
Abstract
Background:
Little is known about elder abuse in the domestic environment. In lower-middle income countries like India, the demographic transition is throwing novel challenges. The older adults are relatively more vulnerable because of coexisting medical and psychological problems. Any form of abuse affects mental health and increases the chances of anxiety and depression among the older adults. The study aimed to assess the burden of abuse amongst older adults visiting a primary health care center of north India.
Methods:
This is secondary data analysis conducted on the data collected in the primary study between September 2017 and June 2018 in northern India among 311 older adult patients attending the noncommunicable disease clinic. Diabetes mellitus and hypertension were diagnosed as per standard guidelines. Vulnerability to Abuse Screening Scale (VASS) was used to assess elder abuse. Depression, anxiety, and loneliness were assessed by using the Patient Health Questionnaire (PHQ)-9, Generalized Anxiety Disorder (GAD)-7, and University of California, Los Angeles (UCLA) loneliness 20-item scale, respectively. Multiple logistic regression was carried out to explore the factors associated with elder abuse after ruling out collinearity between independent variables.
Results:
About 24% of older adults experienced abuse in the last 12 months. One-fourth of the older adults reported vulnerability, nearly half reported coercion and dejection, and most of them reported experiencing dependence. Participants also had a high prevalence of anxiety (39%), depression (54%), and features suggestive of loneliness (38.6%). Multiple logistic regression analysis showed that abuse was predicted by educational status, per-capita income, and loneliness.
Conclusion:
About one-fourth of the older adults experience abuse. This highlights the importance of routine screening of older adults at the primary care level.
Keywords
About one-fourth of the older adults experience abuse. Experience of abuse is associated with the presence of loneliness, anxiety disorder, and depression.Key Messages:
In lower-middle income countries like India, the demographic transition is throwing novel challenges in the social and economic domains. Urbanization, industrialization, and globalization have indirectly encouraged the concept of nuclear family which has, in turn, increased problems for the older adults, making them vulnerable to abuse. 6 With the increase in life expectancy due to better education and health facilities, the proportion of the older adults has increased from 5.3% in 1971 to 8.6% in 2011. 7 Studies from different parts of the world suggest that elder abuse is very common, with a global prevalence of around 16%. 8 Some European studies report prevalence as high as 61.1%. 9 A study from the United States reported prevalence of elder abuse to be around 10%. 10 In a nation-wide survey from China, 36% of the elders reported being a victim of abuse, with no gender variation. 11 Studies from India have also reported a high prevalence of abuse in older adults.12, 13
The older adults are relatively more vulnerable because of coexisting medical conditions such as diabetes mellitus and hypertension, as well as psychological problems like loneliness and fear of impending death. Any form of abuse among the older adults affects psychological health and increases the chances of anxiety, depression, suicide, dementia, malnutrition, somatization, and chronic pathological deterioration, leading to enhanced fragility. 9 Plethora of risk factors like sociodemographic variables such as increasing age and low family income, functional and cognitive impairment, and lack of social support play a crucial role in elder abuse. The victims in India largely underreport elder abuse. 6 The sense of shame to the family and cultural stigma associated with elder abuse may overshadow the motivations to seek interventions. 14 Unfortunately, screening for abuse is also not on the priority list of the clinicians as it is currently not a part of the formal training. 15 Although awareness of the problem is steadily increasing, elder abuse continues to be underdiagnosed and overlooked. With the increasing burden of noncommunicable diseases (NCD), dedicated NCD clinics provide excellent opportunities to screen for abuse. There is a paucity of literature from India that evaluates the prevalence of elder abuse. With this rationale, this study was undertaken to assess the prevalence of elder abuse amongst older adults who are living with vasculometabolic disorders such as diabetes and hypertension and are visiting a primary health care center in North India. Additionally, the study evaluated the relationship of elder abuse with loneliness, depression, and anxiety.
