
Abstract
Objective:
Depression among older adults is a growing problem. With aging being a risk factor for COVID-19 infection, depression in this population may have been exacerbated. This study aimed to describe experiences and changes in depressive symptoms and well-being of older adults during and after the COVID-19 first wave in Spain.
Methods:
The study used a multi-method design. Participants self-reported depressive symptoms (Geriatric Depression Scale) and well-being (Cantril Ladder of Life). Participants were asked about changes in depressive symptoms or well-being during quarantine. If a change was perceived, they were asked to describe the change. In addition, the Patient Global Impression of Change scale was used. Both quantitative and qualitative analyses were performed on the data.
Results:
111 participants (mean age: 71±5 years; 76% women) completed the study. Sixty-three percent reported mild and 2% reported major depressive symptoms. Nearly half (47.7%) reported changes in depressive symptoms during the lockdown. While 37% reported feeling better during the lockdown, about 11% reported depressive symptoms were worse now compared with during the lockdown. 60% reported worsening well-being during the quarantining period. The qualitative analysis revealed 2 main themes: (1) psychological discomfort (mood deflection, fear/worries, and boredom/inactivity) and (2) social issues (inability to go out, missing family members and others).
Conclusions:
Worsening depressive symptoms and lowering of well-being were noticed in this sample of older adults during and post-COVID lockdowns. Evaluation of mental health in the primary care setting and providing referrals for mental health services is essential for older adults who experienced COVID-19-related lockdowns.
Depression is a major contributor to health care costs, and it is estimated to be a leading cause of disease burden in middle- and high-income countries by the year 2030. 1 Moreover, depression is one of the largest contributors to nonfatal health losses, 2 and one of the most common mental disorders in older adults. Nearly 14% of older adults have depression, including 2% with major depression. 3 Depressive symptoms can significantly decrease quality of life even if an individual does not meet the threshold for a diagnosis of major depressive disorder. 4 For older adults, depressive symptoms have been demonstrated to be linked to an array of negative health outcomes, including cardiovascular diseases, dementia, and type 2 diabetes. 5
In December 2019, a new coronavirus was identified as the cause of a disease outbreak in Wuhan, Hubei Province, and subsequently spread rapidly throughout China and worldwide. 6 In March 2020, the World Health Organization declared the outbreak of this disease as a pandemic. Therefore, in this first wave, the Spanish government decreed the state of alarm which allowed the lockdown of the entire population from March 2020 to May 2020, and after lockdown a “new normal” was established where social distance still existed. 7 Existing concerns about the well-being and psychological health of older adults increased during the COVID-19 pandemic. Older adults were identified as especially vulnerable to the virus, with high rates of fatalities during the first wave of the pandemic. 8 In Spain there were 18 342 deceased in this lockdown, with 35.2% being adults over 70 years old living in the community. 9 Therefore, health policies instructed the population, especially older adults, to maintain social distancing and participate in full lockdowns for extended periods, which meant physical and social isolation. 10 Although older adults tend to experience well-being equally or better than that of younger age groups, 11 the COVID-19 quarantine was predicted to influence the well-being of older adults negatively and could have caused an elevation in depressive symptoms. 12 In addition, the high rate of deaths of the older adults’ age group may have also influenced these symptoms.
Previous studies have analyzed the consequences of confinement on older adults, focusing on aspects of nutritional or physical activity13,14 and emotional consequences of lockdown. 15 A systematic review which focused on psychological repercussions of quarantine suggests that the self-isolation due to the COVID-19 pandemic may have presented a serious risk factor. 16 Research showed that older adults with greater social isolation or greater feelings of loneliness, poorer housing conditions, and higher prevalence of chronic morbidities had an increased risk of developing unhealthier lifestyles or mental health decline due to lockdown during the COVID-19 pandemic. 17 Social isolation implies separation from loved ones, the loss of freedom, uncertainty over disease status, and boredom, so it may lead to psychological changes. 16 Although research regarding psychological health changes during the COVID-19 pandemic in older adults has been conducted, qualitative perspectives of these older adults have not been assessed. Given that global disease outbreaks may be a recurrent situation (e.g., SARS, Ebola, and H1N1 influenza), health care professionals and policy makers need evidence to produce guidance for treatment and prevention.
Purpose
Therefore, in this multi-method study, we aimed to describe depressive symptoms and perceived well-being of older adults after the COVID-19 first wave in Spain. Furthermore, this study explores the change in depressive symptoms and well-being during quarantine compared with after the quarantine and patients’ personal experiences of this change.
