
Abstract
Rhesus and cynomolgus macaques are the most frequently used nonhuman primate (NHP) species for biomedical research and toxicology studies of novel therapeutics. In recent years, there has been a shortage of laboratory macaques due to a variety of competing factors. This was most recently exacerbated by the surge in NHP research required to address the severe acute respiratory syndrome (SARS)-coronavirus 2 pandemic. Continued support of these important studies has required the use of more varied cohorts of macaques, including animals with different origins, increased exposure to naturally occurring pathogens, and a wider age range. Diarrhea and diseases of the gastrointestinal tract are the most frequently occurring spontaneous findings in macaques of all origins and ages. The purpose of this review is to alert pathologists and scientists involved in NHP research to these findings and their impact on animal health and study endpoints, which may otherwise confound the interpretation of data generated using macaques.
Introduction
The demand for nonhuman primates (NHPs) to support biomedical research and the development of novel therapeutics is steadily increasing.1,2 Nonhuman primates are a critical resource for the investigation of aging, cognitive research, and infectious diseases. In a National Institute of Health (NIH) report of NHP use by academic centers between 2013 and 2017, this increase was predominantly driven by the use of rhesus and cynomolgus macaques for HIV/AIDS research. In parallel, the development of more biotherapeutic agents, for which NHPs may be the only pharmacologically relevant species, has resulted in increased use of the cynomolgus macaque in toxicology studies.3,4 As a result, the supply chain of these animals, the vast majority of which are imported to the United States from breeding facilities in China, was already strained prior to the outbreak of severe acute respiratory syndrome (SARS)-coronavirus 2. Since the outbreak in December 2019, the shortage of macaques has been exacerbated due to the sudden surge in their use to develop COVID-19 vaccines and therapeutics in combination with the ban on export of cynomolgus macaques from China.5,6 Critical research and toxicology studies have been forced to utilize a more diverse group of macaques including animals with different origins, increased exposure to naturally occurring pathogens, and a wider age range. As a consequence, pathologists are being exposed to an array of spontaneous and background lesions that have not typically been seen in such studies and must be differentiated from study-related effects. The purpose of this manuscript is to review the literature and authors’ experience of such lesions of the gastrointestinal tract and the various causes of diarrhea, which is a ubiquitous problem in captive rhesus and cynomolgus macaques.
The incidence of diarrhea in macaque colonies varies, but up to 30% of a population may be affected annually.7-11 Individual colonies can have differing endemic infections and/or genetic predispositions to diarrhea than others. Therefore, understanding the background rate and causes of diarrhea in the specific colony from which study animals originated can be helpful. The vast majority of cases of diarrhea occur in juvenile animals (less than 5 years of age), which is frequently the age-group utilized in toxicology studies. There are multiple infectious causes of diarrhea, which will be described below, but in the vast majority of cases, an etiologic agent is not identified. 12 Those idiopathic syndromes with specific pathological features are described. However, pathologists and toxicologists should be aware that diarrhea may also be a consequence of social stress (e.g. weaning/shipping/inadequate acclimatization/single housing/social status), dietary insufficiencies, prior antibiotic therapy, or genetics.13-16 Should diarrhea be a concern in a particular study, a thorough understanding of the clinical history and husbandry of the animals and rectal/fecal culture where appropriate, in addition to anatomic and clinical pathology data, will aid in the assessment of the significance of the findings. Table 1 summarizes the various causes of gastrointestinal lesions, their typical gross distribution, and provides a quick reference to their likely frequency.
Distribution of common diseases of the macaque gastrointestinal tract.

Abbreviations: DDx, differential diagnosis; ICD, idiopathic chronic diarrhea; CMV, cytomegalovirus; GIT, gastrointestinal tract.
Normal Anatomy and Physiology of the Macaque Gastrointestinal Tract
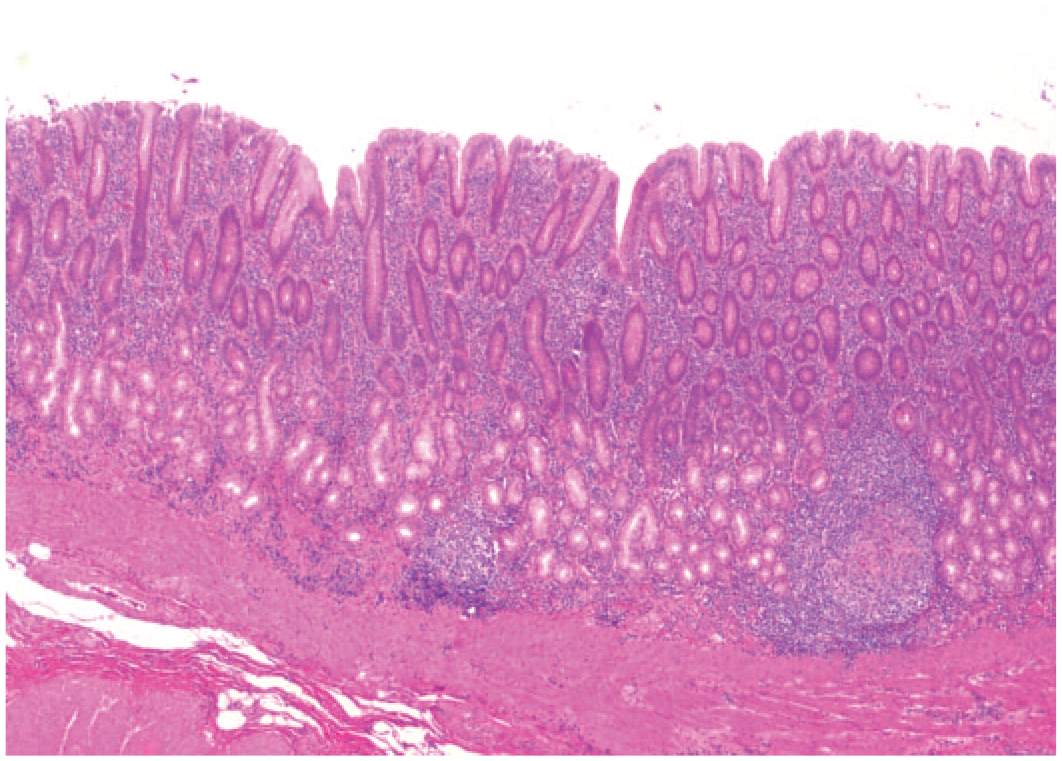
Similar to other monogastric species, the macaque gastrointestinal system is divided into 4 compartments: the stomach, small intestine, cecum, and colon. The stomach has 4 distinct regions, the cardia, fundus, body, and pylorus and is the primary site of protein digestion. 17 Microscopically, the cardia is characterized by the presence of numerous gastric pits lined by tall columnar epithelial cells, interspersed with numerous mucous secreting cells. Within the cardia, basilar glands typically lack parietal and chief cells. 18 The superficial fundic mucosa and deep gastric pits or foveolae are lined by tall columnar epithelial cells and mucous secreting cells. 18 The basilar fundic mucosa contains frequent chief cells and generally lacks parietal cells. 18 The gastric body is identified by the presence of parietal cells, basilar oriented chief cells within elongated gastric glands, and short gastric pits. 18 The gastric pits elongate within the pyloric antrum. Gastric glands are composed primarily of mucus cells, and there are rare chief cells and no parietal cells. 18 Several bacterial and fungal organisms may be seen in the lumen or glands of the stomach of normal macaques including Helicobacter spp., Sarcina spp., flagellates (trichomonads), and Ascomycetous yeasts or “megabacteria” (Figures 1-4). Sarcina spp., in particular, may increase in cases of dysbiosis and may invade and become pathogenic in immunosuppressed animals. These organisms are not typically diagnosed unless invasion and associated lesions are present. Lymphofollicular foci are often present throughout all regions of the stomach and tend to be the largest and most numerous at the junction of the cardia and esophagus. Their presence or size generally does not correlate with the presence of any of the fungal or bacteria agents listed; however, these follicles are generally less frequent in the body of the stomach of rhesus macaques versus cynomolgus macaques (authors’ experience) and less frequent in cynomolgus macaques of Mauritian origin versus Asian origin.18,19 The pyloric sphincter separates the stomach from the small intestine, the primary site of lipid digestion and nutrition absorption.17,20

