
Abstract
Drug-induced kidney injury has historically been associated with renal tubule injury related to small molecule pharmaceuticals such as nonsteroidal anti-inflammatory drugs, antineoplastic agents, or antibiotics, but as a greater number of alternative classes of medicines such as biotherapeutics, molecular-targeted antineoplastic drugs, chimeric antigen receptor T-cell therapies, antibody-drug conjugates, oligonucleotide therapies, or other immunomodulatory drugs come to market, the presentation of drug-induced nephrotoxicity is changing. This review article describes the potential rare clinical events in drug-induced kidney injury that might be noted with these new therapies and their potential impact on patients. Potential pathogenic mechanisms related to immunogenicity, immune complex formation, and stimulation of downstream proinflammatory pathways with some of these alternative medicine classes have resulted in the potential for glomerulonephritis, acute interstitial nephritis, renal vasculitis, and other immune-mediated renal disorders in humans. This contrasts with nonclinical toxicity studies, where biologic therapies more often result in vasculitis and glomerulonephritis associated with antidrug antibodies and immunomodulatory pharmacology, and which are not always predictive of clinical effects. While nonclinical antidrug antibody-related renal disease is generally not clinically relevant, other immune-mediated nephrotoxicities associated with immunomodulatory drugs may be predictive of clinical adverse events. Fortunately, these conditions are still rare and account for a small percentage of serious adverse events in kidneys of patients.
Keywords
Despite advances in diagnosis, renal monitoring, and drug safety, drug-induced kidney toxicity remains a significant contributor to acute renal injury with a frequency estimated at 14% to 26% in hospitalized patients. 1 Historically, drug-induced kidney injury (DIKI) was associated with renal tubular toxicity related to nephrotoxic agents such as nonsteroidal anti-inflammatory drugs, antibiotics, antifungal, and anticancer agents, and much less frequently with immune-mediated effects such as interstitial nephritis (e.g., from cyclosporine or penicillamine). 2 However, in the past decade, the pharmaceutical landscape has undergone changes and the clinical presentation of DIKI has also began to change. Small molecule therapeutics have become a smaller percentage of new drug applications, in the favor of alternative medicine classes including biotherapeutics (antibody and peptide therapies), molecular pathway-targeted antineoplastic agents, immunomodulatory therapies (e.g., checkpoint inhibitors [CPIs]), chimeric antigen receptor T-cell (CAR-T) therapies, antisense oligonucleotides and RNA-silencing drugs. For example, in 2018, the FDA approved 59 new drugs, and of these only 71% were small molecules, with the remainder consisting of biologics, and similarly, in 2020, biologics accounted for 15 of 53 new drug approvals. 3 Cases of DIKI have occurred both during clinical trials and postmarketing with many nonsmall molecule medications, and therefore, it is imperative that clinicians and scientists involved in drug development be familiar with the nephrotoxic potential of these new classes of medicines.