Methods
Participants
A multi-method study was conducted using a convenience sampling approach. Participants were recruited through associations of older adults in the city of Valencia between May 2020 and July 2020, just after the first lockdown. Participants indicating interest in participation were screened via a telephone call. Inclusion criteria were age ≥ 60 years, community-dwelling, and being cognitively able to answer the questionnaires (checked by the ability to understand and answer accordingly the aspects of this telephone call). Exclusion criteria were older adults living in assisted-living residential facilities, any disability that did not allow them to answer the questions, or not being able to provide medical data. The Institutional Ethics Committee on Human Research of the University of Valencia approved the study protocol (IE1490224), and the investigation conforms to the principles outlined in the Declaration of Helsinki. All enrolled participants provided informed written consent before the assessments were performed, and the rights of the participants were protected.
Measurements
Participants were assessed by a telephone call, in a single session. Demographic data such as age, gender, educational level, marital status, or having children or grandchildren were assessed with a questionnaire. Clinical data included comorbidities and were obtained from medical files. Participants were asked to describe their changes in depressive symptoms and well-being during lockdown and after it, using the questionnaires described below.
Depressive symptoms were assessed with the Geriatric Depression Scale. 18 This scale is comprised of 15 items; a score from 0 to 4 is considered normal, 5 to 8 indicates mild depressive symptoms, 9 to 11 indicates moderate depressive symptoms, and 12 to 15 indicates severe depressive symptoms. For the 15 items, older adults could indicate if the listed behavior changed during quarantine or not. If it changed, they were asked to elaborate on this change with an open-ended question. At the end of this scale a question was added based on the Patient Global Impression of Change scale. 19 Participants were asked to indicate how would they describe the change in depressive symptoms during quarantine compared with the present time on a scale from 1 to 7, with 1 meaning “Depressive symptoms have got worse” till 7 meaning “A great deal better, and a considerable improvement that has made all the difference.”
