
Abstract
Determining adversity of effects in toxicology studies continues to pose a dilemma to practicing toxicologists and pathologists. How this determination is made may follow either a focused or broad approach to assessing the study data. The choice of which approach is best is dependent on a variety of factors. Therefore, we present a philosophical perspective on the determination of adversity across toxicology studies that may be applied in inhalation studies and those conducted by other routes of exposure.
While the following series of papers addresses the toxicopathology and adversity of inhaled biologics, a perspective on the evaluation of adversity across toxicology studies, in general, is a philosophically appropriate introduction. The assessment of adverse responses is the basis of toxicology. This is pursued, essentially, from 2 different points of view; either a focused approach where the assessment of a molecule determines adversity at a particular dose in a particular study or a broader approach where reevaluation of lower doses of a study is utilized in defining adversity as an observation that may have initially been regarded as inconsequential but may represent where the adverse effect was first seen when viewed in the context of the entire study as this information would be useful to the clinical investigator. The assessor of the response, usually the toxicologist or pathologist, must decide on the appropriate approach for the assessments she/he is asked to make. The focused approach is based on a particular study, time period, observation, and so on, and ultimately addresses only the specific context of the study under evaluation. The broader approach uses extrapolation of observations from the first point they are observed, through a dose response. The broad approach also addresses the progression of the finding across increasing dose groups and increasing study duration, entering the area of risk assessment. The authors are of the opinion that while theoretically desirable, it is not possible to separate an assessment of adversity within a particular study from an overall risk assessment given the expectations of nonclinical safety evaluations to look at individual responses and form an overall opinion of the acceptability of the observed adverse effect(s) and the progression from nonadverse to adverse in a dose-related fashion.
From the focused point of view, it is acceptable to determine that at a particular dose for a particular duration of exposure an effect is not adverse; however, if at the next highest dose the same response, whether it is an enzyme change, a behavioral observation or an alteration of tissue morphology is determined to be adverse, it may be advisable to provide a perspective on the lower dose as a precursor stage that is actually part of the dose response. Granted, it may be that at the nonadverse dose the change is not physiologically consequential or is reversible, and it would be safe and appropriate to conduct a clinical study to evaluate the human response, utilizing biomarkers, and its relevance to the nonclinical data. The overall assessment of adversity itself is a progressive process, either by dose or duration or both.
It is our ultimate responsibility in evaluating a nonclinical toxicology study to assess monitorability and manageability of potentially adverse findings, in addition to the identification of an adverse effect level. Although many decisions are made at various stages in the drug development process, the ultimate responsibility is to assess the potential for any changes observed to progress with either dose or duration and to ultimately recommend that a potential new drug is appropriate to use under a specific protocol and eventually for the general public, based on a consideration of the patient population, monitorability of effects, reversibility of effects, and available alternative therapies. As such, the more focused view of adversity is specifically applicable to the safety of a proposed clinical trial at specific doses and duration.
As reflected in the following articles, determining the adverse nature of a particular finding in a toxicology study is the cornerstone of the craft and a difficult assessment to make for the practicing pathologist or toxicologist. Despite the difficulty, ultimately the expert opinion is necessary to identify a no-observed-adverse-effect-level (NOAEL) or no-observed-effect-level (NOEL) for the study in question; the keyword in both terms being “observed.” The subjective determination of adversity is critical for risk assessment and regulatory decision-making and is also used to determine a safe clinical starting dose for pharmaceuticals and acceptable exposure levels for agricultural and industrial chemicals. This professional/expert opinion is an iterative process based on the spectrum and severity of lesions present within a particular study and ultimately in follow-up studies. The decision-making can be facilitated by using a consistent definition of what constitutes an adverse effect, but what may appear to be a rather straightforward task has been debated in the literature for over 2 decades to find a universally acceptable definition that can be applied in actual practice.