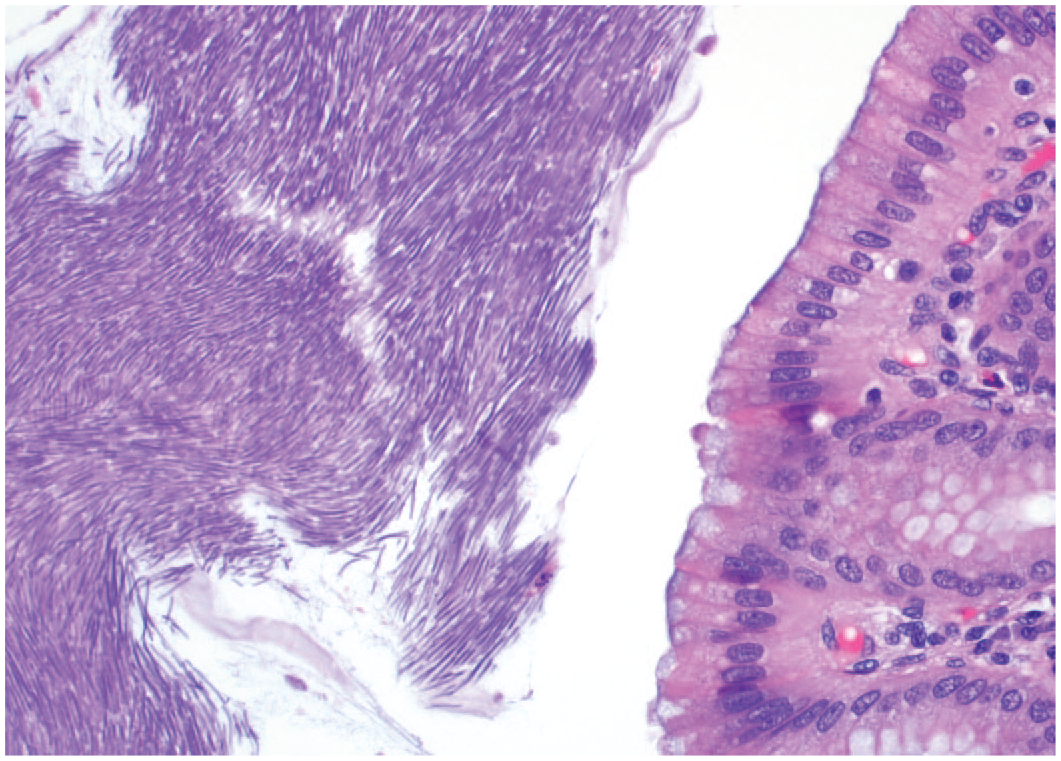
Multiple long spiral bacteria, consistent with H. heilmannii, are present within the gastric pits and minimally dilated gastric glands. There is no inflammatory response associated with these bacteria. Cynomolgus macaque, stomach. Hematoxylin and eosin (H&E).
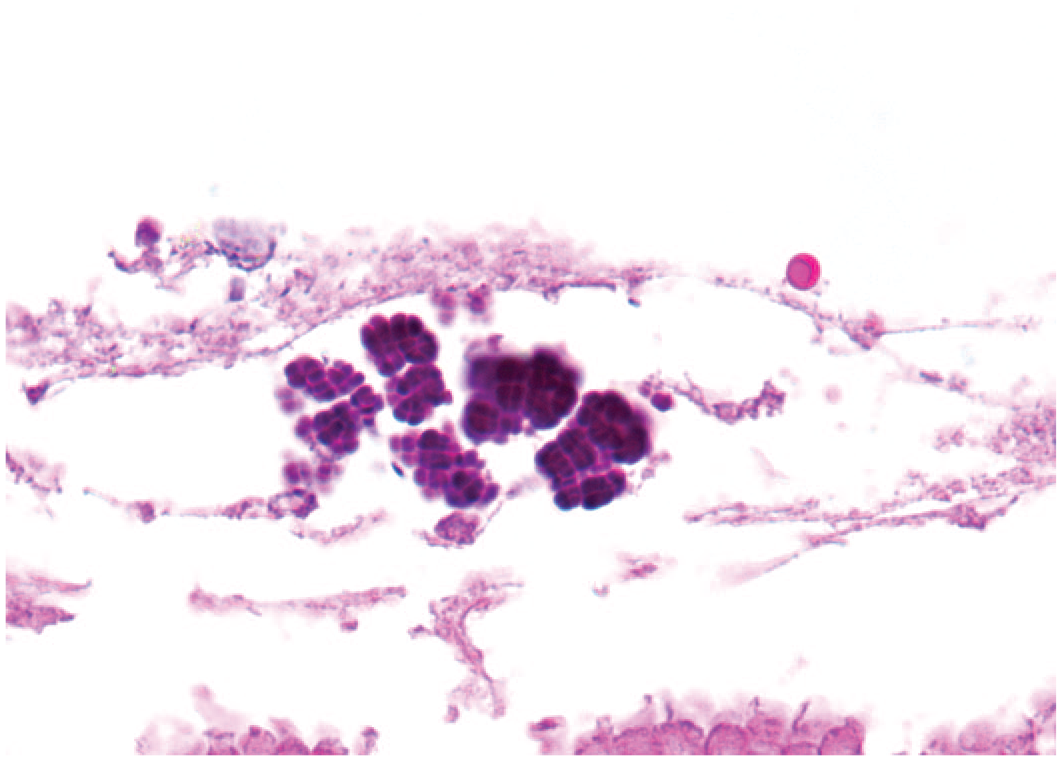
Sarcina occur as groups of cocci arranged in cubes. Rhesus macaque, stomach. Hematoxylin and eosin (H&E).
The gastric lumen contains a large mat of elongate rod–shaped organisms. Historically, these organisms have been referred to as megabacteria; however, they are likely Ascomycetous yeasts. Cynomolgus macaque, stomach. Hematoxylin and eosin (H&E).

The gastric pits contain numerous pear-shaped trichomonads. Similar organisms may also be seen in the colon of normal macaques. Rhesus macaque, stomach. Hematoxylin and eosin (H&E).
The shortest segment of the small intestine is the duodenum, which is distinguished by the distinct basilar band of Brunner’s glands, which are not present elsewhere in the small intestine. The jejunum and ileum are roughly the same length, similar to the ratio in humans, and distinguished microscopically by the presence of variably prominent Peyer’s patches within the ileum (Canfield, Tarara unpublished; Figure 5). Multinucleated syncytial cells are frequently identified in the gut-associated lymphoid tissues of cynomolgus macaques in particular, though they are also seen in rhesus macaques and represent a normal background finding (Figure 6). 12 Within the ileum, the villi are notably shorter than the previous segments of small intestine and may even appear blunted or fused immediately adjacent to the ileocecal junction. Throughout the small intestine, villi frequently contain variably prominent dilated lacteals, and clusters of pigmented macrophages are often present within the lamina propria of the villous tips (Figure 7).19,21

The gastrointestinal segments are highlighted by the following colors: the esophagus is dark yellow, stomach is pink, duodenum is lilac, jejunum is periwinkle, ileum is mint green, cecum is yellow-green, ascending colon is blue, transverse colon is purple, descending colon is bright green, and rectum is yellow. Rhesus macaque, gastrointestinal tract.

Scattered syncytial cells are present within the lymphoid follicles of the normal cecal gut-associated lymphoid tissue. Cynomolgus macaque, cecum. Hematoxylin and eosin (H&E).

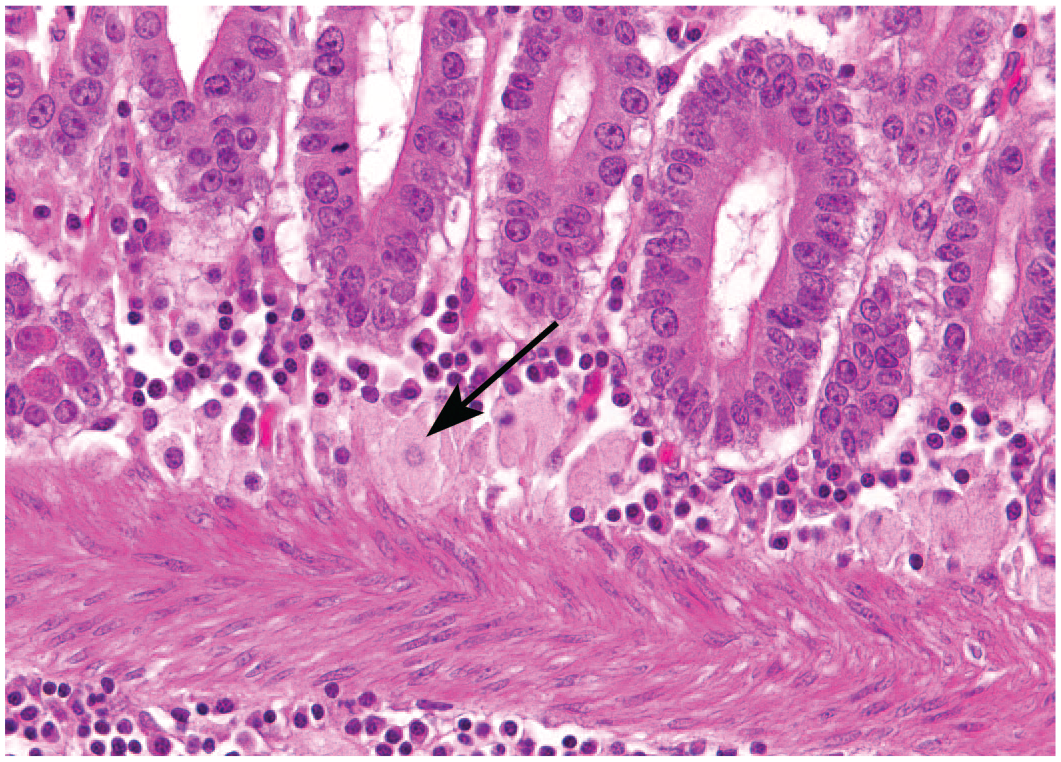
The lacteals of the small intestine are often notably dilated. Macrophages containing apoptotic debris (arrow) are also commonly seen at the villous tips. Rhesus macaque, jejunum. Hematoxylin and eosin (H&E).
The ileocecocolic junction is marked by the ileocecal valve which separates the small intestine from the cecum and colon. The large intestinal muscularis contains 3 distinct linear bands of smooth muscle (taenia coli) that create sacculations or haustra. 20 The cecum is fixed to the right craniolateral abdominal wall by a fibrous attachment extending from the antimesenteric surface of the base. The body of the cecum extends caudally to the lower right quadrant of the abdomen. 20 Unlike humans and apes, macaques do not have a vermiform appendix. The cecum is followed by the ascending colon, the shortest segment of the colon also located in the upper-right abdominal quadrant. The longest segment of the large intestine is the transverse colon, which passes across the upper abdomen to the left side where it courses caudally toward the pelvis and back cranially to the upper left quadrant. 20 This final turn (splenic flexure) marks the transition to the descending colon. The last segment of the intestinal tract is the rectum, which sits within the pelvic canal and is distinguished by the lack of taenia coli. 20 The rectum terminates at the anal sphincter. The large intestinal mucosa is composed of glands of uniform height. The superficial mucosa and roughly upper two-thirds of the glands contain variably high numbers of goblet cells. Foci of foamy macrophages, often referred to as muciphages, may be present in the lamina propria and submucosa of the colon where they may identify regions of prior, minor inflammation (Figure 8).22-24 The superficial mucosal epithelium is variably colonized by Helicobacter macacae (aka the blue brush border), which is often absent in cases of colitis (Figure 9). In addition, protozoa such as trichomonads (morphologically similar to those in the stomach; see Figure 4) and Balantidium coli are often present in low numbers within the colonic lumen or superficial glands of normal macaques (Figure 10). In cases of immune suppression, diarrhea, and/or dysbiosis, the number of protozoa may increase, they may penetrate deeper into the mucosa, and/or they may be identified in more proximal sections of the gastrointestinal tract.
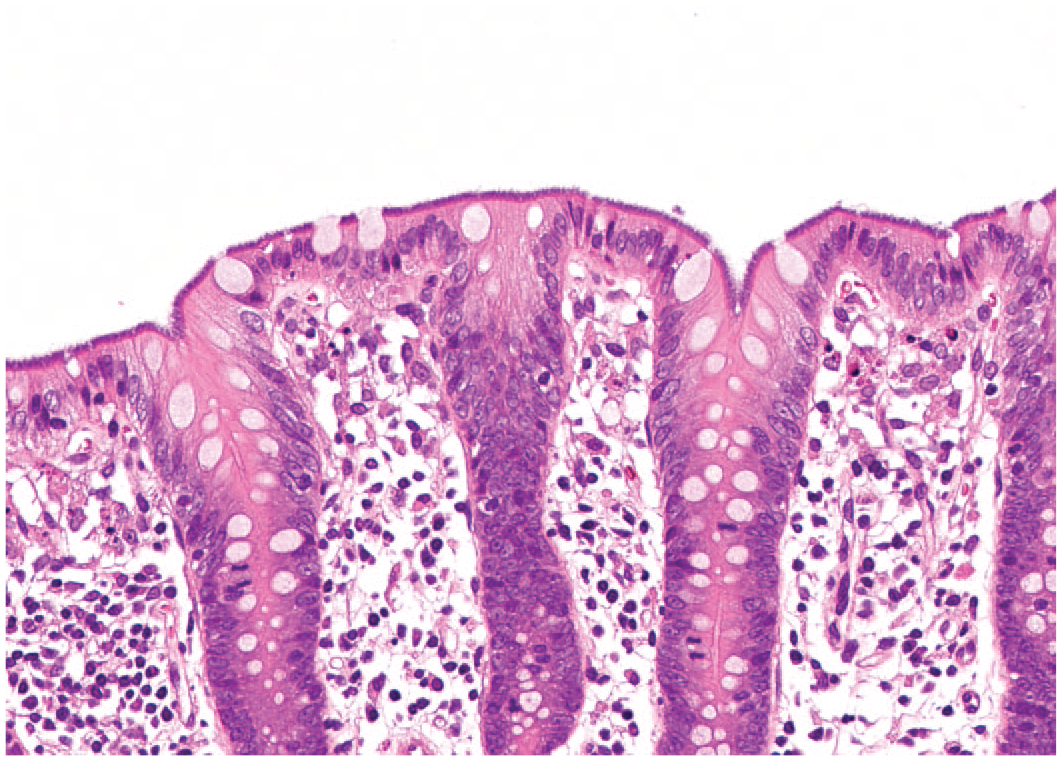
Macrophages with abundant pale eosinophilic to gray cytoplasm (muciphages; arrow) are present in clusters in the basal lamina propria. Rhesus macaque, colon. Hematoxylin and eosin (H&E).
A dense mat of bacteria colonize the apical enterocytes of the normal colon. This finding is sometimes referred to as the blue brush border. These bacteria have been genetically identified as Helicobacter macacae in rhesus macaques and are regularly seen in normal cynomolgus macaques. Cynomolgus macaque, colon. Hematoxylin and eosin (H&E).

