
Abstract
Background:
Parkinson’s disease (PD), the second most prevalent neurodegenerative disorder, presents a significant challenge in terms of both motor and non-motor symptom management. Deep brain stimulation (DBS) emerges as an advanced therapeutic option, showing efficacy in alleviating PD symptoms. However, the literature on educational programs tailored for patients with PD undergoing DBS remains scattered and underexplored.
Objective:
This study sought to map the existing evidence on educational programs designed for patients with PD receiving DBS, highlighting the scope and nature of such interventions.
Methods:
Following Joanna Briggs Institute guidelines and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 extension, a scoping review was conducted. Relevant documents were identified through PubMed, Scopus, CINAHL, EMBASE, Web of Science, and Google Scholar systematic searches up to November 2024. The review examined content, delivery of educational programs, and outcomes, as well as program characteristics, materials used, and involved health care providers. A narrative synthesis was performed to integrate the findings without specific statistical tests due to the scoping nature of the review.
Results:
Seven studies were included. Educational interventions demonstrated a positive impact on social adaptation, physical performance, and patient satisfaction. Notably, innovative tools such as the DBS-Edmonton app were identified as beneficial in enhancing patient autonomy and decision-making.
Conclusions:
The review underscores the critical role of multidisciplinary, tailored educational interventions in supporting patients with PD undergoing DBS. Despite the promising benefits observed, the field requires further standardization and research to optimize educational strategies and to improve patient outcomes.
Keywords
Parkinson’s disease (PD) ranks as the second most prevalent progressive neurodegenerative disorder. 1 This condition is characterized by the degeneration of dopaminergic neurons within the substantia nigra pars compacta of the midbrain. 2 Current estimates suggest that PD affects ~0.3% of the general population, increasing to 1% among individuals over 60 years of age and 3% in those over 80 years. 3 Clinically, PD manifests through a spectrum of symptoms, including motor symptoms such as tremors, bradykinesia, postural instability, and rigidity. It is also associated with a range of non-motor symptoms, including cognitive decline, depression, anxiety, dysautonomia, and sleep disturbances. 4
The cornerstone of PD management traditionally encompasses pharmacological treatments alongside non-pharmacological interventions, 5 including physical and occupational therapies. 6 Nevertheless, the Movement Disorder Society’s evidence-based review on motor symptom management in PD highlights deep brain stimulation (DBS) as a pivotal treatment for the advanced stages of the disease. 7 Indeed, existing literature contains evidence of significant clinical enhancements in both motor and non-motor symptoms responsive to dopaminergic treatment and improved quality of life following DBS, coupled with a notable reduction in medication dependency. 8 Although the precise mechanism by which DBS exerts its effects remains to be fully elucidated, it is posited that the stimulation delivers an inhibitory synaptic effect, thereby modulating the electrical and biochemical activities of cells within the basal ganglia. 9 In this context, the “Core Assessment Program for Surgical Interventional Therapies in PD” protocol has been established to guide the selection, preoperative evaluation, and postoperative follow-up of patients deemed suitable candidates for DBS. 10
Following DBS therapy, a notable improvement in managing PD symptoms could be anticipated, including both motor and non-motor aspects. 11 This advanced treatment, however, is not without its side effects; patients may experience physical changes such as weight gain, dysarthria, and dysphagia. On a psychological level, an increased incidence of emotional disturbances, including anger and suicidal ideation, has been reported. 12 These observations underscore the importance of comprehensive patient education beyond the mere adjustment to enhanced motor abilities or modifying their medication regimen.
Given the complexities of managing PD and the implications of DBS therapy, it becomes pivotal to emphasize the empowerment of patients in the management of their condition. 13 Educating patients about self-care practices is crucial, enabling them to take proactive steps toward managing their symptoms and adjusting to life with DBS. 14 This approach is vital for fostering a sense of self-efficacy among patients, thereby equipping them with the knowledge and skills necessary to effectively navigate the challenges associated with PD and DBS therapy.
Expanding on the conceptual framework of self-care for chronic illnesses, which advocates for health preservation through proactive behaviors and effective illness management, 15 the demand for bespoke educational interventions for patients with PD undergoing DBS is underscored as a pivotal aspect of clinical care. PD’s complexity and personalized nature, particularly at advanced stages necessitating DBS, highlight a significant gap in our comprehension and application of patient-centric educational methodologies. Initiatives to aggregate and examine the current body of research on educational programs for patients with PD receiving DBS are essential. They promise to refine and enhance educational interventions tailored to improve the lives and self-sufficiency of these patients. Although sparse, current literature could elucidate which interventions are most effective in ameliorating patient outcomes, enabling a more seamless adjustment to the multifaceted challenges posed by DBS. In this context, employing scoping reviews as a methodological approach allows for (a) the elucidation of core concepts and terminologies within the scholarly discourse; (b) the identification and articulation of existing knowledge gaps; (c) the provision of a thorough and contemporary synthesis of information for health care professionals, researchers, and educators; and (d) the promotion of further inquiry and innovation in this domain.16,17 Therefore, this study aimed to systematically map the literature regarding educational programs available to patients with PD undergoing DBS.
Methods
Design
A scoping review was conducted to systematically map the literature landscape concerning educational programs for patients with PD treated with DBS. This methodological approach facilitated an exploration into the unsynthesized and heterogeneous body of knowledge relevant to this area of research. 18 The guidelines of the Joanna Briggs Institute Method Manual for scoping reviews were adhered to, 18 and findings reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 19 The protocol of this study is available elsewhere. 20
Research Questions
The main research question (RQ) was developed following the Population, Concept, and Context framework 18 (see Table 1): What does the literature reveal about educational programs for patients with PD in treatment with DBS? Specific subquestions were developed to gain a more nuanced understanding of the literature, focusing on various aspects of educational programs for patients with PD treated with DBS: (RQ1) What characteristics define educational programs for patients with PD and DBS? (RQ2) What types of educational materials are utilized within these programs? (RQ3) Who is responsible for delivering these educational programs? (RQ4) What outcomes have been observed for those who participate in these educational programs?
