
Abstract
Nephrotoxicity is one of the more common causes of attrition in nonclinical drug development. Like most tissues, the kidney has a limited number of ways of responding to toxicological insults from diverse mechanistic pathways, which can limit the ability to determine mechanisms of renal injury using the assays routinely performed in preclinical toxicologic studies. In situations where the renal injury is unusual in morphology or if a therapeutic margin is low, additional investigative techniques may be needed to identify a potential mechanism of toxicity in order to inform clinical risk assessment or establish human relevance and translatability of the toxicity. While routine microscopic evaluation can suggest a specific pathogenesis, understanding the mechanism of renal injury often requires additional hypothesis-driven investigations and specialized techniques to obtain the data necessary to identify a nephrotoxic mechanism. Nonclinical mechanistic investigations can be resource-intensive and often yield limited new information. Although there are multiple avenues to investigate renal toxicity, no single mechanistic study or prescriptive battery of tests will identify the pathophysiologic basis for every potential mechanism of renal injury. To aid the nonclinical investigator, we outline a tiered approach for prioritizing investigations to provide a rational and linear road map for the exploration of mechanisms of drug-induced kidney injury.
Note: This is an opinion article submitted to the Toxicologic Pathology Forum. It represents the views of the authors. It does not constitute an official position of the Society of Toxicologic Pathology, British Society of Toxicological Pathology or European Society of Toxicologic Pathology, and the views expressed might not reflect the best practices recommended by these Societies. This article should not be construed to represent the policies, positions, or opinions of their respective organizations, employers, or regulatory agencies.
The kidney is a common target organ in clinical drug development, and nephrotoxicity is often encountered in nonclinical toxicology studies. Renal injury can occur through direct effects on tubules or glomeruli or indirectly via altered hemodynamics (Frazier et al. 2012). Appropriate evaluation of drug-induced kidney injury (DIKI) requires integration of data from histopathology assessment with macroscopic findings, kidney weights, and clinical pathology. A renal hazard identification and risk assessment strategy is then developed using these data alone or in combination with specialized assays or investigations in a tiered approach. Once nephrotoxicity is observed nonclinically, the toxicologist and pathologist are often asked or expected to provide an explanation or pathophysiologic mechanism to clinicians and regulatory authorities to provide some level of confidence that safety margins will be adequate to inform clinical dosing to avoid nephrotoxicity in clinical trials. In some cases, this is straightforward, as with the well-characterized pathophysiology and lack of clinical relevance of chronic progressive nephropathy in rats, amyloidosis in CD-1 mice, or α2u-globulin nephropathy in male rats (Frazier et al. 2012; Frazier and Seely 2013; Seely and Frazier 2015). However, in other cases or with new pharmacologic targets or xenobiotics, the mechanism of a toxicity is often unknown, requiring project teams to conduct a series of experiments to enable further development of the drug. This can lead to numerous investigative studies with complicated findings that are at best difficult to interpret and, in many cases, provide little or no useful information for clinical safety risk assessment. For example, gentamicin, cisplatin, and cyclosporine, the three most commonly utilized nephrotoxic drugs in animal model studies, share decades of mechanistic investigations with thousands of peer-reviewed publications. Yet, for each of these drugs, the precise mechanism of nephrotoxicity remains controversial, and multiple mechanisms that can be contradictory or redundant are described (Quiros et al. 2011; Reasor, Hastings, and Ulrich 2006; Pabla and Dong 2008; Issa, Kukla, and Ibrahim 2013). There are many other classical nephrotoxicants where the mechanism of renal injury remains undetermined (Lentini et al. 2017; Morgan, Kaler, and Bach 1998).
Over the past few years, GlaxoSmithKline has used a tiered approach to mechanistic investigations of renal toxicity, a strategy we would like to share with others in the pharmaceutical community. We believe this strategy is rational, cost-effective, and provides the best approach for understanding these toxicities while giving helpful information to clinicians and protecting subjects in clinical trials. Our objective is to consolidate information on the types of nonclinical renal toxicity investigative studies and end points that are readily available, and to describe nonclinical approaches to nephrotoxic hazard identification, characterization, and risk assessment to provide a practical reference for nonclinical and clinical safety scientists. This manuscript focuses on nonclinical renal toxicity assays only, provides a general outline of which investigative assays are available, and indicates the type of clinical or nonclinical data that trigger the need to perform these tests using a tiered approach. While the use of a tiered strategy is encouraged, it is assumed that individual assays or end points in the second or third tiers may be requested specifically by regulatory agencies prior to the conduct of routine (tier 1) assays. In other cases, the specific nature of a drug or xenobiotic agent may suggest a particular mechanism of renal injury that is amenable to a second or third tier approach early in development. Therefore, in some cases, the more routine assays might not be performed or needed prior to conduct of more complicated mechanistic studies. However, in general, conduct of a series of technologically challenging and complicated experiments to characterize mechanism(s) of renal injury should be discouraged in initial discussions of nephrotoxic potential until the core or routine assays have been completed, as these data often provide sufficient characterization of the type and nature of renal injury. Many pharmaceutical companies have internal safety panels with expertise in nephrology, which can provide the pathologist and toxicologist with recommendations on types and availability of investigative studies.