Methodology
The primary study was conducted in the state of Punjab between September 2017 and June 2018. It is a prosperous state (ranks second in terms of the human development index) in the northern part of India, with a population of 27 million according to the 2011 national census. 16 There is a high prevalence of hypertension (18.9%–59.7%) and diabetes (1.4%–18.0%) among adults across different age groups in this state.17, 18 The main objective of this study was to assess the burden of co-existing mental illnesses and NCDs amongst the older adults (≥60 years) in Punjab. The primary results are published elsewhere.19–21 Elder abuse was assessed as a correlate of psychiatric morbidity in the older adults.
The secondary data analysis presented in this article was conducted on the data collected in the district of Fatehgarh Sahib of Punjab (population 600,000; area 1,147 km2; sex ratio 871; literacy rate 80.3), with the purpose of evaluating the prevalence and correlates of vulnerability to abuse and other psychosocial comorbidities among the older adult patients attending the NCD clinic.20, 21 Besides preventive and diagnostic services, the patients who were diagnosed with diabetes mellitus or hypertension were also provided medicines and weekly follow-up free of cost through this NCD clinic.
Ethics approval was obtained from the Institutional Ethics Committee. Written informed consent was obtained from the participants before the interview.
Considering the prevalence of abuse among older adults in India as 25%, 13 5% precision, and 10% nonresponse rate, the total sample size was calculated to be 310 (Stat-calc, Epi Info: version 7.2.0.1). All ambulatory patients aged ≥ 60 years and diagnosed with either diabetes mellitus, hypertension, or both were included in the study. Patients who were too ill to participate were excluded. All new patients, that is, those who visited the clinic for the first time, were recruited consecutively until the required sample size was attained.
A preformed semi-structured questionnaire was used to assess the sociodemographic profile, including age, gender, educational status, socioeconomic status (per-capita monthly income was calculated as per BG Prasad socioeconomic classification scale, 2017 22 ), and marital status. Diabetes mellitus was diagnosed as per the WHO guidelines, whereas the diagnosis of hypertension was established using the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7) criteria.23, 24
Vulnerability to Abuse Screening Scale (VASS) was used to assess elder abuse. This tool comprises 12 dichotomous questions that have good psychometric capacity for the screening of abuse over the past 12 months. The English version of the scale was translated into Hindi by using WHO methodology. 25 A total score of ≥6 was used as a threshold to measure the vulnerability to abuse. VASS has four subscales (dependence, dejection, vulnerability, and coercion), each consisting of three items. It provides information on various forms of family abuse, such as emotional, psychological, and verbal abuse. Elder abuse in various domains was considered to be present if the participant reported “yes” to at least one of the items in each of the subscales. Amongst the four subscales, vulnerability and coercion are direct measures of abuse, while dependence and dejection are indirect indicators. Dependence domain indicates a risk for abuse indirectly as older adults requiring assistance for daily activities may be more vulnerable to abuse. The items on the dependence subscale of VASS are worded in such a way that the response “yes” indicates its absence.
Depression was assessed by using Patient Health Questionnaire (PHQ)-9, 26 which is a self-administered questionnaire, scoring each of the nine DSM-IV criteria as “0” (not at all) to “3” (nearly every day). Anxiety was assessed by using Generalized Anxiety Disorder (GAD)-7 Questionnaire, which measures how the patient felt in the last two weeks. 27 Loneliness was measured through the University of California, Los Angeles (UCLA) loneliness 20-item scale designed to measure one’s subjective feelings of loneliness and social isolation. 28 These scales are useful in primary health care settings for screening purposes.
Analysis and Statistics
Quantitative data were double-entered and validated using EpiData Entry Version 3.1 and subsequently analyzed using EpiData Analysis Version 2.2.2.182 (EpiData Association, Odense, Denmark). The key outcome variable was the prevalence of abuse in the older adults, which was expressed in percentages. Pearson’s correlation analysis was used to assess the correlation between vulnerability to abuse and per capita income, duration of physical comorbidities, depression, anxiety, and experiencing loneliness. Stepwise forward conditional binomial logistic regression was used to design the best model for predicting the vulnerability to abuse. Variance inflation factor (VIF) was used to detect multicollinearity between the independent variables before including them in the final regression analysis model. Odds ratios with 95% confidence interval were used to measure the strength of the association.