PCC to Design Question Research.
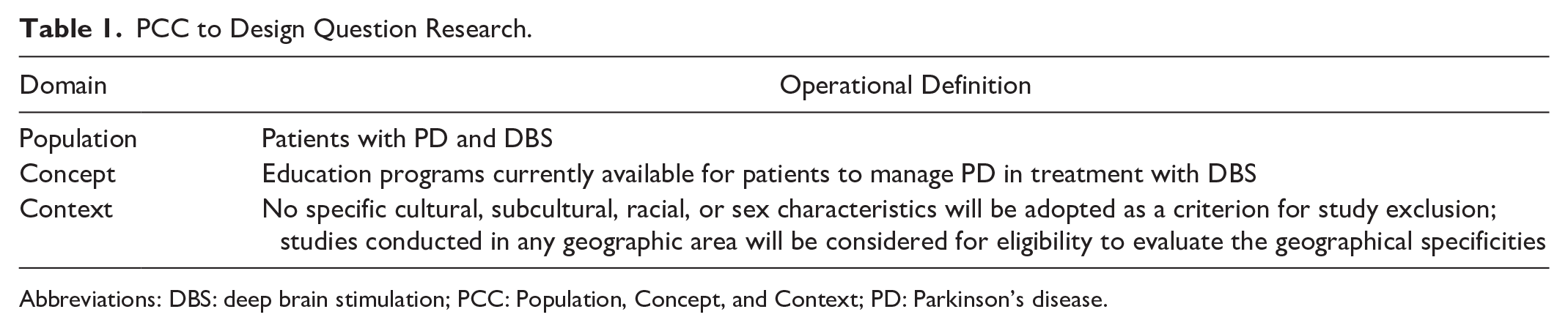
Abbreviations: DBS: deep brain stimulation; PCC: Population, Concept, and Context; PD: Parkinson’s disease.
These subquestions aim to consider the multifaceted nature of educational interventions, offering insights into their composition, delivery, and impact on patient outcomes.
Eligibility Criteria
The inclusion criteria encompassed a wide range of study designs, including systematic reviews, qualitative studies, observational studies, uncontrolled trials, non-randomized controlled trials, perspective papers, editorials, expert opinions, and policy papers. Studies were eligible if they were published in either English or Italian, with no constraints on the publication date.
To ensure a clear and focused selection of studies, educational programs were defined as structured interventions aimed at improving patients’ or caregivers’ knowledge, skills, or self-management related to PD and DBS. These programs could be delivered through various modalities, including written materials, digital applications, in-person training, or multidisciplinary counseling.
Studies were included if they explicitly described educational programs for patients with PD undergoing DBS, including preoperative, perioperative, and postoperative educational interventions. Additionally, studies were considered if they examined structured educational interventions aimed at enhancing patient understanding, decision-making, symptom self-management, or postoperative adaptation to DBS. Research focusing on the role of health care professionals such as nurses, neurologists, or physiotherapists in delivering education related to DBS in PD was also included. Rehabilitation interventions were considered only if they explicitly incorporated an educational component, such as structured guidance on managing motor symptoms, cognitive adaptation, or DBS device management.
Studies were excluded if they solely focused on rehabilitation, physiotherapy, or exercise interventions without an educational component related to DBS. Research evaluating general PD management strategies without addressing DBS-specific education was also excluded. Furthermore, animal studies, conference abstracts, and studies lacking a clear description of an educational intervention were not considered for inclusion. This review did not include books and book chapters, as our search was restricted to peer-reviewed journal articles indexed in major electronic databases.
Search Strategy
To systematically gather pertinent literature, searches were executed across a spectrum of electronic databases with no limitation on the publication period, extending up to November 2024. These databases included PubMed, Scopus, CINAHL, EMBASE, Google Scholar, and Web of Science. The search strategies were designed to encapsulate terms relevant to “Parkinson’s Disease,” “Deep Brain Stimulation,” and educational aspects, ensuring the inclusion of a wide array of studies relevant to the topic (see Supplemental Table S1). In PubMed, a combination of MeSH terms and keywords in titles or abstracts yielded a total of 273 records. EMBASE utilized index terms and keywords in titles and abstracts to search for articles on PD and DBS related to education, resulting in 764 records. CINAHL integrated MeSH headings and keywords in titles or abstracts, capturing literature on PD, DBS, and various educational dimensions, identifying 76 documents. Scopus searched using index terms, uncovering 60 relevant documents. Web of Science combined search terms, leading to the identification of 790 records. Google Scholar focused on title searches that included keywords that identified 739 documents.
Study Selection Process
Identified articles were aggregated and uploaded to the reference management tool Zotero, where duplicate entries were subsequently eliminated. Following this preliminary step, 2 authors independently reviewed the titles and abstracts of the records using the Rayyan software (Rayyan Inc., Cambridge, MA, USA) in a blinded review process. 21 This step facilitated the identification of records potentially eligible for inclusion. Subsequently, the full texts of these articles were meticulously examined to determine their suitability for inclusion in the study. In instances of disagreement regarding eligibility, discussions were conducted until a consensus was reached among the research team members. The outcomes of this search and selection process were documented following the guidelines provided in the PRISMA-ScR. 19
Initially, a total of 2727 records were identified from databases including PubMed, CINAHL, Embase, Web of Science, Scopus, and Google Scholar. From these, 344 duplicate records were removed before screening. The remaining 2358 records were screened, leading to the exclusion of 2311 records. Further refinement during the retrieval process resulted in 47 reports being considered for full-text review. Of these, 5 reports were not retrieved, and 35 were excluded after assessment for eligibility due to discrepancies such as incorrect outcomes (n = 25) or inappropriate publication types (n = 11). Ultimately, 7 studies met the inclusion criteria and were incorporated into the review for a comprehensive analysis (Figure 1).