Tier 1 Assays
Histopathology
In nonclinical toxicity studies, the most reliable evidence of DIKI is the demonstration of dose-dependent renal damage such as degeneration, vacuolation, necrosis, or glomerular injury by light microscopic examination. Kidney histopathology in rodents and nonrodents is highly sensitive and generally provides an indication of the mechanism of injury based on the localization or pattern of injury. Routine H&E staining is usually sufficient to identify the location and type of renal insult, but in certain situations, special stains such as Gomori methenamine silver or Periodic acid Schiff (PAS) may be required to assess subtle glomerular or other changes.
Kidney Weight
For proper assessment of renal injury, histopathology should be accompanied by and correlated with kidney weight, clinical chemistry, and urinalysis data, but this is not always possible in candidate selection or other early toxicity studies where urinalyses and kidney weight data may not be routinely collected. Significant changes in kidney weight are a relatively reliable correlate with morphologic and other measures of nephrotoxicity and are assessed routinely in GLP toxicity studies of 14 days or longer. Multiple pathologic processes can cause increased kidney weights, including tubular vacuolation, degeneration, obstruction, and tubulo-interstitial inflammation, given sufficient severity and/or distribution. Mild dose–related kidney weight increases may also occur as an adaptive phenomenon in response to pharmacologic activity of therapeutic agents, for example, with angiotensin-converting enzyme inhibitors. However, modest increases or decreases in kidney weight in the absence of biochemical or morphologic changes should always be interpreted with caution. Correlations between morphologic changes and slight changes in organ weights are not always valid. For instance, glomerular lesions rarely impact kidney weights.
Clinical Chemistry
Renal injury has historically been monitored clinically by blood urea nitrogen (urea), serum creatinine (sCR), and urinalysis. Nonclinically, urea and sCR are routinely included the chemistry panel on GLP studies and, when increased, are supportive of renal damage. However, these markers lack sensitivity and are only elevated when more than half of renal function is compromised in humans (Bonventre et al. 2010, Ferguson, Vaidya, and Bonventre 2008) or more than 75% of renal functional mass is lost in nonclinical species (Hall 2013). Further, interpretation of urea and sCr elevations is often confounded by prerenal factors such as dehydration, diet, systemic hemodynamic changes, muscle mass, and nutritional status, and both sCr and urea values can be influenced by concomitant drug administration in the absence of renal damage. For these reasons, the routine use of terminal urea and sCr measurements in nonclinical toxicology studies do not provide a sensitive indicator of renal function, in comparison with the serial creatinine monitoring used in clinical veterinary and human medicine, where small changes in sCr can indicate the progression of renal injury due to the low within-individual variability of sCR in humans and animals (Keevil et al. 1998; Almy et al. 2002). Other indicators of kidney function such as serum potassium, phosphorous, or calcium can be of additional benefit in supporting a diagnosis of renal compromise but, because of lack of specificity for renal injury, should be interpreted in the context of other clinical pathology findings.
Urinalysis
Analysis of urine from timed (generally overnight) urine collections is an important component of the clinical pathology data evaluated in GLP toxicity studies. When possible, urinalysis should also be added prospectively to exploratory dose range–finding or candidate selection toxicity studies for compounds where nephrotoxicity was observed in prior toxicity studies or with known class effects for renal injury. Recommended parameters include urine volume, urine concentration (as specific gravity or osmolality), visual assessment, and quantitative determination of urinary protein, glucose, and creatinine concentrations. While qualitative urinalysis using urine test strips can provide semiquantitative data on protein, glucose, blood, and leukocyte levels in urine, quantitative measurement of urine protein, albumin, and/or urine glucose excretion on timed collections is generally more precise. Urine sediment evaluation can also be included but is not commonly performed in nonclinical studies because urine sediment changes in DIKI are typically associated with histopathologic findings that better characterize the renal injury.
Urine electrolyte data are occasionally collected for the estimation of fractional electrolyte excretion or renal clearance in nonclinical toxicity studies, but provide limited information in the toxicologic or veterinary setting. Electrolyte excretion data have limited value for risk assessment due to the lack of specificity for renal disease because of extrarenal effects (including diet, strain, age, sex, feeding, hydration status, and circadian effects), and are difficult to interpret due to the large inter- and intra-individual variability inherent in quantitative urinalysis data (Hall 2013; Lefebvre et al. 2008; Pressler 2013; Stoynev and Ikonomov 1983).
Irrespective of the mechanism or type of renal pathology, where renal injury has been noted microscopically, quantitative urinalysis can be a helpful adjunct to characterize and monitor the extent of renal injury or dysfunction. Therefore, when nephrotoxicity is seen in initial toxicity studies, interim urinalysis data can be collected prospectively in subsequent studies of longer duration at timepoints and doses where microscopic evidence of test article–related renal injury was detected earlier. Use of this approach can efficiently maximize information collected from nonclinical studies to guide clinical decision-making and minimize the use of both animals and scientific resource.
Tier 2 Assays
For most cases of DIKI, tier 1 nonclinical assays including histopathology, serum chemistry, and quantitative urinalysis are sufficient to characterize the nephrotoxic hazard and provide adequate information for clinical risk assessment and decision-making. However, in situations where regulatory authorities or clinicians need further information on the nephrotoxic potential or mechanism of an observed DIKI, tier 2 assays can be added prospectively as additional end points on toxicity studies. The most common tier 2 assays currently used in nonclinical species are measurement of specific urinary proteins that can localize renal injury or identify compromised renal function. Other tier 2 assays used to help identify pathophysiologic mechanisms include electron microscopy, glomerular immunostaining, and quantitative whole body autoradiography (QWBA) data to assess renal metabolism. Specifics on these assays are described below.
