliant with the prohibition.
Pan shops were the most noncompliant point of sale in Vijayapura (54%), while tea shops were the most common noncompliant point of sale in Mandya (55%), Bidar (48%), and Chikkamaguluru (41%). LT was sold more in commercial areas (82%) than residential areas (18%). Sale of LT was more in residential areas (33%) of Chikkamagaluru than other three cities. Most cigarettes (96%) were sold loose, and only 4% were sold in packets. Overall, our observation revealed that LT sale was widely prevalent (94%) in the four cities surveyed. It was comparatively less in Vijayapura city (84%) than in other cities (> 95%).
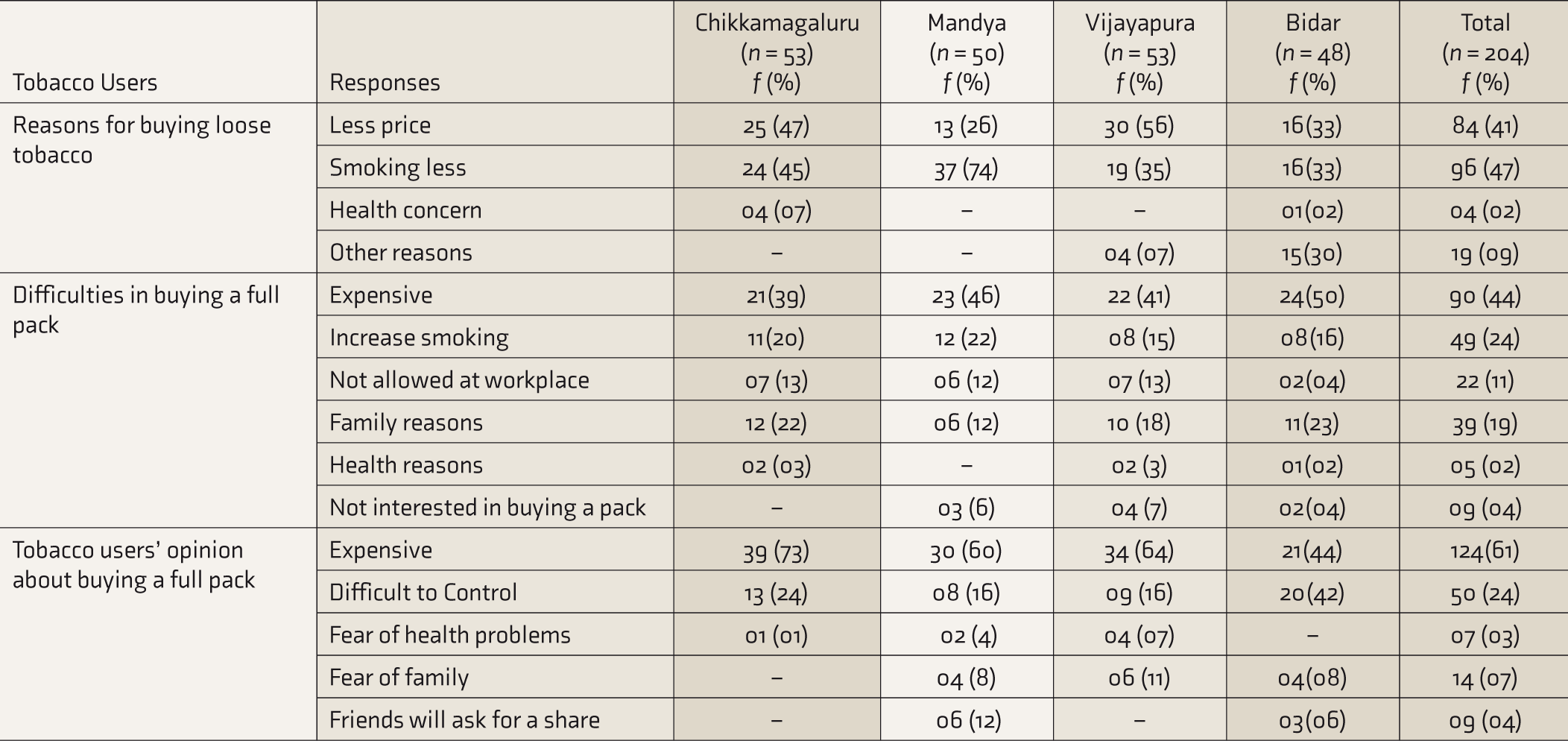
Most smokers reported that the reasons for buying a single cigarette were that they smoke less and that it costs less (Table 4). More smokers in Vijayapura (56%) and Chikkamagaluru (47%) reported that the lower price was the reason for buying LT sticks. In Mandya, most smokers (74%) revealed that the reason for buying LT was that they smoked fewer cigarettes. Most smokers expressed their difficulties in buying cigarette packets, such as the high cost, the belief that buying in packets might increase their smoking, and the fear that family members might come to know about their smoking. It would be difficult for them to reduce smoking, and their friends would ask for cigarettes.
