
Abstract
Despite—or perhaps because of—the rapid expansion of interest in stem cell–derived cellular therapy products, relatively few guidelines have been published to assist in the design of scientifically sound preclinical studies. The field is complex and wide ranging, and of necessity regulators tend to treat each project on a case by case basis. One of the core tenets remains the need to retain all tissues from the study, thereby allowing for further analysis of tissues should unexpected effects be seen in clinical studies; attempts to comply with this may result in an unmanageable financial burden. Judicious input from the pathologist at the earliest stages of study design may not only improve the scientific integrity of the study but also help to mitigate some of the cost. Careful animal selection, the development of robust cell markers, and justifiable triage of tissues based on phased tissue examination can all be discussed with the regulatory authorities at pre-pre-investigational new drug (IND) and pre-IND meetings to achieve optimal study design.
Introduction
Cellular therapeutics, along with medical devices and tissue engineering, form the relatively recent field of regenerative medicine (Jayo et al. 2008). All are aimed at restoring, or replacing, the structure and function of damaged organs and so curing previously untreatable injury or disease. In the case of cell-based therapy, this is achieved by introducing viable cells into the diseased tissue.
Stem Cells—A Primer
Stem cell populations are composed of undifferentiated cells that retain the ability to reproduce themselves even after long periods of inactivity. Under certain physiologic or experimental conditions, these cells also have the potential to differentiate into tissue- or organ-specific cells with specialist properties.
Stem cells exhibit both asymmetric and symmetric division, thereby maintaining the stem cell population while also generating specialized cells. Thus, stem cells can continually reproduce, or they can produce a daughter cell which is more specialized—a progenitor cell. Progenitor cells only replicate symmetrically, producing 2 daughter progenitor cells. Alternatively, they can develop to produce a mature cell type.
Only the zygote and morula retain the capacity to produce placental cell lines in addition to all 3 germ cell layers; the cells of these tissues are considered to be totipotent. Cells from the inner cell mass of the blastocyst are pluripotent and can produce any of the 3 germ layers, while stem cells in the fetus, and postnatal progenitor cells, are considered multipotent and are restricted to the production of multiple, but limited, cell types—for example, the neural stem cell can produce neurons, astrocytes, and oligodendroglial cells.
Derivation of Stem Cells
The derivation of naturally occurring human pluripotent stem cells—or human embryonic stem cells (hESCs)—has been dogged by controversy. The dissection and disaggregation of a blastocyst clearly destroys the embryo. However, in 2006, researchers developed an “embryo-safe” method of harvesting hESCs by using a single cell biopsy technique from an 8-cell morula—a technique commonly used to screen for genetic diseases prior to embryo implantation during in vitro fertilization (Klimanskaya et al. 2006).
So-called adult stem cells, also referred to as tissue-derived or resident stem cells, have been identified in numerous tissues and organs of the body: hematopoietic stem cells, oval cells of the liver (Yovchev et al. 2008), cells deep within the intestinal crypts (Barker, van Oudenaarden, and Clevers 2012), cells in the epithelium of the corneal limbus (Dua and Azuara-Blanco 2000), and cells within the hair follicle bulge (Morris et al. 2004), are all sites of stem cells. There are even stem cell populations in the brain (Sanai et al. 2004) and heart (Leri, Kajstura, and Anversa 2005). Some adult stem cells are easier to harvest than others—the placenta and urine are generally treated as clinical waste, but both can provide sources of adult stem cells (Bharadwaj et al. 2013). So too can the pulp of deciduous teeth if they are extracted before they lose their blood supply (Miura et al. 2003).
Induced pluripotent stem cells (iPSCs) are produced by the activation or suppression of certain genes, critical for the expression of pluripotency. If the gene Oct-3/4 is suppressed in blastomeres or embryonic stem cells (ESCs), the cells will produce cysts of trophoblastic cells similar to the outer capsule of the blastocyst (Niwa, Miyazaki, and Smith 2000). The Sox family of genes is also found in multipotent and unipotent cells, and induction cannot occur without the activation of at least one of these genes (Kuroda et al. 2005). Other genes increase induction efficiency, but are not essential. Multiple methodologies have been successfully used to activate these genes, and the resulting cells have similar biological properties and growth characteristics to ESCs, including long-term self-renewal and the ability to produce other, more mature cell types. Unfortunately, such cells may also retain some less desirable characteristics, such as the ability to develop into teratomas. Critics have also said that these cells may have a tendency to revert to their original cell type with time (Heng et al. 2009). Supporters argue that stem cell therapies generated from the patient’s own cells are unlikely to be rejected.