Biotherapeutics
As antibodies, recombinant peptides and multimeric complex biologics have become increasingly popular as therapeutic modalities, development of kidney-specific autoimmune conditions, termed “biologics-induced autoimmune renal disorders” (BAIRD) have been recognized with greater frequency in patients, but are still considered a rare clinical event.4-6 BAIRD can occur in adult populations of any age, but it is more common in patients with pre-existing rheumatoid conditions. 6 According to the original definition, BAIRD cases are classified either as: a) glomerulonephritis associated with systemic vasculitis; (b) glomerulonephritis in lupus-like syndrome; or (c) isolated autoimmune renal disorders.4-6 This terminology and classification fits some of the original autoimmune presentations in humans, but it is not as applicable in the case of nonclinical toxicities with biologic agents. The relationship between the use of biologics and glomerular injury in laboratory animal (nonclinical) species is generally based on their immunogenicity and the development of immune complex formation related to antidrug antibodies (ADA).5,7-9 The idiosyncratic formation of immune complexes generated by the affected individual animal to the foreign antigen can occur within vasculature or at the endocapillary surface of glomeruli. Deposition in glomerular capillaries induces detrimental immune-mediated effects from cytokine release, complement fixation, and/or secondary thrombosis.7,8 ADA-related glomerulonephritis and vasculitis associated with immune responses to foreign antigens (especially humanized peptides), is commonly identified with the administration of many biologic therapies in nonhuman primates. As a typical example of this condition, administration of obinutuzumab to cynomolgus monkeys resulted in glomerulonephritis, arteritis/periarteritis, and increased incidence of perivascular inflammation associated with ADA-related immune complexes. 9 In contrast, vasculitis-associated glomerulonephritis without ADA involvement rarely occurs in animals as a spontaneous lesion and is very rarely noted as a drug-related phenomenon in animal toxicity studies.7-10 BAIRD lesions in humans that are associated with vasculitis often do not involve ADA, and may lack immune complex formation at the site of injury.6,11 Lupus-like glomerular syndromes are extremely rare as a drug- or chemical-related toxicity in animals, as are “isolated autoimmune renal disorders.” 10 Therefore, none of the three forms of classification for BAIRD have specifically been applicable in nonclinical DIKI. Hence, BAIRD has been considered a clinical syndrome, and one that has not been utilized in the veterinary or nonclinical toxicologic pathology literature. In human patients, ADA may develop to an administered biotherapeutic drug, but this only causes immune complex formation or secondary renal complications in rare instances.12-14 Instead, pharmacologic activity of the biotherapeutic plays a significant role in BAIRD in humans, particularly when the biologic targets a broad spectrum proinflammatory pathway.13,14 Some of the older-generation biologic therapies such as etanercept, adalimumab, infliximab, and tocilizumab have had a greater tendency to result in adverse renal reactions than more recent humanized antibody therapies which target ever more selective immune pathways, so fortunately, the incidence of BAIRD reactions is uncommon.4,15 Drug-induced autoimmune reactions occur in less than 1% of patients exposed to drugs and of these only 5% develop autoimmune or vasculitis-like kidney lesions. 14 The Spanish Study Group of Biological Agents in Autoimmune Disease (BIOGEAS) Registry noted only 50 cases of glomerulonephritis from over 13,000 cases of autoimmune diseases that developed in patients exposed to biotherapeutic drugs. 16 Interestingly, 50% of glomerulonephritis cases with biologic agents were associated with tumor necrosis factor (TNFα)-targeted therapies like etanercept or adalimumab suggesting pathway-specific immunomodulation played an important factor in disease pathogenesis in addition to ADA generation.13,16,17 Further, support for the immunomodulatory mechanism comes from a study that demonstrated glomerulonephritis in 7% of patients receiving TNF-targeted peptide therapy and little evidence of ADA or circulating immune complexes.17,18 It is thought that anti-TNFα agents can cause autoantibody production via a cytokine switch paradigm that results in a shift from Th1 to Th2 cytokine production.19,20 TNFα therapies seem to predispose patients to a host of immune-mediated renal effects by several pathogenic mechanisms in addition to the classical forms of BAIRD and have been rarely associated with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis/ glomerulonephritis, and with exacerbation of IgA nephropathy. 20 Anti-TNF therapies are also more prone to ADA formation as compared with other biologics. 13 Infliximab is a recombinant anti-TNFα peptide that is considered especially immunogenic, and carries the highest risk for ADA among humans. 12 The combination of immunogenicity and immunomodulatory activity may explain the high number of BAIRD cases with these agents. Hypersensitivity reactions to peptides and antibody therapies can result in secondary activation of the complement cascade once immune complexes form. The kidney appears to be particularly susceptible to activation of the alternative pathway, and it has been implicated as a primary driver of atypical hemolytic uremic syndrome, C3 glomerulopathy, and especially ANCA-associated vasculitis. 21