Balantidium coli are large (20-150 µm) ciliated protozoa with a prominent bean-shaped macronucleus. Rhesus macaque, cecum. Hematoxylin and eosin (H&E).
The details of the draining lymph nodes of the macaque gastrointestinal system have received little attention in the literature; however, they are thought to be broadly similar to the human and considerably more complex than in rodents.25,26 The stomach drains to the left gastric lymph nodes and, in addition to lymphatic vessels from the duodenum, the pancreaticoduodenal and hepatic nodes. The small and large intestines are drained by groups of lymph nodes that are sometimes collectively referred to as the mesenteric nodes. These are numerous, amounting to hundreds of individual nodes in humans and include juxta-intestinal (immediately adjacent to the mesenteric side of the intestine), intermediate, and central or superior (at the root of the mesentery) mesenteric nodes that drain the small intestine. The distal intestinal tract is drained by the ileocolic (immediately adjacent to the mesenteric side of the intestine), paracolic, and the colic and inferior mesenteric lymph nodes.
Macaques are hindgut fermenters. The cecum and proximal portion of the colon are the site of abundant microbial activity and fermentation which aids in the digestion of complex carbohydrates, whereas the descending colon is the primary site of water absorption. 17 The normal colonic microbiota develops in the first year after birth and has been demonstrated to be more similar to humans from developing countries rather than western countries. 27 Short chain fatty acids (SCFAs) produced in the hindgut following fermentation of soluble and insoluble fibers may provide a significant amount of macaques dietary nutrition in a calorie-restricted diet. In addition, SCFAs have direct effects on colonic blood flow and water absorption. 28 Therefore, disturbance of the intestinal microbiota, such as may occur following growth faltering, infectious enterocolitides, or antibacterial therapy, may predispose animals to the development of chronic diarrhea syndromes.27,29
Bacterial and Fungal Causes of Gastrointestinal Tract Lesions in Macaques
Bacterial enterocolitis is by far the most common infectious cause of diarrhea and gastrointestinal lesions in macaques and the common agents are all zoonoses. While some agents are more common in outdoor-housed animals and may not be relevant to toxicology studies, others such as Campylobacter, Yersinia, and Shigella species, can be carried subclinically. These bacteria may then result in on study disease or lesions as a consequence of stress or test article–related immunomodulation.27,30-33 An understanding of the typical distribution of the gross lesions induced by bacterial agents associated with enterocolitis will aid in the assessment of such cases. Furthermore, in the event that unexpected diarrhea or gastrointestinal lesions are identified in a study, culture of feces, or gut content should be considered.
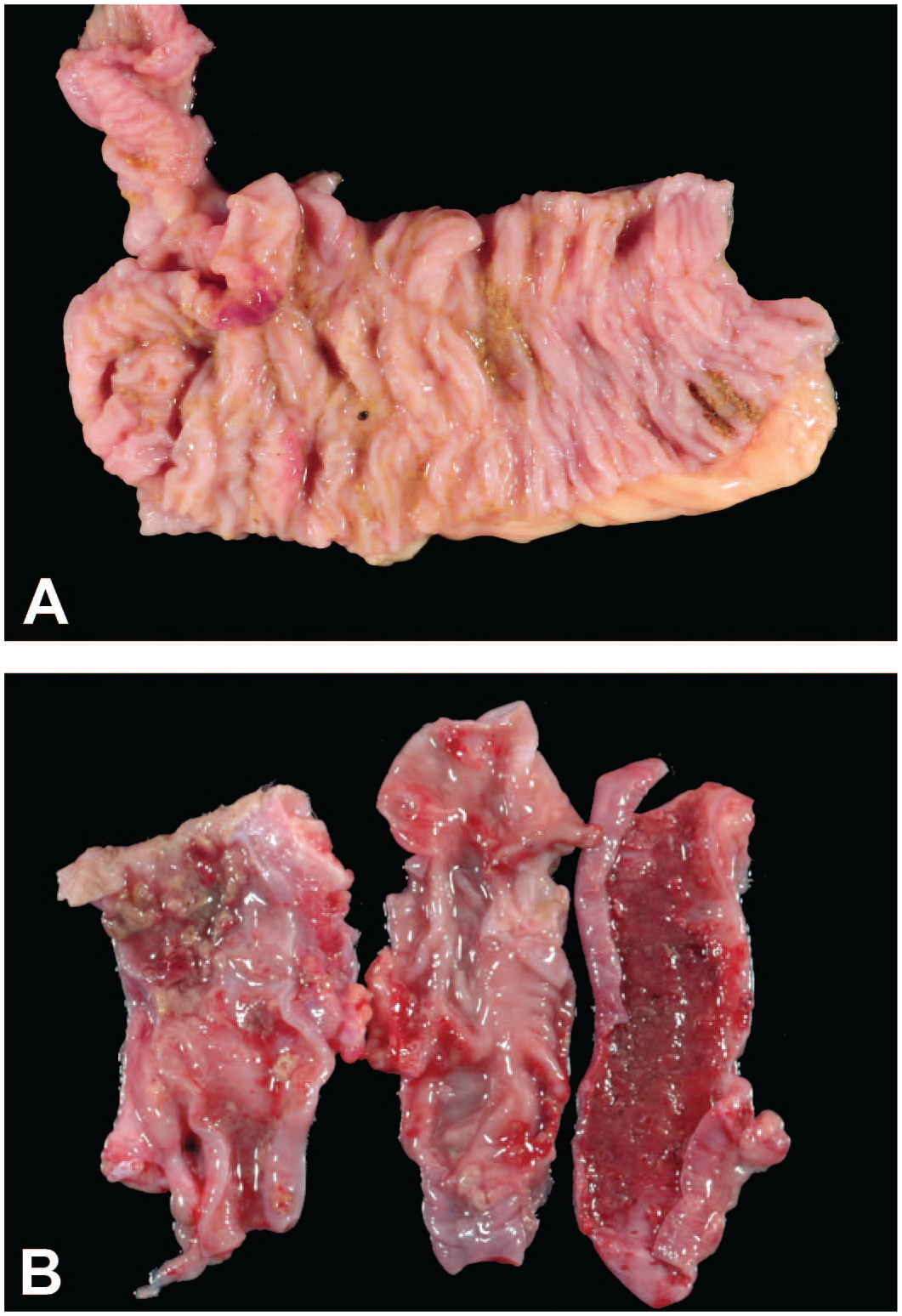
Shigella is a Gram-negative rod-shaped, nonmotile, nonencapsulated, nonspore-forming bacterium in the family Enterobacteriaceae. There are 4 serogroups including S. sonnei, S. boydii, S. dysenteriae, and S. flexneri. The latter is the most common serogroup identified in captive macaques. 34 Fecal-oral transmission is common and endemic infections are maintained through subclinical carriers shedding bacteria into the environment consequently exposing other animals. The frequency of Shigella in newly acquired cynomolgus macaques and rhesus macaques in quarantine is reported as 20.1% and 32%, respectively.35,36 Clinical signs include variably bloody diarrhea, lethargy, dehydration, shock, anemia, and leukocytosis with a left shift.34,37 Infection is often self-limiting but can be severe in young or debilitated animals. Grossly, cecal and colonic walls are thick and edematous, and there may be diphtheritic membranes overlying variably hemorrhagic necrotic and ulcerative mucosal surfaces (Figure 11).34,38 Mesenteric lymph nodes are often enlarged, congested, and edematous. 39 Lesions within the stomach are less common. Microscopically, there are varying degrees of mucosal epithelial necrosis, erosion, ulceration, and hemorrhage (Figure 12).34,39 The mucosal surface is often covered in a mat of fibrin, cellular debris, mucus, but Shigella bacteria are not commonly visible in the authors’ experience.34,35,39 The lamina propria is infiltrated by neutrophils and mononuclear cells that occasionally infiltrate the submucosa.34,39 Other findings include crypts filled with neutrophils (crypt abscesses), decreased goblet cells, as well as fibrin thrombi within the blood vessels in the submucosa and serosa.34,39 Shigella-specific antibodies have identified intralesional bacteria within superficial and crypt epithelial cells, crypt abscesses, lamina propria, and lymphoid tissue.39,40 Diagnosis requires culture, polymerase chain reaction (PCR), wet mounts, or immunohistochemistry (IHC). Shigellosis is zoonotic, with reports of transmission from NHPs to animal caretakers. 41

Necrohemorrhagic and ulcerative colitis with pseudomembrane formation. Rhesus macaque, colon, Shigella flexneri.