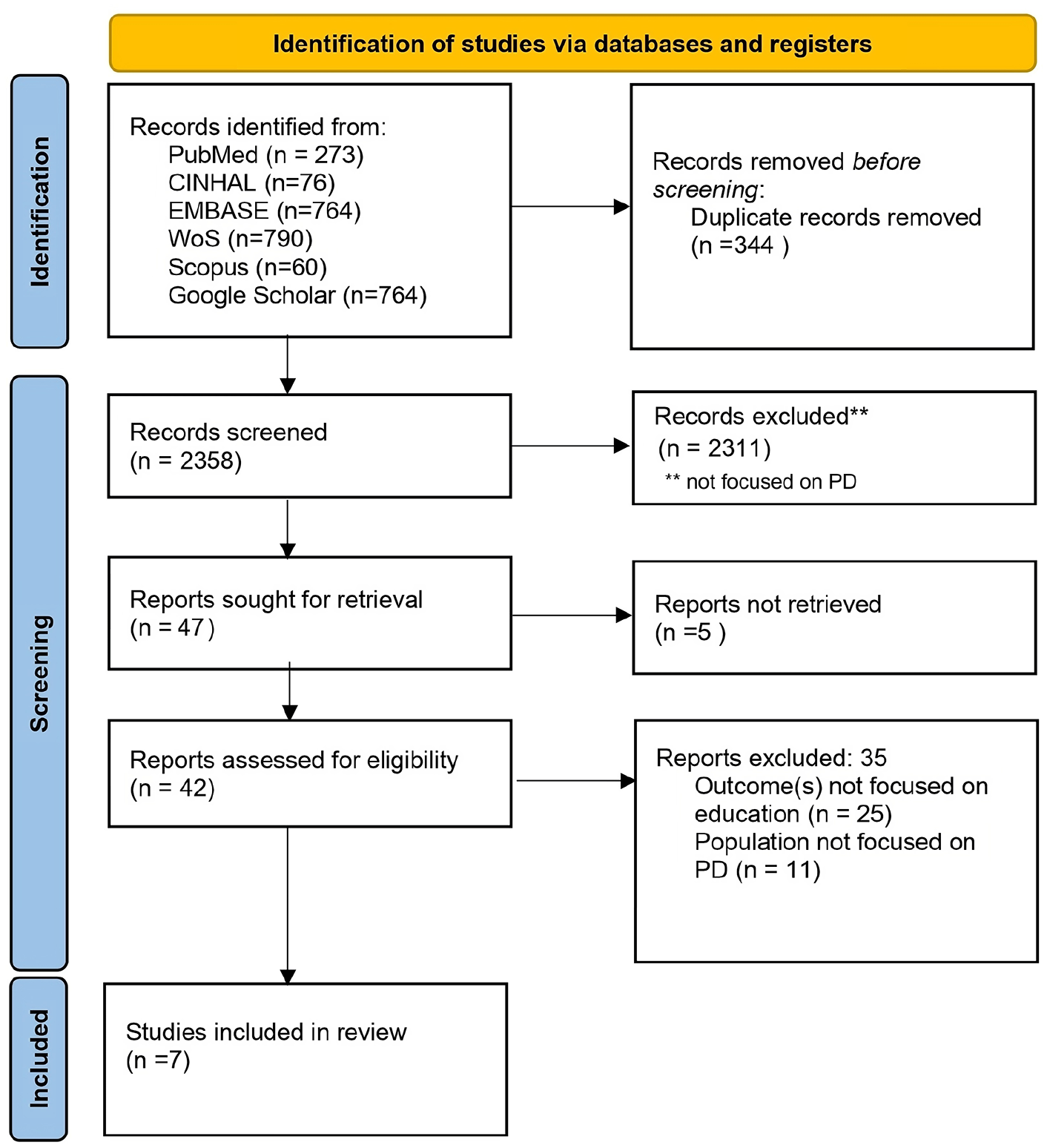
Study inclusion flow diagram.
Data Extraction and Analysis
The authors extracted data from all selected studies using a custom Excel spreadsheet designed for this purpose. The extracted information covered several aspects, including the first author’s name, publication year, country of origin, methodology of knowledge synthesis, objectives, research focus or characteristics of the educational program, demographic and clinical characteristics of the population or sample, the health professionals responsible for delivering the educational program, and the key findings and outcomes or patient-reported outcomes.
Consistent with the methodologies employed in a scoping review, 17 this study did not undertake a risk-of-bias assessment for the included studies. This decision aligns with the nature of scoping reviews, which aim to map the evidence available on a particular topic broadly and inclusively rather than critically evaluating this evidence’s quality or synthesizing results in a detailed manner, as seen in systematic reviews and meta-analyses. Therefore, evaluating the risk of bias, a common step in systematic reviews to assess the reliability and validity of the included studies, was deemed outside of the scope of this review’s objectives. This approach ensures that the analysis remains in line with the established methods for conducting a scoping review, focusing on identifying and summarizing available evidence to highlight gaps in knowledge and areas for future research. The analysis of the included documents and the emerging results were presented in alignment with the framework delineated by the subquestions that guided the objectives of the review, ensuring structured and focused dissemination of findings.