Urine Biomarkers
As a “proximate” biofluid, urine offers an advantage over serum by increasing marker specificity for monitoring of renal injury. In addition to quantitative measurement of traditional analytes such as protein, albumin, or glucose, novel proteins identified through -omics platforms that are specific to either defined nephron segments or pathologic processes are increasingly being used to noninvasively characterize DIKI in nonclinical and clinical studies (Brott et al. 2015; Cardenas-Gonzalez et al. 2016). These urinary markers include serum proteins that passively enter the urine by glomerular filtration or through glomerular and/or tubular injury, and proteins that are upregulated within the kidney in response to renal injury. Based on characteristics unique to each marker such as localization to specific segments of the nephron, constitutive versus upregulated expression, or association with specific pathologic processes, the use of a panel of exploratory urinary biomarkers can provide information on the timing, location, and extent of DIKI.
Consortia involving collaborations across industry, academia, and regulatory agencies have recently qualified several urine biomarkers in the rat (FDA 2018a). Several of these markers have received a Letter of Support encouraging exploratory use in humans, as have several other markers for use in rat (FDA 2018b). Many of these markers can be measured in other nonclinical species (Wagoner et al. 2017; Gautier et al. 2016) and humans (Brott et al. 2014; Brott et al. 2015). A subset of these and other markers for use in nonclinical studies, their relationship to function or nephron segment localization, species applicability, and considerations for use are detailed in Table 1.
Selected Urine Biomarkers of Acute Renal Structural Injury or Functional Compromise.
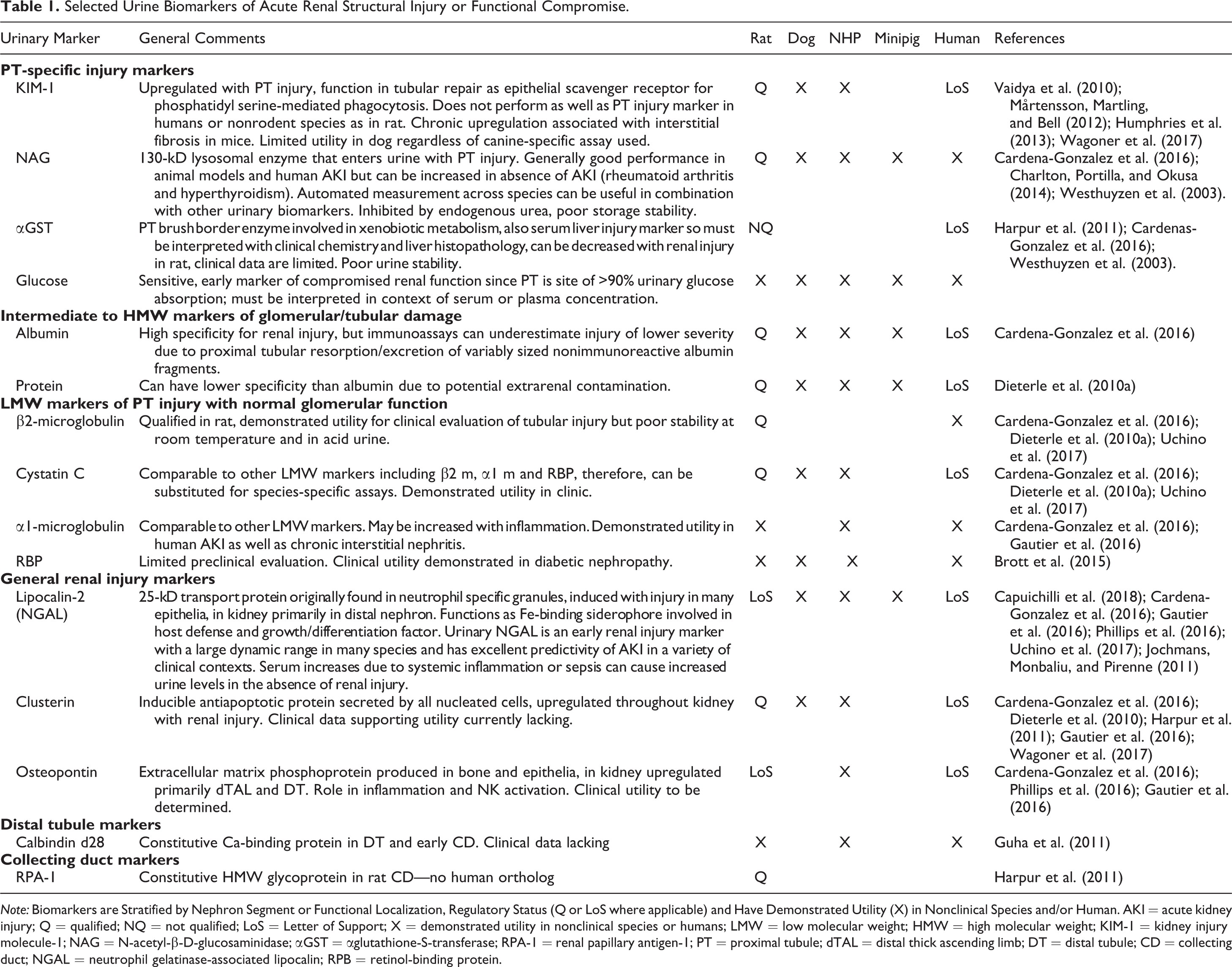
Note: Biomarkers are Stratified by Nephron Segment or Functional Localization, Regulatory Status (Q or LoS where applicable) and Have Demonstrated Utility (X) in Nonclinical Species and/or Human. AKI = acute kidney injury; Q = qualified; NQ = not qualified; LoS = Letter of Support; X = demonstrated utility in nonclinical species or humans; LMW = low molecular weight; HMW = high molecular weight; KIM-1 = kidney injury molecule-1; NAG = N-acetyl-β-D-glucosaminidase; αGST = αglutathione-S-transferase; RPA-1 = renal papillary antigen-1; PT = proximal tubule; dTAL = distal thick ascending limb; DT = distal tubule; CD = collecting duct; NGAL = neutrophil gelatinase-associated lipocalin; RPB = retinol-binding protein.