The mucosa is ulcerated and necrotic with infiltration of high numbers of neutrophils, hemorrhage, fibrin deposition, and formation of a superficial pseudo or diphtheritic membrane. Rhesus macaque, colon, Shigella flexneri. Hematoxylin and eosin (H&E).
Campylobacter is a Gram-negative slender, curved, or spiral rod–shaped, motile microaerophilic bacterium in the family Campylobacteraceae. There are numerous species of Campylobacter, with C. jejuni and C. coli being frequently isolated from both clinically healthy macaques and those experiencing diarrhea.31,42-45 At the CNPRC, C. coli is identified so frequently in clinically normal animals that its role in gastrointestinal disease is often questioned. Other species including C. fetus, C. laridis, C. sputorum, and C. hyointestinalis are identified less commonly.43,44 Fecal-oral transmission results in infection or the development of a subclinical carrier status. 46 The frequency of infection in laboratory macaques is high, ranging from 33% to 100% in infant, juvenile, and adult age groups; infection rates will vary between different colonies. 47 Neonatal and juvenile NHPs, especially those raised in nurseries are more susceptible to infection.7,47,48 Microbiome assessment using 16S rRNA sequencing suggests that Campylobacter species are extremely common even in clinically normal infants. 27 Clinical signs include diarrhea, decreased appetite, weight loss, and lethargy.44,46,49 Gross lesions in macaques are not well described and may vary in different colonies in the authors’ experience. Variably thickened and hyperemic cecal and colonic mucosa with or without hemorrhage (more common in C. jejuni cases), as well as mesenteric lymphadenomegaly are common (Figure 13). The ileum is often similarly affected in animals within the CNPRC colony. Microscopically, the cecal and colonic lamina propria are infiltrated by variable combinations and numbers of neutrophils, lymphocytes, and plasma cells (Figure 14). 49 There are decreased numbers of goblet cells, variable numbers of crypt abscesses, as well as necrosis, attenuation, and erosion of the luminal epithelial cells.49,50 Diagnosis is commonly made with microbial culture performed in microaerophilic conditions on selective media, fluorescent antibody testing, or avidin-biotin antibody staining. 51 However, genotyping may provide more accurate data on incidence and speciation in the authors’ experience.
(A) Proliferative typhlocolitis, with cecocolic valve hyperemia. Rhesus macaque, colon, Campylobacter coli. (B) Hemorrhagic colitis (and enteritis, not shown) may be noted in C. jejuni infections, but this presentation may be colony specific (for example, this is seen infrequently at the California National Primate Research Center but has not been noted at the Oregon National Primate Research Center). Rhesus macaque, colon, Campylobacter jejuni.

The mucosa is hyperplastic with infiltration of neutrophils, lymphocytes, and plasma cells. In addition, there is tufting of the superficial epithelial cells, reduced numbers of Goblet cells, and multifocal crypt abscesses. Rhesus macaque, colon, Campylobacter coli. Hematoxylin and eosin (H&E).
Yersinia is a Gram-negative coccobacillus, nonspore-forming, facultative anaerobe in the family Enterobacteriaceae. Y. enterocolitica and Y. pseudotuberculosis are associated with clinical disease in NHPs, where infections are acquired by the fecal-oral route. 51 Infections are often self-limiting and animals may become subclinical carriers; however, immunosuppressed or immunocompromised animals are more likely to experience severe clinical disease.33,46 Clinical signs of Yersinia spp. infection include depression, diarrhea with and without blood, emesis, abdominal pain, dehydration, abortion, and stillbirths.33,52,53 Additional findings include leukocytosis, neutrophilia, hyponatremia, hypochloremia, prerenal azotemia, and hyperfibrinogenemia. 53 Within the gastrointestinal tract, gross lesions are distinct from those of Shigella and Campylobacter infections and are characterized by discreet, multifocal ulcers that may affect the entire gastrointestinal tract (stomach to rectum) with or without diphtheritic membranes (Figure 15). Enlarged and edematous mesenteric lymph nodes have been described in cynomolgus, bonnet, and pig-tailed macaques.33,52,53 Microscopic lesions within the intestines consist of variably large foci of predominantly superficial mucosal necrosis, with high numbers of infiltrating neutrophils and macrophages, abundant cellular debris, and variably hyperplastic gut-associated lymphoid tissue. High numbers of large bacteria spilling out into the lumen from areas of mucosal necrosis are common, easily seen in H&E slides, and pathognomonic for Yersinia spp. infections (Figure 16).52,54 In cases of systemic yersiniosis, similar lesions have been observed in mesenteric lymph nodes, liver, and spleen. 54 Diagnosis is based on gross and pathognomonic microscopic lesions, culture, PCR, loop-mediated isothermal amplification (LAMP), and impression smears from necrotic foci from solid organs.54-56

Thickened and edematous colonic mucosa, with multifocal well-demarcated ulcers frequently covered by a tan diphtheritic membrane. Rhesus macaque, colon, Yersinia pseudotuberculosis.

There is necrosis of the superficial mucosa characterized by abundant cellular debris and large colonies of bacterial coccobacilli. The lamina propria is infiltrated by high numbers of neutrophils and fewer macrophages. Rhesus macaque, colon, Yersinia pseudotuberculosis. Hematoxylin and eosin (H&E).
Helicobacter is a Gram-negative curved to spiral-shaped, motile bacterium in the family Helicobacteraceae. There are at least 18 species of Helicobacter, including those commonly identified in the macaque H. pylori, H. heilmannii, and H. macacae.30,57-60 H. pylori and H. heilmannii have been associated with chronic gastritis in rhesus and cynomolgus macaques57,58,61,62; however, they are often present in control animals in toxicology studies with no clear correlation to the degree of inflammatory cell infiltrates in the underlying gastric mucosa.19,60,63 Helicobacter has been identified in saliva, feces, and on environmental surfaces; oral–oral transmission is thought to be the primary route of transmission. 64 Gastric colonization of H. pylori in socially housed rhesus macaques happens as early as 12 weeks old, with 90% of animals culturing positive by 1 year of age. 65 Clinical signs range from asymptomatic animals to rare instances of chronic intermittent emesis (authors' experience). In clinically affected animals, gross lesions include variably thickened and reddened gastric mucosa within the body and pylorus, with or without erosions (Figure 17). 66 Microscopic examination reveals predominantly lymphocytic and plasmacytic inflammatory infiltrates, and rarely eosinophils, within the superficial and deep lamina propria, intraglandular neutrophils, epithelial hyperplasia, erosions of the superficial gastric epithelium, and expansion of the gut-associated lymphoid follicles (Figure 18).57,66 H. pylori are identified in the gastric pits and epithelial surface of the gastric body and pylorus as curved to spiral-shaped rod approximately 3 to 5 µm by 0.5 µm. 67 H. heilmannii is longer than H. pylori and is identified in the gastric glands (often dilated), pits, and less frequently the epithelial surface of the gastric fundus as tightly coiled spiral-shaped bacteria approximately 7 to 10 µm by 0.5 µm (see Figure 1). 68 H. heilmannii is more rarely associated with clinical signs or evidence of gastritis than H. pylori. Diagnosis is based on histologic identification on H&E or Warthin–Starry stain, detection of urease activity within gastric tissue, culture (H. pylori), PCR, and serology.57,67,69
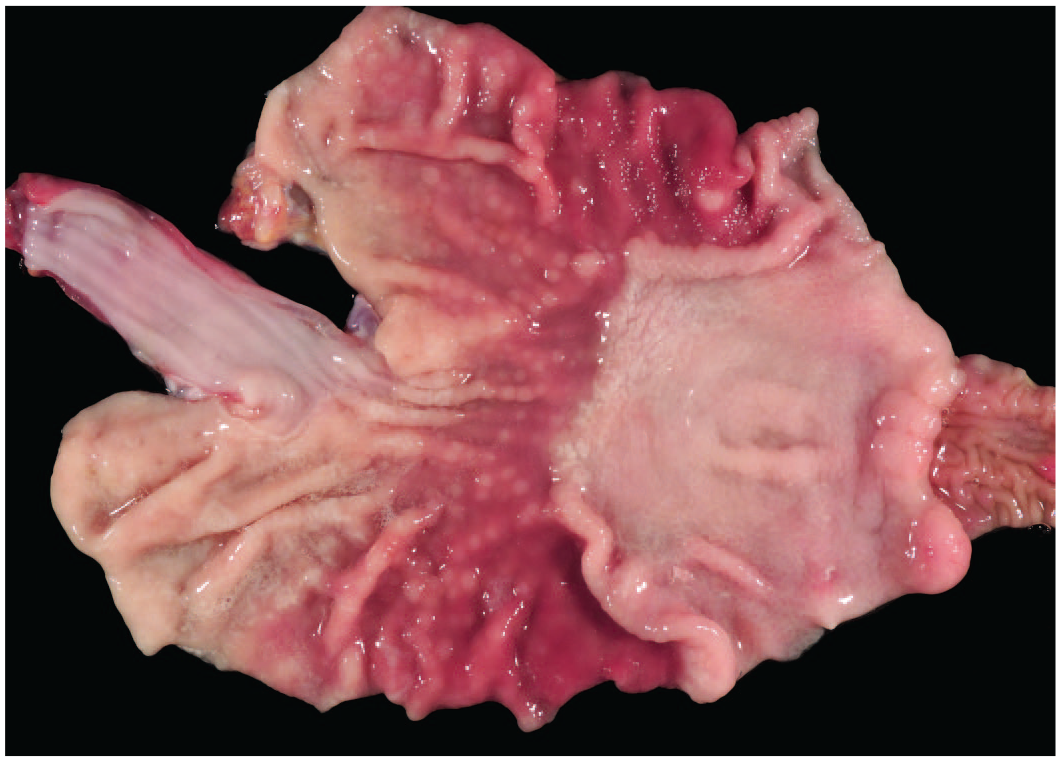
The gastric mucosa is variably thickened with multifocal raised nodules throughout the erythematous body and to a lesser extent the pylorus. Rhesus macaque, stomach, Helicobacter pylori.
The pyloric mucosa is hyperplastic with prominent gut-associated lymphoid hyperplasia. The lamina propria is infiltrated by lymphocytes, plasma cells, and very few eosinophils. Rhesus macaque, stomach, Helicobacter pylori. Hematoxylin and eosin (H&E).
H. macacae is considered a normal inhabitant of the macaque large intestine, where they line the superficial epithelium and have been referred to as the “blue brush border” (see Figure 9). 30 Reduction of loss of these apical bacteria is considered a feature of dysbiosis in macaques with idiopathic colitis. 30
Attaching and Effacing Escherichia coli: Enteropathogenic E. coli is a ubiquitous Gram-negative, aerobic to facultative anaerobic, nonspore forming rod in the family Enterobacteriaceae. Multiple serotypes of E. coli have been isolated from asymptomatic and symptomatic rhesus macaques.70-73 Enteropathogenic E. coli (EPEC) is considered an opportunistic pathogen in stressed neonatal or juvenile macaques, as well as simian immunodeficiency virus (SIV)-infected rhesus macaques. 71 Clinical signs include profuse diarrhea, weight loss, neutrophilic leukocytosis, metabolic acidosis, and hypokalemia.46,71 Grossly the small intestinal, cecal, and colonic mucosa range from unremarkable to variably erythematous with mild mucosal thickening and rarely hemorrhage (Figure 19) (authors’ experience). Microscopic lesions include villous blunting and effacement, where the apical aspect of enteric enterocytes and colonic epithelial cells are lined by bacterial rods (Figure 20).46,71 The colonic epithelial cells have a characteristic flattened, cobblestone, or moth-eaten appearance. 46 Bacteria are visible with H&E, Gram, and toluidine blue stains. 46 Diagnosis is based on characteristic microscopic lesions, electron microscopy, PCR, bacterial culture, and isolate typing.46,71,74
The small intestinal mucosa is mildly thickened and diffusely erythematous. Rhesus macaque, jejunum, attaching, and effacing Escherichia coli.