Rituximab has occasionally been implicated as a potential cause of BAIRD with cases ranging from minimal tubule dysfunction to more severe hypersensitivity reactions and vasculitis. 22 Rituximab leads to B-cell depletion and while it has actions as an immunomodulatory agent, systemic drug hypersensitivities are likely related to the innate immunogenicity of the protein itself. 16 Despite these reactions, Rituximab has been administered safely to large numbers of patients with renal compromise. 23 Antibody therapies that target nonimmune receptors, or synthetic monoclonal treatments targeting foreign (viral) antigens, are generally not as prone to immune complex activation and glomerulonephritis, as long as they are not excessively immunogenic. For example, in response to the COVID-19 pandemic, the anti-SARS-CoV-2 monoclonal antibody therapy bamlanivimab recently has been administered to thousands of patients worldwide. Despite a risk for anaphylaxis and rare cases of infusion reactions, BAIRD has not been reported to be associated with bamlanivimab administration.24,25
Check Point Inhibitors
Other complex types of biologic agents may cause renal effects based on their pharmacology and immunomodulatory properties. Nivolumab and pembrolizumab are members of a novel class of anticancer drugs termed immune CPIs which block PD-1, a molecule expressed in activated T cells, B cells, natural killer T cells, monocytes, and dendritic cells. 26 These drugs have been associated with acute kidney injury (AKI) and/or acute interstitial nephritis (AIN) in approximately 2% of patients. 27 In one study, renal biopsy of 12 patients out of a total of 676 patients administered pembrolizumab resulted in a diagnosis of either AIN, acute tubular injury (ATI) without inflammation, or minimal change disease. 28 While the mechanism of action involves immunomodulatory effects on T cells, the specific pathogenesis for renal changes is not completely understood. Like TNFα inhibitors, immune activation probably predisposes the renal tubulo-interstitium to vascular injury from inflammatory mediators combined with immunogenicity of peptides. Ipilimumab is another CPI that targets CTLA-4 activity and causes migration of activated T cells into the kidney, which can also lead to AKI and AIN. 29 AKI occurs relatively late after initiation of CPI therapy. In a retrospective study of 16 patients, the median time to developing AKI from starting CPIs was 14 weeks (range 6-56 weeks). 30 Interstitial inflammation was the most common biopsy finding, in association with other glomerular pathologies (pauci-immune glomerulonephritis, membranous glomerulonephritis, C3 glomerulonephritis, IgA nephropathy, or amyloidosis). 30 Despite the potential for nephrotoxicity, CPIs have been successfully administered to cancer patients with significant renal compromise without adverse effects and guidelines have been established for patient safety in these populations.27,29,31
Because there is a variable and somewhat muted pharmacologic T-cell response in nonhuman primates with administration of PD-1 or CTLA-4 CPIs, similar inflammatory events to humans were not observed in the kidneys or other organs of cynomolgus monkeys treated with ipilimumab or nivolumab as monotherapies.32,33 However, the combined use of ipilimumab and nivolumab in a 4-week duration cynomolgus macaque toxicity study resulted in dose-dependent diarrhea and weight loss associated with intestinal inflammation. 34 Despite the intestinal inflammation, no renal findings were reported. This demonstrates the clinical nonpredictability of nonclinical species toxicology with some of these alternative classes of agents, particularly with respect to the kidney.
CAR-T Therapies
Axicabtagene ciloleucel and tisagenlecleucel are CAR-T therapies using cytotoxic T cells targeting hematologic cancers. CAR-Ts are genetically engineered surface receptors consisting of an extracellular antigen-binding domain recognizing specific tumor antigens and intracellular T-cell signaling domains incorporated on autologous T cells. 35 Cytokine release syndrome (CRS) is a recognized toxicity of CAR-T and occurs in the majority of patients, but there is also a risk for AKI with this class of treatment. 36 Among 46 lymphoma patients administered CAR-T, the cumulative incidence of AKI was 30% after 100 days, but in general cases were mild and most patients recovered within 30 days. 37 In a separate trial studying 78 patients receiving CAR-T therapy, cytokine release syndrome occurred in 85%. AKI occurred in 19% of patients, and several patients developed decreased kidney perfusion and acute tubular necrosis. 38 Electrolyte abnormalities were also common. Interstitial inflammatory renal lesions similar to AIN have been noted in some animal studies but the pathogenesis may be unrelated to the AKI noted in patients. These included mixed inflammatory infiltrates composed of primarily mononuclear cells and fibrosis that expanded the renal interstitium of monkeys, but lacked necrosis or degeneration of tubules.