Results
Study included 311 participants. Overall, about one-fourth (24%) of the study participants experienced abuse in the last 12 months. The dependence component of abuse, followed by the coercion component, depicted the highest prevalence. Gender-wise subcomponent analysis did not reveal any significant difference across the two genders (Table 1).
The mean age of the study participants was 65.1 years (range: 60–86 years). Half of the older adults (50%) were diagnosed with hypertension, while 29% were diagnosed with diabetes mellitus. The duration of the disease in the majority of the participants was more than ten years (Mean±SD: 10.43±4.6 years). The participants had a high prevalence of anxiety (39%), depression (54%), and characteristics suggestive of loneliness (38.6%).
Table 2 depicts the association of elder abuse with the different sociodemographic variables, loneliness, and psychiatric comorbidities. Only per-capita income of the family, education of the patient, and presence of loneliness depicted a significant association (P < 0.05) with elder abuse. No association was observed for vulnerability of abuse with gender, marital status, physical comorbidities, depression, and anxiety.
The logistic regression model was statistically significant, χ2(7) = 8.388, P = 0.30. The model explained 47% (Nagelkerke R2) of the vulnerability to abuse and correctly classified 76.5% of the cases. Depression and anxiety depicted collinearity with loneliness and hence were not included in the regression analysis. The final model depicted education, per-capita income, and loneliness as the major predictors of vulnerability to abuse. It was observed that illiterate respondents (OR: 0.50; 95% CI 0.28–0.90, and aOR: 0.49; 95% CI: 0.25–0.92), or those with a lower level of education (up to primary classes)(OR: 0.19; 95% CI 0.08–0.45, and aOR: 0.16; 95% CI: 0.07–0.40), were less vulnerable to abuse compared to those with high school and above level of education. Patients in the lower per-capita income group were more vulnerable to abuse (OR: 0.36; 95% CI 0.15–0.85, and aOR: 0.26; 95% CI: 0.10–0.63). Loneliness emerged as a strong predictor of abuse vulnerability (OR: 3.91; 95% CI 2.26–6.76, and aOR: 4.35; 95% CI: 2.43–7.78) (Table 3).
Only loneliness depicted a weak positive correlation with the subscales of the VASS, while no correlation was seen with depression or anxiety (Table 4).
Discussion
Elder abuse is an emerging global public health problem, which is not limited to particular sociodemographic or socioeconomic strata. India is experiencing a demographic transition, and the proportion of older adults is expected to rise to 12.5% of the population by 2026. 29 With the rise in the older adults population, the prevalence of elder abuse is expected to rise.
In our study, about one-fourth of the older adults reported abuse. In terms of abuse as per the various domains of VASS, one-fourth of the older adults reported vulnerability, nearly half reported coercion and dejection, and most of them reported dependence.
The prevalence of vulnerability to abuse varies with ethnicity and people’s perceptions. 30 A study from North India used the same scale for assessing abuse and reported a higher prevalence of older adults abuse in a community-based sample from North India. 12 The authors observed that about twothirds of the older adults reported coercion and dejection, while about half reported dependence and vulnerability to abuse. Another study reported low prevalence of vulnerability (28.4%), dependence (13.7%), dejection (45%), and coercion (2%) among rural older adults. 31 A study from South India reported the prevalence of abuse to be around 10%. 32 In Asia, a study from mainland China reported prevalence of 36.2%, while the data from Africa suggest prevalence to range from 30% to 43.7%.11, 33, 34 In developed countries in the Europe and United States, the prevalence of elder abuse ranges between 2.2% and 47.3%.35, 36 The wide variation in the prevalence reported across the globe is attributed to differences in education level, awareness, and reporting of abuse.
In those who reported abuse, no significant differences were observed between the different age groups of older adults or across the two genders. Previous studies have reported higher percentages of females being victims of abuse.30, 37 This can be related to a higher life expectancy among women because of which they tend to live alone more often as a dependent person compared to their male counterparts, which makes them more vulnerable to abuse. Lack of difference in the elder abuse across the two genders in this study possibly suggests that older males are also equally vulnerable to experience abuse.