Well-being was assessed with the Cantril Ladder of Life. 20 Older adults were asked to imagine a ladder with steps numbered from zero at the bottom to 10 at the top. The top of the ladder represents the best possible life, and the bottom of the ladder represents the worst possible life. Older adults were asked to indicate on which step of the ladder they felt to stand at the time of assessment, and on which step they felt they stood during quarantine. If the well-being had changed during quarantine compared with present time, they were asked to elaborate on this change with an open-ended question. The Ladder of Life has been used in large population studies, and tested for reliability, concurrent validity, and predictive validity. 21
Data Analysis
This study used 2 different methodological approaches for the analysis of the survey data: a quantitative approach for the numerical variables of the instruments and a qualitative approach for the analysis of the open-ended responses. Descriptive statistics were used to describe the demographic and clinical data, as well as the scores on the Geriatric Depression Scale and the Cantril Ladder of Life. Text responses to open-ended questions about Geriatric Depression Scale were transcribed and analyzed using structured tabular thematic analysis (ST-TA; Figure 1). 22 Text responses were read repeatedly for immersion in the data and were independently examined by the author (AD). To avoid being biased, the person who performed the analyses was not aware of the scale items, thus performing the analyses “blinded,” without prejudice, to increase objectivity. The process was purely inductive, based exclusively on what emerged from the answers provided by the participants. Phases are displayed in Figure 1, which is the adaptation of the original methodological paper of Robinson. 22 Several strategies were used to ensure credibility and trustworthiness of the data, 23 including multiple research team members reviewing the transcriptions, multiple team discussions to identify categories, member checking, and coding verification by a second team member. To preserve cultural integrity, quotations are also given in the original language. 24