It should be noted that kidney lesions with either CAR-T therapies or CPIs do not fit the classical definition of BAIRD (biologics-induced autoimmune renal disorders) as neither are really autoimmune disorders, but instead immune-mediated disorders. The immune stimulation is exogenous in origin. Further, these kind of effects by CAR-Ts and CPIs, while BAIRD-like, do not fit neatly into the three common presentation categories for classification of mechanism noted earlier (associated with systemic vasculitis, representing isolated autoimmune renal disorders or lupus-like syndromes). It has been suggested that BAIRD might better fit an acronym for “Biologics Associated Immune-mediated Renal Disorders” which would be a more inclusive term (Piga’s original paper only designated the acronym as “AIRD due to Biologics” and later authors added the “B” so the acronym is not yet established in stone).4,6,11,38 This latter designation would then more closely fit with animal toxicity findings related to immunomodulatory therapies, where interstitial inflammation in the kidney has been identified with some of these new-generation alternative classes of medicine affecting STING and interferon pathways. 38 At present, these nonclinical immunomodulatory toxicities may only represent BAIRD-like lesions since BAIRD has not been accepted as a classification scheme in the nonclinical toxicology community. This gap in agreed-upon terminology between humans and nonclinical species is unfortunate, since ADA-related immune complex glomerulonephritis in monkeys is also considered BAIRD-like. Using terms such as “BAIRD-like” may only confound and confuse clinical trial physicians and pharmaceutical scientists who are trying to determine clinical translatability of such kidney lesions. For example, ADA-linked immune complex glomerulonephritis has no clinical relevance and is not predictive of clinical toxicity, whereas immunomodulatory biologics that induce inflammatory interstitial renal disease may signal a low, but potentially important renal toxicity signal for patients. Whatever the nonclinical immune-mediated renal disorders associated with biologic therapies are classified as, they obviously do not represent a single group with similar clinical relevance, and with some exceptions, do not represent the same type of lesion that encompasses BAIRD in humans. It must be stressed that even in clinical terms, BAIRD is not a diagnosis, but an overall clinical classification scheme of lesion type based on mechanism. In this context, BAIRD classification of a lesion is not intended to be utilized by pathologists and toxicologists as proper nomenclature for nonclinical lesions, but instead only as a way to group DIKI cases with similar pathogenesis. Nomenclature aside, an understanding of clinical BAIRD can help to highlight the potential of a biologic drug to induce immune-mediated lesions in rare patients and to illustrate that the nature and type of lesions produced in animals is often quite different and not necessarily clinically predictive. Whether immune-mediated lesions in kidneys of animals are classified as BAIRD or BAIRD-like are therefore not as important as understanding why and how these lesions develop and how they may translate between the various species.
Targeted Therapies With Small Molecules and Monoclonal Antibodies
Nephrotoxicity with molecular-targeted therapies can arise from direct effects on the specific pharmacologic target, if the target is expressed in normal kidney. Anticancer therapies that affect kinase pathways, and particularly antiangiogenic agents that target the physiologic inhibition of VEGF, including sunitinib, sorafenib, and axitinib have been associated with thrombotic microangiopathy, glomerulonephritis, as well as proteinuria in patients. 39 However, not all kidney effects in this class of anticancer agents are solely related to VEGF inhibition as these agents affect many other tyrosine kinases which have on- and off-target effects in kidney. Sorafenib, sunitinib, and axitinib are all considered multikinase inhibitors and alteration of other kinase pathways may augment renal toxicologic responses. The mechanism for the renal lesions with drugs targeting VEGF pathways are, therefore, multifactorial, but some specific changes in the glomeruli and endothelium are directly target-related effects. VEGF is normally expressed in glomerular podocytes, and VEGF receptors are present on endothelial, mesangial, and peritubular capillary cells. Glomerular injury may develop from loss of VEGF effects on maintaining the filtration barrier, as well as by downregulation of tight junction proteins.39-41 Bevacizumab, a targeted monoclonal antibody, also binds and inhibits VEGF, and can be associated with glomerular effects and pseudothrombi that may arise from endothelial leakage followed by subendothelial accumulation of serum proteins. 40 In a study of 17 renal biopsies from patients taking bevacizumab that had suspected drug-related renal compromise, all had evidence of microangiopathy with pseudothrombi and multiple patients were diagnosed with nephrotic syndrome.40,42 Glomerular effects, including proteinuria, have been noted in nonclinical studies with VEGF inhibitors, with more pronounced changes including glomerular dysmorphogenesis noted in juvenile toxicity studies in rodents. 2 Bevacizumab administration to rats results in damage to podocytes and associated membrane proteins and this is thought to be the mechanism across species. 43
