
Abstract
Background:
Diabetes complications are prevalent in people with diabetes, causing considerable individual suffering and increased health costs. However, the relationships of multidimensional, modifiable, and nonmodifiable factors to diabetes complications and the role of diabetes distress have been rarely examined.
Objective:
The aims of this study were to examine the associations of age, sex, knowledge, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, diabetes distress, social support, and body mass index with diabetes complications and to investigate the mediating role of diabetes distress.
Methods:
In this cross-sectional, correlational study, data on all study variables were collected from 148 people with diabetes through REDCap in 2023. Multiple regression analysis and the PROCESS macro for SPSS were used to address the aims.
Results:
Older age and higher levels of diabetes distress were associated with more diabetes complications. Depressive symptoms were associated with diabetes distress; and diabetes distress, but not depressive symptoms, was associated with diabetes complications, controlling for all other variables.
Conclusions:
Depressive symptoms and diabetes distress were directly or indirectly associated with diabetes complications, and diabetes distress was a mediator in the relationship between depressive symptoms and diabetes complications. Health care providers can target reduction of depressive symptoms and diabetes distress to reduce diabetes complications.
People with diabetes experience a high prevalence of diabetes complications, including macrovascular and microvascular complications.1,2 Macrovascular complications include angina pectoris, acute myocardial infarction, heart failure, and stroke.1,3 Microvascular complications include retinopathy, neuropathy, and nephropathy.1,3 Diabetes complications result in poor quality of life, high rates of hospitalization and mortality, and increased health care utilization and costs.3 -5 For example, new diagnoses of macrovascular and microvascular complications were associated with reduction in quality of life among people with type 2 diabetes in 30 countries. 3 The number of diabetes complications was almost linearly associated with the risks of hospitalization and mortality in people with diabetes. 4 In people with diabetes, the mortality rates in people without complications, one complication, and two or more complications were 5.4%, 7.3%, and 11.8%, respectively. 4 For Medicare beneficiaries, the costs for kidney transplantation, kidney dialysis, and lower extremity amputation at the first year were approximately $79 000, $54 000, and $39 000, respectively. 5 Therefore, prevention of and reduction in diabetes complication are critical.
Multidimensional Factors Associated With Diabetes Complications
To reduce diabetes complications, multidimensional modifiable factors affecting or associated with them should be identified comprehensively. Cognitive (ie, knowledge), psychosocial (ie, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, diabetes distress, and social support), and physiological factors (body mass index) can be associated with diabetes complications (Figure 1). Even though the direct relationship between knowledge and diabetes complications has not been frequently examined, people with diabetes have inadequate knowledge of diabetes complications, 6 which may adversely affect diabetes complications. The relationships of positive psychological factors, including self-efficacy, self-compassion, resilience, and self-esteem, to diabetes complications may exist, but their direct relationships have not been frequently examined. In one study, 7 lower levels of self-efficacy were associated with retinopathy. The direct relationships of self-compassion and resilience to diabetes complications have been rarely examined, but they may be associated with diabetes complications because of their effects on diabetes self-care.8,9 In one study of people with diabetes, 10 lower levels of self-esteem were associated with foot ulcer.
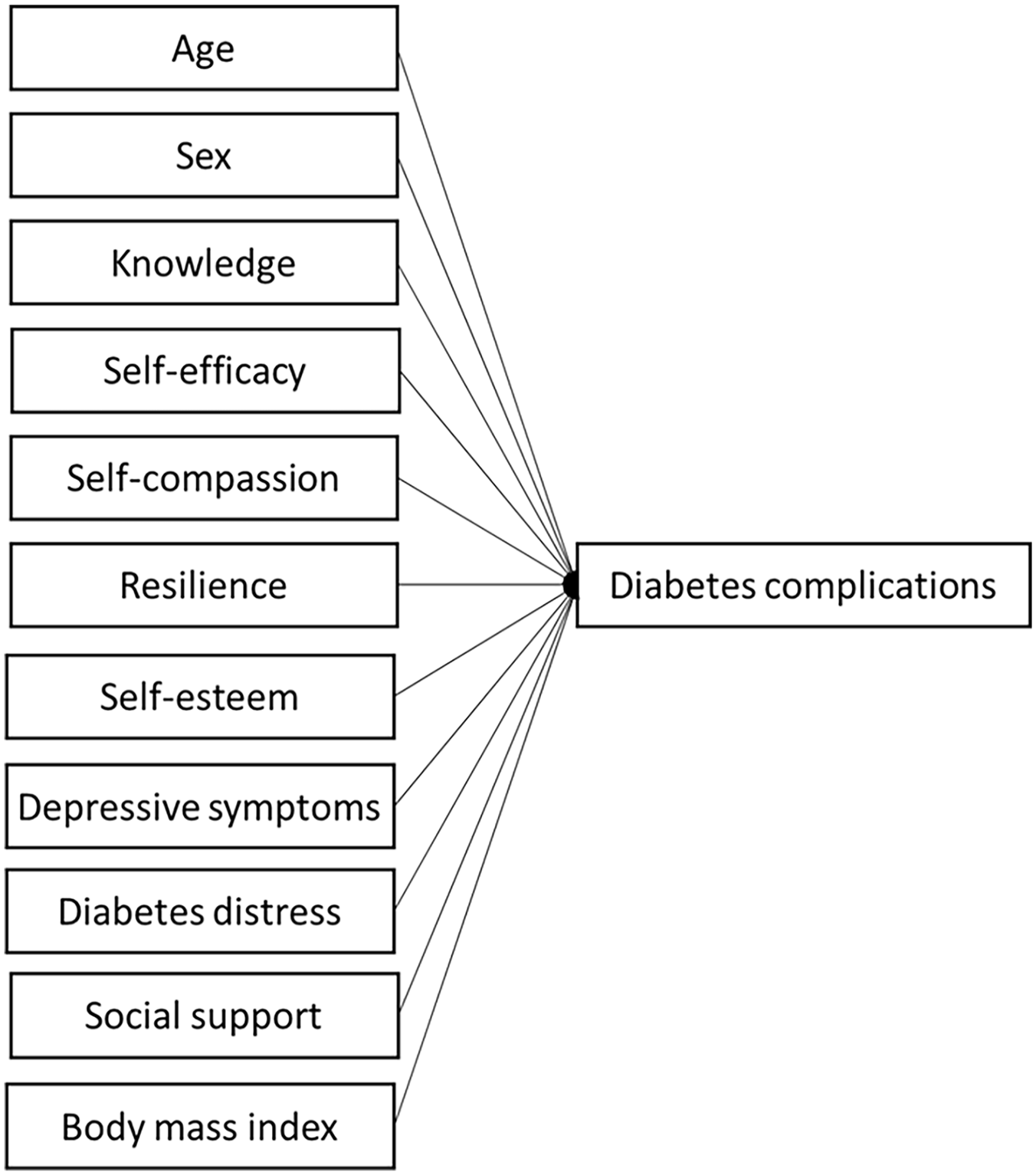
Theoretical framework: factors associated with diabetes complications.
