
Abstract
Significant advances in immunotherapies have resulted in the increasing need of predictive preclinical models to improve immunotherapeutic drug development, treatment combination, and to prevent or minimize toxicity in clinical trials. Immunodeficient mice reconstituted with human immune system (HIS), termed humanized mice or HIS mice, permit detailed analysis of human immune biology, development, and function. Although this model constitutes a great translational model, some aspects need to be improved as the incomplete engraftment of immune cells, graft versus host disease and the lack of human cytokines and growth factors. In this review, we discuss current HIS platforms, their pathology, and recent advances in their development to improve the quality of human immune cell reconstitution. We also highlight new technologies that can be used to better understand these models and how improved characterization is needed for their application in immuno-oncology safety, efficacy, and new modalities therapy development.
Keywords
Introduction
Humanized mice, or human immune system (HIS) mice, are terms used to describe immunodeficient mice reconstituted with a HIS. They are increasingly used for modeling the human immune compartment and are a powerful translational tool for investigating the human immune response in disease states. The ability to investigate human immune behavior in rodent models offers a new generation of in vivo investigations which until now have been futile in murine models without human immune representation.
Human Immune System Mouse Model Platforms
Three major HIS models have been used to examine the human immune response in immunocompromised mice: the human peripheral blood lymphocytes (hu-PBL) model, the human stem repopulating cell (hu-SRC) model, and the bone marrow, liver, thymus (BLT) model. Each model has its own advantages and disadvantages, described in detail below (Figure 1) and a summary of the models can be found in Table 1.
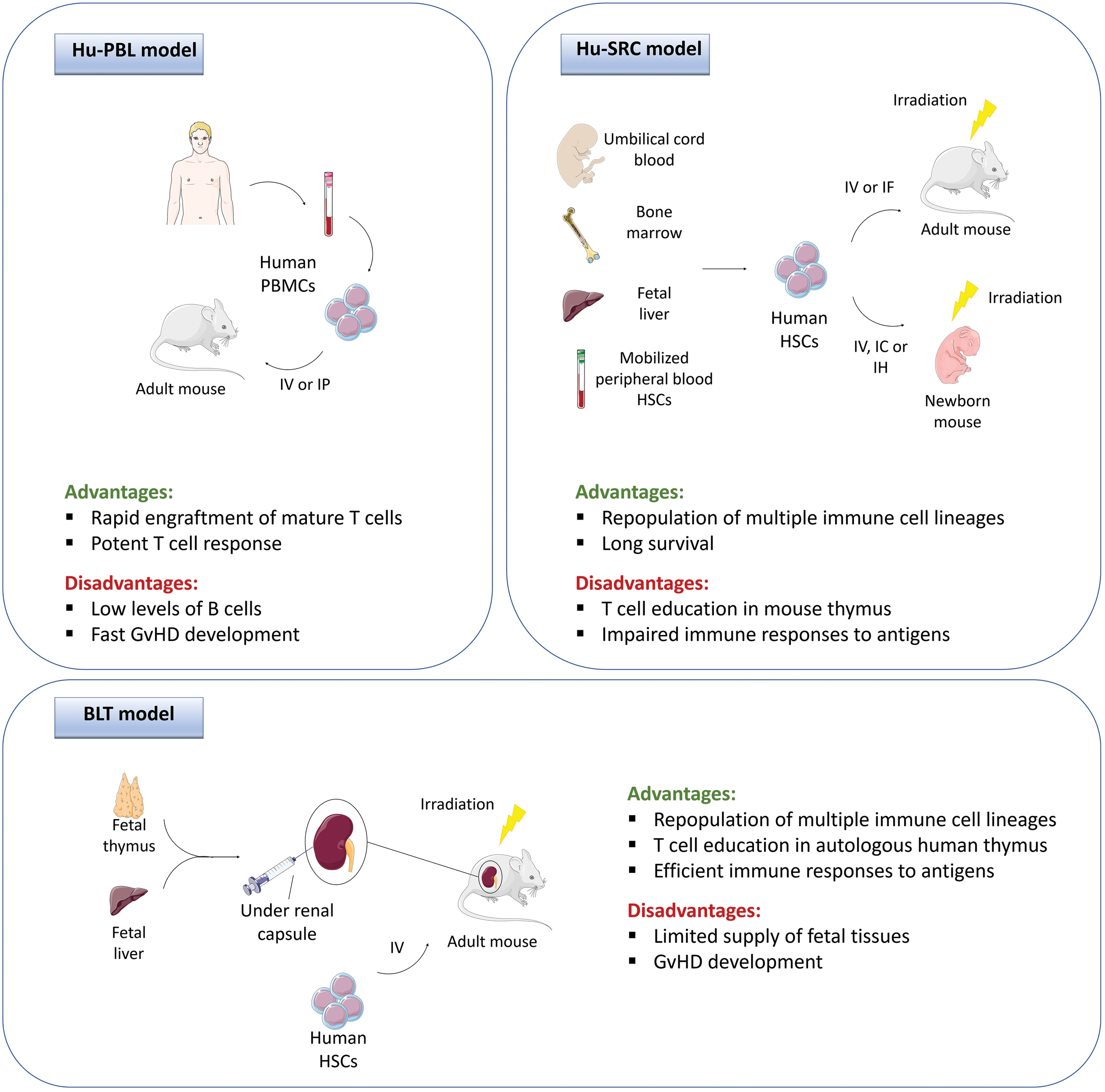
Generation and features of different humanized mouse models: The hu-PBL (human peripheral blood leukocytes) model is generated by intravenous (IV) or intraperitoneal (IP) injection of human peripheral blood mononuclear cells (PBMCS) to an adult immunocompromised mouse. in the hu-SRC (human stem repopulating cell) model, hematopoietic stem cells (HSCS) derived from either umbilical cord blood, bone marrow, fetal liver, or mobilized from peripheral blood, are engrafted into irradiated adult immunocompromised mice via IV or intrafemoral (IF) injection, or into irradiated newborn immunocompromised mice via IV, intracardiac (IC) or intrahepatic (IH) injection. in the BLT (bone marrow, liver, thymus) model, adult immunocompromised mice are irradiated and transplanted under the renal capsule with fetal thymus and liver fragments and injected with autologous hscs. GVHD indicates graft versus host disease; hu-PBL, human peripheral blood lymphocytes.
Immunodeficient Platforms Used for HIS Mouse Models.