Other targeted chemotherapeutics have also resulted in nephrotoxicity. EGFR inhibitors have been associated with proteinuria, IgA nephropathy, and acute tubular necrosis. Cetuximab and panitumumab cause direct cytotoxic effects on renal tubules and AKI. Hypomagnesemia results from the inhibition of ion channel transport functions where the EGFR is co-localized. EGFR is expressed in collecting ducts, and glomerular mesangial and parietal epithelial cells, and EGF is involved in maintaining tubular integrity and function. 41 The tyrosine kinase c-kit inhibitors such as imatinib and dasatinib have resulted in thrombotic microangiopathy, glomerulonephritis, proteinuria, and hypertension in some patients. 44 Vemurafenib, a BRaf inhibitor, has resulted in increased plasma creatinine by the inhibition of creatinine tubular secretion as well as degenerative renal effects. 41 However, recent data suggest that the renal changes are not pharmacologically mediated and instead are off-target effects related to the inhibition of ferrochelatase. 42 Other BRaf inhibitors show no similar adverse effects in kidney and were not nephrotoxic in patients, further indicating this renal effect is unrelated to pharmacologic inhibition of BRaf pathways. While vemurafenib administration resulted in moderate AKI and tubular degeneration in mice after only 14 days, BRaf inhibitors other than vemurafenib have not been associated with significant kidney effects in nonclinical studies. 42 Dabrafenib resulted in distal tubule toxicity in juvenile rodents, but the finding has been shown to be species and age specific and does not translate to patients. 45
Antibody-Drug Conjugates
Antibody-drug conjugates (ADCs) are a class of cancer therapeutics composed of a chemically linked antibody and a cytotoxic drug. Some of the more commonly used cytotoxic moieties are the auristatins such as mono-methyl auristatin E (MMAE) or mono-methyl auristatin F (MMAF). Auristatins induce cell necrosis in tumors via microtubule depolymerization. Some of the older-generation ADCs used for oncologic indications were associated with significant nephrotoxicity and hepatotoxicity. However, newer-generation ADCs such as belantamab mafodotin have MMAF linkages which do not cleave extracellularly or in plasma, and this appears to have markedly reduced the nephrotoxic potential clinically. 46 Renal pathology was noted in preclinical toxicity studies in animals given belantamab mafodotin at high doses, including tubule degeneration, with characteristic bizarre karyomegalic nuclei related to microtubule disruption by MMAF. 38 In addition, and as noted in the 2020 FDA summary basis of approval for this drug, ADA-related immune complex formation resulted in glomerulonephritis in monkeys, but these changes were considered species-specific immunogenic lesions based on positive immunohistochemical stains for immune complexes. Increases in creatinine and/or rare incidences of renal compromise have been noted in patients given belantamab mafodotin, as well as in patients given brentuximab vendotin (an antibody bound to MMAE) but renal insufficiency and related co-morbidities are a common manifestation for the respective cancer patient populations. It thus appears these drugs do not play a significant factor in potentiating kidney effects, and renal adverse events in patients on either drug were considered due to underlying disease factors unrelated to treatment.46-49 Because higher MMAF/MMAE systemic exposures often occur in renally compromised patients given belantamab mafodotin/ brentuximab vendotin, extrarenal adverse reactions are more frequent relative to those with normal renal function.47,49
Antisense Oligonucleotides and siRNAs