The relationships of negative psychological factors, including depressive symptoms and diabetes distress, to diabetes complications have been examined in several studies of people with diabetes.11 -13 In two meta-analyses,11,12 depressive symptoms were associated with fatal or nonfatal cardiovascular disease-related events or nephropathy. Diabetes distress was associated with risk for progressing diabetic nephropathy in men. 13 Furthermore, depressive symptoms were associated with diabetes distress in people with diabetes.14,15 In particular, diabetes distress mediated the relationship between depressive symptoms and self-care in people with diabetes, but depressive symptoms did not mediate the relationship between diabetes distress and self-care. 14 These findings imply the mediating role of diabetes distress in the relationship between depressive symptoms and diabetes complications. However, these relationships have rarely been examined in people with diabetes, controlling for other modifiale factors.
Lower social support (fewer members in social network), which is a social factor, was associated with microvascular and macrovascular complications. 16 Higher body mass index, which is a physiological factor, was associated with diabetes retinopathy. 17 In addition, two demographic factors, older age and male sex, were associated with any types of cardiovascular diseases complications.18,19 All of these findings imply that multidimensional, modifiable, and nonmodifiable factors can affect development and/or worsening of diabetes complications. The comprehensive relationships of those multidimensional modifiable and nonmodifiable factors to diabetes complications have rarely been examined in a single study among people with diabetes. This examination is critically important to understand what factors should be focused on to reduce development or worsening of diabetes complications.
Purpose
The purpose of this study was to examine the associations of age, sex, knowledge, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, diabetes distress, social support, and body mass index with diabetes complications and the mediating role of diabetes distress in the relationship between depressive symptoms and diabetes complications (Figure 2).
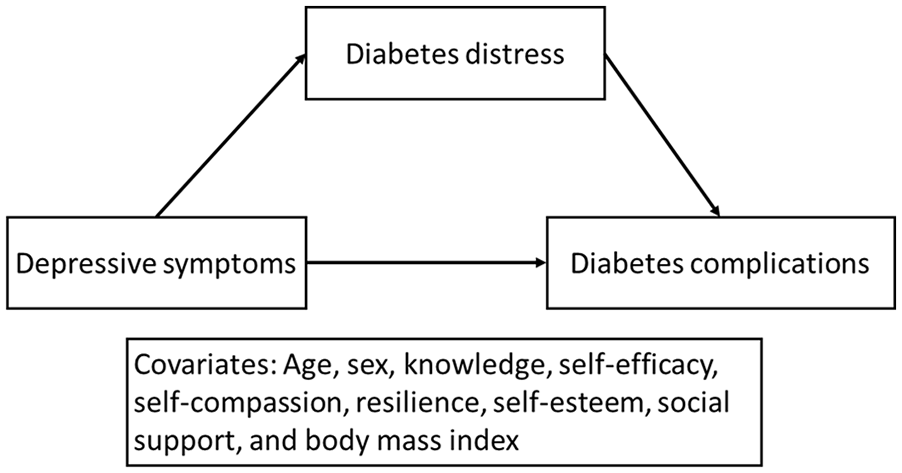
The hypothesized mediating role of diabetes distress.
Methods
Study Design and Setting
This was a cross-sectional, correlational study to examine the relationships of multidimensional modifiable and nonmodifiable factors to diabetes complications in people with diabetes. Study participants were recruited in the United States through a flyer, advertisement statements, recruitment emails, contact messages, and snowball sampling through various institutions, organizations, and individuals where people with diabetes could visit or be contacted. Recruitment was also done through ResearchMatch, which is a national health volunteer registry that was created by several academic institutions and supported by the US National Institutes of Health as part of the Clinical Translational Science Award (CTSA) program. ResearchMatch has a large population of volunteers who have consented to be contacted by researchers about health studies for which they may be eligible. 20 Review and approval for this study and all procedures was obtained from Mercer University Institutional Review Board.
Sample
The inclusion criteria were any types of diabetes based on self-report and adult people (≥18 years old). Exclusion criteria were non-English readers and no access of the survey link because of not having a smartphone, tablet, or computer. The sample size was calculated using G*Power.3.1.9.44. 21 In a meta-analysis, 12 the odds ratio of depressive symptoms predicting nephropathy in diabetes was 1.22 (effect size: 0.67). 22 We conservatively assumed an effect size of 0.15 (medium effect size) because of different variables and data analysis methods between the prior study and this study. Considering an effect size of 0.15, alpha of .05, power of 0.90, and 11 independent variables, the necessary sample size was 152.
