
Abstract
People with Parkinson's disease (PwPD) who undergo deep brain stimulation (DBS) surgery could benefit from remote programming (RP), which has proven to be both effective and economical. However, there is limited research on PwPD with DBS implants who have completed all programming sessions exclusively through remote means (full remote programming, FRP). This case report documents the experiences of five PwPD who underwent FRP, with four demonstrating improvements in motor symptoms, quality of life, and medication reduction. A total of 22 postoperative programming sessions were conducted, all via RP. FRP integrates RP with online consultations. Our findings contribute preliminary evidence supporting the feasibility and safety of FRP in the postoperative care of PwPD with DBS implants.
Introduction
Deep brain stimulation (DBS) is one of the established surgical interventions for refractory Parkinson's disease (PD).1,2 Remote Programming (RP) is a safe and effective technology to adjust the settings of Implantable Pulse Generators (IPGs) via the Internet for patients who have underwent DBS surgery. 3 For those patients living far away from specialized centers, completing all the postoperative programming sessions via RP (Full Remote Programming, FRP) offers a cost-effective solution.
Despite its potential, research on the efficacy and safety of FRP remains limited. A prior study involving 23 people with Parkinson's disease (PwPD) reported satisfactory clinical outcomes with FRP, though it did not detail improvements in motor functions. 4
This study retrospectively follows five PwPD who underwent FRP for the first time, aiming to contribute evidence on the feasibility and safety of FRP in the postoperative management of PwPD with DBS implants.
Case description
FRP
FRP comprises two parts: RP and online consultation. At each scheduled RP session, physicians connect to the IPGs via the internet. Electrode positions are confirmed using fused images from postoperative CT and preoperative MRI scans. Physicians guide patients through various movements to adjust the IPG settings based on observed motor performance. Initial programming for contact screening was also performed via RP. While rigidity cannot be evaluated remotely, visually assessable symptoms such as tremor and bradykinesia are monitored for amplitude adjustments. Additionally, assessments of speech, gait, and movement from a seated position are evaluated. When a new parameter setting is established, the previous setting is saved in case the newer setting is not tolerated over the long term. Patients are also allowed to fine-tune the voltage settings within a prescribed range.
Online consultations complement RP, allowing patients to report symptoms to doctors via communication software, either in video or text format. Doctors could then provide corresponding advice on these reported issues.
Participants
Following a review of treatment histories, five patients were included. All of them had undergone bilateral subthalamic nucleus DBS at Ruijin Hospital in 2022. Clinical outcomes were collected at our center at baseline and during follow-up visits, which included the Movement Disorder Society (MDS)-Unified Parkinson's Disease Rating Scale part III (UPDRS-III) scores, 5 the Chinese version of 8-item Parkinson's disease Questionnaire (PDQ-8) score, 6 and the levodopa equivalent daily dose (LEDD). Higher scores on the UPDRS-III and PDQ-8 indicate poorer motor function and quality of life, respectively. The interval and method of each programming session varied among patients, typically based on their subjective symptoms and personal preferences.
Of the participants, two were female (Table 1). The mean (± SD) age at surgery was 55 ± 11 years, with a follow-up interval of 13 ± 5 months, and an average distance of 582 ± 346 km from their residences to our center. Preoperative UPDRS-III scores averaged 53 ± 12 points, with a 49 ± 15% improvement observed during the preoperative levodopa challenge test (LCT). 7 At follow-ups, with DBS stimulation ON and medication OFF, four patients showed significant improvements in motor symptoms and quality of life, with reductions of over 30% in both UPDRS-III and PDQ-8 scores (Table 2). The exception was Patient 5, who experienced a worsening of motor symptoms. All participants reduced their LEDD by more than 40%.
Characteristics of patients at baseline.

Abbreviation: M, months; Y, years; FU, follow-up interval; UPDRS-III, The Movement Disorder Society Unified Parkinson's Disease Rating Scale—part III; LR, Levodopa responsiveness in the levodopa challenge test; LEDD, Levodopa equivalent daily dose; PDQ-8, The 8-item Parkinson's Disease Questionnaire.
Clinical outcomes at follow-ups.