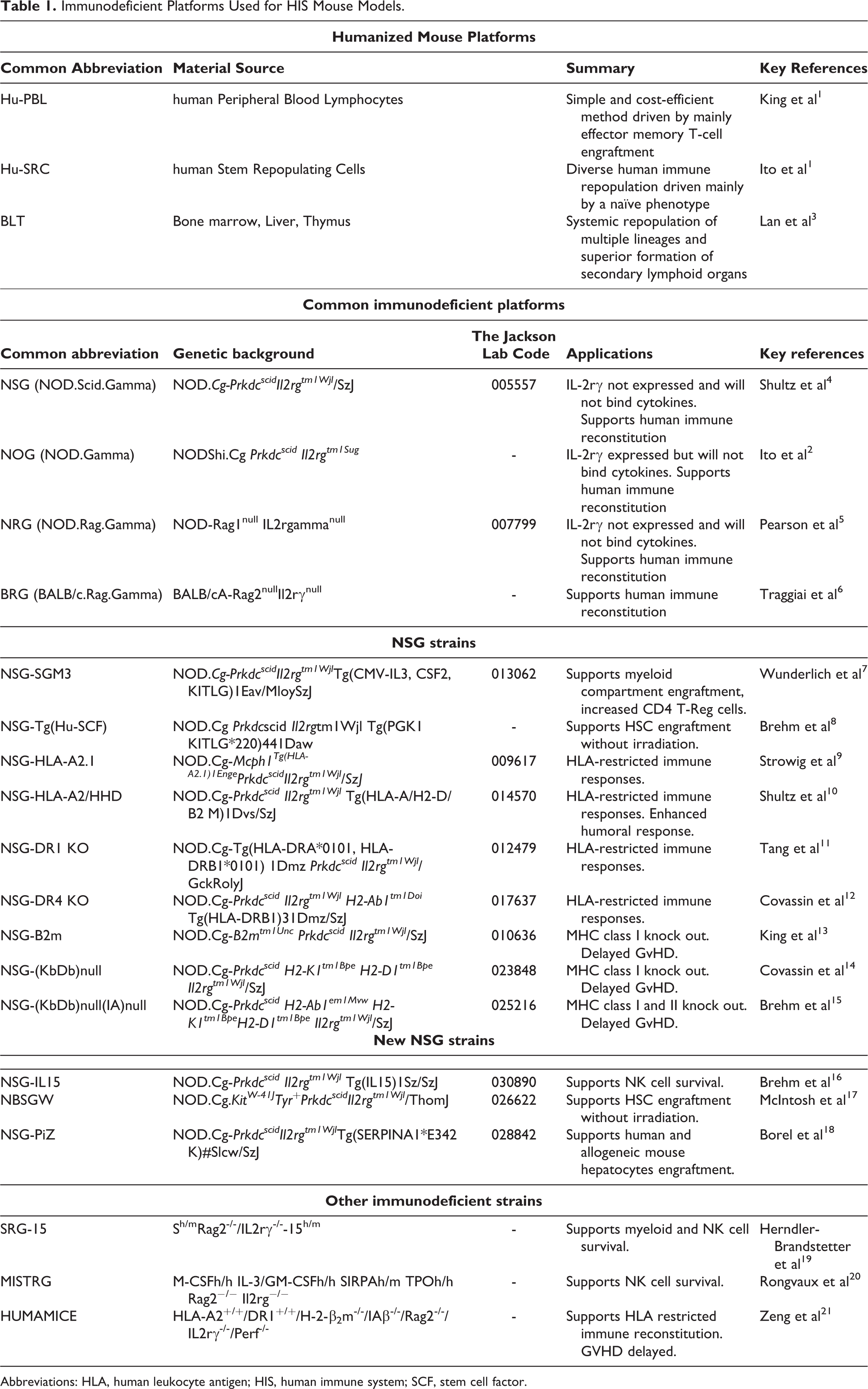
Abbreviations: HLA, human leukocyte antigen; HIS, human immune system; SCF, stem cell factor.
Human-Peripheral Blood Lymphocytes Model
The hu-PBL model has been extensively used for the study of mature immune responses and is the simplest and most cost-efficient method of humanization. Large quantities of human leukocytes can be isolated from peripheral blood, spleen, and lymph nodes. Depending on the model, isolated leukocytes can be engrafted via intravenous (IV), intraperitoneal, intrafemoral (IF), intracardiac (IC), or intrahepatic (IH) injection, which may be preconditioned with a sublethal dose of irradiation (Figure 1). Preconditioning of NSG mice in this model is not necessary because the human cells injected in the peripheral blood mononuclear cell (PBMC) inoculum are already mature human leukocytes, which will not need to undergo differentiation in the mouse environment. It has been reported that a low dose of irradiation facilitates engraftment and colonization of human PBMCs in the mouse immune compartments. However, it also accelerates xenogeneic graft versus host disease (GVHD), resulting in a shorter survival than that of nonirradiated mice receiving PBMCs. 13 This advantage of this model is that it avoids significant delay in engraftment as the human leukocytes injected are already mature. Human leukocytes can be found circulating in the murine peripheral blood within days after injection and can be maintained for up to 4 to 6 weeks. Human T cells are the main population present in this model, with an activated memory/effector phenotype. 1,22 Additional populations including human B cells and myeloid cells are present, but at much lower levels. This is likely due to the lack of human specific cytokines required for their survival and the dominant expansion of T cells. 23,24 The main disadvantage of this model is the rapid development of GvHD, directly correlated with the levels of human activated T cells present in the host due to their recognition of the murine environment. Hence, the experimental window of this model is limited to short-term studies. 13 However, utilization of new strains of mice deficient in the major histocompatibility complex (MHC) class I and/or II, can delay GvHD and increase survival to widen this experimental window. 15
Human Stem Repopulating Cell Model
The hu-SRC model is established following injection of human hematopoietic stem cells (HSC) in immunocompromised mice engrafted either as adults 2 or new-borns. 25 For this model, preconditioning with sublethal irradiation is essential. Although the NSG strain is one of the most immunocompromised mouse strains described, these mice still have some immune cells present, mainly neutrophils and monocytes, together with defective dendritic cells and macrophages. In order to achieve effective levels of human HSC engraftment, myelosuppression to deplete mouse HSCs is necessary. Moreover, after preconditioning, the expression of stem cell factor (SCF), which is critical for HSC engraftment, proliferation and survival, is increased. 26 Limited success in engrafting human HSCs in non-preconditioned NSG mice has been described previously. 17 The development of new mouse strains, with mutations in c-Kit (SCF receptor) 17 or with transgenic expression of membrane-bound human SCF, 8 allow the successful engraftment of human HSCs without previous irradiation.
Hematopoietic stem cells can be obtained from cord blood, 27 bone marrow (BM), 28,29 fetal liver 29 or BM-derived HSCs mobilized into the peripheral blood with granulocyte-colony stimulating factor. 4 Cells are injected IV or IF in adult mice and either IV (facial vein), IC or IH in new-borns 22 (Figure 1). In this model, a diverse repertoire of cell populations are generated. Engrafting new-born or young mice (up to 4 weeks) allows accelerated generation of T cells in comparison to adult mice. 30 The main caveats of this model are the time taken to establish this model (typically 16 weeks or more), a lack of a functional B cell compartment which is in part due to inadequate CD4 helper functions, and lastly impaired antigen response by the HIS. 31 –33 This is partly due to the absence of human primary lymphoid organs and therefore limited differentiation of human cells in the mouse environment, and secondly due to the lack of human leukocyte antigen (HLA) on thymic epithelium and therefore a lack of HIS, specifically T cells, education. Advances in the development of new strains which incorporate human growth factors and cytokines through genetic manipulation, summarized below (Table 1), may help to overcome some of these deficiencies.