Procedure
This study was approved by the Mercer University Institutional Review Board (IRB#: H2302037). Data collection was done through REDCap. Two hundred thirty-six people with diabetes started the survey, but 10 did not give their consent and did not start data collection. Forty-eight people gave online consent but did not start the data collection process. Thus, 178 people completed data collection. Among them, 30 cases were excluded because of missing data in ≥30% of the items in each scale with multiple items, one item variable (eg, age, sex, weight, or height), or the outcome variable (diabetes complications). Thus, 148 cases were included in this study.
Measurements
Diabetes complications referred to incidence(s) of 7 categories of diabetes-related complications.23,24 Diabetes complications were assessed by the Diabetes Complication questionnaire that was developed by the authors based on a prior study to use it for the online survey. 23 In the prior study, 23 considering 7 complications of cardiovascular disease, metabolic, nephropathy, neuropathy, peripheral vascular, retinopathy, and stroke, a higher number of diabetes complications was associated with higher odds of mortality during a 4-year follow-up period. The Diabetes Complication questionnaire assesses the 7 complications using response options of 0 (no) and 1 (yes). One example item is “As a result of diabetes, do you have any kidney problems, such as kidney infection, high urine protein, high creatinine, chronic kidney disease, renal failure, or hemodialysis?” Possible total scores range from 0 to 7, with higher scores indicating more diabetes complications.
Knowledge referred to people’s understanding of diabetes self-care and its effects. 25 Knowledge was measured using the Short Diabetes Knowledge Instrument (13 items). 25 Available response options for each item vary. An illustrative item with its respective response options is: When diabetes is not under control, the blood sugar: (a) is normal, (b) is high, (c) is low, (d) can be high or low, or (e) I don’t know. The correct response is scored as 1, while 0 is given for any incorrect responses or don’t know response. The potential total score range is 0 to 13, and higher scores indicate greater knowledge. In a prior study, 25 the reliability was supported with Cronbach’s alpha of 0.75, and the validity was supported with the significant correlation between education level and knowledge. Cronbach’s alpha in this study was 0.68.
Self-efficacy refers to the level of confidence that people have in managing diabetes self-care. 26 Self-efficacy was measured using the Perceived Diabetes Self-Management Scale (8 items). 26 Some items were reverse-coded. The potential total score range is 8 to 40, and higher scores reflect greater confidence in diabetes self-care. In a prior study, 26 the reliability was supported by a Cronbach’s alpha of 0.83, and the validity was supported by the significant correlation of self-efficacy to the number of self-care activities. Cronbach’s alpha in this study was 0.88.
Depressive symptoms referred to people’s diminished emotional function, characterized with feelings of sadness, low mood, and loss with some reduced physical function. 27 Depressive symptoms were measured using the Patient Health Questionnaire. 27 The potential total score range is 0 to 27, and higher scores reflect more severe depressive symptoms. In a prior study, 27 the reliability was supported by a Cronbach’s alpha of 0.87, and the validity was supported by acceptable structural validity in people with type 2 diabetes. Cronbach’s alpha in this study was 0.88.
Diabetes distress refers to people’s subjective perceptions of psychosocial burdens associated with diabetes and its management. 28 Diabetes distress was measured using the Diabetes Distress Scale (17 items). 28 The potential total score range is 1 to 6, and higher scores reflect more diabetes distress. In a prior study of people with diabetes, 28 the reliability was supported by a Cronbach’s alpha of 0.93, and the validity was supported by significant correlation between diabetes distress and depressive symptoms. Cronbach’s alpha in this study was also 0.93.
Self-compassion refers to people’s subjective perceptions of being supportive toward themselves during periods of suffering or pain. 29 Self-compassion was measured using the Self-Compassion Scale-Short Form (12 items). 29 The negative subscale items were reverse-coded before summing the total score. The potential total score range is 1 through 5, and higher scores reflect higher levels of self-compassion. In a prior study, 29 the reliability was supported by a Cronbach’s alpha of 0.86, and the validity was supported by acceptable structural validity in students and general populations. Cronbach’s alpha in this study was 0.87.
Resilience refers to people’s ability to bounce back from adversities.30,31 Resilience was measured using the revised version of the Connor-Davidson Resilience Scale (10 items). 30 The potential total score range is 0 to 40, and higher scores reflect greater resilience. In a prior study of people with lower limb amputation, 30 the reliability was supported by a Cronbach’s alpha of 0.89, and the validity was supported by the significant relationship between resilience and perceived functional capacity. Cronbach’s alpha in this study was 0.90.
Self-esteem refers to the extent of people’s subjective assessment of their own value or abilities. 32 Self-esteem was measured using the Rosenberg Self-Esteem Scale (10 items). 33 The potential total score range is 10 to 40, and higher scores reflect higher levels of self-esteem. In a prior study of people with diabetes, 34 reliability was supported by a Cronbach’s alpha of 0.90, and the validity was supported by the significant relationship between perceived competence in diabetes and self-esteem. Cronbach’s alpha in this study was 0.93.
Social support refers to people’s perceptions of assistance from family, friends, and significant others. 35 Social support was measured using the Multidimensional Scale of Perceived Social Support (12 items). 35 The potential total score range is 12 to 84, and higher scores reflect more assistance from others. In a prior study of people with diabetes, 36 the reliability was supported by a Cronbach’s alpha of 0.96, and the validity was supported by the significant relationship between social support and alexithymia. Cronbach’s alpha in this study was also 0.96.