Prevalence of Abuse Older Adults
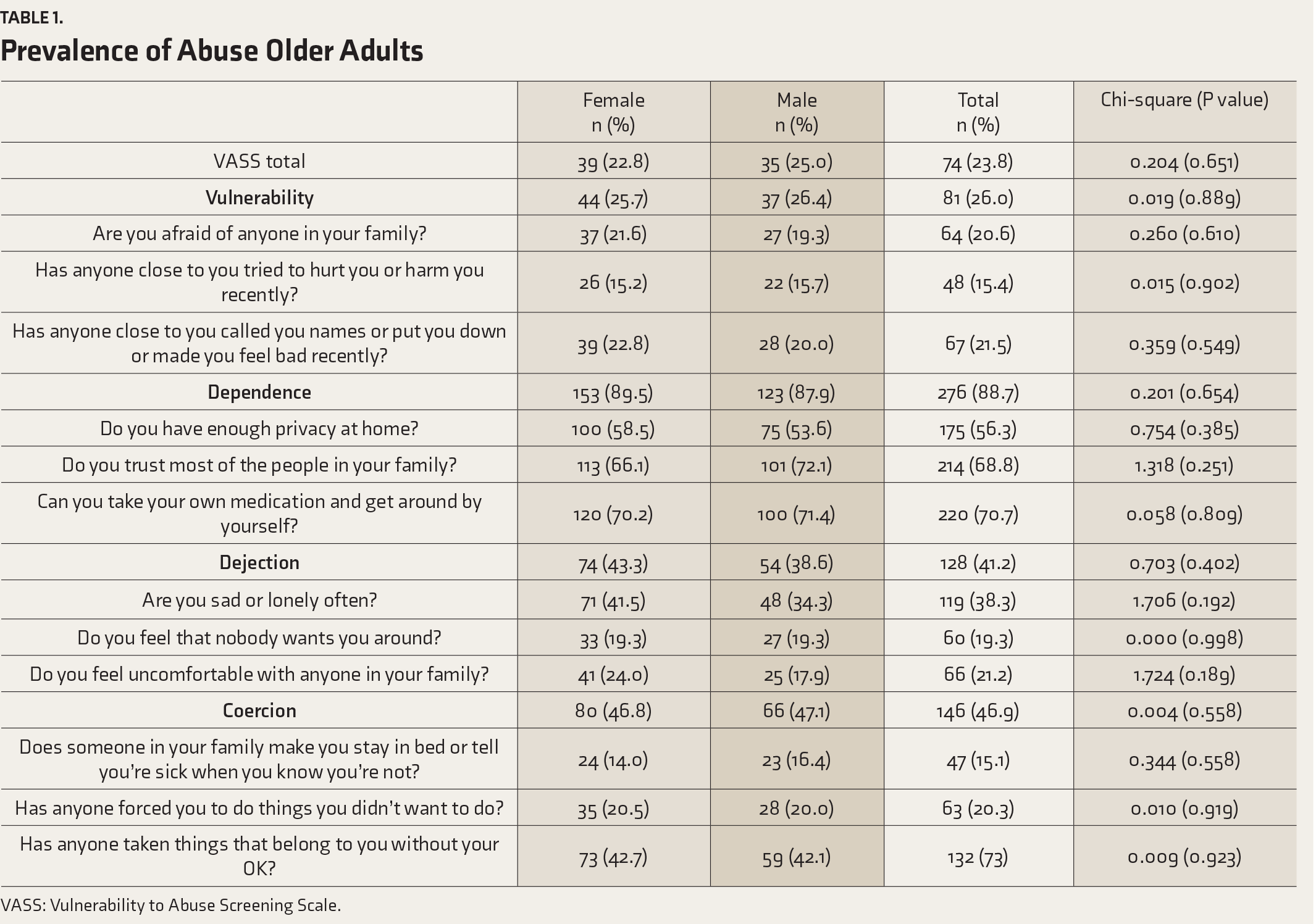
VASS: Vulnerability to Abuse Screening Scale.