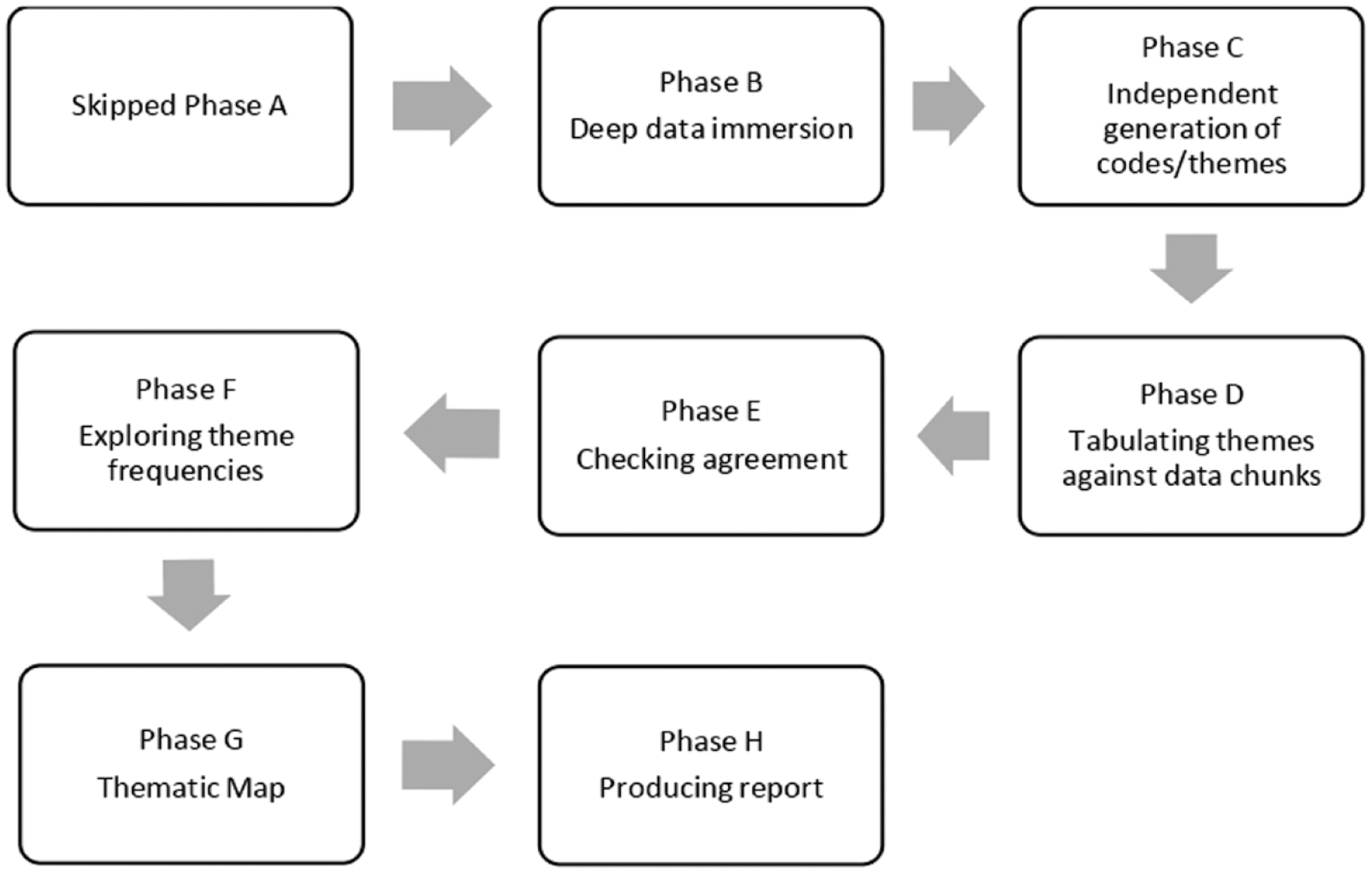
Conducting thematic analysis on brief texts: The structured tabular approach. Qualitative Psychology. Phase A: A priori theme development.
Results
From a total of 189 older adults who were assessed for eligibility, 111 participants took part in the study. The mean age was 71 ± 5 years, 76% women (n = 84), over half were married (54%, n = 60), and most had university studies (76%, n = 84) (Table 1). The main reason for exclusion was unwillingness to participate.
Demographic and Clinical Characteristics of Older Adults During Quarantine (N = 111).
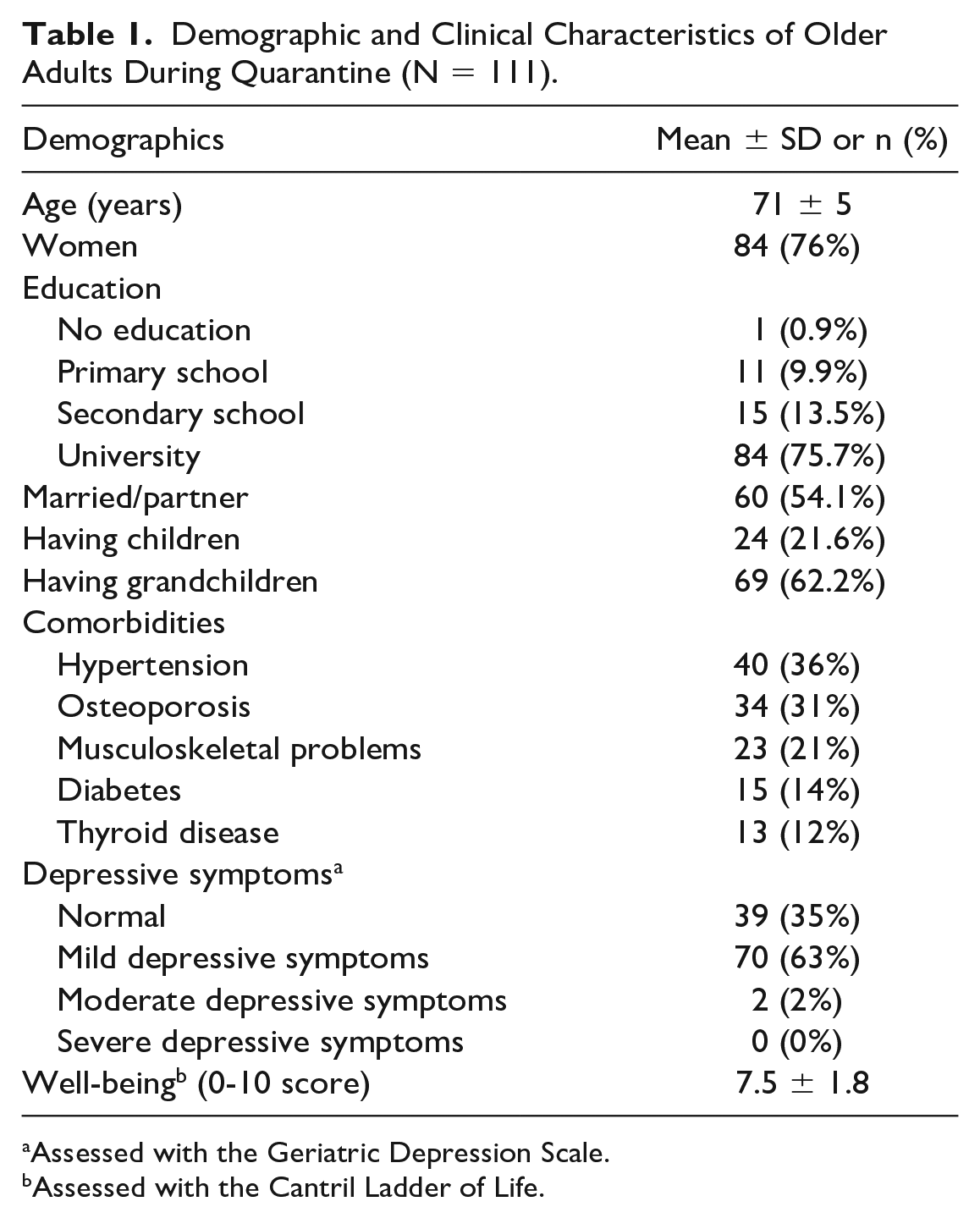
Assessed with the Geriatric Depression Scale.
Assessed with the Cantril Ladder of Life.
Depressive Symptoms, Well-Being and Change During and After Quarantine
During quarantine, over half of the participants (63%, n = 70) suffered from mild depressive symptoms, up to 2% (n = 2) from moderate depressive symptoms, and 35% (n = 39) had normal depressive symptoms. No participant reported severe depressive symptoms (Table 1). In total, 58 (52%) older adults did not notice any difference in their depressive symptoms during and after lockdown, and 53 (47.7%) did find a change, with 41 (37%) feeling better now compared with the lockdown period, and 12 (11%) feeling worse now compared with lockdown.
After the quarantine, most of the older adults felt wonderful to be alive (97%, n = 108), happy most of the time (90%, n = 100), in good spirit (89%, n = 99), satisfied with life (86%, n = 95), and full of energy (83%, n = 92). Most of them were not afraid that something bad would happen (84%, n = 93), they did not have memory problems (89%, n = 99), they were often bored (93%, n = 103), they did not feel hopeless (95%, n = 105), they did not feel that life was empty (94%, n = 107), or did not feel that life was helpless (96%, n = 106), neither that other people were better (99%, n = 100) nor that they wanted to stay at home (82%, n = 91). None of the older adults felt worthless (Figure 2).