Tobacco Users’ Reasons for Buying Loose Tobacco.
More vendors (n = 17) were aware of the ban on selling LT than consumers (n = 16). Across the four cities, level of awareness of the LT ban and compliance with section 7 (2) of COTPA, 2003, was poor.
Discussion
Almost all surveyed smokers in this study were male. Previous studies have found that 1% of women purchased LT7, 8 and that 43% of current female smokers bought loose cigarettes. 8 We found that 4% of tobacco vendors were female, whereas earlier studies did not report the gender of the vendors. It may be possible that in a few shops, both male and female (married couples) sell tobacco together during peak hours. We found that people from all age groups and educational levels purchased LT. More than half of the smokers who buy loose cigarettes were of young age (20–39 years). Earlier studies reported that half of the LT buyers are 15–30 years of age.7, 8
We found that most smokers’ and vendors’ education level was 10th or below. As per previous research, those who are males, young adults, unmarried, less educated, unemployed, living in metropolitan cities, current smokers, and planning to quit in the next 30 days are more likely to purchase loose cigarettes.8, 9
Most of the surveyed smokers were from lower and middle socioeconomic status. Earlier studies reported similar findings that the purchase of loose cigarettes is more among those who are poor or less educated or are from informal economic sector or lower socioeconomic communities.10, 11 In contrast, Singh et al. 8 reported that smokers from all socioeconomic statuses bought loose cigarettes. Previous studies showed that urban disadvantaged smokers were more likely to buy loose cigarettes. 12 The present study was carried out in four cities. Therefore, rural and urban comparisons could not be made.
We found a high degree of noncompliance with the ban on LT sales in the four cities. Previous studies reported high rates of noncompliance with the ban on the sale of LT in Udupi and Ahmedabad.7, 13, 14, 15 Most cigarettes were sold loose in Chennai, Delhi, Jaipur, Patna, Agartala, Baroda, Shimla, and Bengaluru.10, 16 Goa had the lowest proportion of LT sale and higher pack sales. There is a wide variation (59%–87%) in the proportion of LT sale across Indian states. 10
Most vendors sold loose cigarettes. Possible reasons are buyers not asking for packs and motives for profit or tax evasion. In a previous study, vendors’ reasons for selling loose cigarettes were demand from smokers, absence of health warnings, and benefits of selling more. 7 We found that the most common points of sale of LT were tea stalls, petty shops, pan shops, and bakeries. In earlier studies, they were general stores, followed by petty shops, bakeries, and street vendors.7, 17
We found that most smokers bought LT. The most cited reasons for buying LT were smoking less and lesser cost, as the pack is expensive. A single cigarette of yellow flake (name changed) costs ₹18–20, and the pack costs ₹175. Previous research has found that in a few places, single cigarettes are sold at almost double the unit cost of cigarettes sold in packs. 18 This price increase causes fewer sales of factory-made cigarettes and higher sales of LT. 19 Previous studies reported that smokers buy LT because they smoke less, ease of buying, being less expensive, perceived approval, nondaily smoking, the intention to reduce and quit, and the wide availability and sale of single cigarettes daily in their neighborhood.7–8, 11, 20-21 Most loose cigarettes were sold in commercial than residential areas. An earlier study reported that loose cigarettes were sold more in residential and commercial areas than in industrial areas of Bengaluru. 16
Our observation revealed a high percentage of loose cigarette sales (94%) across four surveyed cities. A previous study reported a similar finding that the prevalence of loose cigarette sales was 93% in four states surveyed in India. 22 Kapoor et al. 23 reviewed India’s tobacco control policy responses toward banning singles and other products sold as LT. 17 Indian states and jurisdictions provide sufficient legal framework to substantiate their complete ban on LT. We found that tobacco sales points were fewer in and around health care facilities and educational institutions. Previous studies reported similar findings that compliance with COTPA 2003 was more in and around health care facilities and educational institutions.24–26
LT sale is widely prevalent in many developed and developing countries where the law prohibits such sales. In developed countries, individuals with less income or less education and socioeconomically disadvantaged people tend to buy single cigarettes more. 17 In Africa, advertising for LT occurs through different channels. 27
The World Health Organization Framework Convention on Tobacco Control (FCTC), article 16, bans the sale of tobacco products in loose or small units to prevent children from accessing tobacco as it increases the affordability and accessibility. Recognizing the threat to public health, the Department of Consumer Affairs, Government of India, amended the Legal Metrology Act to prohibit the sale of loose cigarettes. Considering the amendment of the Legal Metrology Act by the Central Government, the state’s anti-tobacco cell, the Department of Health and Family Welfare, Karnataka, banned the sale of loose cigarettes, bidis, and chewing tobacco. Despite the ban, the sale of LT continues.