Although many of these markers monitor similar types of renal functional loss or injury, they generally are evaluated concurrently because of differences in marker biology, species cross-reactivity, or storage stability. For example, low-molecular-weight markers such as β2-microglobulin, retinol-binding protein, or cystatin C freely pass the glomerular filtration barrier, and presence in urine suggests impaired tubular absorption, whereas intermediate or high-molecular-weight proteinuria is considered indicative of concomitant glomerular and tubular disease. Also, while both urinary albumin and protein reflect tubuloglomerular disease, proteinuria may be less specific for renal injury because of potential lower genitourinary tract contamination. Urinary proteins such as kidney injury molecule-1 (KIM-1) or renal papillary antigen-1 (RPA-1) can localize renal injury to proximal or distal nephron, respectively, and can be upregulated in response to renal injury (KIM-1) or constitutively expressed (RPA-1). In contrast, clusterin and lipocalin-2 (neutrophil gelatinase-associated lipocalin [NGAL]) are upregulated in many nephron segments with nephrotoxic injury. For low-molecular-weight markers of proximal tubular injury, β2-microglobulin was qualified in the rat, but it is acid labile and can have high variability due to poor storage stability. For this reason, other markers such as retinol-binding protein and urinary cystatin C are preferred in dog, and α1-microglobulin can be favored in the clinic (Brott et al. 2015; Vaidya, Ferguson, and Bonventre 2008). KIM-1 has performed well in the rat but has not proven to be a sensitive marker in the dog (Wagoner et al. 2017) or minipig (K. Lynch, personal communication). In contrast, NGAL and clusterin have largely been effective in rat, dog, nonhuman primate, and minipig (Wagoner et al. 2017; Gautier et al. 2016; Phillips et al. 2016).
Newly qualified urine biomarkers should not be routinely included on all nonclinical toxicity studies. Instead, they should be employed prospectively in selected nonclinical studies only upon identification of drug-induced renal microscopic lesions in initial nonclinical toxicity screening or subacute GLP toxicity studies when their use may provide information for clinical risk assessment. As with all biochemical data, interpretation of changes in these markers should be done in the context of concomitant changes in histopathology, urea, sCR, traditional quantitative urinalysis, and renal weight data. In this way, findings can be put into proper context with other supporting data. Inclusion of multiple urine analytes measured in parallel can increase the sensitivity and specificity of identification or confirmation of DIKI by urinary biomarker changes. The elevation of a single exploratory parameter in isolation, while potentially informative, should not be interpreted as compelling evidence of renal toxicologic injury and should not be the primary basis for decision-making.
Novel urinary biomarkers should not be added to definitive GLP study designs simply because renal pathology was noted in candidate selection studies, particularly when these changes were only observed at nontolerated doses. Urinary biomarker evaluation is also not indicated when renal effects are only noted above the MTD or at doses where there are mortalities. Potential triggers for inclusion of urinary biomarkers (or other tier 2 assays) in subacute or chronic toxicity study protocols might include the presence of renal pathology in previous studies and one or more of the following: Presence of renal pathology in both rodent and nonrodent species. Little or no toxicologic cover between exposure at which the renal lesions are noted nonclinically and the expected or measured exposures at the proposed clinical dose. Very rapid onset ( Clinically determined need for monitoring urinary biomarkers in patients, where inclusion of urinary biomarkers in a nonclinical study might confirm effectiveness of a marker for a specific manifestation of renal injury. Drug indication for kidney disease where target patient population with renal impairment poses greater concern.
It must be stressed that the inclusion of exploratory urine biomarkers in clinical trials with a compound does not necessitate the use of such markers in future nonclinical studies with that compound, except where their use in animal toxicity studies may provide clinicians with additional information on the timing or mechanism of injury. Conversely, inclusion of urinary biomarkers in nonclinical studies does not necessitate their measurement in human trials but is determined by therapeutic dose margin, presence of other renal signals, drug indication, or target patient population.
At present, these next generation urinary biomarkers are considered exploratory and have only been qualified in the rat or evaluated in humans (Brott et al. 2014; Brott et al. 2015), and many have received regulatory support in the form of a Letter of Support. While many assays for these urinary proteins are available for use in the dog, cynomolgus monkey, and minipig (Table 1), the majority of the exploratory urinary marker data in dogs and monkeys currently in the public domain were obtained from studies that used a limited number of toxicants, primarily gentamicin and cisplatin, with rare inclusion of development compounds. It is unlikely that these markers will undergo a robust biologic qualification process in the collaborative precompetitive space in nonrodents as was conducted in the rat, therefore biological characterization of these next generation renal markers will require a prolonged and iterative learning process. However, with the increased use of these markers in nonrodent toxicology studies, a robust biologic qualification evaluation could be performed if sponsors were willing to share anonymized biomarker and histopathology data to a meta-analysis to more objectively assess utility of these markers in nonrodents for drug development.