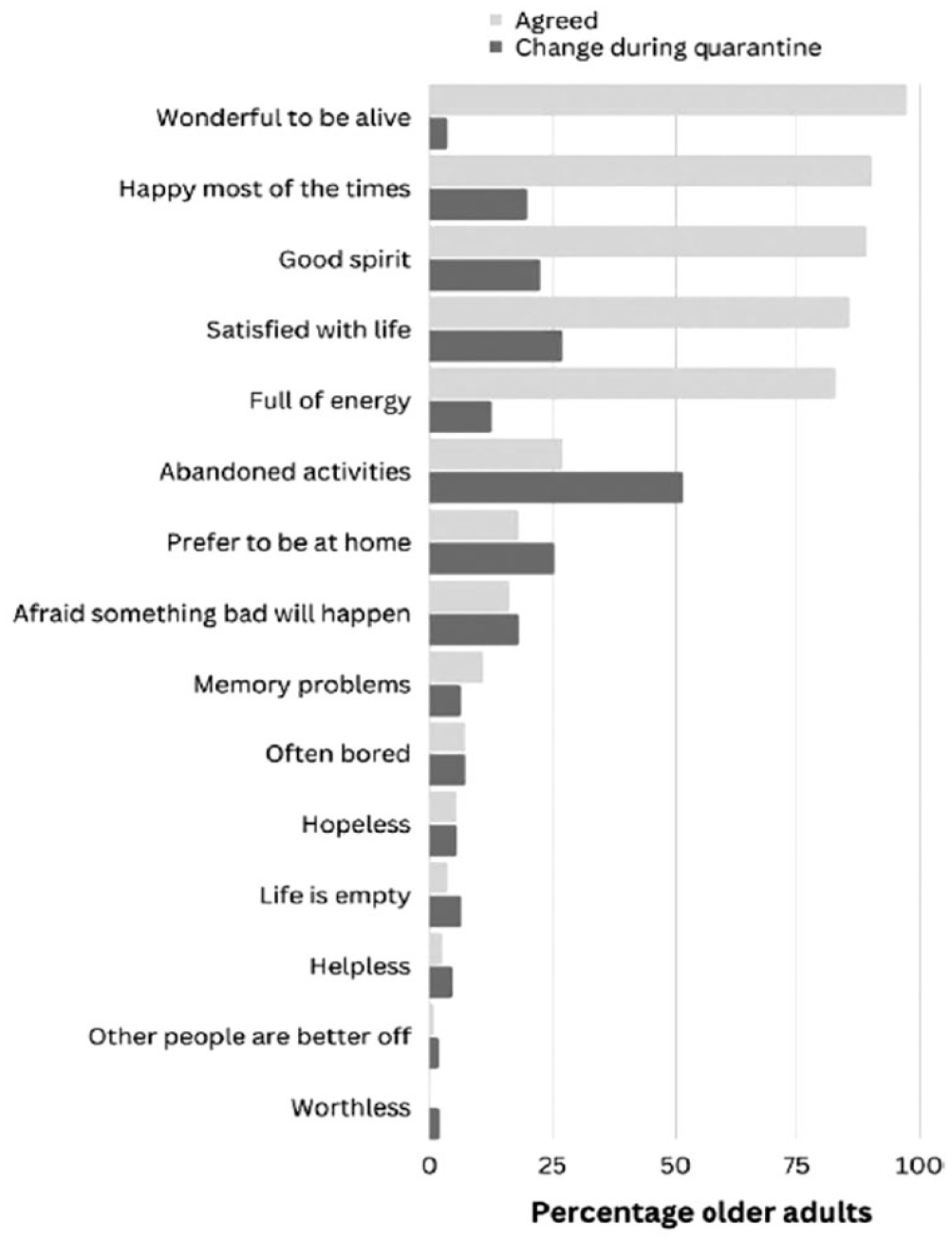
Experiences of depressive symptoms after quarantine and change in depressive symptoms during quarantine in older adults (n = 111).
Older adults scored a 7.5 (±1.8) on well-being after quarantine, while during quarantine they scored a 6.3 (±2.2). In total, 60% (n = 66) had a worse well-being during quarantine, 31% did not report a change in well-being, and 9% (n = 11) felt better well-being during quarantine compared with after quarantine. Figure 3 depicts the change in well-being in older adults during quarantine compared with after the quarantine.
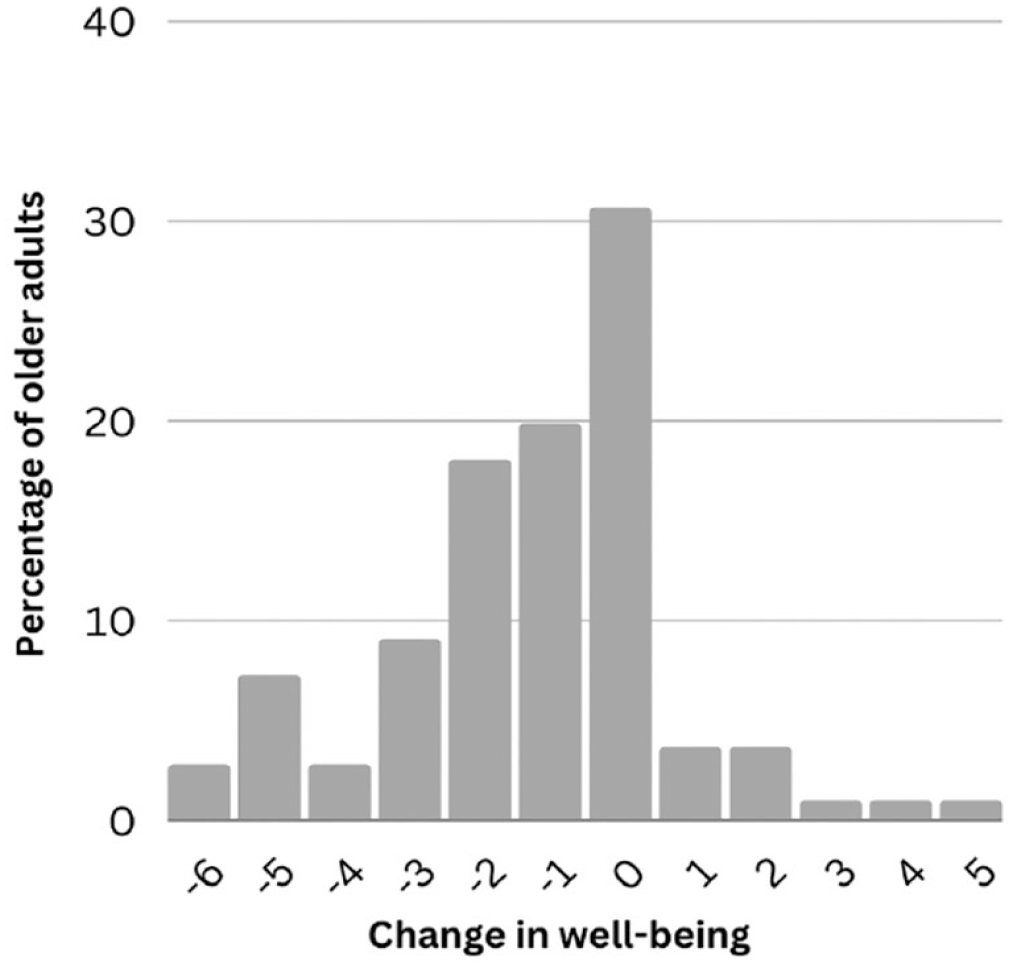
Change in well-being in older adults during quarantine compared with after the quarantine.