The amended Legal Metrology Act makes it mandatory for loose cigarettes and other tobacco products to bear the specified health warnings. Persons violating the ban are liable for punishment under Section 20 of COTPA: imprisonment up to one year, a fine up to ₹1,000, or both, in the case of first conviction. A repeat offense may result in imprisonment of up to two years and a fine of up to ₹3,000. The Indian government increased the excise duty on cigarettes by 11% to 72%, depending on the stick’s length. Despite the hike, cigarettes are still cheaper in India than in other countries. Most cigarette sales happen through kiosks and tobacco vending machines. The sale of loose cigarettes leads to tax avoidance, and vendors tend to buy packs from states with lower cigarette taxes.
Single cigarettes are sold at higher prices in India. There are myriad challenges in the enforcement of its ban. Buyers of single cigarettes are less exposed to health-warning labels. The ban on LT sale is largely not complied with, and such bans would likely increase the level of contraband and illegal trade and shift tobacco consumption to other forms. Only a few smokers would be able to afford the packets. Further, many tobacco cessation clinics consider purchase of single cigarette as an effective strategy in quitting.
Poor compliance with the ban on LT sale shows a need for rigorous enforcement. Educating sellers about laws prohibiting such sales through mass media and strict licensing procedures are the few ways to ensure compliance with Section 7 (2) of COTPA. Results of this study would be helpful for advocacy, policy makers and enforcement agencies to strengthen the ban on LT sale. The study provides evidence of the wide prevalence of LT sale and identifies the implementation gaps in the four surveyed cities.
We recommended few strategies to contain loose tobacco sales include, rigorous enforcement and public education, activities to improve awareness of the LT ban, geographic information system to map tobacco vendors, more robust quality monitoring processes and surveillance across taluks and cities, formation of anti-tobacco squad cells at the taluk levels, education of tobacco retailers about ban of LT sale, statutory health warnings on single sticks, strict vendor licensing, and printing expiry date on a single cigarette.
Limitations
Only four cities in Karnataka were surveyed. Hence, the study findings cannot be generalized. Information on the motivation of smokers, employment status, duration of smoking, earlier quit attempts, numbers of cigarettes smoked daily, type of tobacco products, and brands sold in loose by vendors were not elicited. The public health impact of the sale of single cigarettes was not studied.
Conclusion
There is a high degree of noncompliance with the LT ban in Bidar, Chikkamgaluru, Mandya, and Vijayapura cities of Karnataka. Most consumers and tobacco vendors were unaware of the LT ban. Most consumers prefer to buy, and vendors prefer to sell LT.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Dr Selvaraj, Deputy Director (Medical), Dr Sridevi Deshpande, Consultant, Mr Prabhakara, Programme Manager, State Tobacco Control Cell, National Tobacco Control Programme (NTCP), Department of Health & Family Welfare, Government of Karnataka, for funding. The authors thank Mr Vishnu Prasad and Mr Pradeep Kumar CB, Research Assistants (NTCP), for data collection. Dr Marimuthu, Professor, Department of Bio-Statistics, NIMHANS, Bengaluru for sample size calculation.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by State Anti-Tobacco Cell, National Tobacco Control Programme, Department of Health and Family Welfare, Government of Karnataka.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.