Demographic characteristics were measured using a standard demographic questionnaire based on self-report of participants. Age, sex, marital status, education level, employment status, weight, and height were assessed. Race and ethnicity were also assessed based on the categories of Asian, African American, any other races, Hispanic, and White that the investigators defined. Any other races were those races that did not belong to other categories of race and ethnicity. Weight in pounds and height in feet and inches were transformed to kilograms and meters. Then, body mass index was calculated based on the following formula: weight (kg)/(height [m]) 2 .
Data Analysis
Descriptive statistics were used to describe sample characteristics and study variables using IBM SPSS Statistics for Windows (Version 29.0). 37 Two-tailed tests and P value <.05 were used for all the tests. Multicollinearity was checked using variance inflation factor, and there was no multicollinearity. Normal distribution was checked during multiple regression analysis based on residual analysis, and there was normal distribution. Multiple regression was used first to examine the relationships of demographic characteristics (ie, age and sex), a cognitive factor (ie, knowledge), 6 positive and negative psychological factors (ie, self-compassion, self-esteem, resilience, and self-efficacy; depressive symptoms and diabetes distress, respectively), a social factor (ie, social support), and a physiological factor (ie, body mass index) to diabetes complications. PROCESS macro for SPSS (version 4) 38 (Model 4) was used to examine the mediating role of diabetes distress in the relationship between depressive symptoms and diabetes complications, controlling for all other factors in the multiple regression model.
Results
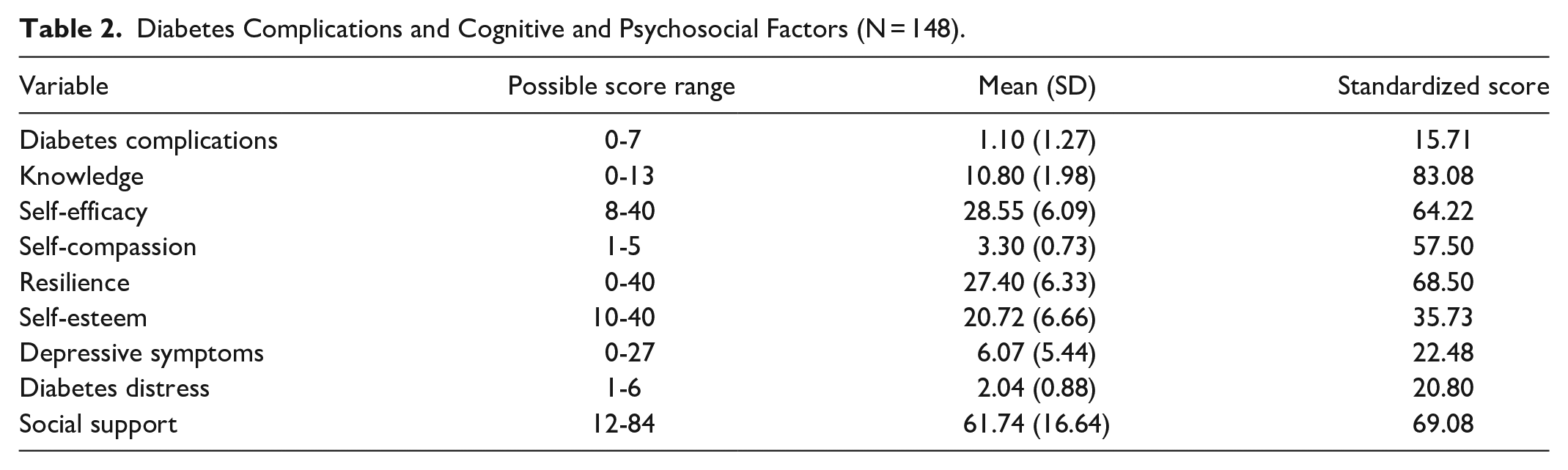
The sample characteristics are presented in Table 1. The mean age was 57.6 years, and mean body mass index was 30.6 kg/m2. Most of the participants were White (87.2%) and retired or full-time workers (83.1%). Slightly more than half (58.8%) were married. The mean number of diabetes complications was 1.1 (this information is not presented in Table 1). In the sample, 60.8% of people had at least one diabetes complication. Furthermore, 16.2% had 2; and 12.3% had 3 or more diabetes complications (this information is not presented in Table 1). Approximately 54.7% of people had microvascular complications, and 23.6% had macrovascular complications. The mean scores with the possible score ranges and the standardized scores of diabetes complications and cognitive and psychosocial factors are presented in Table 2. Based on the standardized scores, the mean score for knowledge was 83.08 out of 100. The mean scores of positive psychological factors were 64.22 for self-efficacy, 57.50 for self-compassion, 68.50 for resilience, and 35.73 for self-esteem. The scores of negative psychological factors were 22.48 for depressive symptoms and 20.80 for diabetes distress. The mean score for social support was 69.08.
Sample Characteristics (N = 148).