Historical Perspective
The first cell-based therapies were derived from animal tissues, and records of such treatments exist dating back to the Egyptians, more than 3,000 years ago. However, despite the continuing presence of clinics offering “fresh cell therapy,” this form of cell therapy is now widely shunned by mainstream medicine. Attention has shifted instead to human-derived products—first, blood transfusion, then organ transplantation, and now stem cell transplantation.
The first human–human cell therapy was a blood transfusion performed by James Blundell (1828) in London in the 1820s. In 1954, the first successful organ transplant was performed when a kidney was transplanted into the donor’s identical twin (Merrill et al. 1956), and this was followed only a couple of years later by the first bone marrow transplant between identical twins (Thomas et al. 1959). In both these cases, the problem of rejection was minimized by the identical genetic profile of donor and recipient.
The term “stem cell” was first used in 1908, when the Russian scientist, Alexander Maksimov presented a paper on the putative existence of self-renewing precursor cells in the bone marrow (Igor 2000). It would not be until 1963 that his hypothesis was proven (Becker, McCulloch, and Till 1963), but within 5 years of this work the first successful allogeneic bone marrow transplant between 2 human leukocyte antigen (HLA)-matched siblings was performed in Minnesota (Gatti et al. 1968), and in 1973, an HLA-matched donor in Denmark provided marrow for an unrelated child in New York (Kharrazi and Rizk 2002). Another 8 years would pass before ESCs were first successfully derived from mouse embryos (Evans and Kaufman 1981).
Stem cells derived from placental cord blood (PCB) were found to hold several advantages over bone marrow stem cells: they carry a lower risk of graft versus host disease (GVH) because the stem cells are less developed; they can be cryogenically stored, allowing the possibility of “banking” them at birth for possible later use; and only 100 ml of PCB is required to perform a transplant (Rubinstein et al. 1995). However, engraftment of stem cells from PCB does take longer than marrow engraftment. PCB transplant was first performed in 1988, between an HLA-identical sister and brother (Gluckman et al. 1989).
Although there has been considerable research using adult stem cells in this millennium, the induction of pluripotency was first achieved in 2006 (Takahashi et al. 2007; Yu et al. 2007)—only 7 years ago—and it is only 4 years since the first clinical trials using ESC-derived products were approved by the Food and Drug Administration (FDA; Schwartz et al. 2012). The pace continues to quicken, with 2013 seeing both the development of a technique to induce pluripotency via chemical means (Hou et al. 2013) and the announcement of the first functional liver tissue to be grown from iPSCs (Takebe et al. 2013). In Japan, the first patient to receive autologous iPSCs on a clinical trial was implanted with a sheet of induced retinal pigment epithelial cells in September 2014, in an effort to treat age-related macular degeneration (Cyranoski 2014).
Preclinical Study Design for Cellular Therapeutic Agents—The Pathologist’s Contribution
Histopathological evaluation accounts for a significant portion of the cost in preclinical studies of cellular therapeutics. Pathologists are involved in the evaluation of cell biodistribution, to illustrate the in vivo distribution of the cells and determine their engraftment and/or persistence within the host; safety, to determine whether the cells are likely to cause harm; and efficacy, to determine whether the cells injected produce their intended effect.
Involvement of pathologists in early stages of study design is important for optimal tissue collection conditions during necropsy, choice of tissues evaluated, method of tissue evaluation, and the identification of key study end points. Input on several parameters in the study design, such as species and strain selection, development of robust and specific cell markers, and triaging of tissue selection and examination on a group-specific and time point–specific basis can significantly impact the costs and feasibility of otherwise challenging studies without compromising the quality and integrity of study outcomes.