For all nonclinical species, urine protein, albumin, glucose, and n-acetyl-β-d-glucosaminidase (NAG) can be measured on automated analyzers and provide readily translatable indicators of proximal tubular injury or functional compromise. In addition, NGAL, an inducible protein marker has demonstrated utility across species as a general renal injury marker. In all cases, the choice of exploratory markers should include several parameters measured simultaneously in a study. As emphasized earlier, study designs should include sCR, urea, and quantitative urinalysis of some or all of the above traditional parameters for comparison with histopathology and novel urinary parameter data.
Many years of testing will be required before there is consensus on the optimal selection of markers for evaluation of early acute kidney injury or what types of injury are best diagnosed by which marker. No single biomarker will likely be applicable across the varied contexts and temporal presentations of nonclinical investigative or toxicity study designs; however, the use of these novel urinary markers of renal injury can provide added sensitivity and specificity over serum markers and, in some cases, traditional urinary markers for detection and monitoring of renal injury.
Immunohistochemistry or Special Stains
α2u Globulin Nephropathy
Hyaline droplets are frequently found in the cytoplasm of proximal tubules in male rats, generally localized to the S2 segment, and are manifested as variably sized, refractile, brightly eosinophilic ovoid droplets composed of lysosomal accumulations of α2u-globulin. There are a large number of agents (d-limonene, hydrocarbon or petroleum products, and decalin) that will cause α2u-globulin nephropathy, characterized by an increase in droplet number and distribution and/or altered pattern of droplets (Frazier et al. 2012). However, drugs may produce hyaline droplets that are unrelated to α2u-globulin and/or result in drug-related effects that are atypical of this nephropathy. Because α2u-globulin nephropathy has little clinical relevance but other types of hyaline droplets can be clinically important, further evaluation may be needed in some cases. The presence of α2u-globulin in droplets can be determined relatively easily by special procedures such as Mallory Heidenhain, Martius Scarlet Blue, or chromotrope aniline blue stains or by the use of immunohistochemical stains directed against α2u-globulin. Special stains are particularly useful in cases where the presentation is atypical for α2u-globulin nephropathy, such as high incidence in females, presence in a nonrodent species, or presence as very irregularly shaped or sized droplets.
Other Uses for IHC and Special Stains: Mechanistic Studies with Glomerular Injury
The glomerulus is the initial site of exposure for a nephrotoxicant within the nephron, but glomerular changes occur much less commonly than tubular changes in nonclinical toxicologic studies. However, with the increasing prevalence of biopharmaceuticals and complex macromolecules (e.g., antisense oligonucleotides) in active drug development, glomerulonephritis and other related glomerular changes have recently been noted with greater frequency in association with immune complex (IC) disease (Frazier et al. 2015). Damage may result from effects on specific cell types (podocytes and mesangial cells), effects on the vascular supply, or from impairment of the charge- or size-selective properties of the glomerulus. Due to the lack of a specific biomarker of glomerular damage, it often is useful to do mechanistic studies to determine the type and nature of glomerular injury. Since glomerular cell types are often difficult to differentiate with routine H&E stains, particularly with glomerular pathology, PAS stains, silver-based stains, or specific immunohistochemical stains may be utilized to better identify cells of the glomerulus. Both PAS and silver stains may help delineate the mesangium, but silver stains may also help differentiate details of the basement membrane since they will specifically stain the lamina densa. PAS stains also help delineate details of the capillary loops. Immunohistochemical stains for synaptopodin will specifically stain podocytes, while immunostains for nephrin target the adjacent slit diaphragms of the podocytes, von Willebrand factor delineates glomerular endothelial cells, and CD90/thy-1 labels mesangial cells in the rat. Immunohistochemistry can be particularly useful in determining the presence of IC disease in monkeys given biotherapeutic agents. Stains directed against IgG, IgM, and complement fragments, as well as demonstration of the peptide or antibody itself within a glomerulonephritis or renal vasculitis, can be definitive evidence of IC disease (Rojko et al. 2014; Frazier et al. 2015). This information is vital, as an IC mechanism, especially when related to antidrug antibodies, may have little or no clinical relevance. In practice, however, IHC is usually not necessary, as most cases of IC glomerulonephritis have characteristic morphology, measurable antidrug antibody, and/or significant and accompanying decreases in systemic drug exposure. Atypical cases lacking these features may warrant inclusion of tissue IHC to help confirm IC suspicion.
Electron microscopy can be of particular benefit in demonstrating ultrastructural changes within the glomerulus when alterations are noted with routine stains in animals on toxicologic studies. Ultrastructural examination in concert with immunohistochemistry is often recommended in these situations. Ultrastructural examination has been effective in demonstrating inclusions in podocytes, mesangial cells, or endothelium and is particularly effective at characterizing fibrillar deposits (Frazier et al. 2014). Electron microscopy is not a particularly effective means of determining toxicologic mechanisms of tubular injury and is rarely performed for this purpose, except where phospholipidosis is suspected.