Bone Marrow, Liver, Thymus Model
In the BLT model, mice are surgically transplanted with fragments of human fetal liver and thymus under the kidney capsule of sublethally irradiated immunocompromised mice. This is followed by an IV injection of autologous HSC cells 3 (Figure 1). This model allows systemic repopulation of multiple lineages of human immune cells including T, B cells, monocytes, macrophages, and dendritic cells. Superior to the other models is the enhanced reconstitution of secondary lymphoid organs which aid in HIS education and therefore enhance immune responses to antigens. 34,35 Because human T cells are educated in autologous thymic tissues in the BLT model, it has been important in the investigation of human T cell development. 36,37 Furthermore, this model has had a great impact on the study of infectious diseases, especially HIV, as this model improves the colonization of lymphoid organs, together with the human reconstitution of the mucosal and gastrointestinal tracts. 35 In this model, BLT mice can recapitulate mucosal transmission of HIV via vaginal and rectal routes. 38 Nevertheless, these mice exhibit a higher incidence of GvHD compared to the hu-SRC model, some of them earlier than 20 weeks posttransplantation. 39
Immunodeficient Platforms
A variety of immunodeficient mouse strains can be used to host human immune cells, each appropriate for different experimental aims. A number of immunodeficient strains have been developed through genetic manipulation of Prkdcscid and the recombination activating gene (RAG) to ablate adaptive lymphocytes. 40 Immunodeficient scid and RAG mice are crossed with nonobese diabetic mice which have a dysfunctional innate immune compartment. The introduction of an interleukin (IL)−2Rγ knock-out blocks the signaling pathways of a diverse repertoire of cytokines and therefore results in the absence of functional natural killer (NK) cells. The main immunodeficient platforms include NSG, 4,25 NOG, 2,41 NRG, 5,42 and BRG 6,43 Their genetic background, full names, acronyms, and descriptions of their acronyms are summarized in Table 1. Comparison of human CD45 engraftment in NSG, NOG, and BRG show that NOG and NSG have higher engraftment levels than BRG. 30 In this study, higher engraftment of cord blood reconstituted mice was reported in NSG mice compared to 3 other immunodeficient strains. Furthermore, higher engraftment in NSG females has also been described. 44 Therefore, NSG are the most widely used platform for HIS mice. A wide variety of NSG strains have been developed in recent years to overcome issues such as GvHD, lack of HLA-specific responses, and lack of innate immune cell survival. Several of these NSG strains have been previously reviewed by Shultz et al 43 In our review, commonly used strains 7 –14,15,45 –48 are summarized in Table 1. More recent advancements in immunodeficient platforms are also summarized in Table 1 and described below. 16,17,18 –21
The survival of NK cells and the myeloid compartment has been a major limitation in HIS mouse models. Recently, new immunodeficient strains have been developed to address this shortfall. Interleukin-15 is imperative for NK cell development and this has been exploited in order to improve NK cell engraftment in immunodeficient models. 16,19 A number of strains have been developed to increase NK cell development and survival in HIS mice. Firstly, the NSG-IL15 model, with transgenic IL-15 expression, show enhanced CD56+ NK cell development in blood, spleen, and BM. 16 Secondly, the SRG-15 model is another immunodeficient mouse model which supports NK cell development. 19 A human SIRPα knock-in on a BRG background (SRG) was crossed with a human IL15 knock-in mouse to generate SRG-15 mice. Mice humanized with CD34+ fetal liver hematopoietic stem and progenitor cells, supported CD8+ T cell, NK cell, and innate lymphoid cell development. In this model, higher circulating NK cells were found in the blood compared to SRG and NSG without IL-15 expression. Furthermore, both major NK cell subsets, CD56bright CD16− and CD56dim CD16+ NK cells, were present in the blood and spleen of SRG-15 mice 7-week postengraftment. These NK cells shared phenotypic similarities with circulating human donor NK cells and were highly functional as shown by evident tumor infiltration. Lastly, another model, MISTRG mice (Table 1) also supports myeloid and NK cells. 20 However, MISTRG mice develop anemia early and therefore their lifespan is a limiting factor in experimental design. This is not an isolate example on how manipulation of genes involved in immune responses and hemopoiesis could have an impact on the health and life span of immunocompromised mice, which are well known to display greatly increased susceptibility to infections caused by viral, bacterial, fungal, and parasitic agents. 49,50
In order to allow or increase engraftment, immunodeficient mice are commonly irradiated before reconstitution with the human compartment. In addition to the desired myeloablation that favors engraftment of human cells, total body irradiation conditioning regimens are associated with a plethora of side effects. 51,52 These can occur with an acute or delayed onset affecting multiple organ systems such as the hematopoietic system, gastrointestinal tract (eg, radiation enteropathy 53 ), kidney, 54 and several others. While a considerable amount of literature has been published on the effects of radiations in humans and animal models, few studies have specifically addressed the consequences of current irradiation regimens in HIS mice and how these could influence the outcome of studies, for example, confound the interpretation of test item-related effects or limit animal life span. A new model has been developed to increase HIS engraftment without the need for preconditioning. The NBSGW mice (Table 1) support CD34+ HSC engraftment without irradiation. These mice are generated through crossing NSG mice with the C57Black mice homozygous for c-Kit, the SCF receptor required for haematopoiesis. 17