Species Selection
The behavior of stem cells, and stem-like cells, is strongly influenced by local environmental factors, and accurate administration to the intended target site is crucial for proper assessment of cell safety (Baker and Jackman 2014, poster). Xenogeneic implantation of the intended clinical grade cell therapy test article, versus autologous implantation of clinically relevant cell types, can markedly influence the reliability and translatability of study outcome. Consequently, optimal species and strain selection increase the potential for the use of the most appropriate systems for modeling particular human disease conditions (Table 1).
Preclinical stem cell study design.
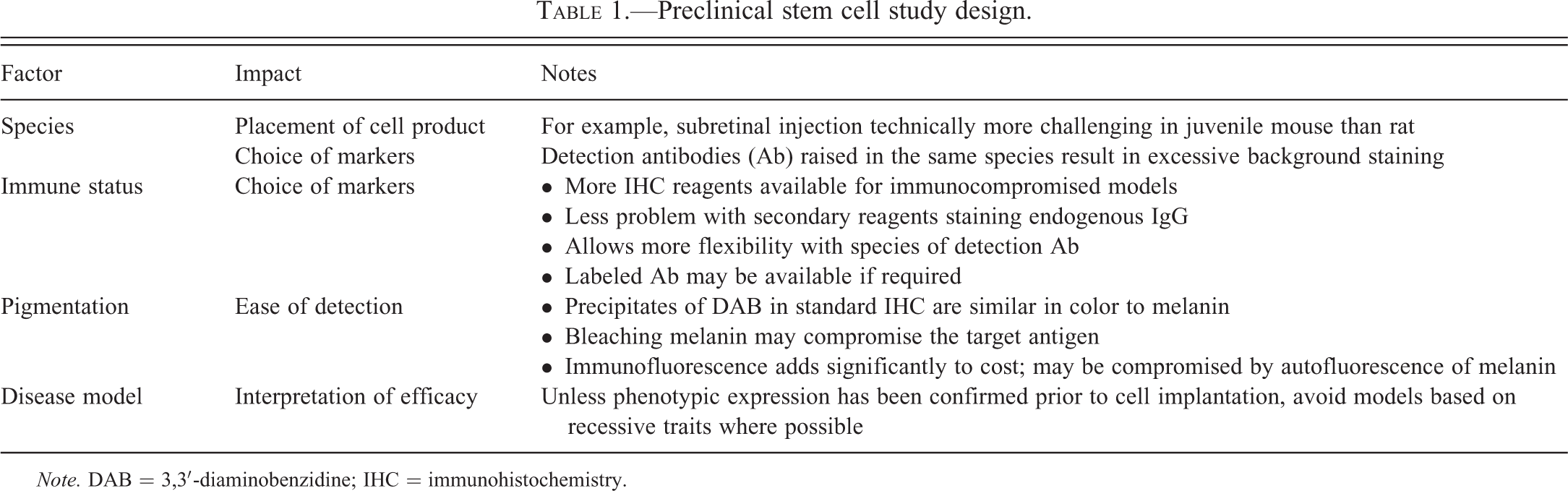
Note. DAB = 3,3′-diaminobenzidine; IHC = immunohistochemistry.
Larger animal species, such as dogs and pigs, provide greater accuracy of cell placement over a mouse model. Similarly, the use of an immunocompromised animal model reduces the likelihood of rejection of the cells and facilitates the development of more robust cell detection methods, with less background, nonspecific staining. Immunohistochemical detection of cells in tissue sections may prove more reliable in albino strains when using 3,3′-diaminobenzidine (DAB) substrate for color detection; target sites are unpigmented, removing any need to bleach naturally occurring melanin pigment—a process that may interfere with immunostaining of critical markers and with data interpretation.
A major hurdle in the choice of larger animal species is the limited availability of species-specific reagents.