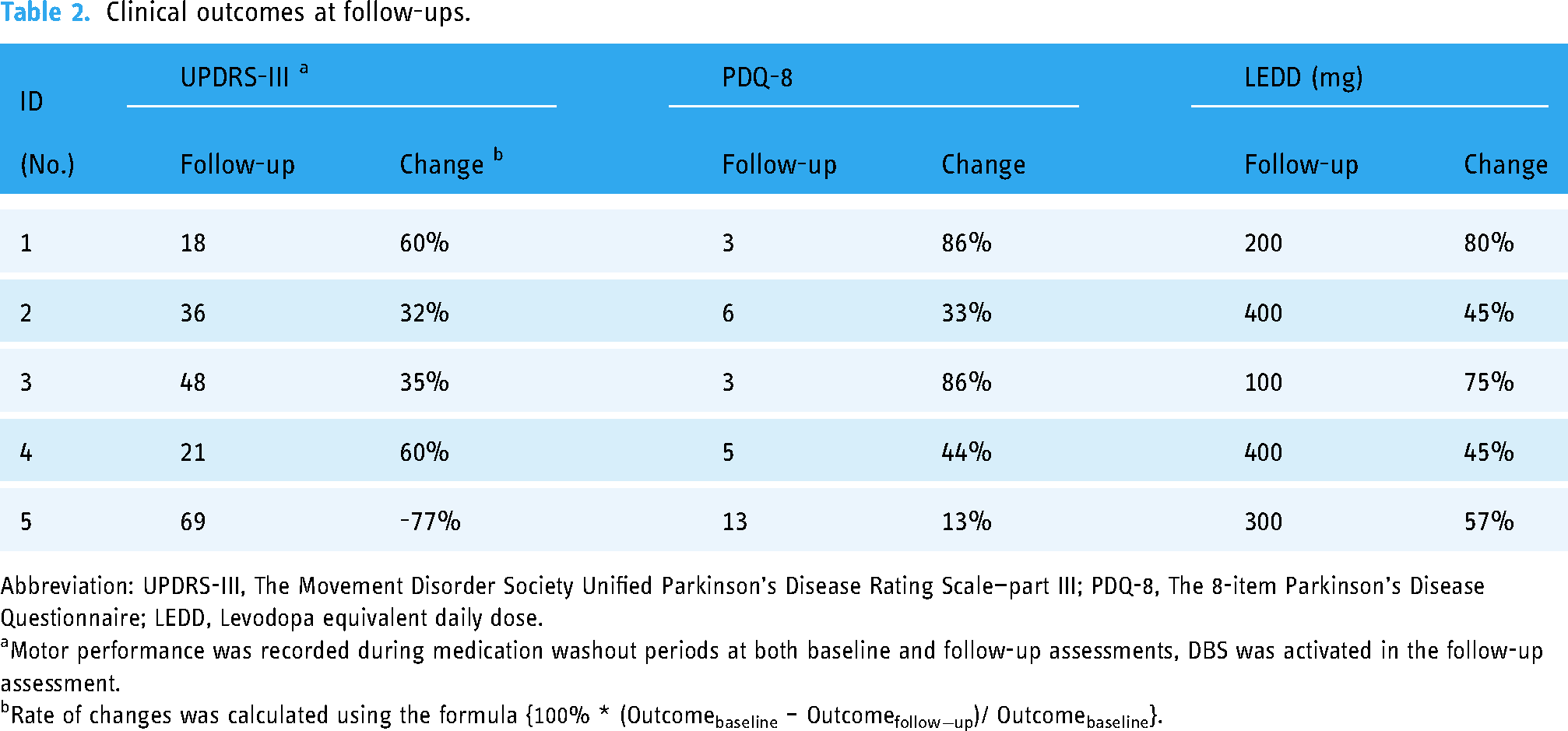
Abbreviation: UPDRS-III, The Movement Disorder Society Unified Parkinson's Disease Rating Scale—part III; PDQ-8, The 8-item Parkinson's Disease Questionnaire; LEDD, Levodopa equivalent daily dose.
Motor performance was recorded during medication washout periods at both baseline and follow-up assessments, DBS was activated in the follow-up assessment.
Rate of changes was calculated using the formula {100% * (Outcomebaseline – Outcomefollow−up)/ Outcomebaseline}.
Before the follow-ups, five patients underwent postoperative programming via FRP an average of 4.4 times annually following DBS (Table 3). After the initial programming, the most commonly adjusted parameter was voltage, while changes to electrode contact were the least frequent. Additionally, 15 online consultations were recorded, with voltage adjustment being the most frequently common topic, while device-related problems were the least frequent. No unexpected network disconnections occurred during these sessions.