Another major limitation with HIS mice has been the lack of human-specific HLA responses. Although advances have been made to increase HLA restricted responses in HIS mouse models, they have been restricted to introducing specific HLA molecules. A new immunodeficient model, HUMAMICE (Table 1), express all human HLA molecules (HLA-A2+DR1+) instead of mouse MHC molecules. 21 The HUMAMICE were generated through depletion of murine Rag 2 allele, IL2rγ allele, and the perforin allele (Perf), from a Sure-L1 background, which are mice expressing human HLA molecules. The HUMAMICE reconstituted with HLA-matched (HLA-A2+DR1+) PBMCs showed T and B cell survival up to 12 weeks and showed evidence of functional humoral immunity demonstrated by immunoglobulin (Ig)G and IgM responses to immunization. Furthermore, there was no evident GvHD compared to NSG knock out for the MHC class I. 21
Pathology of HIS Mouse Models
Limited information is available concerning the morphological aspects of tissue repopulation and the prevalence of histopathological lesions in immunodeficient mice engrafted with a human immune compartment. Functional defects of the immune system in immunodeficient mice are paralleled by abnormal development of the primary and secondary lymphoid organs, which vary structurally across strains. 55 For example, NSG mice, 2,56,57 exhibit small poorly developed primary and secondary lymphoid organs, which lack typical lymphoid structures and are composed solely of reticular stromal cells. 4,43,55,58 Following transplantation of human cells, factors such as donor cell source, features of the recipient host system, and engraftment methodologies have a great influence on the extent, cell composition, and morphological aspects of reconstitution in the different organs. 30 Many murine models of human immune engraftment exhibit variable proportions of multilineage repopulation in the hemolymphatic organs. Here, human cells form variably sized aggregates that in general do not fully recreate the lymphoid tissue architecture typical of immunocompetent organisms, nor form distinctive lymphoid structures such as lymphoid follicles, germinal centers in the spleen or lymph nodes, nor lead to identifiable cortical and medullary structures in the thymus. 3,5,59 Repopulation of the latter appears to be more efficient in immunodeficient mice transplanted shortly after birth, while thymuses of mice engrafted in adult age are alymphoid exhibiting cysts and are less prone to support human cell engraftment. 30,60
As previously indicated, mice engrafted with human cells may develop xenogenic GvHD within a few weeks posttransplantation. 61,62 Prevalence, onset, and the morphological features of GvHD vary greatly across the various experimental models. However, GvHD occurs with high incidence and severity in those models where mature T cells represent the primary population of engrafting cells, like the HU-PBL model, in line with the pathogenesis of this immune-mediated condition in which activated T cells play a crucial role. 63 –65 Clinically, GvHD occurs as a generalized wasting syndrome leading to progressive body weight loss and/or a severe skin condition characterized by alopecia; the latter is associated histologically with dermatitis and scleroderma. 66,67
Graft versus host disease can however manifest also as a systemic inflammatory reaction affecting multiple organs including the hemolymphoid organs, liver, lungs, and several others (Figure 2). Inflammatory infiltrates are dominated by lymphocytes (mainly CD3+ T cells, with a prevalence of CD4+ lymphocytes) and macrophages, with occasional formation of microgranulomas. 66,68 Mice exhibiting symptoms of GvHD are often excluded from studies, although little is known concerning the actual prevalence of subclinical GvHD within each single model. While further work is required to establish whether FACS parameters or other biomarkers can be used to allow early and accurate identification of mice affected by GvHD, histology represents a valuable tool to appreciate this potential confounding effect when interpreting engraftment and experimental data. 43
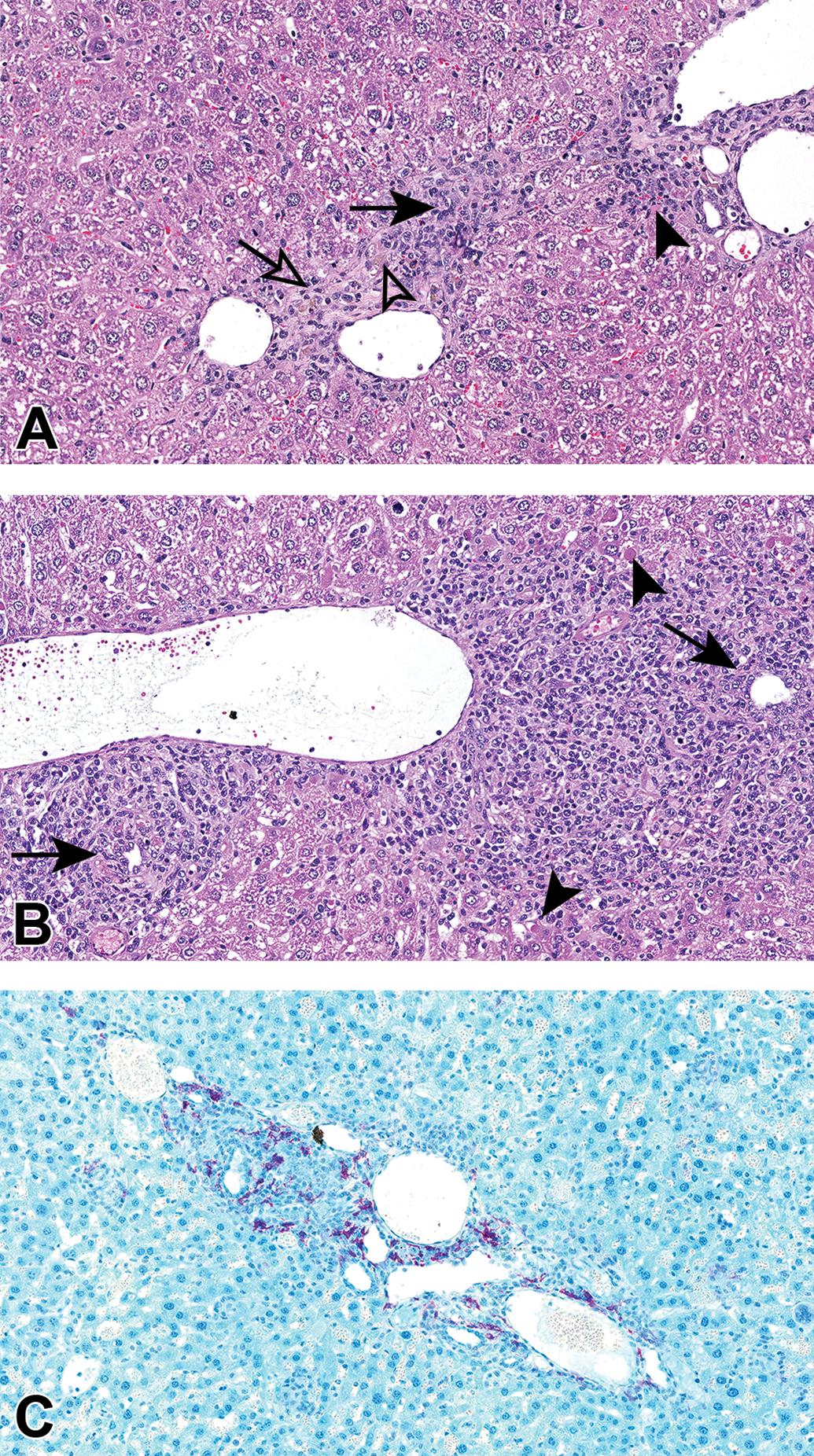
Graft-versus-host disease (GvHD) in the liver of NSG mice transplanted with human leukocytes (A; hu-PBL model) or human hematopoietic stem cells (B and C; hu-SRC model). (A and B) The inflammatory reaction in both models is characterized by infiltrates of mononuclear cells surrounding the bile ducts (solid arrows), accompanied by single hepatocyte apoptosis/necrosis (solid arrowheads), fibrosis (open arrow, A), and hemosiderin-laden macrophages (open arrowhead, A). hematoxylin and eosin. (C) cd4t cell accumulation (purple signal) in liver of hu-SRC model is a feature of GvHD. immunohistochemistry (FFPE). original scans ×20. hu-PBL, human peripheral blood lymphocytes; hu-SRC, human stem repopulating cell.