Bacterial rods line the apical aspect of villous enterocytes. Rhesus macaque, jejunum, attaching, and effacing Escherichia coli. Hematoxylin and eosin (H&E).
Salmonella is a Gram-negative, motile rod and facultative anaerobe that is a member of the family Enterobacteriaceae. Of the 2 species of Salmonella, only S. enterica is associated with disease in animals, but there are thousands of different serotypes. S. typhimurium, S. stanley, S. dublin, and S. enteriditis are most common serotypes associated with disease in macaques.75,76 Transmission occurs via the fecal-oral route. Naturally occurring salmonellosis is extremely rare in well-maintained colonies, but outbreaks have been reported in imported macaques following shipping stress. 76 The prevalence of Salmonella infection may be higher in wild populations of macaques in regions where they cohabitate with humans.77,78 Generally, self-limiting watery or hemorrhagic diarrhea with mucus are the most common clinical signs in affected animals; however, severe signs of disseminated infections resulting in death may be seen in immunosuppressed animals.79,80 Salmonellosis may affect the small and large intestine and can also be found in the stomach.76,80,81 As a result, the gross lesions may be indistinguishable from those of Campylobacter jejuni or Shigella cases. The mucosa of the small and large intestine is thickened with variable hemorrhage and/or necrosis. Microscopically, degeneration of the small and large intestinal mucosa with villous blunting and fusion is accompanied by a mixed cell infiltrate that may be predominantly mononuclear in regions, and crypt dilation. Diagnosis is typically achieved by culture in selective media.
Mycobacterium avium: Intracellulare complex is an acid-fast bacillus in the family Mycobacteriaceae. Intestinal infection occurs through ingestion of contaminated water, food, or soil. Disease is usually self-limiting and is extremely rare in well-managed colonies, except in SIV-infected macaques, where it is considered an opportunistic infection associated with a marked decline in CD4+ T cells.82-85 Clinical signs include lethargy, diarrhea, and weight loss. 86 Grossly, the distal small intestine, cecum, and colonic walls are variably thick and edematous with prominent yellow-white mucosal folds (Figure 21).82,83,86,87 In addition, the mesenteric lymph nodes are enlarged and edematous with prominent lymphatic vessels.82,83,86,88,89 Microscopically, the lamina propria and submucosa are expanded by high numbers of large foamy macrophages that contain abundant intracytoplasmic bacilli, identified by an acid-fast stain (Figure 22). 82 Within the mesenteric lymph nodes, foamy macrophages expand the subcapsular and cortical sinusoids and infiltrate and efface the adjacent architecture. 82 Diagnosis is based on characteristic gross and microscopic lesions, PCR, and culture.

The small intestinal mucosa is thick and edematous with elevated yellow-white folds. Rhesus macaque, jejunum, Mycobacterium avium.
Villi are expanded and distorted by high numbers of foamy macrophages. Macrophages contain abundant intracytoplasmic acid-fast bacilli (not shown). Rhesus macaque, jejunum, Mycobacterium avium enteritis. Hematoxylin and eosin (H&E).
Candida albicans is a ubiquitous commensal fungal organism that causes no disease in immunocompetent animals. 90 In neonatal or immunocompromised macaques, Candida can cause white plaques grossly within the oral mucosa, esophagus, and stomach with clinical signs of diarrhea, dysphagia, and difficulty breathing.91-93 Histologically, there is most often hyperplasia and hyperkeratosis (upper alimentary tract) of the superficial mucosa with large numbers of hyphae and blastospores90,91 that can be highlighted by periodic acid Schiff or Gomori methenamine silver stains and little inflammation (authors’ experience). With severe disease, organisms can invade deeper into the mucosa, causing ulceration, and necrosis. 91 Diagnosis is based on the classic gross and microscopic lesions and culture where necessary.
Parasitic Causes of Gastrointestinal Tract Lesions in Macaques
Protozoan parasites of the gastrointestinal tract with direct transmission lifecycles, including Giardia and Cryptosporidium, are common in macaque colonies despite screening and therapy and are zoonoses. They most commonly cause clinical disease in infant or juvenile animals, but may also cause disease in immunosuppressed adults. Clinically significant infections with helminths and cestodes are rarely seen in well-managed colonies. However, individual luminal parasites or remnant cysts/parasitic granulomas may be noted despite anthelmintic treatment, particularly in imported animals that have had shorter acclimatization periods.
Giardia duodenalis is a flagellated, pear-shaped, 12-15 × 5-9 μm protozoa that commonly causes diarrheal disease in juvenile macaques. In a review of Chinese NHP colonies, the prevalence of Giardia infections in macaques ranged from 0.5% to 8.5%. 94 Infection occurs by the fecal-oral route and the cyst form is extremely stable in the environment. There are no consistent gross lesions. The trophozoites are typically observed in the lumen or attached to the surface epithelial cells of the proximal small intestine, predominantly in the mid-jejunum, and do not invade.95,96 The small intestine may be otherwise microscopically normal or there may be variable villous blunting and mild infiltrates of inflammatory cells. 97 Diagnosis can be confirmed with fecal antigen capture tests that are often combined with Cryptosporidium and/or Entamoeba assays. 90
Cryptosporidium parvum is a 3 to 4 μm spherical, protozoan that is found primarily in the small and large intestine in immunocompetent animals. Infection is common in macaque colonies, with 95% seropositivity by 2 to 3 years of age, and occurs via fecal-oral transmission of oocysts. 90 Infection is often clinically silent and gross lesions are minimal. However, juveniles, immunocompromised animals, or those receiving immunomodulatory test articles may present with chronic diarrhea, anorexia, and weight loss.90,98 In those animals, the organism may be observed within the small intestine, colon, and in other sites including the stomach, biliary tree, conjunctiva, trachea, and lungs.90,99 Microscopically, the spherical, basophilic protozoa are easily identified in less inflamed H&E sections at the apical surface of the epithelial cells, where they occupy an intracellular but extracytoplasmic niche (Figure 23). Trophozoites in addition to microgametes and macrogametes (evidence of the sexual reproduction phase) may be identified. Epithelial loss and shedding leads to villous blunting and fusion, which may be accompanied by eosinophilic inflammation in the acute phase. Marked epithelial hyperplasia with prominent mitotic figures are present in the repair phase. Microscopic identification of the organism is pathognomonic of the disease, but diagnosis can be supplemented by an immunohistochemistry or fecal antigen test.90,100

There are numerous 2-5 micron diameter spherical trophozoites lining the apical enterocytes. Rhesus macaque, ileum, Cryptosporidia. Hematoxylin and eosin (H&E).
Trichuris trichiuria has an incidence of ~24% in wild rhesus macaques in Nepal 101 and is difficult to eliminate completely in colony-reared macaques. 90 Small numbers of parasites are often seen in the large intestines of control animals. Infection does not cause significant clinical disease with a light burden, but animals can have diarrhea or weight loss with severe burden. At necropsy, the parasites can be observed attached to the mucosa, primarily in the cecum and proximal colon, although a large burden can extend the length of the colon (Figure 24). Histologically, the parasites can be observed within the mucosa with minimal or no mucosal changes or inflammatory reactions (authors’ experience). Parasitic granulomas including large numbers of eosinophils can occasionally be observed. 90

Within the ascending colon, there are numerous slender nematodes whose narrower anterior ends are embedded in the superficial mucosa. Rhesus macaque, colon, Trichuris trichiuria.
Oesophagostomum spp are one of the most frequent helminths in imported NHPs and include O. apiostomum, O. bifurcum, O. aculeatum, and O. stephanostomum. In previous studies, the incidence can be up to 70% in rhesus and 62% in cynomolgus macaques per direct detection methods. 102 No clinical disease is reported, 103 and lesions are caused by the fourth to fifth stage larvae encysting within the wall or serosa of the cecum or colon, causing small dark brown to black nodules (Figure 25). 102 These cysts are more common in imported cynomolgus macaques used in toxicology studies, particularly when quarantine periods are shorter. Histologically, the nodules contain sections of the parasites associated with granulomatous or pyogranulomatous inflammation and referred to as “parasitic granulomas” in the literature.12,102