Results
Characteristics of Included Studies
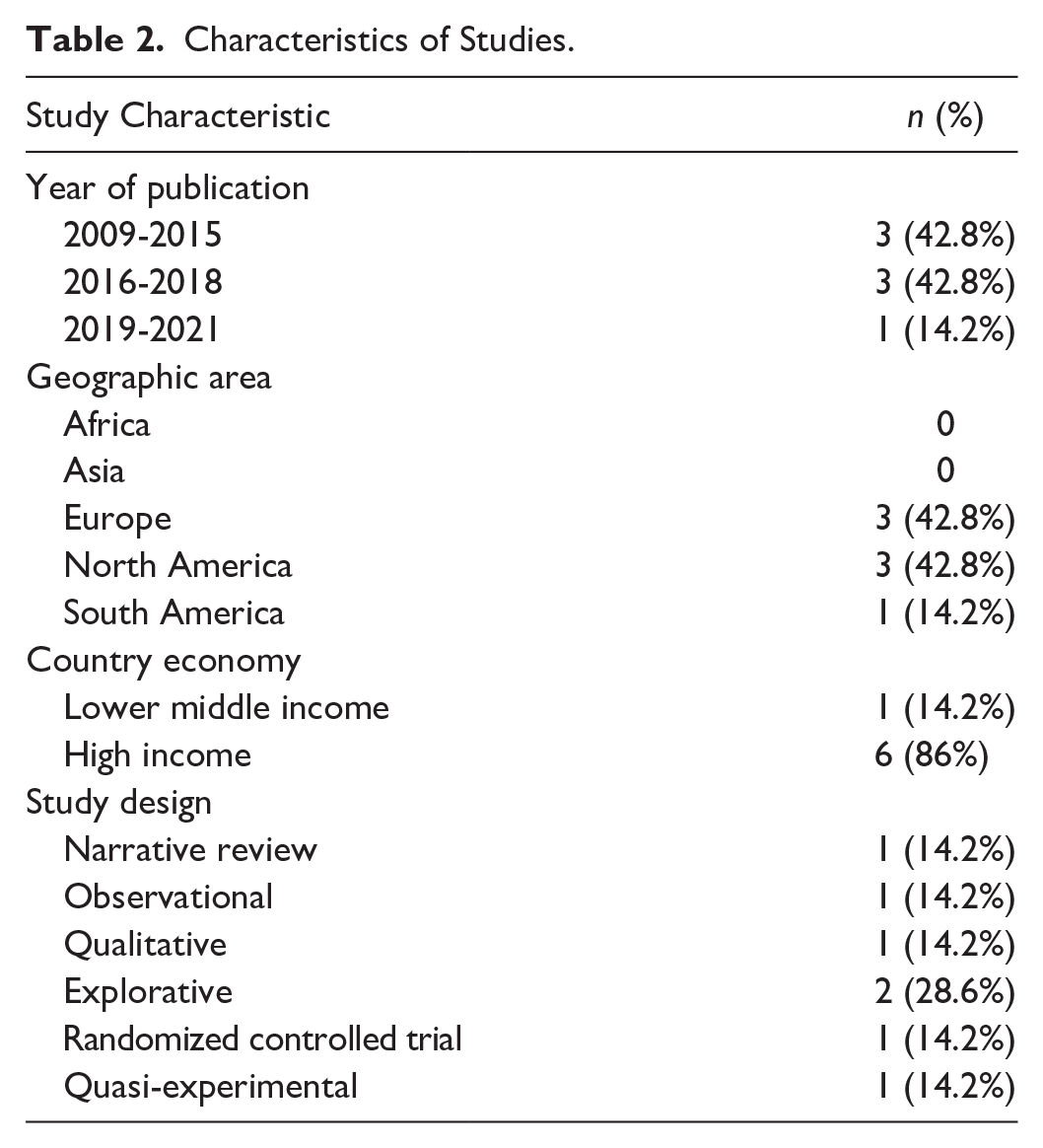
The studies analyzed were primarily published between 2011 and 2021, with the majority of contributions originating from Europe and North America (each accounting for 42.8% of publications) and South America (14.2%), as illustrated in Figure 2. High-income countries were responsible for 86% of the research output (n = 6). All included papers were original journal articles. The prevalent study designs encompassed explorative studies (n = 2), randomized controlled trials, qualitative studies, narrative reviews, and quasi-experimental studies, each constituting 14.2% (n = 1) of the total, as detailed in Table 2.