The choice of healthy animals versus animal model of disease is another consideration. While traditional toxicology studies focus on the use of healthy animals, the dynamic nature of cell therapy encourages the examination of product safety in combination with efficacy studies, using animal models of disease. Such animal modeling provides a better definition of the activity–toxicity and risk–benefit ratios, and may indicate biomarkers of safety and efficacy translatable to the human condition. Consequently, rigorous validation of the animal model of disease is necessary in such a scenario. If the disease trait is linked to an autosomal recessive gene, only a proportion of the animals will express the condition; unless the affected animals can be detected prior to dose administration, there is a risk of poor distribution of those animals across the groups. For example, retinal degeneration in the Royal College of Surgeons (RCS) rat is due to a defect in the Merkt gene, which results in loss of phagocytic activity by the retinal pigment epithelium (RPE) and subsequent loss of photoreceptors. This condition is uniformly and predictably expressed with onset at postnatal day 21 and complete loss of photoreceptors by postnatal day 240. In contrast, the NIH-III mouse exhibits retinal degeneration only in individuals homozygous for the Pde6brd1 (rd1) mutation; affected animals lose all rods by 35 days of age and can be recognized by fundic examination as early as day 15. Heterozygotes show no retinal degeneration.
Other factors important in the choice of animal model include organ and tissue size, ideally permitting administration of the intended human dose levels using the targeted delivery device and location, feasibility of statistically sound group sizes, and the availability of animal model autologous cells that are analogous to the intended human cellular product. From a regulatory perspective, the FDA does not require the “standard” animal selections applied to small-molecule drugs, as long as scientific justification for the choice of animal species and model is provided (FDA Cellular and Gene Therapy Guidance 2013).
Robust Detection Methods
Evaluation of complex stem cell biology in vivo requires careful method development and the identification of robust and sensitive markers. Studies in animal models and humans have shown significant cell death after transplantation, with limited engraftment and differentiation of transplanted stem cells. So while it may be possible to detect a bolus of administered cells within a tissue using hematoxylin & eosin (HE)-stained tissue sections, detection of small numbers of migrating cells using HE alone may not be feasible. This may be further complicated by the proposed mode of action of stem cells; the stem cells, or derived progenitor or differentiated cells, may exert their function through direct tissue regeneration or through the activation of endogenous stem and progenitor cells reprogramming in situ. Determination of the latter may require consideration of endogenous biomarkers of safety and efficacy, such as enhanced expression of targeted endogenous growth factors, or may result in off-target cellular toxicities associated with cellular implantation. Immunohistochemical (IHC) staining, using labeled antibodies, can aid in the detection of administered cells in tissue sections, determine whether or not the cells proliferate and/or persist, and can demonstrate the cells’ ability to differentiate—into the intended cell type, or into a nonintended cell.
Various markers, including human nuclear antigen and human mitochondrial antigen, have been used to demonstrate human origin; different cell lines react better with some than with others. Proliferating cell nuclear antigen (PCNA) or ki67 may be used to look for evidence of proliferation. On the other hand, assessing cell differentiation can be challenging due to limitations when developing a staining method that is species-specific for the human cells with antibodies compatible with the research model species.
Integration of molecular markers, such as gene expression by polymerase chain reaction (PCR), and endogenous protein interactions and functions at molecular, biochemical, cellular, and tissue levels are current technologies that aim to improve the safety and efficacy evaluation of stem cells in a more comprehensive fashion. This approach provides a more thorough tissue biodistribution screening, allowing for the evaluation of larger tissue samples, particularly in nontarget tissues.
Inherent to stem cells is their ability to acquire chromosomal aberrations during expansion in culture. Hence, markers of transcriptional activation, proliferation, and differentiation should also be further evaluated in vivo. The evaluation of endogenous protein interactions and functions at molecular, biochemical, cellular, and tissue levels are current technologies that are aiming to improve the safety and efficacy evaluation of stem cells.