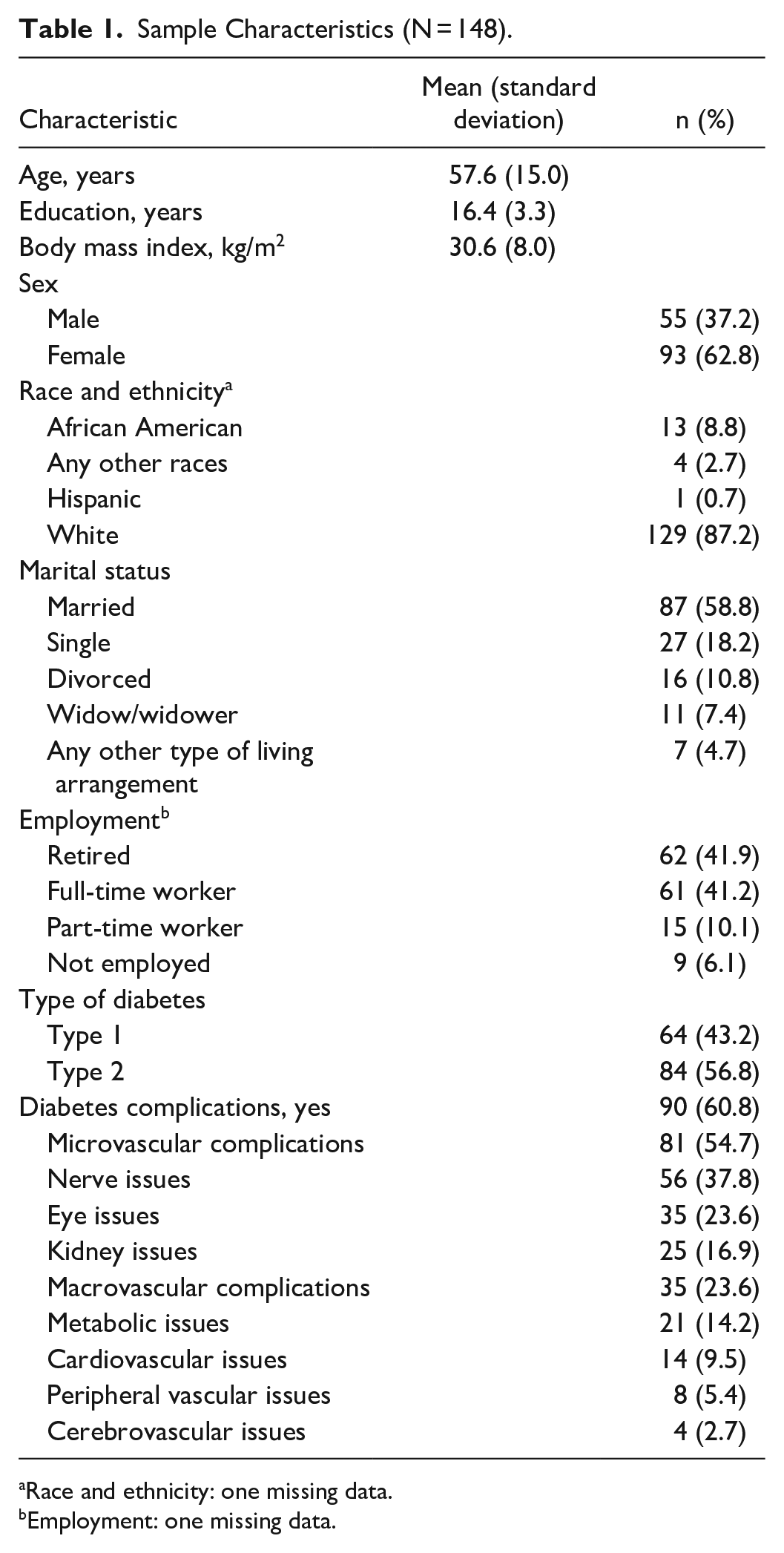
Race and ethnicity: one missing data.
Employment: one missing data.
Diabetes Complications and Cognitive and Psychosocial Factors (N = 148).
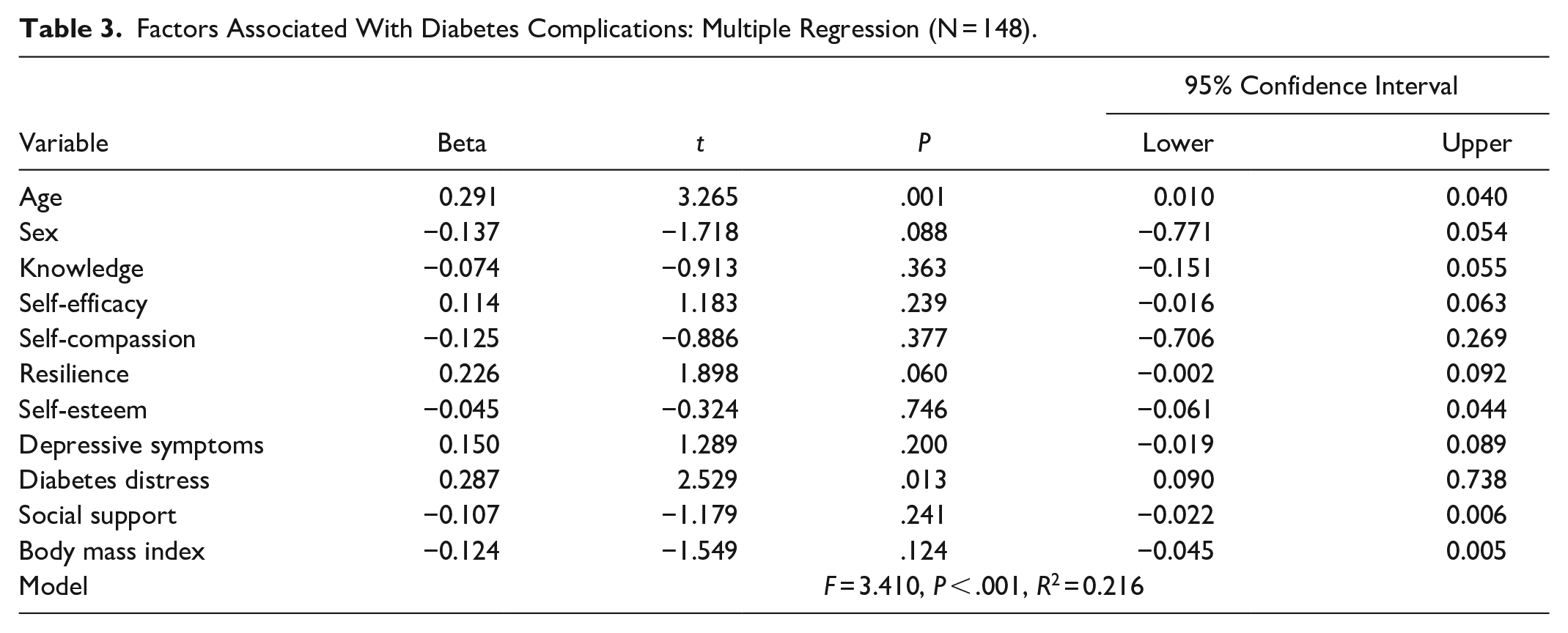
In multiple regression analysis, age, sex, knowledge, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, diabetes distress, social support, and body mass index were entered into the model simultaneously. Age (β = 0.291, t = 3.265, P = .001) and diabetes distress (β = 0.287, t = 2.529, P = .013) were associated with diabetes complications (F = 3.410, P < .001, R2 = 0.216; Table 3). Old age and higher levels of diabetes distress were associated with a greater number of diabetes complications and explained 21.6% of the variance in diabetes complications. Sex, knowledge, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, social support, and body mass index were not associated with diabetes complications.