In the past 5 to 10 years antisense oligonucleotides (ASOs) and silencing RNAs (siRNAs) have increasingly achieved clinical success. The single-stranded 2-methoxyethyl phosphorothioate-substituted (PS) ASOs are the most common type currently marketed, represented by mipomersen, nusinersen, and inotersen. They bind to proteins in serum, on the cell surface, and within cytoplasm, potentiating the possibility for toxic interactions. 50 ASOs utilize RNAse H degradation of mRNAs for inhibitory activity, but successful use in pharmaceutical interventions has been potentially limited by selective uptake into specific cell types. This has been circumvented by ASO versatility in delivery, using intravenous, subcutaneous, intraocular, and intrathecal administration. Specific organ and tissue targeting has been achieved via GalNAc conjugation and glucagon like peptide 1 receptor (GLP1r) agonist conjugation to selectively target liver and pancreas, respectively.50,51 In contrast, double-stranded siRNAs, represented by the recently approved treatment patisiran, are 20- to 25-nucleotide-long duplexes that load into the RNA-induced silencing complex (RISC) for mRNA inhibition. 52 They are cleared rapidly in urine if delivered as unconjugated molecules, and therefore must either be formulated in lipids or nanoparticles, or be chemically modified or conjugated to cell surface ligands (e.g., GalNAc) for effective tissue delivery. 53 A few ASOs and siRNAs have resulted in off-target nephrotoxicity in rodents or monkeys related to aptameric binding to renal epithelial cytosolic proteins.5,54 These include renal tubule toxicity associated with some locked nucleic acid (LNA) ASOs, which appear to lack a clinical correlate. 54 Fortunately, drug candidates of either class that are inherently nephrotoxic or hepatotoxic are identified in nonclinical toxicity studies and terminated early in development.,53,55 Other instances of renal tubular and glomerular toxicities with some 2-oMe and 2-MOE PS ASOs have been reported in rodents but similarly do not appear to translate clinically to patients.5,55,56 Glomerulopathy and mesangial hyperplasia have been noted in monkeys with the same class of PS ASOs, but this toxicity is related to monkey sensitivity to complement and enhanced complement responsiveness, thus it also has very little clinical relevance.57,58 Rarely ASOs have shown increased creatinine/AKI in patients in early clinical trials but these have discontinued development.59,60 Hence, marketed RNA therapeutics are considered reasonably safe for patients, but there are some examples of renal adverse events (noted below) that should be monitored for in at-risk patients. In a retrospective study, effects of eleven 2-MOE ASOs on renal function were assessed in 2435 patients from 32 clinical trials. Authors found no evidence of clinically significant renal dysfunction after up to 52 weeks of treatment. 59 Unfortunately, three cases of glomerulonephritis with inotersen were not included, and the meta-analysis was further limited by a very small number of patients with pre-existing renal disease (n = 18, 6 of which on placebo). There have been well publicized, albeit rare, adverse renal events with ASO therapy, including with drisapersen and inotersen.5,60,61 These few cases were considered drug-related and involved rapidly progressive glomerulonephritis (RPGN) that developed during treatment. Patients with underlying glomerular pathology or predisposition for immune complex formation are considered at increased risk.5,60
The situation with siRNAs appears different, as glomerulonephritis has not been identified in patients given this class of RNA therapeutics. GalNAc conjugation of patisiran (a marketed siRNA and one of several similar drugs targeting liver indications) limits the amount of siRNA that can enter the renal tubular epithelium, thus alleviating much of the nephrotoxic risk. 53 However, basophilic granules in renal epithelium, and vacuolated macrophages, both nonadverse findings representing drug accumulation, are noted in the kidneys of animals given many siRNAs, as they are with ASOs.5,52,61
Conclusion
Although serious adverse events in the kidney with drug therapy are changing from the classical presentation of small molecule tubule toxicity, the potential for rare clinical cases of drug-induced nephrotoxicity remains a concern with alternative classes of medications (Table 1). Detecting and monitoring for these rare occurrences of immune-mediated renal disease including glomerulonephritis and AIN will become an increasing concern for physicians and scientists involved in drug development as alternative classes of medicines play an ever greater role in the pharmaceutical landscape. Vasculitis and glomerulonephritis in monkeys given biologic therapies continue to occur commonly in nonclinical studies, but have little or no clinical relevance. In contrast, BAIRD occurs in a small but significant number of human patients given biologic therapies, especially those with significant immunomodulatory pharmacologic activity. Some of these agents do have similar renal lesions noted in kidneys of preclinical species, so the recognition and differentiation of BAIRD-like lesions in animals from ADA-related immune complex effects is an emerging and important area of interest for toxicologists and pathologists involved in drug development.