New Technologies for Advanced Phenotyping and Analysis of HIS Models
Flow cytometry, which uses fluorescent markers to identify cells, is a convenient, cost-effective method for evaluating human cell engraftment in HIS mice. Peripheral blood, spleen, BM, and other tissues can easily be processed to analyze percentages of murine and human CD45+ cells. This can be extended to evaluate other human immune subsets as T cells (CD3, CD4, CD8), B cells (CD19), macrophages (CD68), and neutrophils (CD15). 69,70 Flow cytometry technology has advanced in recent years, with capabilities to measure an increasing number of parameters. New flow cytometers such as the BD FACSymphony system allows measurement of up to 50 different parameters on a single cell. To complete and validate the characterization of human immune reconstitution by flow cytometry, immunohistochemistry (IHC) offers spatial context and histopathology to better understand tissue homing of human cells and identify instances of GvHD, that is, inflammatory lesions dominated by T cells (CD4+ mainly) and macrophages, which must be considered in data interpretation. 71 –73
Despite technological advances, the evaluation of human immune cells by flow cytometry and IHC is limited by technical constraints. Most flow cytometers are limited to 12-18 parameters per single sample and issues with spectral overlap make analysis difficult. Furthermore, the possibility of multiplexing on IHC is even lower (Table 2). To properly describe and understand the complexity of these mouse models, new high dimensional parameter analysis tools are essential.
Comparison of Technologies for Analyzing HIS Mouse Models.
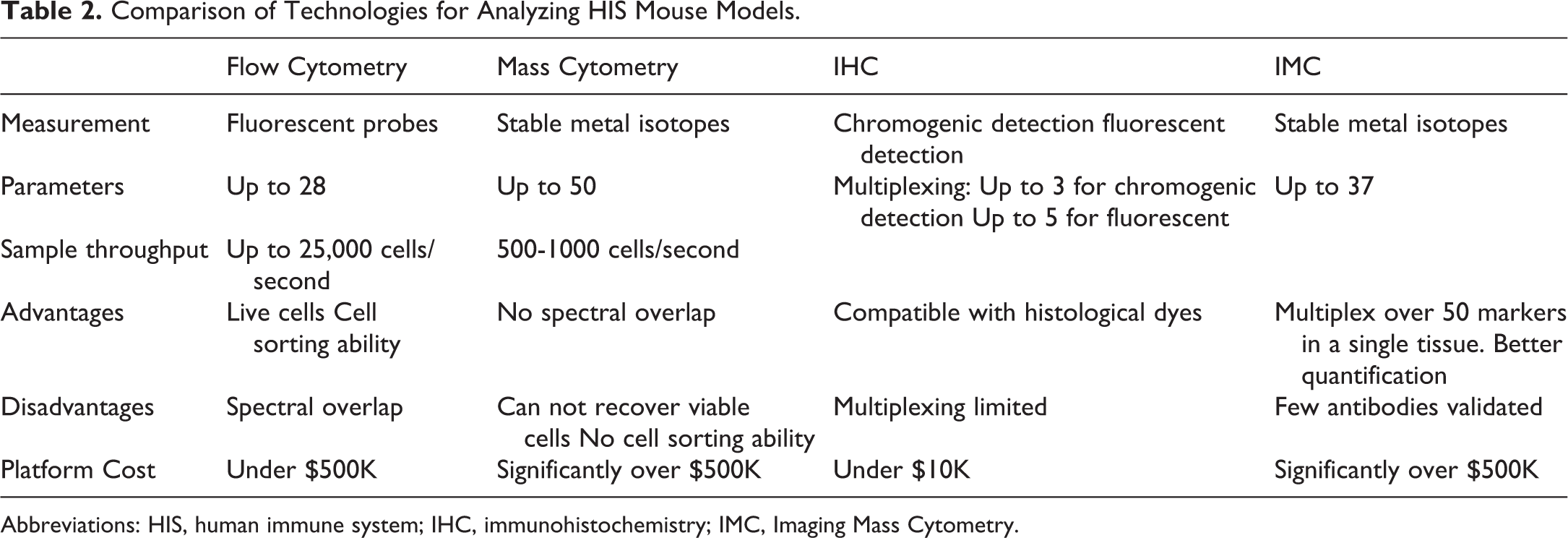
Abbreviations: HIS, human immune system; IHC, immunohistochemistry; IMC, Imaging Mass Cytometry.
A new phenotyping platform has been developed that couples flow cytometry with mass spectrometry known as mass cytometry. Mass cytometry offers single-cell analysis of up to 50 simultaneous parameters without spectral overlap. 74,75 Cell surface and intracellular markers are coupled with stable metal isotopes, which are identified by mass through time-of-flight (TOF) and linked to each single cell by a cell-ID incorporated before acquisition. Many of the antibody-metal isotope pairs are available and customizable from Fluidigm (South San Francisco, California).
Mass cytometry has become a popular tool for deep immune profiling across innate 76 –78 and adaptive immune subsets in humans. 79 –81 More recently, Herndler-Brandstetter et al (2017) performed deep immunophenotyping using 33 parameter mass cytometry of NK cells engrafted in SRG-15 HIS mice. 19 This supports the power and future scope of using mass cytometry to phenotype HIS mice.