Among the 111 older adults, 53 (48%) elaborated on the change they felt during quarantine in depressive symptoms and well-being. They described that they experienced emotional discomfort during quarantine. This emotional discomfort can be divided into its emotional spheres: that of self-reflection, and that of emotions caused by and reflected on the environment. Two main overarching themes were identified: psychological discomfort and social issues. Regarding psychological discomfort, 3 categories were determined: (1) mood deflection, (2) fears and worries, and (3) boredom and inactivity. With regard to social problems, the 3 identified categories were (1) inability to go out, (2) missing family members, and (3) missing others (Figure 4).
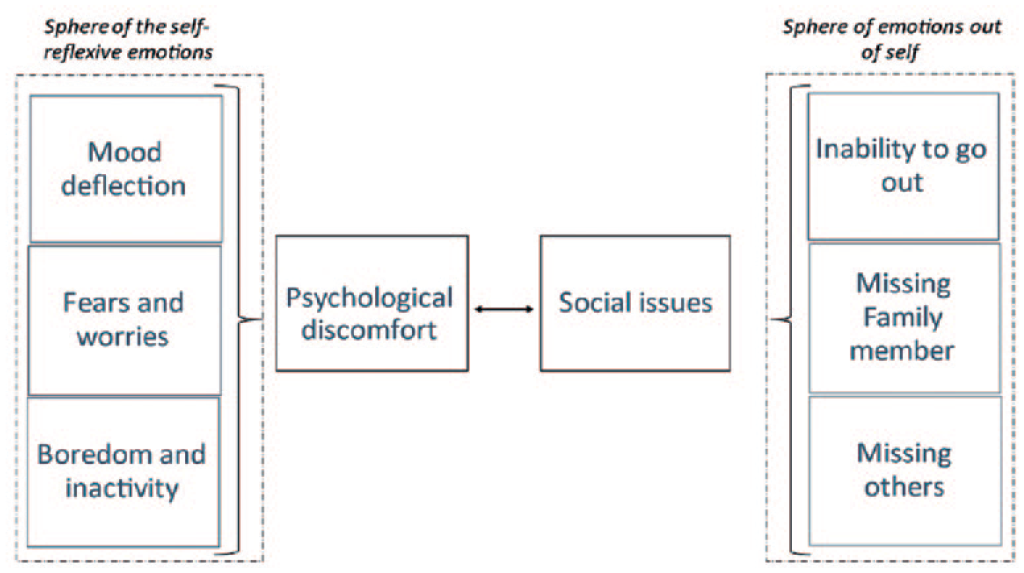
Map of themes and categories of emotional discomfort during lockdown.