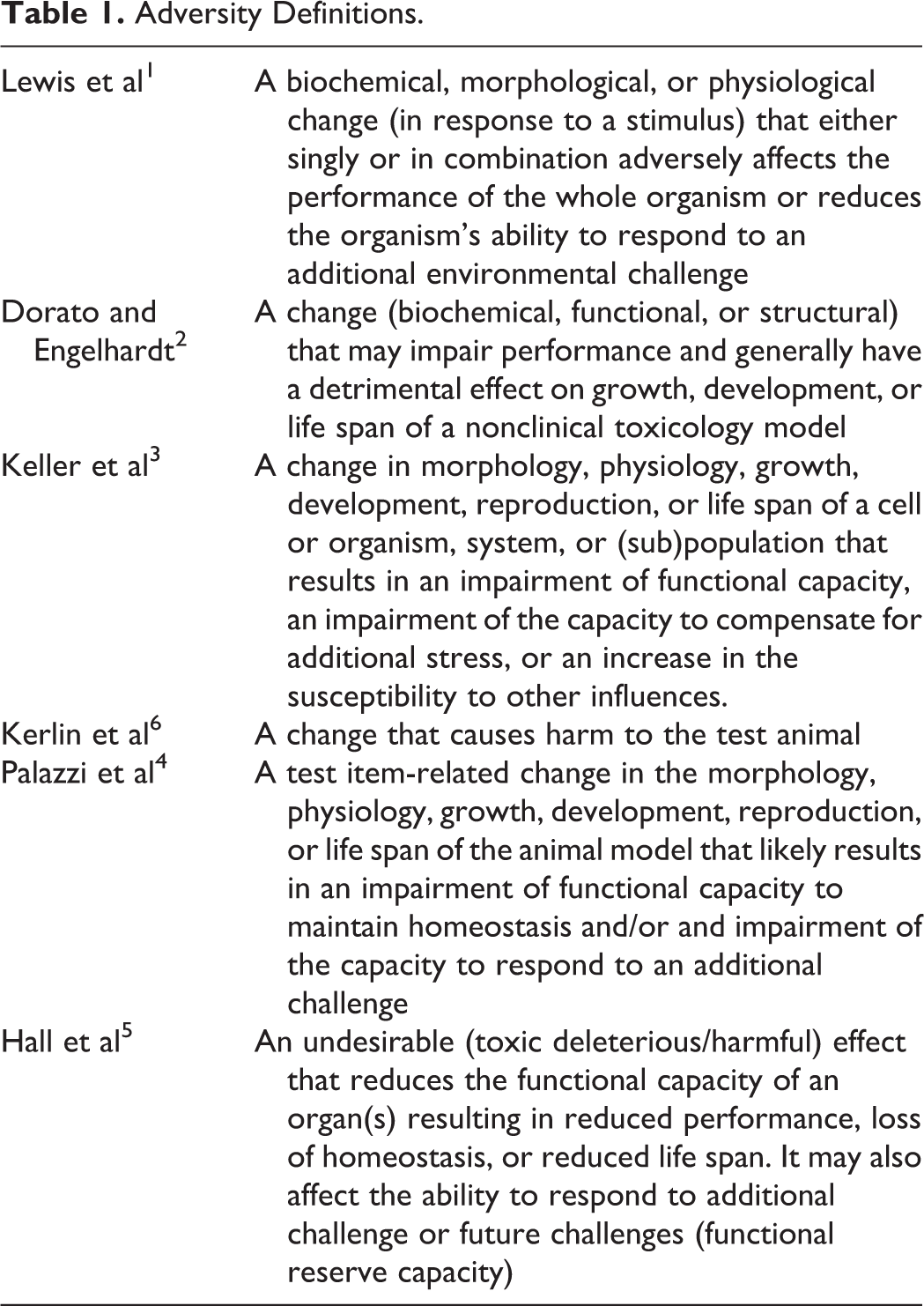
Thoughts relative to how best to define adversity within the context of a toxicology study have continued to mature since the paper by Lewis et al was published in 2002. 1 The definitions of what constitutes an adverse finding are presented in Table 1. A common theme through all the definitions, though, is the impairment of organ function or loss of capacity to respond to additional challenges that can shorten the life span of a test subject. Causing harm to test subjects is, therefore, the apical consideration in determining whether or not a finding may be interpreted as being adverse. Harm may come from a disturbance in functional capacity of an organ or system, an impairment of the capacity to compensate for additional stress, or an increase in the susceptibility to other influences, but ultimately it may be interpreted that a harmful event, be it clinical signs or functional changes, should be regarded to be adverse. In the earlier publications, 1 -3 there remained room for disagreement on interpretation. By codifying an adverse finding as harmful or “…an effect that would be unacceptable if it occurred in a human clinical trial,” 2 interpretation should be more consistent. Based on this definition, some findings in a study may be inherently adverse while in many cases it will be dependent on the specific characteristics of a pathological change including severity, distribution, accompanying/collateral effects, impairment of reserve response capacity, and related lesions, recognizing that “there is no one formula or method that can be applied to all adversity decisions.” 4 As such, alterations that are minimal or slight in severity are less likely to be adverse than those of moderate or greater severity, but this is also dependent on the type and location of the lesion. This is consistent with the premise that low severity perivascular/peribronchiolar mononuclear cell infiltrates, pure alveolar macrophage proliferation, and alveolar inflammatory cell infiltrates with no accompanying changes in the lung structure or lung function would not be regarded to be adverse, as outlined by Hall et al. 5
Adversity Definitions.