As indicated earlier, the choice of an albino species may aid in DAB detection in otherwise naturally pigmented target tissues, such as retina, and the choice of a mouse model, or immunocompromised animal species, may facilitate reagent selection and result in less background, nonspecific staining. Another alternative is the use of immunofluorescence to overcome background staining. However, the instability and transient nature of fluorochromes necessitates image capture and photographic recording of all slides for permanent recordkeeping; a potentially cost-prohibitive factor in a large-scale Good Laboratory Practice (GLP)-compliant preclinical study. Conversely, multicolor spectral imaging of multiply marked histochemically or fluorescently stained slides may prove critical in the early proof-of-concept small-scale studies, allowing complex tissue analysis, colocalization, and subcellular localization, and evaluation of implanted cell–endogenous marker interactions. Having demonstrated colocalization in these early studies, a case can then be made for comparing the location of different markers in adjacent serial sections during the safety assessment studies.
Potential tumorigenicity is a major public concern regarding stem cell–derived therapies. Given their pluripotent nature, tumors derived from administered cells have the potential to develop a phenotype very different from the original cells. To determine whether a tumor is derived from the administered cells or is a spontaneous tumor, it is necessary to look for markers specific to the administered cell line that will remain constant in the face of phenotypic variation; in this regard, species-specific markers, such as human mitochondrial antigen or human nuclear antigen, may prove invaluable.
Cell Scaffolds
Tissue engineering introduced the physical microenvironment into the formulation of stem cell products and has demonstrated a pivotal role in improving exogenous or endogenous stem cell regenerative capacity. Such modification includes 3-dimensional biodegradable scaffolds, the addition of “support cells,” and/or other bioactive active molecules such as bone morphogenetic protein (BMP). The multicomponent nature of these products results in a more complex category of cellular/device combination products that require comprehensive evaluation of each component separately or contextually together. Further role delineation may be necessary in the event of detecting component-specific hazard/toxicity. Graft versus host reactions, biocompatibility of the scaffold material to both the host and the combined cellular component, and immunogenicity of the final combination product are crucial parameters in the safety evaluation tissue-engineered combination products. Additional study design and technical considerations may be required or modified depending on the nature of the scaffold material involved, such as the evaluation of scaffold degradation and modification of tissue fixatives and embedding medium during tissue analysis.
Tissue Triage
Tissue archiving in large-scale GLP-compliant studies is extensive and cumbersome. The costs of producing and archiving the material (wet tissues, formalin-fixed paraffin-embedded blocks, and tissue slides) increase with progression from wet tissues to stained or unstained tissue slides. Maintenance of unstained tissue sections is further complicated by the need to store such slides in slotted slide boxes, increasing the space required for archiving. Tissue triaging and the selection of appropriate and scientifically sound tissue collection and sectioning will consequently have a dramatic impact on the final feasibility of the study.
Tissue List
A tiered system of tissue selection can be designed by the route of administration (ROA), draining lymph nodes, anticipated product biodistribution, and hypothesized product’s mode of action. Table 2 provides an example of such a system.
Preclinical stem cell study design.
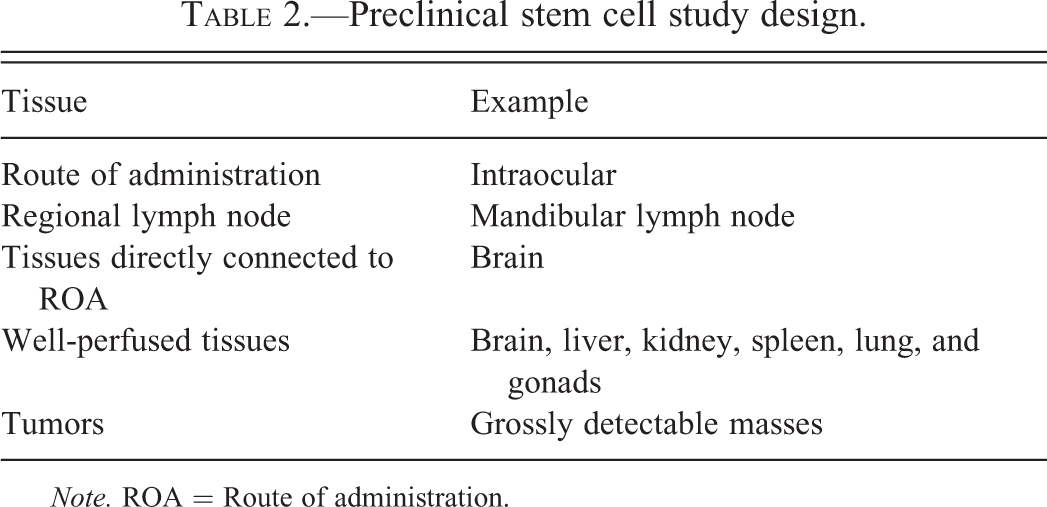
Note. ROA = Route of administration.