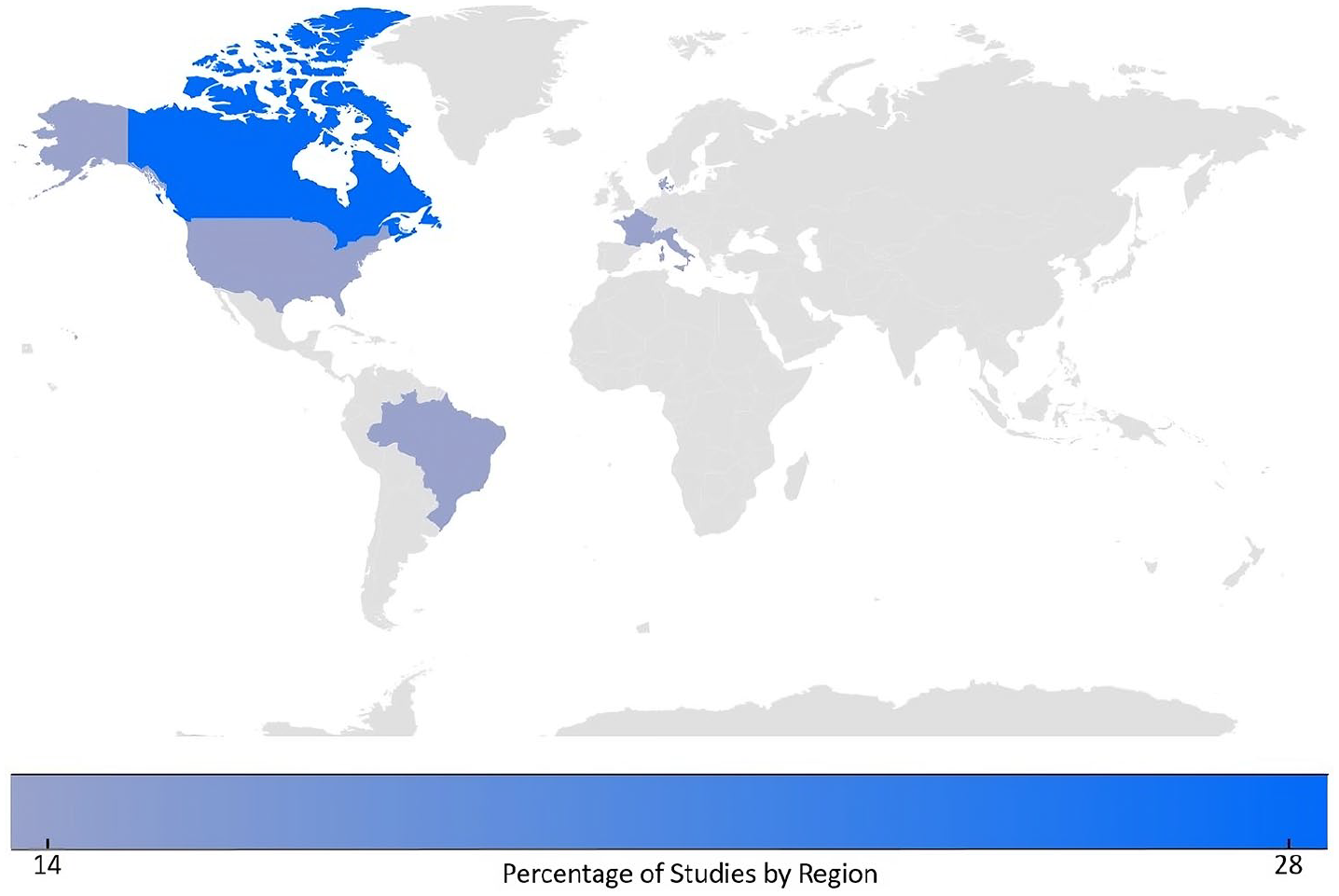
Heat map of study distribution across the globe.
Characteristics of Studies.
Overview of Educational Interventions for DBS in PD
Figure 3 depicts the synthesis of findings, offering a structured overview that elucidates the characteristics of educational programs (RQ1), the types of materials employed (RQ2), the professionals involved in delivering these programs (RQ3), and the outcomes for patients and caregivers (RQ4). This map serves as a comprehensive guide that reflects the analysis of the included studies (see Table 3) to grasp the full breadth of educational strategies and their pivotal role in patient care, as described below.
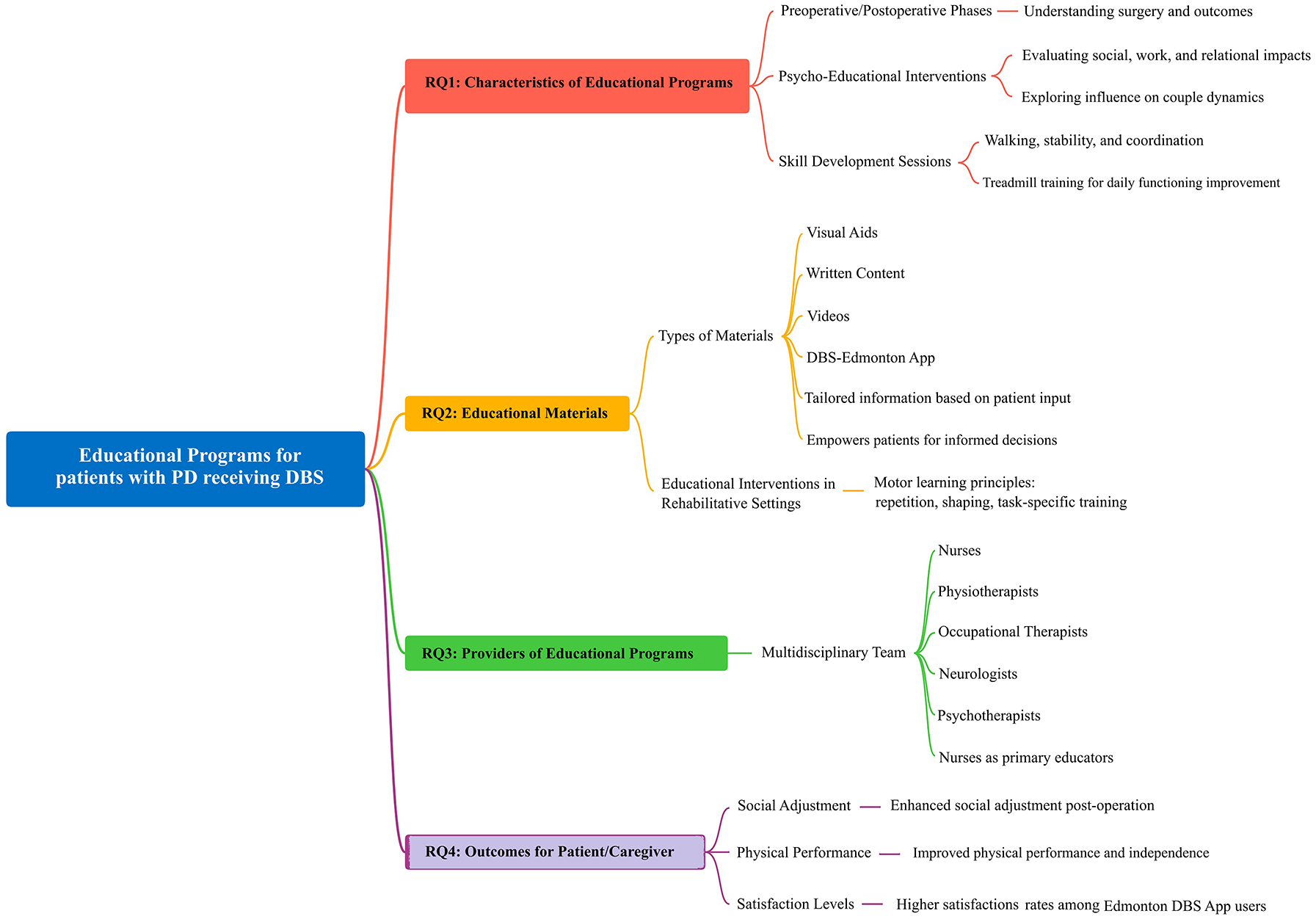
Map of the emerging results.