Factors Associated With Diabetes Complications: Multiple Regression (N = 148).
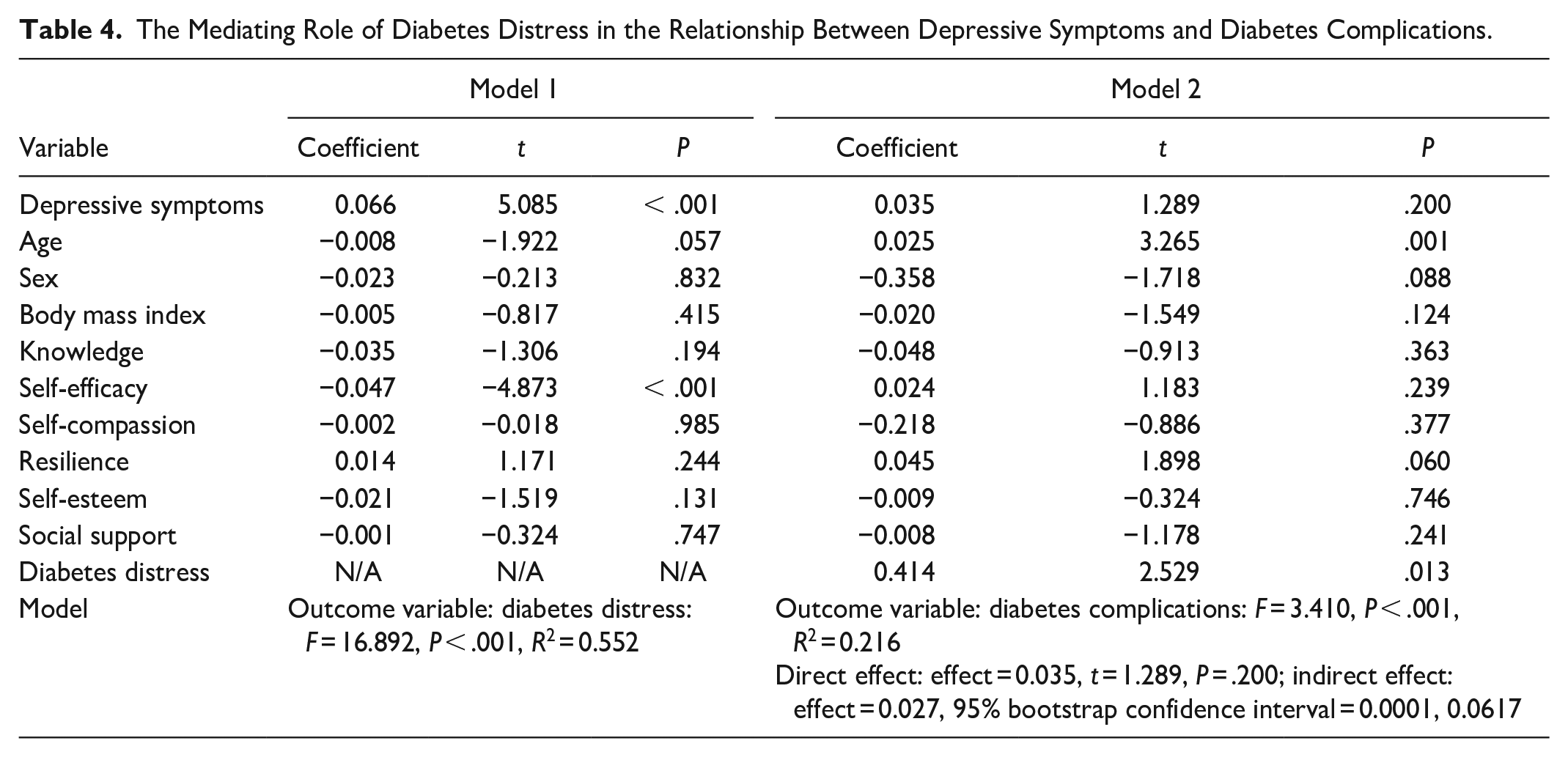
We then examined the mediator role of diabetes distress. In the mediator analysis, depressive symptoms (effect = 0.066, P < .001) were significantly associated with diabetes distress, controlling for all the demographic, psychosocial, and physiological factors (F = 16.892, P < .001, R2 = 0.552; Table 4; Figure 3). Then, diabetes distress (effect = 0.414, P = .013), but not depressive symptoms (effect = 0.035, P = .200), was significantly associated with diabetes complications (F = 3.410, P < .001, R2 = 0.216). The indirect effect of depressive symptoms on diabetes complications through diabetes distress was significant (effect = 0.027, 95% bootstrap confidence interval: 0.0001, 0.0617). In addition, higher levels of self-efficacy were associated with lower levels of diabetes distress.