Visible from the serosal surface, are multifocal to coalescing raised reddish-brown submucosal abscesses or granulomas. Pigtailed macaque, colon, Oesophagostomum spp.
Strongyloides spp (most often Strongyloides fuelleborni, but S. stercoralis also reported) is a soil-transmitted nematode parasite with infection rates up to 27% in captive breeding colonies of macaques. 90 This parasite is rarely seen in indoor housed colonies or in toxicology studies. Clinical signs can include diarrhea due to infection of the small and large intestines, or cough, dyspnea and dermatitis due to migration.90,102 Occasionally heavy infestations may lead to death. Parasites can be histologically observed in the mucosa of the small intestine, rarely in the large intestine, and are associated with inflammation in the lamina propria.
Cestodes of numerous genera, and both adults and larval forms (cysticercosis and sparganosis), have been observed within macaques. Clinical disease or enteric lesions are rarely associated with infection with either adults or larvae and thus they are considered an incidental finding. Diagnosis is based on eggs, proglottids, or adults passing in the feces or observation of adult worms or larval forms at necropsy. Cestode larvae within a cyst can be found anywhere in the body and have been reported in the body cavity, subcutaneous tissues, muscle tissues, and retroperitoneal space. Histologically, there is often little to no inflammation unless the larvae die. 95
Viral Causes of Gastrointestinal Tract Lesions in Macaques
Clinical disease as a result of viruses targeting the gastrointestinal tract is rare in immunocompetent animals. However, subclinical infections of both cytomegalovirus (CMV) and adenovirus are common and associated incidental lesions may be seen at necropsy. Furthermore, test article-mediated immunosuppression may lead to recrudescence of viruses and clinical disease. While rotaviruses and caliciviruses have been implicated in infant diarrhea in individual animals/colonies, they do not appear to be a common cause of gastrointestinal disease in macaques.104-106
Cytomegalovirus is an enveloped virus, in the family Herpesviridae and the subfamily Betaherpesvirinae. Cytomegalovirus is a slowly cytolytic virus that results in nuclear and cytoplasm enlargement of infected cells. 107 Virus persists as a latent infection in glandular tissue, kidneys, and lymphoreticular cells. 107 Cytomegalovirus is endemic in both wild and captive macaques, where 92% of rhesus macaques become infected by 1 year of age and seroprevalence in adult rhesus and cynomolgus macaques is 90% to 100%.108-110 Infection is generally asymptomatic in immunocompetent animals but can result in illness and death in macaques concurrently infected with SIV.107-109 Transmission is horizontal with intermittent virus shedding in blood, saliva, milk, urine, and semen. 111 In immunosuppressed animals experiencing viral reactivation, clinical signs and gross lesions are related to the organs involved, which include lung, central nervous system, liver, lymphoid tissues, and blood vessels in addition to the gastrointestinal tract. 107 Clinical signs of diarrhea may be present with multifocal red raised proliferative masses throughout the stomach and small and large intestines (Figure 26). 112 Microscopically, the lamina propria is infiltrated by high numbers of neutrophils, with lower numbers of macrophages, lymphocytes, and plasma cells that occasionally infiltrate the submucosa and muscularis externa. 112 Inflammatory foci are often associated with varying degrees of gland/crypt hyperplasia, hemorrhage, edema, vasculitis, and are frequently punctuated by large cytomegalic cells that contain a large basophilic to amphophilic intranuclear inclusion body surrounded by a clear halo (Cowdry Type A) (Figure 27).107,112 Smaller eosinophilic intracytoplasmic inclusions are less frequent. Intranuclear inclusions are less commonly identified within the stromal cells of the lamina propria, endothelial cells, smooth muscle cells, and macrophages. 112 In the authors’ experience, rare foci of neutrophilic inflammation surrounding cytomegalic cells with or without local vasculitis may also be seen in clinically normal animals. Diagnosis is based on characteristic cytomegalic cells with inclusion bodies, as well as immunohistochemistry. 112

The small intestinal mucosa is expanded by multifocal red, raised proliferative masses. Rhesus macaque, jejunum, cytomegalovirus.

The lamina propria is predominantly infiltrated by high numbers of neutrophils, with low numbers of cytomegalic cells that contain large basophilic intranuclear inclusion body surrounded by a clear halo (Cowdry Type A) characteristic of cytomegalovirus. Rhesus macaque, jejunum, cytomegalovirus. Hematoxylin and eosin (H&E).
Adenovirus is a nonenveloped virus in the Adenoviridae family and the genus Mastadenovirus, where there are more than 50 serotypes that have been isolated from NHPs, including rhesus and cynomolgus macaques.107,113-115 Immunocompetent macaques experience subclinical infections, in contrast to immunosuppressed animals who can develop severe and potentially fatal disease. 107 The gastrointestinal tract is the second-most common organ system affected, where infection is maintained in the intestinal epithelium. 107 Fecal shedding occurs in 13% to 100% of indoor housed rhesus and cynomolgus macaques. 115 Gastrointestinal transmission occurs through the fecal-oral route.107,115 Neonatal macaques are more susceptible to infection when compared to adults. 107 Clinical signs of gastrointestinal adenoviral infection range from asymptomatic to diarrhea and dehydration.107,113 Gross lesions in the gastrointestinal tract are either absent or include congestion and edema of the gastric and intestinal mucosa. 107 Microscopically, the stomach and intestines are often unremarkable, except for occasional small intestinal villous blunting and the presence of large basophilic to amphophilic intranuclear inclusion bodies within intact gastric epithelial cells and enterocytes of the small and occasionally large intestine (authors’ experience) (Figure 28). More severe lesions within the small intestine are described as foci of erosion and ulceration, with necrotic epithelial cells containing characteristic adenoviral intranuclear inclusion bodies. 113 Diagnosis is based on histopathologic lesions, serology, IHC, in situ hybridization (ISH), and electron microscopy (EM).

Multiple enterocytes contain large basophilic intranuclear inclusion bodies, characteristic of adenovirus. Cynomolgus macaque, colon. Hematoxylin and eosin (H&E).
Measles virus is an enveloped, negative-sense single-stranded RNA virus, genus Morbillivirus and family Paramyxoviridae. While this virus is highly infectious and can result in severe disease, it is rarely of concern in well-managed colonies in which macaques are vaccinated. Infection has been described in a number of NHP species, including cynomolgus and rhesus macaques in newly quarantined animals experiencing stress from importation.93,116-118 High-mortality epizootics have been described in a group of SIV-infected immunosuppressed macaques. 119 Within a naïve population of animals, transmission occurs rapidly via aerosolization. Gross and microscopic lesions may be identified in the skin, lung, lymphoid tissue, and rarely the central nervous system and reproductive tissues in addition to the gastrointestinal tract. Gastrointestinal clinical signs in stressed or immunosuppressed macaques include anorexia and diarrhea.93,116,120 Gross gastrointestinal lesions are considered infrequent but include gastric mucosal reddening and small intestinal congestion and petechiae.93,120 Microscopically, intact and desquamated gastric epithelial cells contained round intranuclear inclusion bodies and were immunoreactive for measles virus immunohistochemistry. 93 A transient immunocompromised state characterized by lymphoid depletion of the spleen and lymph nodes may develop, resulting in susceptibility to enteric and opportunistic pathogens, including Shigella flexneri and CMV.93,121,122 Other reports of measles outbreaks in rhesus macaques did not describe gross gastrointestinal lesions, but did note the presence of indistinct syncytial giant cells within the small intestinal epithelium and the colonic crypt epithelium, where there were foci of mild epithelial necrosis. 123 Syncytial cells may also be present in the gut-associated lymphoid tissue (GALT). Diagnosis is based on characteristic clinical findings, histopathologic, and ultrastructural findings (including in extra-intestinal tissues), seroconversion, virus isolation, and identification. Measles is an anthropozoonotic and zoonotic virus that is most frequently introduced to macaque colonies from unvaccinated humans.119,122
Noninfectious Causes of Gastrointestinal Tract Lesions in Macaques
Idiopathic chronic diarrhea (ICD
Animals with ICD present with recurring or intractable non-bloody, watery green diarrhea, dehydration, and weight loss. Macroscopic findings in animals affected with ICD are typically restricted to the colon and in early or less-severe cases only the proximal colon may be affected. The mucosa is diffusely thickened, but nonulcerated and colon contents consist of tan-green liquid. Colonic lymph nodes are enlarged and in some cases dilated with fluid. Microscopic findings in the colon consist of lymphoplasmacytic infiltrates in the lamina propria and mucosa, mucosal hypertrophy with reduced goblet cell number and variable attenuation or tufting of the superficial mucosa (Figure 29). Crypt abscesses may be present in some animals.10,30,127 The usual blue brush border is reduced or absent, and there may be evidence of overgrowth of luminal trichomonads and Balantidium. Increased density of enterochromaffin cells has been reported using anti-serotonin IHC. Microscopic changes in the small intestine are infrequently reported but may include lymphoplasmacytic infiltrates in the lamina propria and increased intraepithelial lymphocytes.30,126,131 Idiopathic chronic diarrhea is a clinical syndrome that is diagnosed following the exclusion of the common bacterial and parasitic causes of diarrhea in juvenile macaques.

The mucosa is markedly hyperplastic with decreased numbers of goblet cells and attenuated (but nonulcerated) superficial enterocytes. The lamina propria is expanded by a lymphocytic and plasmacytic infiltrate, and there is a focal-dilated gland containing cellular debris. Rhesus macaque, colon, idiopathic chronic diarrhea. Hematoxylin and eosin (H&E).
Chronic cicatrizing ulcerative colitis represents a form of chronic colitis in macaques with a distinct gross and microscopic appearance that may affect juvenile or adult animals.134-136 The cause is unknown, but is thought to represent a post infectious syndrome. Clinical signs are non-specific including weight loss and chronic diarrhea. Grossly, the lesions appear as discrete, constricting annular ulcers that are often segmentally distributed in the cecum and proximal half of the colon (Figure 30). Partial obstruction of the lumen and secondary dilation of the proximal intestines is common and regional lymph nodes are enlarged. The gross appearance is similar to and must be differentiated from intestinal carcinoma. Microscopically, chronic ulcers are comprised of beds of granulation tissue infiltrated by neutrophils. The adjacent mucosa is hyperplastic and occasionally dysplastic with irregular branching glands. The underlying submucosa is markedly fibrotic with numerous lymphoid follicles that may extend transmurally. It is frequently associated with secondary systemic amyloidosis.