Study Characteristics.
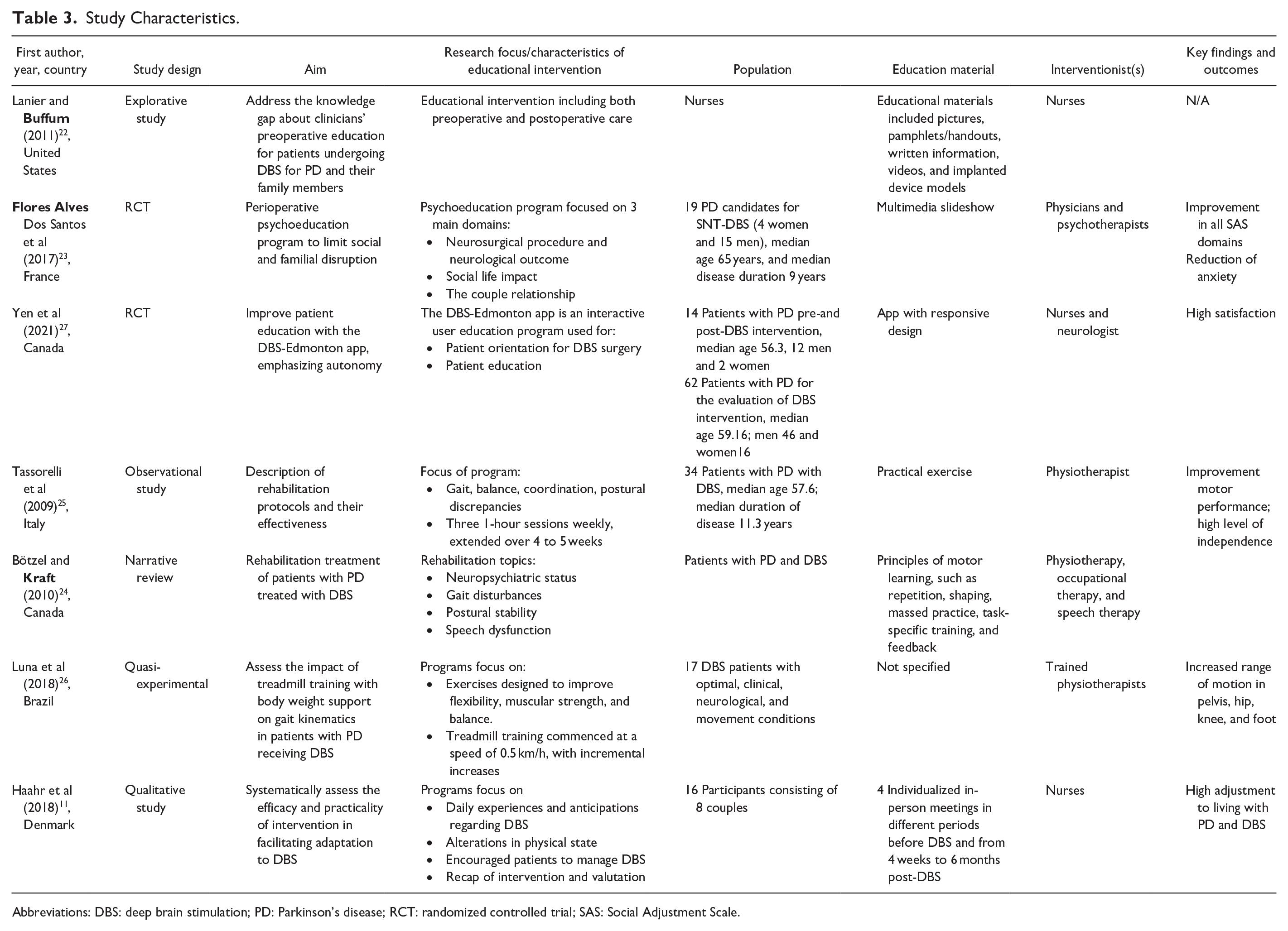
Abbreviations: DBS: deep brain stimulation; PD: Parkinson’s disease; RCT: randomized controlled trial; SAS: Social Adjustment Scale.