Abuse was significantly associated with educational status and loneliness. Available data also suggests that the presence of loneliness is associated with increased risks of psychological abuse in elders.40, 41 Studies from other parts of the globe suggest that depression and anxiety are risk factors as well as consequences of abuse.30, 39, 42, 43 However, in this study, depression or anxiety were not included in the final multiple regression model as they demonstrated multicollinearity with loneliness.
Association between Older Adults Abuse and the Sociodemographic and Clinical Variables
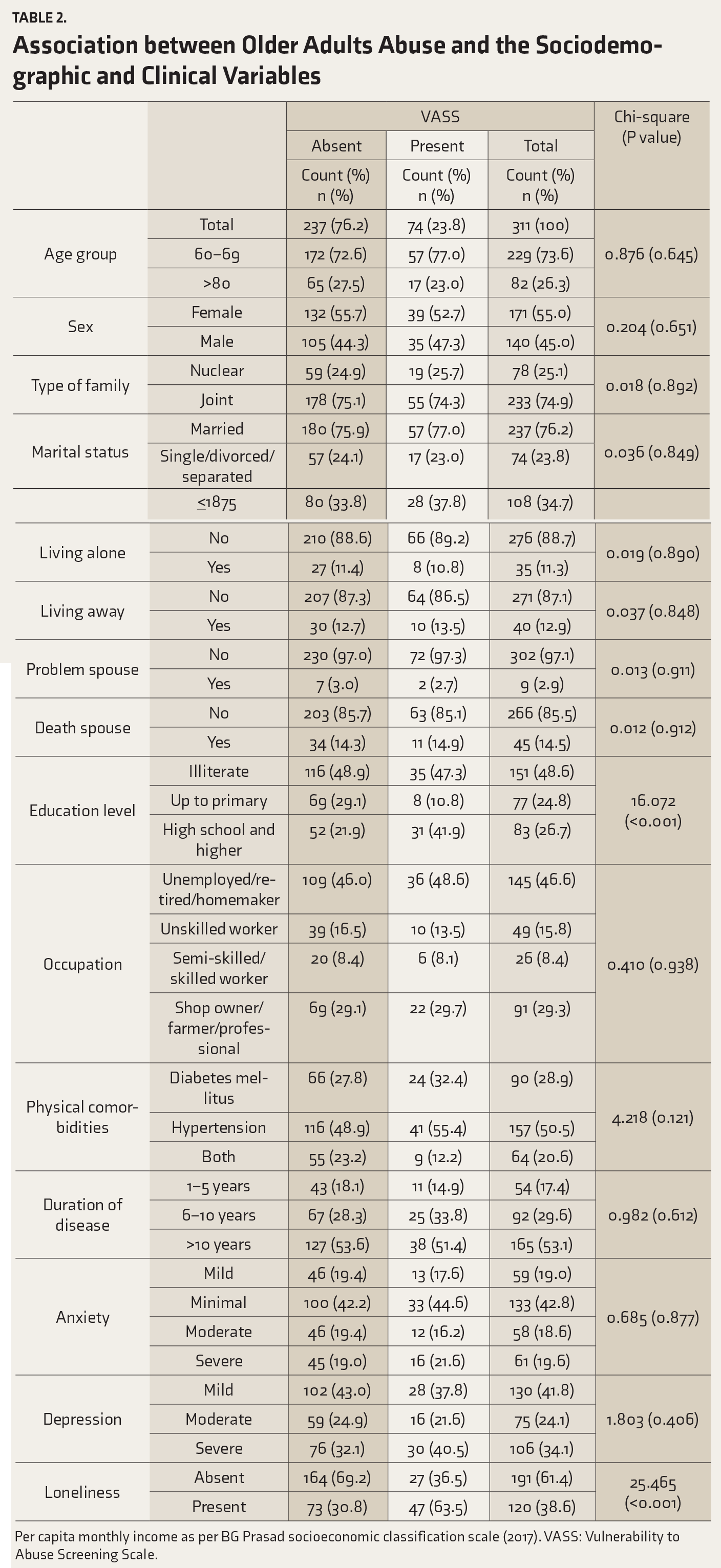
Per capita monthly income as per BG Prasad socioeconomic classification scale (2017). VASS: Vulnerability to Abuse Screening Scale.