Imaging Mass Cytometry (IMC) performed on the Hyperion Imaging System using metal-tagged antibodies empowers simultaneous imaging of up to 37 protein markers at a time. 82 Imaging Mass Cytometry combines a precisely directed laser beam focused on 1 µm tissue section to collect biological samples stained with metal-tagged antibodies and directs these tags for analysis by cyTOF technology described above, while preserving the information in tissue architecture and cell morphology (Figure 3). This can be done on fresh-frozen and formalin fixed paraffin embedded tissue sections. 83,84
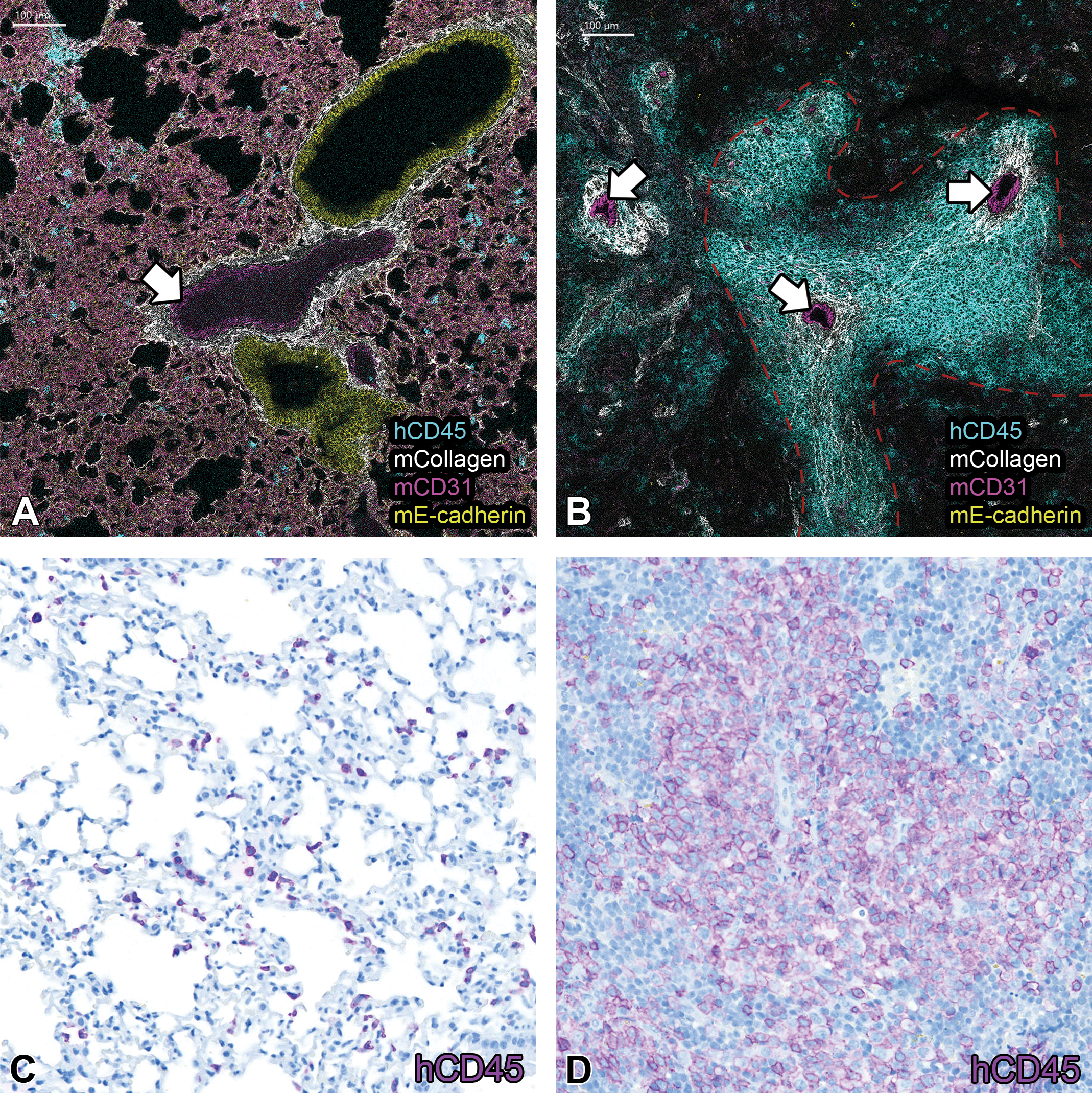
(A) Human cd45 infiltration into the lung in the hu-PBL model shown by IMC (fresh-frozen). White arrow indicates cd31+ blood vessel in the lung. (B) Human cd45 infiltration into the spleen of the hu-PBL model shown by IMC (fresh-frozen). White arrows indicate CD31+ blood vessel in the spleen. Red dotted line indicates aggregates of human CD45+ cells consistent with PALS in the white pulp and surrounding the blood vessels in the spleen. (C) Human cd45 infiltration into the lung of the hu-PBL model shown by IHC (FFPE), consistent with IMC analysis. (D) Human cd45 infiltration into the spleen of the hu-PBL model shown by IHC (FFPE), consistent with IMC analysis. IHC indicates immunohistochemistry; IMC, imaging mass cytometry.
In addition to mass cytometry, single-cell transcriptomics has led to new insights into the immune system. A combination of phenotypical (mass cytometry) and transcriptional (single cell RNA-sequencing) profiling have been used by Winkels et al (2018) to define an atlas of the immune repertoire in a murine atherosclerosis model, revealing new immunologic mechanisms and cell-type-specific pathways. 85
The high throughput capabilities of multi-parameter flow cytometry, mass cytometry, single cell transcriptomics, and IMC allows powerful high content analysis. T-distributed stochastic neighboring embedding (tSNE), spade, and citrus algorithms offer visualization of multidimensional data which can quickly identify subtle changes in immune populations. Several platforms can be used for this analysis, including Cytobank, 86 FlowJo, R-studio, and MATLAB. Furthermore, Fluidigm have coupled their human immune monitoring kits with an automated gating software which uses probability state modeling and Cen-se algorithms to effectively and rapidly analyze 25 key immune subsets. In addition to the informative images acquired by IMC, quantitative analysis can be performed using various image analysis software such as Halo, Cell Profiler, and HistoCAT. The development of a multimodal approach with mass cytometry, IMC, and single-cell RNA-sequencing coupled with high dimensional analysis platforms supports next generation analysis of HIS mouse models with great implications for their use in preclinical studies. Some of the promising applications of HIS mouse models in preclinical immuno-oncology studies are discussed below.
Preclinical Applications of HIS Mouse Models
Using HIS Models for Preclinical Toxicology
The detrimental impact of cytotoxic and immunomodulatory drugs on the HIS has long been a cause for concern with regard to the safety profile of therapeutic agents. Traditionally, toxicity testing of new small molecule drug candidates is undertaken in healthy preclinical species in clean housing facilities. Thus, although the drug candidate is pharmacologically active in the chosen toxicology species, translation of the pathway of interest and the immune context of the human patient population can result in adverse events manifesting in the clinic that were not evident preclinically. For biologics, preclinical testing is further limited by the high specificity of the drug product, so that the effect on the immune system of lower mammalian species may not recapitulate the likely outcome in humans. This was most dramatically illustrated in the phase 1 clinical trial for TGN1412, a novel monoclonal antibody super agonist of the CD28T cell costimulatory molecule. Six healthy volunteers had life-threatening adverse events following a single dose of this T-cell activator. Events were later attributed to a cytokine storm event within the first 4 hours following dosing. 87 The preclinical assessments of this monoclonal antibody, including in vivo nonhuman primate studies, had not indicated signs of proinflammatory effects or toxicities as indicated in the investigator’s brochure 88 and thus the severe adverse events were not predicted during drug development. A potential solution to this challenge has been for the tests to be routinely conducted in nonhuman primates. However, this approach does not fully address interspecies differences and is additionally associated with significant ethical and economic considerations. 89
Reconstitution of immunocompromised mice with a HIS has the potential to provide a step change in the prediction and translation of adverse events. The HIS mouse models have been used successfully to assess BM toxicity and haematotoxicity of cytotoxic oncology treatments. 90 More recently, the opportunities afforded to novel drug development by HIS mouse models has been explored further, particularly with regard to human-specific drug modalities where preclinical models are limited. The HIS mice have been utilized to investigate the efficacy of human checkpoint inhibition 91 and the common adverse events observed with chimeric antigen receptor (CAR) T therapies.
In humanized mice reconstituted with cord blood-derived CD34+ cells and transplanted with tumor tissue from established patient-derived xenograft (PDX) models, treatment with anti-PD1 antibodies increased the number of tumor-infiltrating IFNγ-producing T cells and decreased T-regulatory cell numbers. 91 This immune activation resulted in tumor growth inhibition. Furthermore, HIS mouse models have provided mechanistic understanding for the cytokine release and neurotoxicity which occur with CAR T therapies. Investigations with HIS mice with a high leukemic burden have defined that monocyte-derived IL-6 is responsible for the cytokine-release syndrome observed with these therapies, while IL-1 appears linked to the life-threatening neurotoxicity. The HIS studies have enabled mitigation strategies to be identified and thus providing opportunities to mitigate these adverse events. 92 Indeed, there are exciting opportunities for HIS mouse models to provide a translatable, preclinical safety assessment of cell therapy approaches, where standard toxicology testing is unsuitable.