RQ1: Characteristics of Educational Programs
As shown in Table 3, the literature emphasizes the necessity for educational interventions across various stages of DBS treatment for PD, including the preoperative and postoperative phases. 22 Such interventions are pivotal for managing complications associated with DBS surgery, addressing potential changes in both mental and physical states. 22 Psycho-educational interventions during the perioperative period are deemed essential, focusing on 3 primary areas: understanding the surgery and its outcomes to align with patient and caregiver expectations; evaluating the social, work, and relational impacts of DBS; and exploring the influence on couple dynamics. These comprehensive approaches are designed to support patients in navigating the complexities of DBS treatment, enhancing their overall well-being and satisfaction levels. 23
The creation of the DBS-Edmonton app in Canada signifies an innovative approach to patient education, aiming to empower patients by providing tailored information based on their input, thereby facilitating informed decisions regarding DBS placement. 24 Similarly, educational programs in Italy underscore the importance of developing new skills, such as walking, stability, and coordination, through structured physical therapy sessions. 25 This focus on rehabilitation is echoed in Brazilian programs, which incorporate treadmill training to improve physical attributes essential for daily functioning. 26
Moreover, Danish research highlights an educational program that assists patients and caregivers through several critical stages of their DBS journey, from decision-making to adapting to postsurgery. 11 This holistic approach underscores the significance of structured support systems in enhancing patient autonomy and care management capabilities.
RQ2: Educational Materials
Within this scoping review, 6 studies out of 7 highlighted the diverse educational materials employed in programs for patients undergoing DBS treatment for PD (see Table 3). Lanier and Buffum identified a range of instructional resources, including visual aids, written content, and videos, to facilitate learning. 22 Furthermore, these studies emphasized the importance of personalized interactions, utilizing direct teaching methods and, where applicable, telemedicine to enhance patient education. 11
The use of the DBS-Edmonton app stands out as a notable innovation in patient education, offering a responsive, interactive platform for patients to understand their treatment better and manage their condition. This app allows patients to input symptoms, identify their most troubling issues, and access tailored information, significantly contributing to informed decision-making and patient autonomy. 27
Additionally, the review highlights educational interventions in rehabilitative settings, emphasizing the critical role of motor learning principles such as repetition, shaping, and task-specific training. These approaches are fundamental in helping patients improve motor skills and adapt to life with PD and DBS, underscoring the value of practical exercises and feedback in the learning process. 24
RQ3: Providers of Educational Programs
Educational interventions for patients undergoing DBS treatment for PD are delivered by a multidisciplinary team, as evidenced in the literature. Nurses play a pivotal role in this educational process and are directly involved in 3 studies that were reviewed.11,22,27
Additionally, physiotherapists, occupational therapists, neurologists, and psychotherapists contribute significantly to imparting education, highlighting the collaborative nature of patient care. Specifically, the studies by Lanier and Buffum and Yen et al emphasize the nurse’s role as a primary educator in managing DBS, underscoring the nurse’s expertise in navigating the complexities of DBS treatment and its impact on patients’ lives.22,27
RQ4: Patient and Caregiver Outcomes of Educational Programs
Findings from the reviewed literature indicate that within 1 to 2 years postoperation, both caregivers and patients with PD undergoing DBS treatment who participate in educational interventions show enhanced social adjustment as assessed by the Social Adjustment Scale (SAS). 23 Additionally, there is evidence of improved physical performance among these patients, contributing to greater independence.25,26 Furthermore, users of the DBS-Edmonton app experienced higher satisfaction rates than nonusers, suggesting that the app effectively contributes to better disease management and potentially enhances disease-modifying practices.11,27
Discussion
This review addressed the need to consolidate the fragmented knowledge surrounding educational programs for patients with PD undergoing DBS. The comprehensive assessment of available literature indicates that well-structured educational interventions play a crucial role at various stages of the DBS treatment process. Our synthesis of the data underscores that tailored educational materials and the involvement of a multidisciplinary team are instrumental in enhancing patient and caregiver outcomes.23,24 Notably, innovative tools such as the DBS-Edmonton app have been shown to empower patients in their treatment decisions. 27 Overall, the review highlights the significant benefits of education in helping patients adapt to the changes brought about by PD and DBS, particularly regarding social reintegration and psychological well-being. 23 With these insights, our findings reveal that such initiatives could significantly enhance social adaptation and mitigate anxiety in managing the disease, highlighting the profound impact of education on patient well-being. 23
Addressing the educational needs of patients with PD undergoing DBS is vital for ensuring optimal outcomes throughout the treatment continuum. 22 The research emphasizes that education should be tailored and integrated into every phase of the DBS journey—from preoperative preparation to postoperative care—to manage the treatment’s physiological and psychological complexities effectively. 22 Studies demonstrate that educational programs have evolved to include a variety of tools and approaches, from traditional materials to innovative technologies like the DBS-Edmonton app, which offers personalized guidance and support. 24 Furthermore, incorporating physical rehabilitation into educational curricula, such as in Italian and Brazilian studies, supports patients in regaining and enhancing motor functions, a key component of maintaining independence.25,26 The involvement of a multidisciplinary team, including nurses, therapists, and neurologists, contributes to a well-rounded educational strategy that addresses diverse aspects of living with PD and DBS. 11 Collectively, these educational interventions are shown to foster significant improvements in social reintegration and mental health, underscoring the transformative potential of education in patient care. 23
The array of educational materials available to patients undergoing DBS for PD indicates a broader shift toward patient-centered care, where information is not only shared but individualized to meet each patient’s unique needs. 22 Integrating varied instructional resources, from visual aids to immersive videos, enhances the learning experience and ensures that patients have access to information in a format that resonates with them. The DBS-Edmonton app exemplifies technology integration in patient education, merging responsiveness with interactivity, which aligns with the modern health care emphasis on patient engagement and self-management. 27 This reflects a trend toward digital health solutions that empower patients; this trend is also echoed in the wider literature that advocates for using health technologies to support chronic disease management. 28
Incorporating principles of motor learning into educational programs, as observed in rehabilitative settings, aligns with evidence suggesting that active participation and practice are key to skill acquisition in patients with PD. 24 Such an approach is supported by research indicating that motor learning strategies are effective in neurological rehabilitation, providing patients with the tools to maintain and improve motor function, which is crucial for independence. 29 The emphasis on repetition, shaping, and task-specific training not only aids in consolidating motor skills but also fosters a sense of progress and autonomy in patients. Through this lens, educational materials serve as both a source of knowledge and a means to facilitate active learning and engagement in the therapeutic process.