Psychological Discomfort
Mood deflection
Among the most recurrent codes (25 of 53 participants [47%]) was sadness accompanied by a general mood deflection with variable feelings sometimes difficult to label. Participants reported a sincere decrease in mood, but they could not quite define or attribute it to anything. In fact, they often referred to the “situation” in a general way or specified which positive feelings they were missing; some examples follow: Sometimes I was less in the mood because of the situation. (Woman, 74 y/o) A ratos estaba con menos ánimos por la situación. (Mujer, 74 a) Happiness was a bit absent; I wasn’t laughing, I wasn’t in the mood. (Woman, 70 y/o) La felicidad estaba un poco ausente, no reía, no tenía mucho ánimo. (Mujer, 70 a)
This result was confirmed by the change that participants felt in depressive symptoms during quarantine, with some older adults feeling less satisfied with life (27%), with decreased spirit (23%), and not happy most of the times (20%) (Figure 2).
Fears and worries
Psychological discomfort was certainly among the most present consequences of the pandemic. Among the most predominant feelings were fear and worry (56% of participants, 30 of the 53 who experienced changes). Worries were both for oneself and for others, often also directed at a future that seemed to be very uncertain. Often the level of worry increased to the point of becoming a real fear. As one older adult stated: I was afraid but not because of the COVID, I thought it was like a bloodless pre-war that was going to exterminate us all, escape; fear of being with others, you would cross the pavement if you saw others. (Woman, 68 y/o) Tenía miedo, pero no por el COVID, pensaba que era como una preguerra sin sangre que nos iba a exterminar a todos, huida; miedo a juntarte con otros, cruzabas de acera si veías a otros. (Mujer, 68 a)
This was also reflected in the quantitative data on depression, where 16% of the older adults were afraid that something bad would happen after the quarantine, and 18% of the older adults were more afraid that something bad would happen during quarantine.
Boredom and inactivity
Twenty-three statements were related to boredom and inactivity codes, subsumed in the absence of routine activities that involved being out of the house or interacting with other people: I could not exercise with my physical therapist. (Woman, 84 y/o) No podía hacer ejercicio con mi fisioterapeuta. (Mujer, 84 a) Go to the swimming pool, I couldn’t walk, or go to play dominoes. (Man, 77 y/o) Ir a la piscina, no podía andar, ni ir a jugar al dominó. (Hombre, 77 a) There were times when I did get bored, it was a lot of hours cooped up at home. (Woman, 65 y/o) Había momentos en que sí me aburría, eran muchas horas encerrada en casa. (Mujer, 65 a)
This result was also reflected in the answers on the change in depressive symptoms. Approximately half of the older adults abandoned activities during quarantine (51%) compared with 27% after quarantine. Also, a quarter of the older adults preferred to be at home, compared with 18% after quarantine. In total 7% of the older adults felt bored after quarantine and in 7% of the older adults this was higher during quarantine.
Social Issues
Inability to go out
Limitations in terms of activities, given by lockdown, were the prevailing code for 31 of the 53 participants (58%). Moreover, the repercussions of these limitations then affected relationships and even psychological aspects. This was the most intersectional code among all the others. The impact of this code had a direct bearing on family and social relationships, as seen in the example below: I have given up everything I did before the confinement, I do nothing, no English class, no pilates, no lectures, etc. (Woman, 68 y/o) He abandonado todo lo que hacía antes del confinamiento, no hago nada, ni inglés, ni pilates, ni conferencias, etc. (Mujer, 68 a)
Missing family members and others
In total, 30 of the 53 participants (57%) talked about how confinement had caused them to miss others, especially family affections. Regarding family affections, many referred to children and grandchildren whom they routinely cared for: My son wasn’t at home, and I was sadder because he was away. (Woman, 68 y/o) No estaba mi hijo en casa y estaba más triste porque él estaba lejos. (Mujer, 68 a) When you are not able to go out, you stop socializing. (Woman, 65 y/o) Al no poder salir, las relaciones sociales dejas de hacerlas. (Mujer, 65 a)
The situation was even worse for those who lived alone: Living alone, I felt the need for a call from administrations/health or something to ask how he was doing. (Man, 75 y/o) Al vivir solo, sentía la necesidad de una llamada de administraciones/sanidad o algo para preguntarle que tal estaba. (Hombre, 75 a) I felt a little lonely, I’m on my own if something happens to me, what do I do? (Man, 65 y/o) Me sentí un poco solo, estoy solo si me pasa algo, ¿qué hago? (Hombre, 65 a)
Discussion
The first aim of this study was to describe psychological health in older adults after the COVID-19 first wave. The second aim was to explore the change in depressive symptoms and well-being during quarantine compared with after the quarantine and patients’ experiences of this change. Among this sample of older adults, 37% felt their depressive symptoms got worse during the quarantine and 60% reported less well-being during quarantine compared with after quarantine.