The Mediating Role of Diabetes Distress in the Relationship Between Depressive Symptoms and Diabetes Complications.
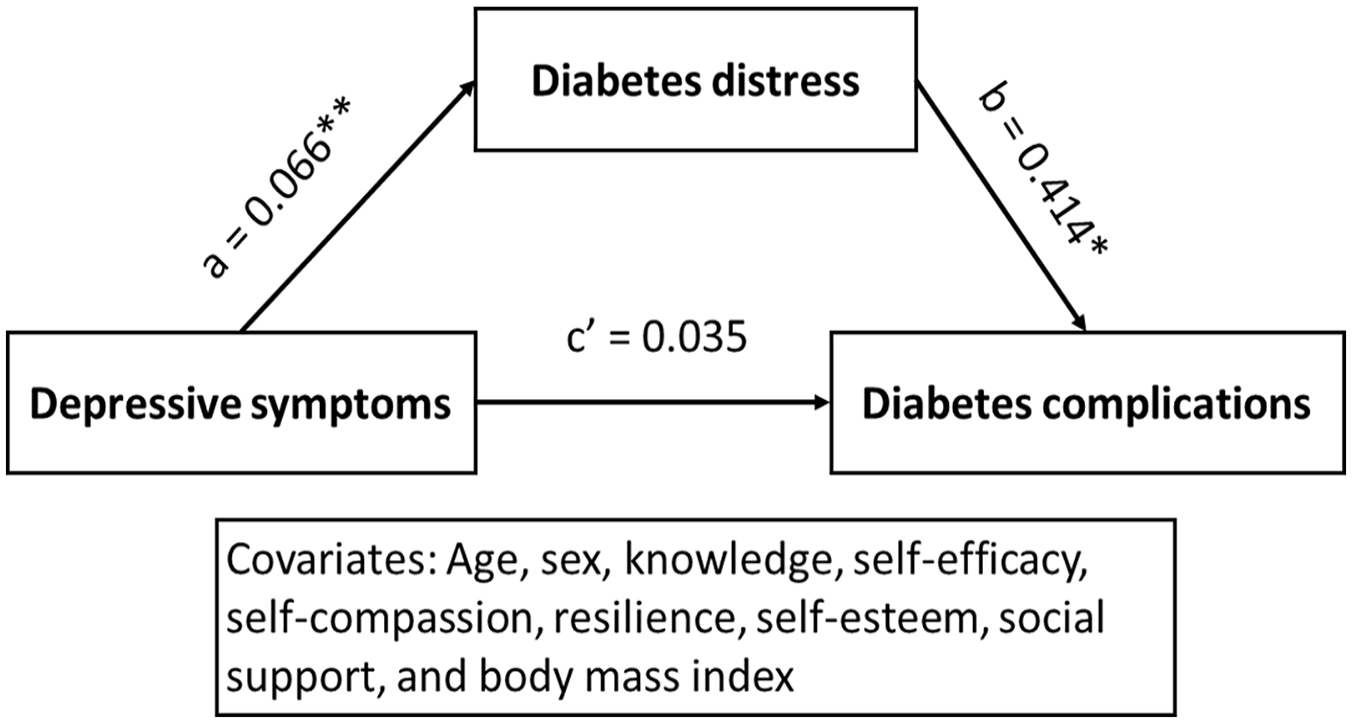
The mediating role of diabetes distress in the relationship between depressive symptoms and diabetes complications. Indirect effect: effect = 0.027, 95% bootstrap confidence interval = 0.0001, 0.0617.
Discussion
We examined the relationships of multidimensional, modifiable, and nonmodifiable factors to diabetes complications, which have been rarely examined among people with diabetes in a single study. Among those cognitive (ie, knowledge), psychosocial (ie, self-efficacy, self-compassion, resilience, self-esteem, depressive symptoms, diabetes distress, and social support), physiological (body mass index), and demographic factors (ie, age and sex), diabetes distress and age were significantly associated with diabetes complications. In addition, diabetes distress played as a mediator in the relationship between depressive symptoms and diabetes complications. Therefore, the findings of this study suggest two important intervention targets of depressive symptoms and diabetes distress, to improve diabetes complications.
Diabetes complications in this study were more prevalent than those in a prior study of more than 11 000 people with type 2 diabetes from 33 countries. 2 In the prior study, 2 approximately 32% and 17% of people had at least one microvascular or one macrovascular complication at the end of the 3-year follow-up, while in this study, approximately 55% and 24% of people with diabetes had at least one microvascular and macrovascular complications, respectively. However, both studies demonstrate a high prevalence of diabetes complications in people with diabetes. Considering the remarkable negative effects of diabetes complications on quality of life, hospitalization and mortality rates, and health costs in prior studies,3 -5 diabetes complications need to be reduced.
Consistent with the findings of this study, diabetes distress was associated with one diabetes complication (diabetic neuropathy) in a prior study of people with type 2 diabetes. 13 In contrast, diabetes distress in a prior study was not associated with incidence of microvascular or macrovascular complications at 2-year follow-up among newly diagnosed people with type 2 diabetes. 39 One difference among the 3 studies was differences in the variables included in the models. None of the prior studies included all the positive and negative psychosocial factors of this study, and both prior studies mainly included demographic and clinical characteristics and physiological and laboratory test factors in the models.13,39 The second difference was the outcomes. In this study, the number of diabetes complications was the outcome, while only diabetic neuropathy or combined microvascular or macrovascular complications were used as the outcome(s) in the prior studies.13,39 Even though these 2 differences could lead to the different outcomes among the 3 studies, the population difference between the first 2 studies and the third study might offer a better explanation of the different outcomes. The study by Ismail et al 39 alone included only newly diagnosed people with type 2 diabetes. In prior studies,2,40 duration of diabetes was associated with diabetes distress or diabetes complications. Fewer people with newly diagnosed type 2 diabetes (<5 years) belonged to the high distress group compared to those with diabetes for more than 15 years. 40 Longer duration was also related to more microvascular complications. 2 These findings imply that over time, diabetes distress may have more effects on diabetes complications. In addition, the findings of this study imply that more attention is needed for older people with diabetes to reduce or prevent diabetes compilations.