Multiple linear circumferential ulcers with associated mild fibrous constrictions are present in the cecum and ascending colon. Rhesus macaque, ileocecolic junction, cicatrizing ulcerative colitis.
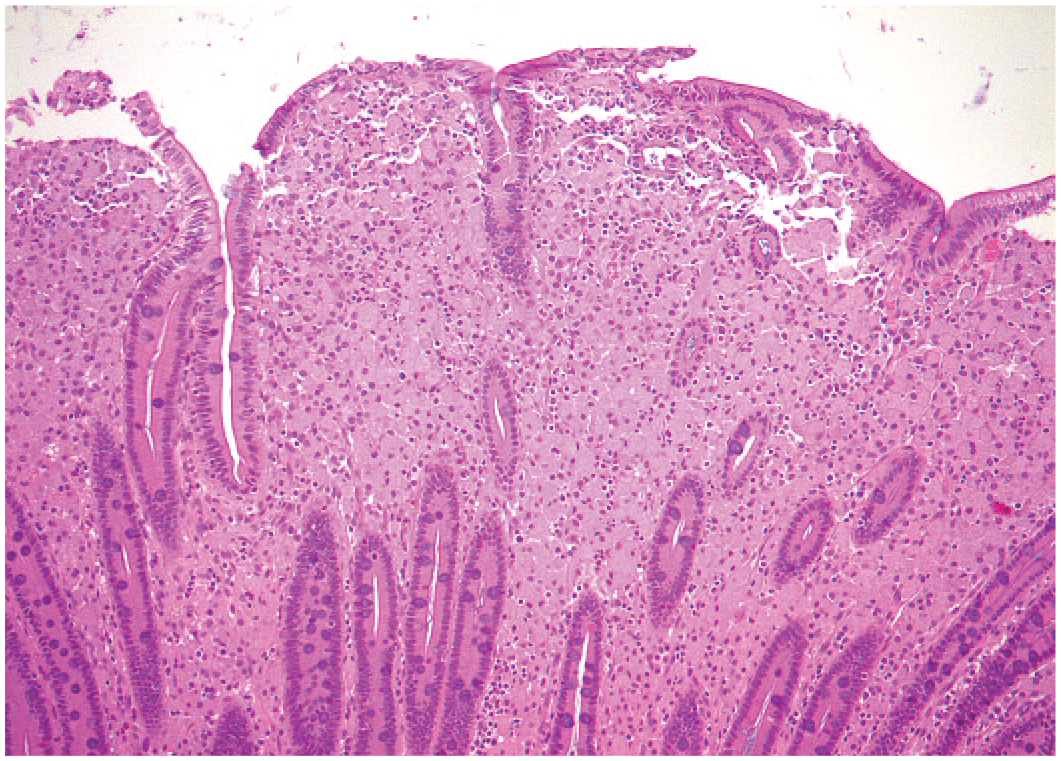
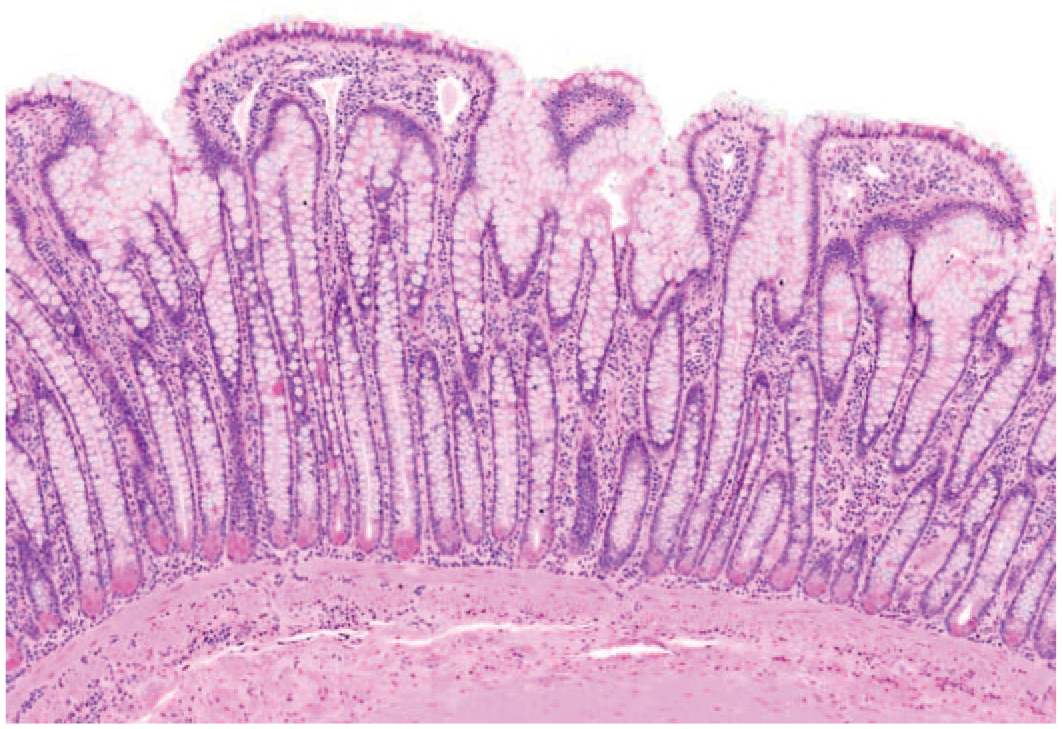
Malabsorptive enteropathy with villous atrophy has been reported in adult macaques in some primate colonies.137-140 Gluten sensitivity was demonstrated in one rhesus macaque with chronic diarrhea by response to gluten-restricted diet, gluten challenge, and the presence of circulating anti-gliadin antibodies. The principal histologic findings were nonspecific and included villous blunting, crypt hyperplasia, and increased intraepithelial lymphocytes. 137 A different form has been seen in both rhesus and cynomolgus macaques that may present with grossly apparent abundant luminal mucin (Figure 31). Microscopically, it is characterized by severe villous blunting, marked goblet cell hyperplasia, and mild eosinophilic, plasmacytic inflammation (Figure 32). When severe, the mucosa undergoes colonic metaplasia, and there is marked hypertrophy of the muscular tunics.

Abundant soft tan material fills the intestinal lumen (mucus). The muscular tunics are markedly hypertrophic. Rhesus macaque, small intestine, malabsorptive enteropathy with goblet cell hyperplasia.
There is marked goblet cell hyperplasia and loss of villous structures (large intestinal metaplasia). Rhesus macaque, jejunum, malabsorptive enteropathy with goblet cell hyperplasia. Hematoxylin and eosin (H&E).
Secondary systemic or reactive amyloidosis is an amyloidotic disease in which insoluble AA amyloid fibrils are deposited in multiple tissues. Amyloid deposition is associated with high circulating levels of serum amyloid A, an acute phase reactant produced by the liver. In the context of chronic inflammation, AA amyloid deposits are relatively common in some macaque colonies affecting up to 15% or more of animals submitted for necropsy in a given year.134,141,142 Although larger studies have focused on rhesus and pig-tailed macaques,134,142,143 the disease occurs in cynomolgus and other macaques. 144 Animals as young as 1 year of age may be affected, and there is no sex predisposition.134,145 The most commonly reported predisposing causes are chronic colitis, inflammatory and degenerative osteoarthritides, intestinal adenocarcinoma, endometriosis, simian retrovirus (SRV) infection, and chronic gastrointestinal (GI) ulceration.134,141,146 The tissues most commonly affected are the stomach, small and large intestines, liver, spleen, renal medullary interstitium, adrenal glands, and lymph nodes. Enteric amyloidosis may be incidental or can result in a syndrome of protein losing enteropathy characterized by low total protein and low albumin. The resulting diarrhea is often intractable and associated with profound weight loss.
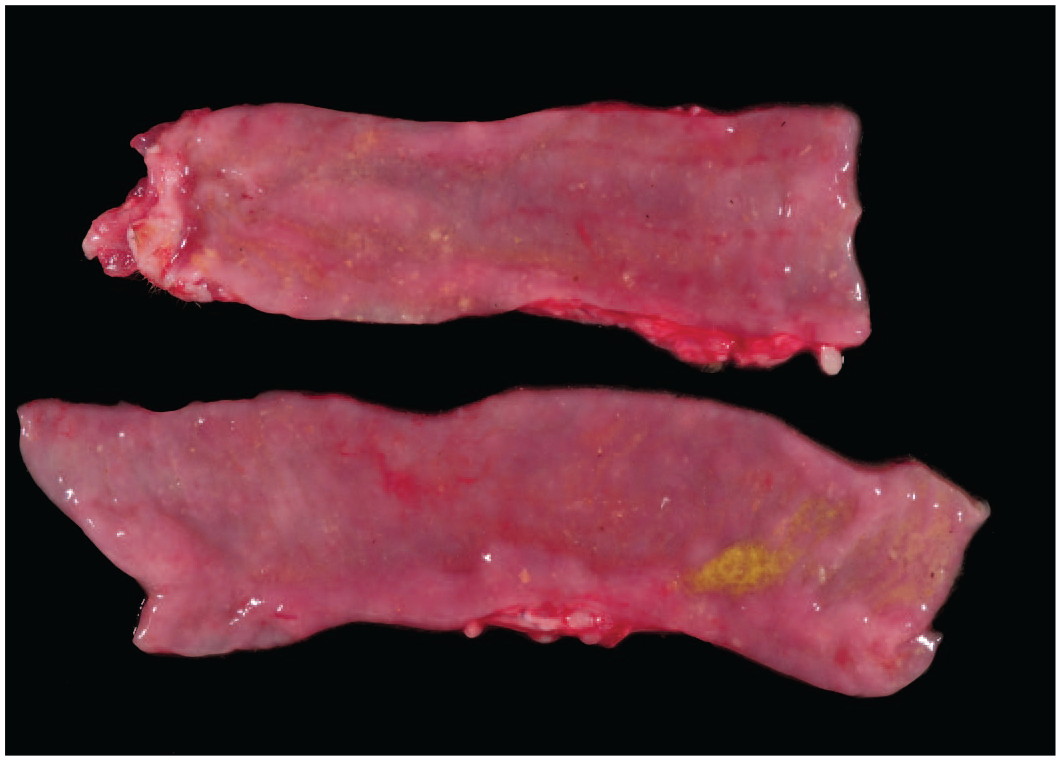
Grossly, amyloid deposits in the small intestine may cause villi to become visibly enlarged and irregular or the mucosa to appear diffusely smooth (Figure 33). When severe, superficial mucosal erosions or ulcerations can occur, particularly in the stomach, distal ileum, and rarely in the colon. Microscopically, amyloid appears as homogenous to fibrillar, eosinophilic extracellular material with HE staining (Figure 34). Amyloid deposits in the gastrointestinal tract occur in the lamina propria and in the walls of small arterioles of the mucosa and submucosa. In the small intestine, amyloidosis is frequently associated with secondary changes to villous architecture, resulting in stunted, fused, and irregularly shaped villi and crypt hyperplasia. AA amyloid stains positively with Congo red, exhibits apple green birefringence under polarized light and is susceptible to the potassium permanganate method (distinguishing it from other forms of amyloid).

The small intestinal mucosa is diffusely thickened by crowded mucosal folds. Rhesus macaque, jejunum, amyloidosis.