Multiple Logistic Regression Analysis Showing the Association between the Vulnerability to Abuse and Other Variables
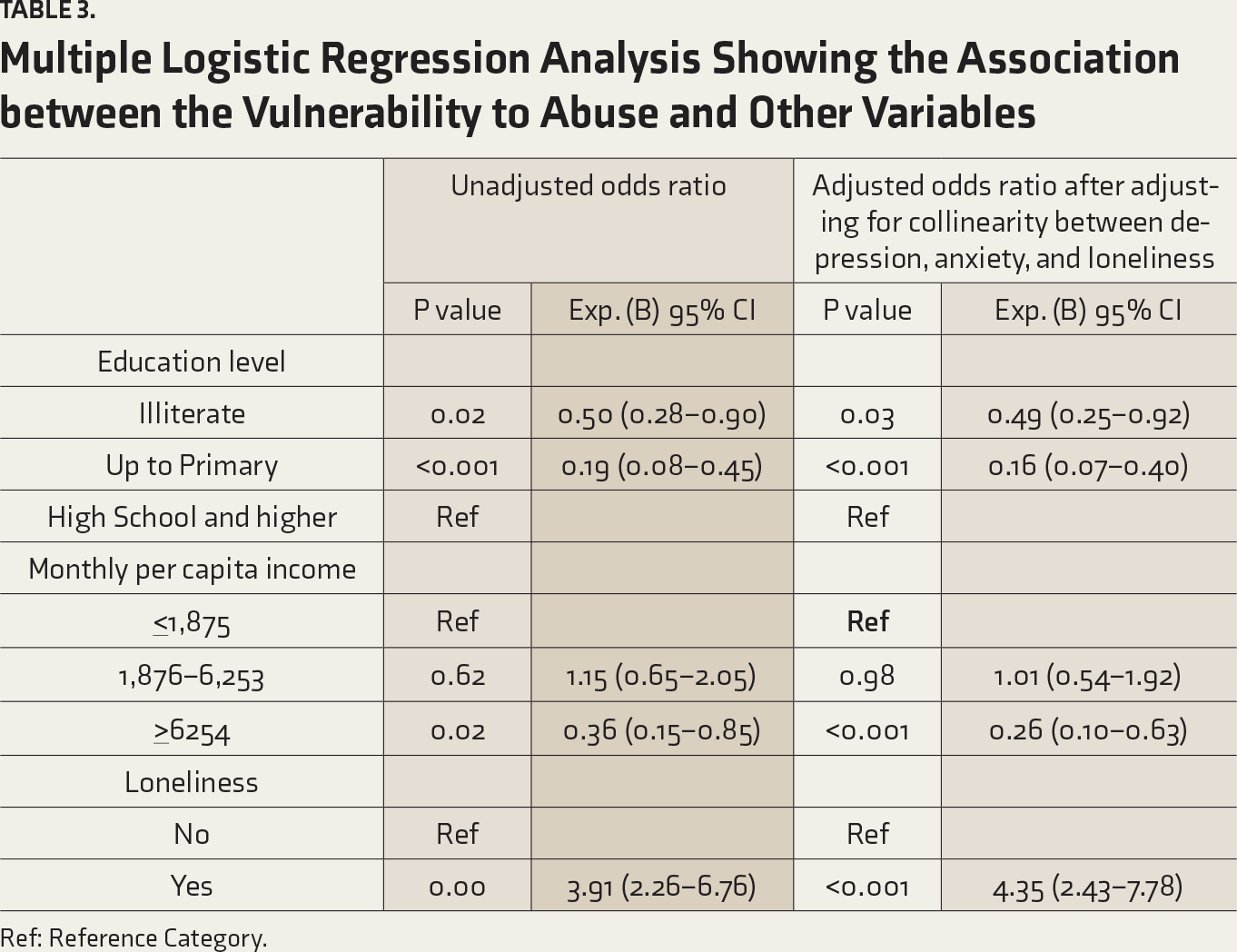
Ref: Reference Category.