An area of drug safety that is particularly challenging to model preclinically are the immune-related adverse events (irAEs) observed with immune-oncology agents, such as checkpoint inhibitors. 93 These adverse events do not manifest reproducibly in standard toxicological testing. In particular, combinations of checkpoint inhibitors can result in exacerbations of toxicity in the clinic, which would greatly benefit from more accurate preclinical modeling. 93 Human immune system mouse models may provide a bridge to translate preclinical testing to the clinic, particularly given the opportunities to humanize mice with cells and/or human tissue fragments from patients to replicate the diseased state. For example, reconstitution of immunocompromised mice expressing human MHC class II, reconstituted with cells from a human donor deficient in FOXP3 function due to a single point polymorphism resulted in manifestation of autoimmunity pathologies mimicking those noted in humans with immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome. 94 These animals developed symptoms similar to those noted in IPEX individuals, with increased multiorgan inflammatory infiltrates, evidence of autoantibodies, and increased mortality. This promising finding raises the prospect that the HIS mouse model might, with optimization and further development, be able to predict adverse immune events observed in the clinic. In particular, HIS mice may be predictive for preclinical tumor studies and adoptive cell therapy (ACT) models which are discussed below.
Using HIS Mouse Models for Tumor Studies
Traditional mouse models do not recapitulate the heterogeneity and complexity of the original tumor and often lack predictive power, with over 80% of oncology drugs failing clinical trials. 95,96 Patient-derived xenograft models have been shown to better retain tumor heterogeneity and have been used to study disease stabilization, progression and response to chemotherapy treatments in a range of tumor types. 97 –102 However, one major limitation of this model is the use of immunocompromised mice, hindering evaluation of tumor immune interactions and immunotherapies. Immunotherapies aim to treat cancer indirectly through reinforcing the anti-tumor immune response and can be administered in the form of vaccines, ACT, and immune checkpoint inhibitors. Cytotoxic T-Lymphocyte-Associated Protein 4 (CTLA-4), Programmed Cell Death Protein 1 (PD-1), and Programmed Death Ligand 1 (PD-L1) are common targets for immunotherapies and have shown promising yet highly variable response rates. 103 For example, response rates to PD-1/PD-L1 targeted immunotherapies, such as pembrolizumab and atelizumab, is seen in only 20% to 30% of patients despite demonstrated efficacy in a variety of tumor types. 104 Immune-related adverse events such as colitis, rashes pneumonitis and neuropathy present as a major challenge for immunotherapy. 105 For instance, Robert et al 106 found that metastatic melanoma patients treated with Ipilimumab (anti-CTLA-4) showed an 8.6% increase in survival over 3 years, however 56.3% of these patients developed grade 3 to 4 irAEs. These irAEs are thought to be linked inflammatory tissue damage, brought about through nonspecific activation of the immune system. Furthermore, it has been shown that many patients receiving immune checkpoint inhibition have gone on to present clinical manifestations of rheumatic diseases. These include inflammatory arthritis, 105 inflammatory myopathy, 107 sicca syndrome, 108 and lupus nephritis. 109 Findings such as these highlight the need for well-designed preclinical models that can accurately assess safety and efficacy of immunotherapies at varying doses, schedules, and combinations.
The HIS mouse models have been developed to more accurately depict the tumor microenvironment evolution and progression. As can be seen in Figure 4, HIS PDX (HuPDX) models are typically established through humanization of mice, as described earlier, followed by implantation of early passage xenograft tissue. HuPDX models have been applied to assess clinically approved immunotherapies in a variety of tumor types. 110 A key confounding factor is that in these studies the tumor and immune cells are obtained from different donors, thus overlaying an allogeneic immune response which can complicate interpretations of outcomes. Nonetheless, these models can be very informative. For example, Rosato et al 111 evaluated nivolumab (anti-PD-1) in a HIS model of triple negative breast cancer finding a positive correlation between PD-L1 expression and treatment response, similar to that seen in patients. 112 The HIS models also show great potential in assessing treatment toxicity. For examples, HuPDX models of hepatocellular carcinoma, have been used to assess organ damage linked to ipilimumab, verifying toxicity in the liver, lung, and kidneys. 113 The HIS models have also proved valuable in modeling drug refractory tumors and identifying effector mechanisms involved in treatment resistance. 114 However, the short lifespan of HIS mice makes these models ill-suited for longitudinal experiments as they do not truly reflect clinical scenarios such as drug discontinuation and reduction. Furthermore, it is often not feasible to reconstitute mice with autologous patient derived lymphocytes, especially in large-scale preclinical studies and many models rely on partial HLA-matched HSCs for reconstitution. Despite these limitations, HIS mouse models represent a novel and sophisticated tool in immuno-oncology research that will continue to evolve over time.