In this study, depressive symptoms were associated with diabetes complications only through the effects on diabetes distress, indicating the mediating role of diabetes distress. The mediating role of diabetes distress in this relationship has been rarely examined in people with diabetes, controlling for multiple positive and negative psychosocial, cognitive, physiological, and demographic factors. However, the relationships between depressive symptoms and diabetes distress, between depressive symptoms and diabetes complications, and between diabetes distress and diabetes complications have been examined in some prior studies.11 -13,15,41 In a prior study of people with type 2 diabetes, 15 higher levels of depressive symptoms were associated with higher levels of diabetes distress, which was consistent with the finding in this study. In several studies, depressive symptoms were associated with diabetes complications,11,12,41 which was inconsistent with the finding in this study. Two of the prior studies were meta-analyses,11,12 and one was a large sample study (>5000). 41 In large sample studies, even small differences in variables can result in significant outcomes. As shown, diabetes distress was associated with diabetes complications in one prior study, 13 which was consistent with the finding of this study. The findings of all the prior studies imply the mediator role of diabetes distress in the relationship between depressive symptoms and diabetes complications. It is meaningful to examine the mediator role suggested from the findings of the prior studies, especially considering all possible other psychosocial factors. All the findings suggest that health care providers should manage both depressive symptoms and diabetes distress to reduce or prevent development of diabetes complications.
Furthermore, in addition to depressive symptoms, self-efficacy was also significantly associated with diabetes distress in this study, controlling for multiple other cognitive, psychosocial, physiological, and demographic factors. Even though not many psychosocial factors were included, self-efficacy was associated with diabetes distress in a prior study of people with type 2 diabetes. 42 Thus, reduction of depressive symptoms and enhancement in self-efficacy may improve diabetes distress, which is a factor associated with diabetes complications.
Other cognitive, positive psychological, and social factors were not associated with diabetes complications or diabetes distress in this study. The relationships of knowledge, self-compassion, resilience, and self-esteem to diabetes complications have been rarely examined in people with diabetes. In a prior study of people with diabetes, 10 60% of people with foot ulcer, while only 14% of people without foot ulcer, belonged to the lowest self-esteem group. However, it was a descriptive study without considering any other variables. In another prior study, 16 social support assessed by network size and percentages of family members and friends was associated with macrovascular complication in men and women. However, other psychological and demographic factors that can affect diabetes complications were not controlled in the prior study. In this study, the levels of positive psychological factors were low, and self-efficacy was associated with diabetes distress. Even though it is beyond the scope of this study, other positive psychological factors may be associated with diabetes complications through the effects on other psychological factors, such as self-efficacy and self-care.43,44 Therefore, further studies with larger samples are needed to examine the direct and indirect relationships of cognitive and psychosocial factors to diabetes complications.
An 8-week mindful self-compassion intervention reduced diabetes distress and depressive symptoms and improved self-compassion and self-care in a prior study of people with diabetes. 45 In another study of people with type 2 diabetes, 46 diabetes distress and depressive symptoms in the intervention group (a collaborative, structured self-monitoring of blood glucose) and the control group were reduced, but the reduction in the intervention group was bigger than that in the control group. These findings imply that meditation intervention and self-care intervention could improve diabetes distress and depressive symptoms, which can lead to reduction in diabetes complications.
Limitations
There are some limitations of this study. Diabetes complications were assessed based on self-report, which could affect the study validity. Most participants were White, which could limit the generalizability of the findings of this study. Cronbach’s alpha (0.68) in the knowledge instrument was lower than the cut point for acceptable internal consistency reliability (0.70), even though it was very close to the cut point. Duration of diabetes was not included in this study. Its inclusion could potentially alter the findings of this study because it can be associated with diabetes complications. 47 People with type 1 or type 2 diabetes were included in this study, but type of diabetes was not included as a factor affecting diabetes complications. This nonmodifiable factor may affect diabetes complications, but in our exploratory analysis, type of diabetes was not associated with diabetes complications (P < .076). In addition, factors associated with diabetes complications in people with type 1 diabetes may differ from those in people with type 2 diabetes, potentially limiting the applicability of the findings of this study. However, at the same time, the findings of this study can be generalized to people with type 1 and also type 2. The multidimensional modifiable and nonmodifiable factors can affect diabetes self-care, which can affect diabetes complications. The theoretical framework of this article, however, did not include self-care. Thus, further studies with appropriate sample size can be beneficial to test the mediating role of self-care in the relationships between those multidimensional modifiable and nonmodifiable factors and diabetes complications.
Conclusions
The relationships suggested in the theoretical framework were supported partially, while the mediator role of diabetes distress in the relationship between depressive symptoms and diabetes complications was supported. Higher levels of negative psychological factors, including depressive symptoms and diabetes distress, were associated with more diabetes complications. In addition, one nonmodifiable factor of age was also associated with diabetes complications. One positive psychological factor of self-efficacy was associated with diabetes distress. Health care providers can target reduction of depressive symptoms and diabetes distress to reduce diabetes complications. Further studies are needed to examine the direct and indirect relationships of cognitive, psychological, social, physiological, and demographic factors to diabetes complications more comprehensively.
Footnotes
Acknowledgements
We wish to extend our sincere appreciation to Dr Justus Randolph for his statistical consultation.
Data Availability
The data underlying this article will be shared on reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.