Our study findings are comparable with findings in the general population. 25 In a study of 1143 adults conducted in the U.S., 26 depressive symptoms increased and life satisfaction decreased when comparing before to during COVID-19. A study from the United Kingdom on 3077 adults found that mental health and well-being were negatively affected during the initial phase of the COVID-19 pandemic. 27 Another study looking at Google Trends in Europe and the United States found an increase in searches regarding boredom, loneliness, worry, and sadness during lockdown compared with before the pandemic. These results also show that psychological health was negatively affected by the pandemic and lockdown. 28 A study from the United Kingdom including 5146 older adults showed that depressive symptoms, loneliness, and poor quality of life increased significantly during COVID-19.29,30 Interestingly, a study including 1071 older adults from Sweden, where there were no lockdowns, found that on average older adults rated their well-being as high as, or even higher than, previous years during the early stage of the pandemic, compared with the 5 years previous to the pandemic. 31 However, those who worried more reported lower well-being. In this sense, previous literature has highlighted that cognitive behavioral therapies could be delivered online to increase well-being and even decrease loneliness. 32
According to our qualitative findings, participants experienced psychological discomfort and social issues during quarantine. Regarding psychological discomfort, although this was generalized in the population during quarantine, certainly older adults and often lonely people suffered the most. This finding is consistent with studies from another European countries particularly affected by the first pandemic. 33 Moreover, in Spain, where this study was conducted, there is a familistic welfare system, which is a welfare state model in which the family plays a key role in the overarching architecture of the welfare system, acting as the main provider of care and welfare for children and dependent individuals. 34 Therefore, older adults, who were used to being cared for and accompanied by family, could have noticed even more loneliness during lockdown. 34 With older adults being at high risk of mortality for a crisis such as the COVID pandemic, interventions to counteract social isolation and support an active lifestyle that can be preserved or even empowered in emergencies should be investigated and employed. 35 For example, one strategy to decrease loneliness during a pandemic could be video conferences with family. 25 Other strategies that could be used are focusing on leisure activities and skill development. This could include indoor gardening programs, computer/internet use, voluntary work, holidays, and sports.36-38 Such interventions should not be reserved for emergencies but adopted as constant and consistent policies over time given the permanent demographic change in Southern European countries and across the globe. 39
Regarding the social issues experienced in the pandemic, they highlight the importance of social connections that have a significant impact on both community-living older adults and those in nursing facilities. 40 The negative experiences, such as not being able to leave their home, were common across the globe in countries that instituted lockdowns and not just in Spain. However, such lockdowns can have a disproportionate impact on communities. Indeed, in Spain, it is very common for people over age 60 to gather in cafés and town squares in the evening. Given also the familistic welfare system 34 and the frequent construction of the households of successive generations in proximity, the disruption of the habit of seeing each other daily with children and grandchildren created a very pronounced discomfort. These cultural elements have also led offspring reconnecting with their village of origin, thus being closer to the town where their parents lived. In fact, in Spain some rural areas have seen a repopulation during the pandemic, 41 precisely dictated by the reasons described above.
It seems interesting to see how no aspect of physical discomfort, other than related to the lack of being able to do physical therapy, emerges with preponderance. This, from a policy perspective, would also merit reflection. For health care professionals such as nurses, physical therapists, geriatricians, psychologists, and social workers, who have direct contact with older people, it is important to know how this social isolation affects well-being and depression. Certainly, actual health care system policies support older people to live a life with well-controlled physical comorbidity symptoms, 42 but perhaps there is a mental and social well-being aspect that now needs attention.
The results of this study must be taken into consideration alongside its limitations. First, this was a retrospective cross-sectional study conducted in a single country. Second, there was the possibility of recall bias, since participants were asked to recall a past event that, overall, negatively impacted them. Thus, there was a risk of an overestimation and underestimation in recall, given the negative meaning of the event, or that they may have had an unclear memory. Third, qualitative data were collected using a survey, which limited the spontaneity of the answer and the length of responses. Fourth, the sample was primarily university-educated and consisted mostly of women. Finally, one last point should be made about those who suffer from mild depressive symptoms, which was found in more than 60% of our sample. Since they are not overt or declarable pathological symptoms, these are often not identified in time until they become moderate. A path to early diagnosis and counteracting symptoms could affect many people if the rates from this study are confirmed in a larger sample. Future studies should also investigate the consequences of the worsening of depressive symptoms and lowering of well-being in older adults and implement appropriate protocols to ensure appropriate health outcomes in this population, considering the assessment of depressive symptoms and well-being during critical periods. Thus, evaluation of mental health in the primary care setting and providing referrals for mental health services may be essential for older adults who experienced COVID-19-related lockdowns.
Conclusions
During quarantine, 37% of the older adults in our sample felt a worsening in their depressive symptoms and 60% had less well-being compared with after quarantine. Moreover, when asked to elaborate on this worsening change with an open-ended question, 2 main themes were identified, psychological discomfort and social issues. These issues are not isolated to a specific region or country, and need to be further evaluated to inform policies to improve psychological health and well-being among older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.