Normal villous appearance is distorted and the lamina propria is expanded by variable amounts of homogenous eosinophilic extracellular amyloid. Rhesus macaque, jejunum, amyloidosis.
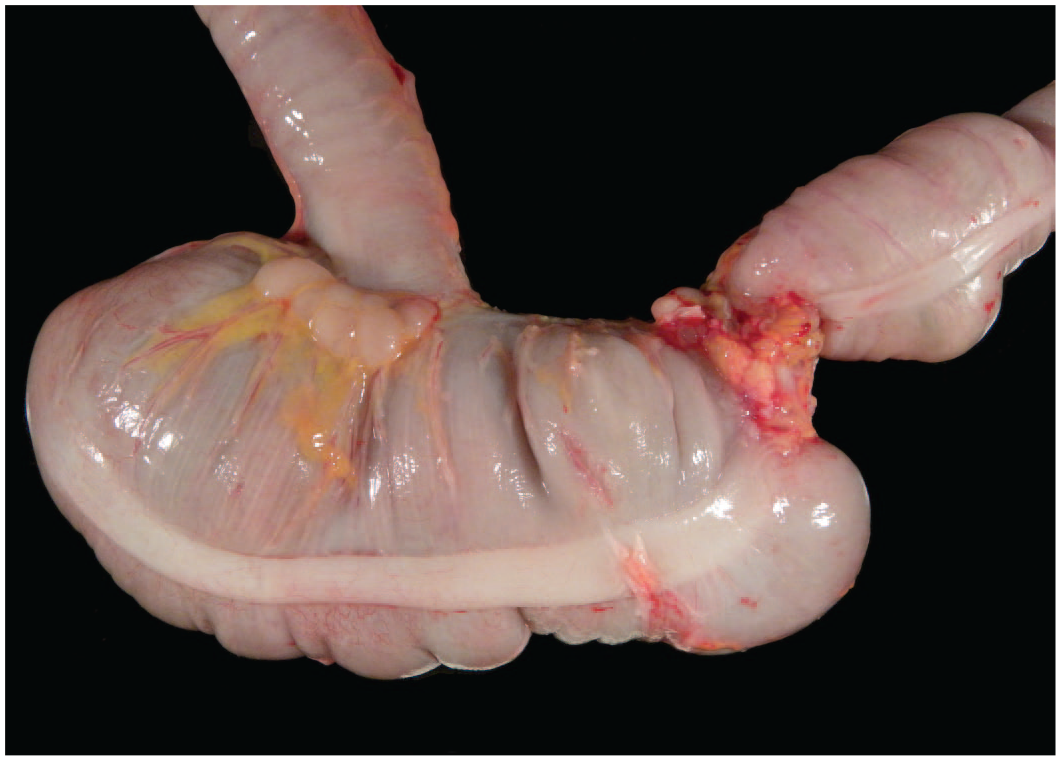
Colonic diverticulosis is common in older animals and is defined as outpouching of the mucosa and submucosa through the muscularis. Predisposing factors are unclear, but there is some thought that it may be due to spastic contraction of the colon, low dietary fiber, or it may have genetic associations. Grossly, there are saccular protrusions between the taenia coli which are readily evident on the serosal surface (Figure 35). The entire wall of the diverticulum, including the muscular wall of the colon itself can become extremely attenuated and thin (Figure 36). Lesions may be focal or multifocal and involve extensive regions of the colon. The diverticulae may become impacted, filled with debris and rarely inflamed, which is then termed diverticulitis.145,147-149

Saccular protrusions are evident between the bands of taenia coli. Rhesus macaque, colon, diverticulosis.

The diverticulum is composed of a normal, to slightly inflamed mucosal layer surrounded by markedly attenuated submucosal and muscular layers. Rhesus macaque, colon, diverticulosis. Hematoxylin and Eosin (H&E).
Gastric dilation (bloat) was first described in nonhuman primates by Chapman 150 in 1967 and is currently a rare occurrence in well-managed colonies that predominantly affects juveniles and adults. Animals are often found dead with an enlarged and taut abdomen. Gastric distention with fermented gaseous ingesta is a consistent finding. Progressive gastric expansion is associated with vascular stasis in the stomach and compression of spleen, liver, diaphragm, portal vein, and vena cava. This may lead to respiratory distress, a fall in arterial blood pressure, metabolic acidosis, electrolyte disturbance, and shock. When intragastric pressure exceeds gastric venous pressure and causes mucosal ischemia irreversible necrosis of the stomach wall, perforation, and sepsis will occur. 151
Microscopically, the gastric wall can be extremely attenuated, epithelial cells may have sloughed from the mucosa and blood vessels in the mucosa and submucosa are severely congested. If the stomach ruptures, there usually is evidence of necrosis within the gastric wall. The absence of hemorrhage at the rupture site indicates that rupture occurred after death. In severe cases, as well as gastric rupture, there may be rectal or vaginal prolapse.
Clinical histories often include overeating (with rapid fermentation of carbohydrates), food restriction, or anesthesia. Clostridium perfringens type A has received much attention as the cause of gastric dilation and can be isolated in large numbers 152 in some but not all cases and may be responsible for gas production. Other gastric bacteria like Lactobacillus, Enterobacter cloacae, and E. coli may also be involved.151,153
Rectal prolapse, defined as the protrusion of one or more layers of the rectum through the anus, is a relatively common occurrence in young animals with diarrhea but often spontaneously resolves. Diarrhea, tenesmus, and parturition are risk factors. 154 Intermittent or recent prolapse may be identified at necropsy as a dark red, edematous region of rectum/distal colon within the pelvis/caudal abdomen because of intermittent compromise to venous return. Persistent prolapse may result in complete devitalization of the bowel with full-thickness necrosis and is easily recognizable at gross necropsy. Microscopically, the involved region of rectum has edema accompanied by an inflammatory cell infiltrate including moderate numbers of neutrophils in the submucosa and sometimes the muscular layers. Vessels in the submucosa are often dilated and may contain fibrin thrombi. Superficial epithelial cells may be sloughed, and the lumen may contain necrotic cells.
Intussusceptions occur when one segment of the intestine telescopes or slides inside another often resulting in intestinal obstruction. They are usually seen in younger animals and commonly involve the small intestine and ileocecal junction. In rare cases, a colonic intussusception may become prolapsed through the anus (Figure 37). Risk factors include diarrhea and intestinal hypermotility. In an early intussusception, the involved intestine may be red to dark red and congested due to compromised venous return. As the lesion ages, the bowel may become progressively more devitalized and difficult to reduce with fibrin adhesions between serosal surfaces. Microscopic lesions may range from early congestion with or without hemorrhage and edema, and neutrophilic to mixed inflammation to more chronic and severe mucosal to transmural necrosis and inflammation with peritonitis and fibrin adhesions.

An intussusception of the descending colon at the level of the pelvic canal shown here was associated with rectal prolapse of a portion of the intussuscepted colon. Rhesus macaque, pelvic canal, intussusception.
Colonic torsions are infrequently identified in juvenile and adult macaques.155,156 Risk factors include previous abdominal surgery, abdominal adhesions, recurrent or persistent diarrhea, idiopathic megacolon, semipurified (atherogenic) diets, and sedentary existence. Animals usually present with marked abdominal distention and shock. At necropsy the affected sections of large intestine are markedly dilated with gas and the serosa and mucosa markedly thickened and sometimes necrotic ranging from red to purple or black. The contents of the affected colon are generally brown and bloody, and the bowel distal to the obstruction is usually pale and empty. Microscopic lesions are similar to those seen in intussusceptions because the pathogenesis involves compromised venous return and later ischemia. Gastrointestinal volvulus is rarely reported in nonhuman primates.
Intestinal carcinoma is the only common malignancy of macaques, generally older macaques, and is of importance when working with aged animal cohorts. The affected age range from published reports is 7 to 40 years, with mean ages of 22.1 to 26.4 years from larger studies, reflecting its occurrence in aged animals.145,157,158 Although the majority of reported cases have been in rhesus macaques, it occurs in cynomolgus 157 and Japanese macaques (authors’ experience). There is no apparent sex predisposition. Clinical symptoms include weight loss, inappetence, and/or reduced fecal production. The majority of tumors arise from the ileocecal junction, cecum, and proximal colon and have a relatively indolent growth pattern with metastasis in approximately one-third of cases.145,157 Involvement of draining lymph nodes and diffuse peritoneal carcinomatosis occur with some frequency. Extra-abdominal metastases are much less common.145,157
These tumors appear grossly as constricting annular masses often with proximal secondary obstructive enteropathy, similar to chronic cicatrizing ulcerative colitis (Figure 38). The mucosal surface exhibits extensive ulceration overlying the mass with variable proliferation of adjacent mucosal surface. Polyp formation is unusual. The intestinal wall is transmurally thickened and firm. In the mucinous adenocarcinoma subtype extension to the serosal surface imparts a finely “bubbly” appearance due to the presence of numerous neoplastic cysts filled with abundant mucin (Figure 39). Microscopically, tumors are composed of crowded cuboidal to columnar cells forming irregular glands, tubules and acini surrounded by dense fibrovascular stroma (desmoplastic response). The neoplastic cells frequently invade the submucosa and traverse the muscularis in columns extending to the serosal surface. The mucinous adenocarcinomas produce abundant mucin and form lakes of basophilic material partially lined by flattened neoplastic cells (Figure 40).
The presence of an adenocarcinoma has created a stricture in the colon and subsequent dilation of the proximal intestinal tract. Rhesus macaque, colon, adenocarcinoma.

Transmural invasion of a mucinous intestinal adenocarcinoma imparts a “bubbled” appearance to the serosal surface. Rhesus macaque, colon, adenocarcinoma.

Lakes of pale basophilic mucin, partially lined by neoplastic columnar to attenuated epithelial cells distend the submucosa. Rhesus macaque, ileocecocolic junction, mucinous adenocarcinoma. Hematoxylin and eosin (H&E).
Summary and Conclusion
Diarrhea and associated gastrointestinal lesions are the most common spontaneous findings in macaques at the national primate centers and in other captive macaque colonies. This review provides pathologists, toxicologists, and researchers with a comprehensive understanding of these findings that will be useful in determining the cause and test article–relatedness of gastrointestinal lesions identified in toxicology and research studies utilizing macaques.
Footnotes
Acknowledgements
T.N., S.N., and R.A. are thanked for their assistance in generating photomicrographs. The histotechnicians of the CNPRC, ONPRC, Charles River, and Genentech are also thanked.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Pathology Cores at the Oregon National Primate Research Center (ONPRC) and California National Primate Research Center (CNPRC) which are supported by NIH Awards P51 OD 011092 and P51 OD 011107, respectively.