Tier 3 Assays
Several other assays, methodologies and special techniques are available that may be used in specific situations to address regulatory questions regarding nephrotoxicity and mechanisms of renal injury. These techniques and assays are not recommended for routine addition to toxicity studies or to nonclinical regulatory packages, but are used in specific situations where routine or core assays fail to address safety concerns. The addition of tier 3 assays should be done in consultation with advisory panels or, if necessary, with regulatory authorities. They should be designed to address specific questions or concerns and be focused on particular suspected mechanisms.
QWBA
QWBA is a technique where a single dose of radiolabeled drug is given to partially pigmented rats, and the distribution of radiolabel is monitored throughout the body over time. QWBA studies are performed routinely by drug metabolism/pharmacokinetic analysts during development and may be helpful in elucidating possible mechanisms of nephrotoxic injury associated with extensive renal uptake or retention of a drug in kidney tissue. Furthermore, when nephrotoxicity is a concern, microautoradiography of sections of kidney obtained in a QWBA study can provide insight into the cellular distribution or accumulation of drug-related material in the kidney. Several nephrotoxins have demonstrated marked uptake and increased or prolonged accumulation in the renal cortex or medulla. Examples include aminoglycoside antibiotics and antisense oligonucleotides (Geary 2009; Hasegawa et al. 1994). One limitation of routine QWBA is that the images, although quantitative, cannot distinguish parent drug from metabolites.
Matrix-assisted Laser Desorption/Ionization
Matrix-assisted laser desorption/ionization (MALDI) imaging has emerged as a powerful technique for analyzing the spatial arrangement of proteins, peptides, lipids, small molecules, and metabolites in tissues such as kidney. Because MALDI imaging does not require generation of a radiolabeled drug, lead times to the start of MALDI studies are shorter than for QWBA studies. In addition, this tier 3 assay can be utilized to gain qualitative spatial views of drug and metabolites in kidney subregions and can provide more complete characterization of metabolite lipid, protein, or mineral composition. In our hands, MALDI has been successfully utilized to localize and image drug product at the site of kidney injury as well as to determine the makeup and character of crystals and deposits within tubules (Groseclose et al. 2015). MALDI has thus been highly effective in helping to inform the toxicologic mechanism of some nephrotoxic drugs in rodents. As more institutions become familiar with the technique, MALDI will continue to gain regulatory acceptance in mechanistic toxicologic investigation.
Renal Blood Flow (RBF) Measurement
Measurement of changes in RBF associated with the administration of a compound might be required in cases where the morphologic changes associated with DIKI are suggestive of transient or sustained vascular compromise or reduced renal clearance. Potential triggers for RBF evaluation would be the presence of renal ischemia and one or more of the following: a reduction in systemic arterial pressure (>20 mmHg), a profound reduction in glomerular filtration rate (GFR), significant elevations in sCR or urea, and/or a reduction in urine output.
Ischemic necrosis tends to follow a zonal distribution involving the corticomedullary junction during diffuse organ hypoperfusion, or as wedge-shaped infarcts when occlusion of specific branches of the arcuate arteries occurs (Frazier and Seely 2013). The distal straight segment of the proximal tubules and the thick ascending limb are particularly sensitive to hypoxia due to their high metabolic and transporter activity. When injury is suggestive of an ischemic pathophysiology, and particularly when a compound is found to have vasomodulatory properties in cardiovascular safety pharmacology studies, it may be advantageous to evaluate RBF after administration. RBF can be determined by a variety of imaging techniques, and RBF with simultaneous measurement of GFR can help in differentiating renal hemodynamic effects from other mechanisms of injury (Feingold et al. 2010; Houbois et al. 2018; Mariager et al. 2018). Investigators have developed and optimized techniques for quantitatively assessing organ perfusion using flow cytometric analysis of fluorescent microspheres to measure the effect of various interventions on regional blood flow (Prinzen and Bassingthwaighte 2000). One set of microspheres is injected intra-arterially prior to dosing to establish a baseline, and additional doses of microspheres are injected at up to 3 timepoints postdose. The difference in fluorescence intensities in kidney extracts is proportional to the change in RBF. There are also a variety of other techniques that can be used, and these would most likely be done at academic research institutions.
GFR Measurement or Estimation
GFR has been shown to be decreased after as little as a 20% decrease in renal function, so decreased GFR can potentially demonstrate drug-induced renal damage prior to increases in urea or sCR. Due to expense and logistical challenges, however, GFR measurement is rarely performed in either clinical drug safety evaluation or clinical practice and is more often simply estimated via creatinine clearance using widely accepted formulas. Estimated GFRs are routinely calculated in clinical studies, and when renal signals are noted, subjects may be referred to nephrologists for further evaluation. When measurement of GFR is requested in clinical studies, this generally is performed in specialty centers in prospective studies with small numbers of individuals.