Correlates of Abuse Older Adults
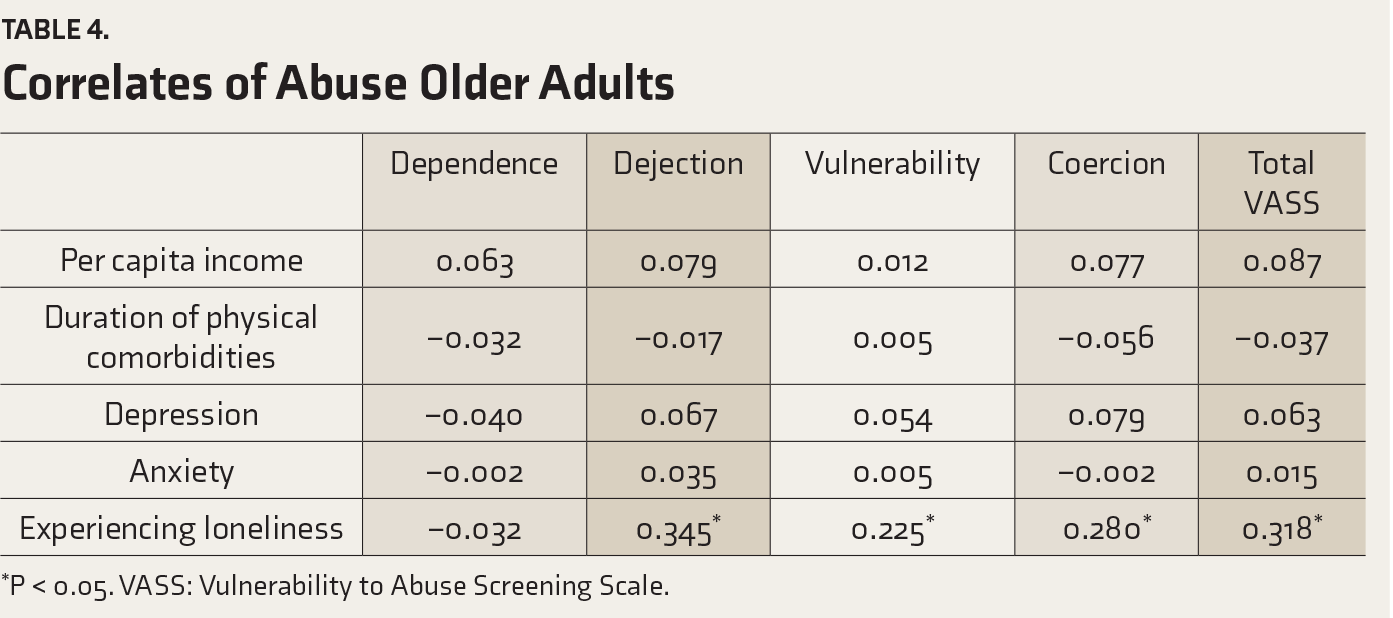
*P < 0.05. VASS: Vulnerability to Abuse Screening Scale.
There are certain limitations to the study. First, being a cross-sectional study, it is difficult to conclude which factor came first and which factors followed as the sequelae. Existing knowledge may benefit from repeated measures of these comorbidities during intensive screening camps, which in itself is a mammoth task in a resource-constrained country like India. Second, abuse may be under-reported because of the associated stigma. Third, we did not examine the physical abuse. Fourth, the diagnosis of depression and anxiety disorder was based only on assessment questionnaires. Fifth, the tool relies on reporting of abuse in the past 12 months. Hence, chances of recall bias cannot be ruled out.
Conclusion
Elder abuse is highly prevalent. With the increasing proportion of older adults in India, the burden of these problems is expected to escalate. Accordingly, there is a need to routinely screen the older adults for abuse.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.