History of RP and online consultation sessions a.

Abbreviation: Volt., Voltage; Freq., Frequency; P.W., Pulse Width; Med, Medication; DRC., Device Related Consultations.
Table 3 reports the count of all remote programming sessions and online consultation. Additionally, the changes of each parameter and the topic of each online consultations were also recorded.
The change between electrode contacts.
Discussion
This study highlights the continued preference for FRP among PwPD with DBS, even post-COVID-19 restrictions, indicating high satisfaction with this method. Patient 5 discontinued FRP after the follow-up, she experienced worsening motor symptoms following an allergic reaction and the development of urinary retention three months prior to follow-up. Those problems unlikely linked directly to the DBS programming.
Satisfactory improvements in QoL might be the reason for the continuation of FRP in these PwPD, with an average 53% reduction in PDQ-8 scores. Particularly, Patients 1 and 3, who continued working normally, showed the greatest QoL improvements (86% reduction). Current literature suggests that QoL improvements correlate more with daily living activities rather than motor impairments or complications. 8 Chen's study 4 found comparable clinical outcomes across three groups of PwPD with different postoperative programming methods (the RP alone group, the RP + SP group, the SP alone group), except for a more apparent medication reduction in the SP alone group. In our cohort, the four patients with improved motor symptoms saw a 47% average reduction in UPDRS-III scores, aligning with previous findings. 9 Moreover, two patients (P1 and P4) with greater levodopa response in LCT also demonstrated a stronger response to DBS, supporting the predictive value of preoperative LCT. 10
In addition to the treatment effect, cost also likely influenced the continuation of FRP. A Hungarian study indicated that, ten years after DBS implantation, the average cost of each travel-related expense amounted to approximately 922.7 Euros (≈1003.9 US dollars). 11 Given the average travel distance of over 500 kilometers for our patients, RP was notably more cost-effective.
During RP sessions, stimulation parameters were adjusted based on teleconference assessments of patient performance. Remote assessments during COVID-19 were well-received. 12 However, the inability to directly assess rigidity or balance was a shortcoming of RP. In this study, comprehensive motor symptoms were managed by addressing visually assessable symptoms, such as bradykinesia and tremor. However, these symptoms respond more slowly and their assessment may be biased by the patient's condition. 13 In this study, we observed each increment in amplitude for up to five minutes to thoroughly assess the full response to stimulation.
During FRP, online consultations complemented RP sessions. Some patients experienced effects like stimulation-induced dyskinesia, 14 which required timely treatment. Most of these issues could be resolved by minor adjustments in voltage or medication, making online consultations more suitable for such situations than visits for reprogramming.
Conclusions
Despite these challenges, the study confirms the feasibility and preliminary safety of FRP in managing DBS in Parkinson's disease patients, suggesting that it could be a viable long-term treatment option. The study's results, while promising, are constrained by its small sample size (n = 5) and the lack of a control group, categorizing the findings as Class IV evidence. The variability in the types of DBS devices and the platforms used for remote programming also add layers of complexity that could affect patient experiences and outcomes. Consequently, further research is essential to establish robust criteria for participant selection and to standardize the application of FRP. This would help in building more definitive evidence for FRP's efficacy and safety, ultimately guiding clinical practices for the better management of Parkinson's disease through technological advancements in DBS programming.
Footnotes
Acknowledgements
We thank all the patients for participating in this study. We are grateful to Dr Haiyan Zhou for her invaluable feedback and critical comments that significantly improved the manuscript.
Author contributions
XW: Data curation, Writing – original draft. ZL: Data curation, Formal Analysis. ZZ: Writing – review and editing. CD: Writing – review and editing. CZ: Writing – review and editing. DL: Conceptualization, Supervision, Writing – review and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article: This study was funded by the Shanghai Municipal Health Commission [grant Number 202140181 to DL], the Shanghai Science and Technology Commission [grant Number 22Y11903900 to DL], and Guangci Innovative Technology Launch Program [GCQH202205 to DL].
Patient consent and Ethical approval
Written informed consent for the research was obtained from all participants prior to their follow-up. The study protocol was approved by the Ethics Committee of the Ruijin Hospital (Clinical Ethics Review (2023) No. 231) and adhered to the Declaration of Helsinki.