Despite recent improvements in GFR measurement in animals, it is not clear that GFR data increase sensitivity for monitoring laboratory animals for nephrotoxicity or provide additional insight into the mechanism of renal injury in nonclinical studies. Renal safety pharmacology studies are not specifically required by worldwide regulatory guidelines for nonclinical testing of pharmacologic agents (ICH S7A and B), but they have historically been used as adjunct investigations to address the extent or mechanism of injury to the kidney once renal lesions have been identified in toxicity studies. However, direct measurement or estimation of GFR is rarely considered as part of a renal safety pharmacology study for similar technical reasons in nonclinical species as in humans and, also because of the availability of exploratory renal biomarkers that may be more sensitive or altered earlier in renal injury (Hamdam et al. 2013). There are rare circumstances where GFR determination in nonclinical species may have merit, for instance, where a compound is suspected to cause DIKI in humans but lacks histologic evidence of renal injury, or where changes in novel renal biomarkers occur in nonclinical toxicology studies without accompanying histopathologic changes in kidney. The most commonly performed assays in animals involve measurement of GFR via renal clearance. GFR can be calculated based on the fractional excretion of creatinine but is most precisely determined by measuring the clearance of compounds such as inulin, iohexol, or iothalamate. Of these, inulin is considered the gold standard for GFR determination in animals as in man since inulin is inert, nontoxic, freely filtered through the glomerulus, and neither secreted nor reabsorbed. While inulin clearance is relatively straightforward in the dog, it is more difficult to measure accurately in rodents. New transcutaneous techniques have recently become available to noninvasively and continuously monitor GFR in rodents and dogs (Friedemann et al. 2016; Schock-Kusch et al. 2011; Wang et al. 2012).
Creatinine Clearance Measurement
Creatinine is cleared primarily by the kidneys by filtration and active secretion, with little involvement of renal reabsorption, thus creatinine clearance (Clcr) is often used as a surrogate for GFR. Creatinine clearance is used most often in human patients in clinical trials but can also be performed in animal studies. It has been particularly useful in cases where creatinine is elevated without any other concomitant elevations representing renal injury or histologic damage. In several of these cases, results have identified a physiologic or pharmacologic perturbation in creatinine excretion by the drug or agent. However, Clcr may overestimate GFR due to active secretion by peritubular capillaries and proximal tubule, and is subject to effects unrelated to GFR such as decreased tubular creatinine secretion due to inhibition of renal tubular transporters by xenobiotics. Other methods have been used to improve accuracy of GFR determination, including application of correction factors to creatinine measurements and estimation via endogenous markers such as serum cystatin C, however, these methods are not validated in nonclinical species. The typical approach to calculate Clcr is to measure sCR in association with urine creatinine and urine volume.
Imaging of Renal Structure and Function
Imaging modalities such as ultrasound (US), magnetic resonance imaging (MRI), and computed tomography can be used for the assessment of renal structural and functional changes related to drug administration and can be safely applied in rodent and nonrodent species, providing end points that can be translated into human patients and clinical trials. US Imaging is considered the gold standard for the diagnosis and management of renal disease in humans and animals (Ferguson and Waikar 2012; Sharkey et al. 2012). Cost-effectiveness, rapid results, ease of use, and safety and translatability of end points make US a useful approach for the assessment of kidney toxicity. In animal species, reduction in size with or without changes in the normal echographic pattern may suggest chronic alterations, while mild enlargement or normal size is more indicative of acute toxicities. In patients, changes in kidney size and volume may be indicative of acute or chronic renal disease, although acute or chronic nephropathies are not always associated with changes in renal dimensions (e.g., HIV-associated nephropathy, diabetic nephropathy, and monoclonal gammopathies). Strong correlation between 3-D US and MRI modalities for changes in renal volume has been reported in rodent and canine models (Feingold et al. 2010).
RBF, as noted above, is a particularly useful assay when ischemic mechanisms of toxicity are suspected and can be estimated with US Doppler modalities, especially with the ability of Color Doppler imaging able to detect high velocity flow to and from the kidney. However, imaging signals can be affected by background noise. To overcome these limitations, Power Doppler modalities have been developed to maximize the ability to evaluate low velocity intraparenchymal blood flow. Using Power Doppler US, it is possible to evaluate regional or generalized changes in RBF due to direct or indirect toxicological effects. Power Doppler applications have been validated in humans for the detection of perfusion abnormalities, renal ischemia, arterial stenosis, and venous thrombosis (Granata et al. 2015).
Urine Metabolomics
Metabolomic approaches have long held interest for nonclinical and clinical renal biomarker discovery, but use in toxicological applications has diminished since 2000 (Robertson, Watkins, and Reily 2011). Successful development of urinary metabolomic markers requires a systems biology approach and meta-analyses of large data sets to identify candidate markers, yet one of the problems with statistical data mining approaches to biomarker discovery, particularly for—omics parameters, is false discovery (Xia et al. 2013). Thus, biological plausibility and role in pathophysiologic processes must be key determinants of candidate renal injury marker selection. Characterization of nonclinical urinary metabolomic parameters for routine use is particularly challenging because of the complexity of variables such as matrix, diet, microbiome, species, sex, and age differences (Emwas et al. 2015, Capati, Ijare, and Bezabeh 2017). Candidate urine metabolomic safety biomarkers also face developmental challenges due to the inconstant volume and composition of urine which creates variability in urinary analytes regardless of normalization practices (Warrack et al. 2009). Metabolomics data might aid prediction of kidney toxicity under controlled experimental conditions and may be of value in investigational studies looking for particular endogenous metabolites. However, use of metabolomics data in nonclinical or clinical decision-making should be preceded by meta-analyses of data from studies that include both nephrotoxicants and nonnephrotoxic compounds that are adequately curated for comparability of elements of study design and data normalization. In addition, translation of urinary metabolomic marker data from experimental model to naturally occurring disease or clinically relevant drug-induced target organ toxicity will require understanding of species metabolic differences. Thus, metabolomics data may be more relevant for understanding biological or metabolic processes than for development of renal biomarkers, particularly safety markers.