Examples of drugs from alternative medicine classes that have the potential for nephrotoxicity in rare clinical patients.
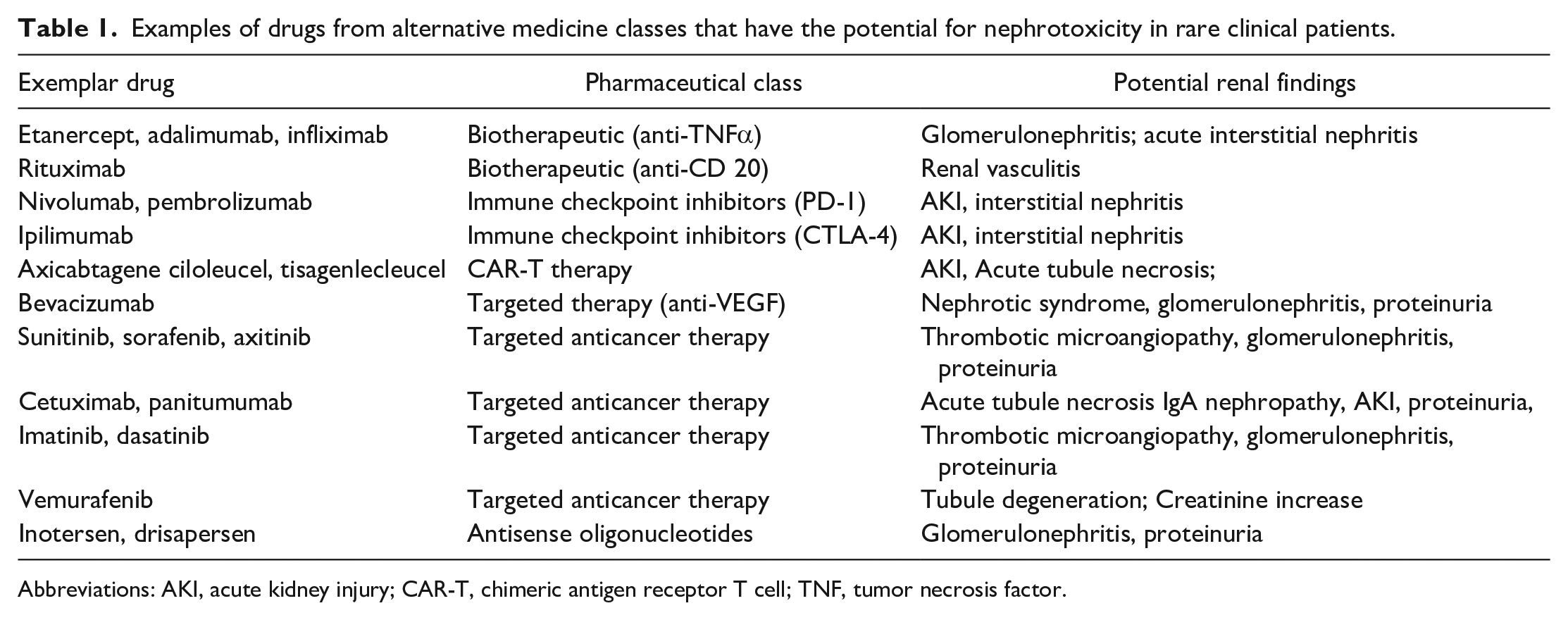
Abbreviations: AKI, acute kidney injury; CAR-T, chimeric antigen receptor T cell; TNF, tumor necrosis factor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.