ROA and the associated draining lymph nodes are most likely to demonstrate efficacy and safety parameters. The potential for hematogenous spread demands the evaluation of well-perfused tissues such as the liver, spleen, and lung. Evaluation of specific connected and proximal tissues may be necessary, for example, the retina should be considered an extension of the optic nerve and brain. Gonads may be a consideration if reproductive toxicity is expected due to stem cell–released factors. Finally, any unusual masses should be screened to exclude the possibility of stem cell tumorigenicity.
Tissue Handling
The identification of small numbers of administered cells in “standard” 5-µm HE-stained sections can prove difficult, and searching for the systemic spread of a percentage of the administered cells in large volume tissues such as the liver is likely to prove even more challenging. Similarly, serial sectioning of an entire tissue in search of rare cells is impractical due to the demand to retain the intervening serial sections to avoid the permanent loss of tissue. Integration of stereology and proper tissue sampling in the study design can significantly facilitate proper tissue sampling and generating whole tissue inferences based on a smaller and more practical tissue sample. For example, serial tissue segments obtained at 1-mm intervals using stainless steel or acrylic tissue matrices and separately embedded into serially labeled blocks can be used to examine defined step sections in a single slide fashion with no loss of the intervening tissue, thereby allowing practical and cost-effective evaluation of the entire tissue examined.
Alternatively, integration of molecular tools (such as quantitative polymerase chain reaction [Q-PCR]) to screen a larger tissue volume of nontarget tissues for the presence of cells reduces the need for the examination of IHC-stained sections of the nontarget tissues.
Tissue Triage Based on Group Assignment
If no cells have been injected into a control group, tissue collection can be modified and minimized to include only sufficient tissue to demonstrate both the background staining pattern—for HE and for IHC markers—and the background pathology if we are using a disease model. The remaining tissue can be maintained in a more space- and cost-effective wet format or tissue blocks.
Use of Phased Tissue Examination
Nonpersisting implanted cells with transient kinetics are less likely to prove a long-term or permanent hazard in vivo. Tracking the disappearance of such cells in pilot studies may justify a reduced duration for later studies, and negative results from Q-PCR used to screen the nontarget tissues at 1 time point may be used to justify less rigorous examination of those tissues at the intermediate time points. While there may be additional cost incurred by processing and examining tissues at each time point, this can be more than rewarding if findings from an early time point can be used to justify a less aggressive sectioning protocol at later time points.
Conclusion
The field of regenerative medicine is continuously and rapidly evolving with the advancement of science. Stem cells, neo-organs, and combination regenerative medicine products are samples of such complex fields that require a comprehensive and integrated approach at the molecular, cellular, and tissue levels in the safety and efficacy evaluation of such products. Novel testing paradigms in risk assessment, development of efficacy biomarkers, and better understanding of the product mechanism of action will aid in the translatability of preclinical studies into clinical trials. Toxicologic pathologists possess training and expertise in integrative systems biology and preclinical study design and implementation. The involvement of toxicologic pathologists from the earliest phases of study design results in time-saving, cost-effective, scientifically sound, and translational-ready studies to evaluate cellular products. The pathologist can make invaluable contributions to species and strain selection, design of robust biomarkers, and identification of safety and efficacy end points in addition to method development, tissue processing, and tissue triage. Topics that remain elusive and provide opportunities for further pathologists’ contributions include the distinction of optimal tissue regeneration, definition of differentiation markers, evaluation of host immunological response, and better characterization of safety and efficacy end points.
Footnotes
Author Contribution
Julia F. M. Baker and Basel T. Assaf contributed to conception or design; Julia F. M. Baker drafted the manuscript; Basel T. Assaf critically revised the manuscript. Both authors gave final approval and agree to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.