Relative to the administration of inhaled biologics, as discussed in this special journal edition, the evaluation of bronchoalveolar lavage (BAL) fluid, as with other clinical pathology parameters, should not be used in isolation in the determination of adversity; however, it should be part of an integrated assessment of morphological changes in the respiratory tract alongside systemic hematology and clinical chemistry parameters. 7 This is particularly important as BAL fluid analysis only visualizes what is occurring at the epithelial surface (inflammation, epithelial cell injury) and cannot assess deeper alterations that may occur with chronic injury. Decisions should be made on a case-by-case basis utilizing all of the available study data, with systemic effects also being considered in view of the local organ effects (ie, secondary toxicities).
Progression of an adverse lesion should only be considered when data are available that demonstrate progression. A theoretical prediction of progression should not be taken into account in assessing the adversity of a particular lesion in any specific study. Pragmatically, the discussion of progression should be a retrospective look across studies for an indication of first occurrence, probably not judged initially to be adverse, of something that was called adverse at a higher dose or longer duration. 1 It is also important to frame adversity within the context and parameters of a given study 2 as adversity designations and NOAEL will likely change as more data become available over the course of a development program. Further, context beyond the histopathology description has the potential to influence an adversity designation suggesting that adversity should not be determined by histopathology in isolation 8 unless no other contextual data are available. 4 There is jeopardy in making an adversity call–based solely on histopathology observations as is suggested in different instances in the following reviews in this compendium. There may be species-specific changes that may be termed adverse but have negligible relevance for the overall clinical risk assessment. Also local versus systemic effects need to be considered, which is why all data for a given study must be subjected to an integrated analysis.
In the overall evaluation of toxicology studies that are part of a development program, it is important to revisit the nexus between adversity assessment in nonclinical studies and the risk assessment as it would be applied to human exposure. We realize that adversity in test animals does not necessarily translate to adversity for human exposure. However, decisions regarding adversity of the study data should be made with some consideration of the risk assessment, as the 2 processes follow a similar pathway and are linked. Further, an adversity call need not “adversely” affect development of a drug candidate; as mentioned previously, the patient population and available therapy must be considered.
During the interpretive phase of the overall development process, conducted by the pathologist and toxicologist, general statements regarding the monitorability and manageability of adversity, in any organ system should be made and not just name an adverse effect and a NOAEL. This discussion is most appropriate in the Investigator Brochure or Investigational New Drug application/Investigational Medicinal Product Dossier overview rather than in the individual study report. 4,6 No matter how we look at it, defining adversity is still an iterative, holistic, process that must take into account not only the morphologic alteration but also its effect on the whole animal and whether or not there is human relevance that can be monitored and mitigated. Therefore, in the holistic evaluation of adversity and the overall assessment of the ability to develop a particular molecule, the relationship of an adverse response assessed in an individual study and the potential reassessment of the dose producing an adverse effect in studies of longer duration must be integrated with the overall risk assessment for a program that allows a molecule to move forward in development or terminates development.
Ultimately, the assessment of adversity for a particular study is generally recognized as an expert opinion based on the specific context of study conduct, reinforcing the more focused view of assessment of adversity when asked if a specific clinical trial, or a specific study duration, would be safe to conduct. A useful practical definition of an adverse finding 3,4,6 focuses on functional organ capacity, although evaluation of pulmonary function is uncommon in Good Laboratory Practice compliant studies. The lung, however, has a remarkable compensatory capability to allow continued gas exchange, so the functional definition is, as with all definitions of adversity, not perfect. In addition, the somewhat subjective assessment of severity can lead to differences of opinion between different individuals. As we see emphasized in the following papers, 5 the assessment of adversity of a study-specific finding is in fact a professional/expert opinion related to the relevance of the nonclinical model and the context of the specific clinical trial the work is to support. As such, conclusions in the narrative regarding the adversity of a particular findings should be supported by an adequate explanation of the rationale used regarding how the effect was determined to be adverse or not.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.