Renal Transporter Studies
Many drugs and xenobiotic agents are actively moved into or out of the renal tubular epithelium via organic anionic transporters (OAT), organic cationic transporters (OCT), multidrug and toxic compound extrusion antiporters, ATP-binding cassette transporters, or other agent-specific transporters located on tubular epithelial basolateral and apical surfaces. Exploratory investigations involving these transporters can help identify mechanisms of renal toxicity related to intracellular accumulation of toxicants and metabolites due to transport into or inhibition of export out of the epithelial cell. These prospective investigations are typically initiated after tubular injury has been identified by the pathologist in nonclinical toxicity studies, or in cases where the structure and physicochemical properties of the agent might suggest the possibility of transporter involvement (such as strong anionic or cationic surface groups, limited permeability, or kidney accumulation as seen in QWBA). To address potential mechanisms of accumulation, both in vitro and in vivo transporter studies can be conducted. For example, an in vivo mechanistic study is performed by co-administrating a test compound with inhibitors of OATs and/or OCTs such as probenicid, para-aminohippurate, or cimetidine in a study design that mimics studies where renal lesions were noted previously. The outcome of such a study may demonstrate reduced toxicity in the presence of the transporter inhibitors. Confirmatory assays can also be performed in OAT or OCT knockout mice by administering relevant doses of an agent and comparing lesion severity and onset to controls of the same strain. Because there are numerous transporters and well-characterized species and sex differences in transporter expression in the kidney, it is recommended to consult experts in this area for detailed advice prior to study initiation.
Other Assays
Primary renal cultures and renal slices have been used to characterize toxicologic mechanisms associated with drug-induced renal injury but to date have not been successfully adapted as screening assays. Several commercial in vitro kidney platforms are also available, but in addition to limitations seen with primary cultures, most or all lack true polarity, and most lack consistent cellular transporter expression. To date, the predictivity of in vitro techniques and genomic assays on cultured cell lines of renal origin has been disappointing, except in the case of severe nephrotoxicants such as cisplatin or gentamicin. However, several new kidney-on-a-chip 3-D in vitro methodologies are in development, and it is expected that these may be utilized in the near future as complimentary tools for nephrotoxic screens (Soo et al. 2018). At present, the optimal screen for renal toxicity during early drug development remains the short-term in vivo assay in rodents with a limited microscopic tissue list (e.g., kidney, liver, lung), ideally with urinalysis. These studies can be as short as 4 days, but may be of 7- to 10-day duration and are generally performed in rodents, usually prior to candidate selection. Obviously, these screening studies would be unable to detect toxicities that require chronic dosing to manifest.
Conclusion
In the absence of a clear clinical, regulatory, or program need, chasing down mechanisms of nonclinical toxicity in nonclinical species can be an extremely resource intensive and lengthy endeavor that may yield little information to aid clinical progression. Given adequate clinical margins and experience with typical nonclinical renal findings, drug development can generally safely proceed into clinical trials with the support of only a standard toxicity study package (tier 1 assays) and without a detailed characterization of the mechanism of nephrotoxicity. However, mechanistic studies may be needed to better inform human risk assessment or clinical translation when the nature of a nephrotoxic injury is poorly understood or the safety margin is narrow. This could include cases where there are unusual findings (novel histologic lesions or locations), multispecies involvement, or the need to understand a species-specific nonclinical finding, potential renal biomarker utility, or mechanism of renal injury to aid backup molecule selection. Renal investigative studies should be conducted on an as-needed basis and in a hypothesis-driven fashion. Tier 1 assays include data that are typically acquired in standard (or slightly modified) toxicity studies. While often it is not possible to glean detailed mechanistic pathway information from these studies, the data set will generally permit a histopathological finding to be correlated with physiological changes, thus allowing a clinical pathology end point to be used as a monitorable change in the clinic or provide insight into where further nonclinical investigative effort should be directed. Tier 2 assays are designed to anatomically localize the initiating toxicity within the nephron and/or cell type, primarily narrowing the initiating insult to a glomerular or tubular origin. Depending on the timing, end point, and technique utilized, some of these activities are amenable to use in archived samples or may be prospectively incorporated into a planned toxicity study. Additional assays such as QWBA and urinary drug or metabolite quantification, coupled with pharmacokinetic data from tier 1 assays, can better define drug (or metabolite) disposition and the potential for drug redistribution and accumulation to help strategize clinical dose management. Due to the specialized nature of techniques used in tier 3 assays and the additional time needed for assay validation, use of tier 3 assays should be limited to specific programs in need of clarification of probable mechanistic pathways based on information gleaned in earlier investigational work. Data sets pursued at the tier 3 level are best acquired in dedicated prospective investigative studies that are uniquely designed for sample collection at the appropriate timepoints. For instance, evidence of crystalluria may point investigators toward MALDI evaluation of tubular deposits, while lesions limited to S3 segments may lead to investigations of transporter activity. This tiered approach for investigating mechanistic renal injury, which our institution has now adopted for several years, will continue to evolve, based on empirical institutional experience, rapidly evolving technologies, and as molecular pathways of renal injury become further elucidated.
Footnotes
Author Contributions
Authors contributed to conception or design (DE, KF); data acquisition, analysis, or interpretation (DE, MR, KF); drafting the manuscript (DE, MR, KF); and critically revising the manuscript (DE, MR, KF). All authors gave final approval and agreed to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.