In this context, the role of nurses and other health professionals in providing educational interventions for patients with PD undergoing DBS is multidimensional and underscores the importance of interprofessional collaboration and team functioning.30,31 The literature consistently highlights that nurses, by virtue of their training and roles, often serve as primary educators, navigators, and liaisons for patients and their families throughout the DBS treatment journey.11,22,27 The efficacy of educational programs in health care, particularly for complex interventions like DBS, could be significantly enhanced when delivered by a multidisciplinary team. 32 This approach ensures that patients receive a comprehensive education that addresses all aspects of their care, including physical rehabilitation, psychological support, and disease management. Such a team typically includes nurses and physiotherapists, occupational therapists, neurologists, and psychotherapists, each contributing their expertise to create a cohesive educational experience for the patient. The emphasis on nurses and interprofessional collaborative practice in the literature aligns with broader health care trends promoting team-based care to provide comprehensive, patient-centered services. 33 Additionally, this is particularly important in the context of chronic conditions like PD, where managing the disease is complex and multifaceted.
In the included literature, the outcomes related to educational programs for patients with PD receiving DBS underline a significant improvement in the quality of life for both patients and caregivers.23,25 -27 Enhanced social adjustment, as measured by the SAS, highlights education’s positive impact on patients’ ability to reengage with their social environment following surgery. 23 This improvement in social functioning is critical, as it aligns with the goals of DBS to alleviate motor symptoms of PD and enhance overall well-being. Physical performance improvements post-DBS suggest that educational interventions could play a pivotal role in rehabilitation, potentially accelerating recovery and enabling patients to regain a level of independence that PD had previously compromised.25,26 This aspect of physical rehabilitation is essential, as it contributes to the autonomy of PD patients, allowing them to perform daily tasks more effectively, reducing caregiver burden and improving the quality of life for both parties. The increased satisfaction rates reported by users of the Edmonton DBS app indicate that patient-centered technological solutions are a valuable addition to traditional educational methods.11,27 The app’s ability to facilitate informed decision-making and provide tailored information addresses the growing demand for personalized health care tools that empower patients in the management of their conditions.
Limitations
This scoping review presents some limitations that warrant discussion. One such limitation may be the potential for publication bias, as studies with positive outcomes are more likely to be published, which could skew the overall perception of the effects of these educational programs. Another limitation is the heterogeneity of the educational interventions studied, ranging from innovative apps to more traditional methods like pamphlets and direct teaching. This variability makes it challenging to directly compare the interventions or to determine the best practices across different health care settings. The inclusion criteria and the sources of literature could also serve as a limitation. The review focused on studies published in English, which may overlook valuable research published in other languages and potentially relevant findings that could contribute to a more comprehensive understanding of the topic. Additionally, books and book chapters were not included in this review, as our search was restricted to peer-reviewed journal articles indexed in major electronic databases. While this approach ensured the inclusion of contemporary empirical research, it may have excluded valuable insights from books that provide historical context, theoretical foundations, or practical guidance on educational interventions for patients with PD undergoing DBS. Future research could consider integrating book-based literature to enhance the comprehensiveness of evidence synthesis.
Moreover, the reliance on self-reported measures such as the SAS for outcomes may introduce subjective bias, as these are based on the individual’s perception, which various external factors could influence. Lastly, the studies included were predominantly from high-income countries, which may not reflect the experiences or resources available in low- to middle-income countries. This aspect could limit the generalizability of the findings to a global context. Despite these limitations, the review provides critical insights into the role of education in managing PD and DBS, highlighting the need for further research to establish standardized educational protocols and assess their long-term impact on patient outcomes.
Conclusions
This scoping review synthesizes evidence on the role of educational interventions for patients with PD undergoing DBS treatment. The findings underscore the importance of personalized, multidisciplinary educational approaches encompassing various stages of the DBS treatment continuum, while the evidence is still limited. Innovative tools like the DBS-Edmonton app, alongside traditional educational materials, have been instrumental in empowering patients, facilitating better disease management and enhancing patient autonomy. Integrating motor learning principles into rehabilitative education further supports patients in improving motor functions, which is crucial for maintaining independence. Educational interventions represent a critical component of the care continuum for patients with PD receiving DBS, with significant implications for improving outcomes. Clinicians and researchers alike must continue to innovate and evaluate these programs’ efficacy to support this patient population’s evolving needs.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251341814 – Supplemental material for Education Programs for Patients With Parkinson’s Disease Receiving Deep Brain Stimulation: A Scoping Review
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251341814 for Education Programs for Patients With Parkinson’s Disease Receiving Deep Brain Stimulation: A Scoping Review by Monica Petralito, Chiara Tedesco, Gianluca Pucciarelli, Francesco Fanari, Arianna Magon, Stefano Terzoni, Maura Lusignani and Rosario Caruso in Western Journal of Nursing Research
Footnotes
Author Contributions
Study design: MP, RC. Data collection: MP, RC. Data analysis: RC. Study supervision: RC. Manuscript writing (draft): all the authors. Manuscript writing (editing and revision): all the authors. Critical revisions for important intellectual content: all the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This was a review study. No primary data were collected from human participants for this work. Institutional review board/ethics committee review and informed consent were not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.