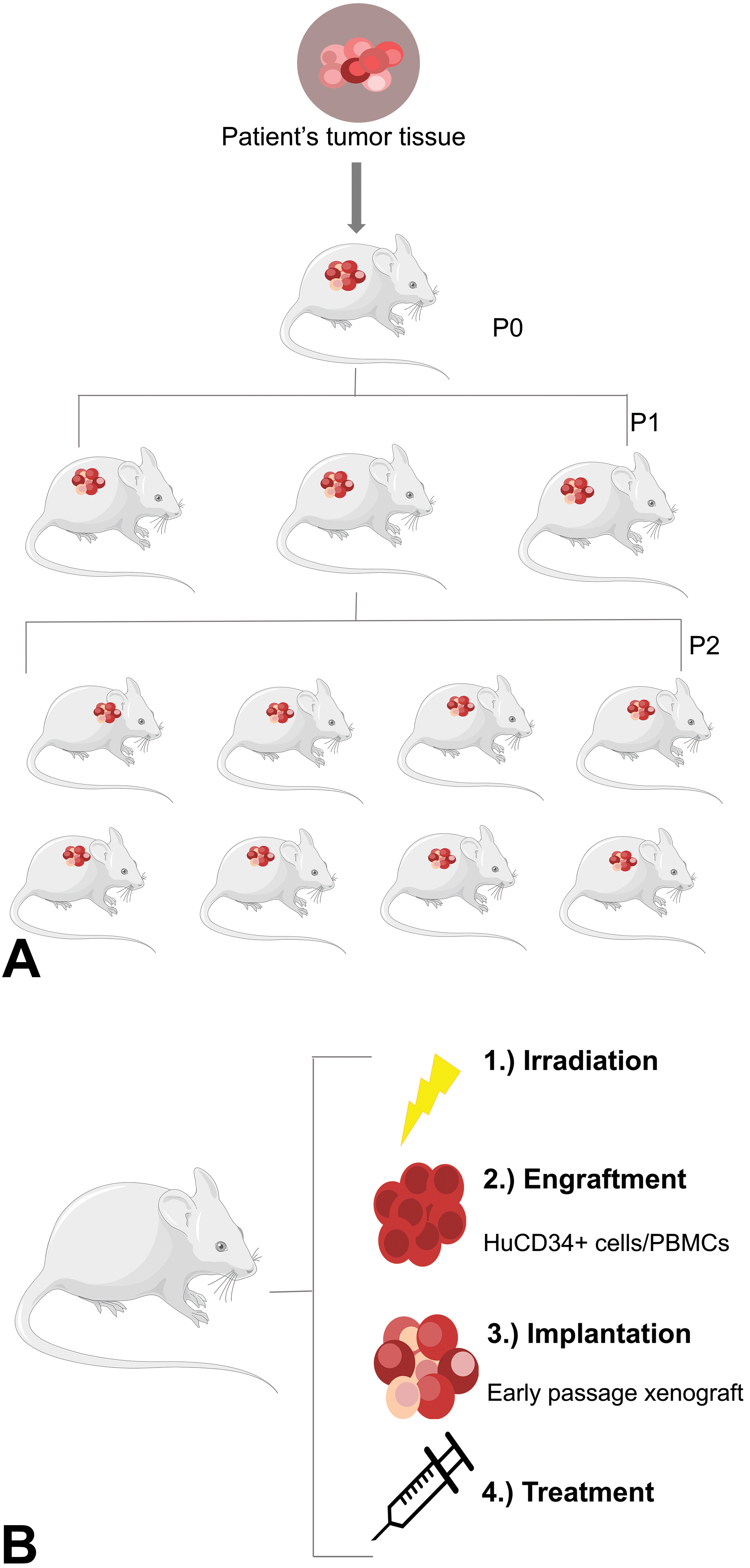
(A) Establishing a PDX line: Small fragments (∼2 mm3) of recently resected primary tumor tissue is implanted into immunodeficient mice with no in vitro manipulation. the xenograft is grown in vivo (∼1000 mm3) sectioned and reimplanted to create experimental cohorts (P2). samples can be taken for characterization between passages. (B) Humanized PDX model: peripheral blood mononuclear cells (PBMCS) or hu-cd34+ cells (derived from peripheral blood stem cells, bone marrow, fetal liver, or umbilical cord blood) are engrafted into irradiated immunodeficient mice. Early passage PDXS are then implanted. this model can be used for pharmacological evaluation of immunotherapies.
Using HIS Mouse Models for ACT
Adoptive cell therapy, such as CAR-T cell therapy, has shown great efficacy in the treatment of hematological cancers, with remission in up to 90% of cases. 115 Two T-cell therapies based on a CAR recognizing CD19 (CAR19) have been approved by US Food and Drug Administration (Kymriah and Yescarta). They both direct autologous T cells to CD19-expressing tumor cells in acute lymphoblastic leukemia and B cell lymphomas (B-ALL). 116,117
Both in vivo and in vitro models have been applied to further understand the underlying mechanisms behind CAR-T cell therapy and increase its clinical relevance. The xenograft mouse models have contributed to the development of better next-generation CARs with different signaling moieties 118 –122 and “on-target/off-tumor” toxicity, 123,124 whereas the syngeneic mouse models have been instrumental in understanding the interplay between the tumors and the CAR T-cells in the context of an intact host immune system 125 –127 and long-term engraftment of CAR T-cells. 128 The major disadvantage of these systems, however, is the lack of translatability to clinical outcomes, which is due to inability of these systems to mimic faithfully the patient’s immune system or to the absence of other immune cells which contribute to the efficacy, persistence, and safety of CAR T-cell therapies. Several preclinical and clinical studies are now ongoing to translate CAR T-cell efficacy to solid tumors; however, this is proving less successful due to several factors, including inefficient trafficking of CAR T cells into solid tumors and the presence of immuno-suppressive tumor microenvironments. 129
Human immune system mice engrafted with tumor and CAR T-cells from the same donor, should provide a more clinically relevant model for cancers. So far, CAR-T cell therapy has been successfully modeled in HIS mice, recapitulating the posttreatment immune changes observed clinically. 130 –132 Recently, a HIS mouse model with a functional HIS and an autologous tumor has been used to study CAR19 T-cell therapy for B-ALL pre-clinically. 133 This strategy avoided allogeneic responses by using fetal CD34+ cells pooled from several donors to generate all the required human cells, and it recapitulated most of the clinical signs of CAR T-cell therapies. The question remains whether next-generation models will recapitulate mechanisms for tumor resistance and development of immune memory. Moreover, toxicity associated with cytokine release syndrome (CRS) observed in clinical trials of immunotherapies including CAR T-cells was not observed in these mice which may be due to undetectable levels of human IL-6, a primary driving force for CRS. 134 As this is a key parameter in assessing the safety of CAR T-cell therapies, it is vital to predict CRS in a preclinical manner.
Together with the success for the CAR19 T-cell therapies, CRISPR technology has the potential to increase the efficacy and safety of reprogrammed T cells. Several publications have shown that knock-out of immune checkpoints (eg, PD1 135 ) or insertion of CAR gene into the TRAC locus, so that its expression is controlled by the endogenous promoter, 136 enhanced edited T-cell potency and clearance of tumor xenografts. To our knowledge, pre-clinical studies have only been conducted in immunodeficient mouse models in which the full potential and safety of CRISPR-edited T cells cannot be fully evaluated. This warrants further investigations into the use of HIS mice as a preclinical model for T-cell therapies.
Conclusions
The HIS mouse platforms are useful for investigating human immune responses in an experimental setting and may have a part to play in the safety and efficacy evaluation of new immunotherapeutics, where no other relevant preclinical animal model exists. With advancements in new immunodeficient mouse strains and novel technologies to fully characterize these platforms, the expanding scope and application of HIS mice is emerging. Once fully characterized, HIS mice may have the potential to be an informative preclinical animal model for safety and efficacy evaluation. However, HIS mice also have several limitations that must also be fully understood, and caveats applied where needed. For the efficacy evaluation of immunotherapies, huPDX models may offer a more representative human tumor microenvironment that better mimics the immune context in the patient. The HIS mice have already been employed to investigate the safety and efficacy of adoptive cell and gene edited T cell therapies. Human immune system mice represent an exciting opportunity in the field of immunotherapy and we can expect to see a surge in our knowledge around these models in the coming years.
Footnotes
Acknowledgments
The authors would like to acknowledge Stephanie Ling from CPSS, BioPharmaceuticals R&D, AstraZeneca, Cambridge, United Kingdom for her contribution to IMC images used in this review. Secondly, the authors Michelle Curran and Ardi Liaunardy are fellows of the AstraZeneca postdoc programme. This review was requested, endorsed and sponsored by the British Society of Toxicological Pathology (BSTP).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.