
Abstract
The first effective immunosuppressive drug (ISD) was azathioprine, approved in 1968. Early experience with this drug suggested that patients might have an excess risk of tumors including lymphoma and skin tumors. Comparison among various registries has shown that the cumulative risk of tumors increases over time. The risk is additionally increased by the more intense immunosuppressive regimens needed for lung or heart-lung transplants. The link between immunosuppression and tumorigenesis was further reinforced by the high concordance of tumor types between transplant and HIV patients. The role of the immune system in tumor defense includes both direct tumor surveillance and immunity against oncogenic viruses. In transplant patients, at least two-thirds of the lymphomas are Epstein-Barr virus (EBV)–positive. Existing methods of testing for carcinogenicity are not considered adequate to identify the hazard of tumorigenesis due to these drugs. Research is ongoing in Food and Drug Administration laboratories and at collaborators’ laboratories to evaluate experimental systems that may have the ability to adequately identify this class of hazard. Initial work is on various model systems similar to EBV. These include the MHV-68 mouse model, lymphocryptovirus (LCV-1) in the cynomolgus monkey, and preliminary work with mice with humanized immune systems using EBV directly.
The testing of pharmaceuticals for their risk of causing cancer has a long and complex history (Diener 1983). The basic guidelines were developed in the 1940s and have been extended and modified a number of times in the intervening 60+ years. A basic assumption in this testing strategy is that the test material itself is able to invoke the formation of the tumor. For most compounds, this is a valid assumption; however, evidence from a variety of sources suggests that immunosuppression itself raises the cancer risk. Furthermore, this increased risk is largely independent of the cause of the immunosuppression. This is an important distinction because methods currently used to test for the risk of carcinogenicity assume that the test substance fits in the classical inducer/promoter paradigm. In the following sections, we will briefly review published data on the reports of cancer in association with immunosuppression by three different classes of causes.
Cancer and Immunosuppression by Genetic Defect
Primary genetic immunodeficiencies as a class have been linked with a very wide variety of tumor types. Approximately 15 different immunodeficiencies have been identified to have a reported excess tumor risk (Salavoura et al. 2008). A specific syndrome is typically limited to one or a few types of tumors. As would be expected with major disruptions in leukocyte homeostasis, a wide variety of lymphomas is observed. The incidence of proliferative disease can range from rare to as much as 30% of all patients (Salavoura et al. 2008). Studies of viral association are limited, but lymphoma associated with Epstein-Barr virus (EBV) or human herpes virus-8 (HHV-8) has been reported in selected cases, such as severe combined immunodeficiency disease or chronic variable immunodeficiency disease (Tran et al. 2008).
Cancer and Immunosuppression by Disease
The poster child of disease-associated immunosuppression is infection with HIV. Prior to the advent of accurate viral load assays, the diagnosis was by depressed CD4 count and a specific list of opportunistic diseases. This listing is maintained and updated and is known as the list of AIDS-defining conditions (Centers for Disease Control and Prevention 2008). On this list are several malignant conditions: invasive cervical cancer, Kaposi’s sarcoma, Burkitt’s lymphoma, immunoblastic lymphoma, and primary central nervous system (CNS) lymphoma (PCNSL). Among these tumor types, most have an association with viral disease. The association between cervical cancer and human papillomaviruses is clearly established (Cogliano et al. 2005). The linkage between HHV-8 and Kaposi’s sarcoma was established following the observation of a novel HHV sequence present in the lesions (Chang et al. 1994). This connection has been confirmed and extended to other populations, including transplant patients (Mesri, Cesarman, and Boshoff 2010). Several of the types of lymphoma associated with HIV infection are usually positive for EBV. These include PCNSL, diffuse large B-cell lymphoma, Burkitt’s lymphoma, plasmablastic lymphoma, and Hodgkin’s lymphoma (HL). Primary effusion lymphoma is usually HHV-8–positive (Wang and Castillo 2011). In summary, HIV disease is associated with several different types of tumors. These tumors are often linked with various types of virus infections.
Cancer and Immunosuppression by Drugs
The development of drugs to suppress the immune system passed its first major hurdle in 1968 with the approval of azathioprine for immunosuppression in renal transplant patients. Soon after this approval, reports began appearing of primary malignancy in transplant patients (McKhann 1969). A series of studies published in the 1970s showed a consistent risk in transplant patients for skin tumors, lymphomas, and a small number of other tumors including Kaposi’s sarcoma (reviewed in Kauffmann et al. 2006). As additional drugs entered service for solid organ transplants, the data remained largely consistent in that immunosuppressive drugs generally have an increased risk of these tumor types (Kauffmann et al. 2006; Gutierrez-Dalmau and Campistol 2007). The evidence is also clear that mammalian targets of rapamycin inhibitors have a lower risk than calcineurin inhibitors and older drugs (Gutierrez-Dalmau and Campistol 2007). The data consolidated from numerous studies also suggest that risk increases with both the time on therapy and also on the intensity of the regimen (Gutierrez-Dalmau and Campistol 2007).
Cancer and Immunosuppression
The data from genetic, disease, and drug-induced immunosuppression are relatively consistent in two conclusions: first, that immunosuppression is associated with increased risk of certain types of cancer. The second finding is that a significant fraction of the excess cancers is associated with viral infections such as EBV, HHV-8, and human papilloma virus (HPV). This connection between immunosuppression and cancer has been directly examined in a meta-analysis of tumor incidence rates comparing HIV patients and organ transplant recipients (Grulich et al. 2007). This study compared data from seven studies of HIV patients and five of transplant patients with more than 475,000 patients and 9,900 cancers. The HIV studies are largely from the era before highly active anti-retroviral therapy (HAART) was available, so that the disease process was active during the study period. The combined data set has findings on a total of 33 tumor types or locations. The data show an increase in standardized incidence ratio (SIR) for both patient populations for a number of tumor types. These tumor types include the expected findings for HL and non-Hodgkin’s lymphoma, Kaposi’s sarcoma, and HPV-related tumors. Less expected but also plausible are elevated risks for liver (hepatitis B virus [HBV]/hepatitis C virus) and gastric adenocarcinoma (Helicobacter pylori). The association between H. pylori infection and risk of gastric carcinoma has been established in multiple studies (Cavaleiro-Pinto et al. 2011). The findings of elevated liver and gastric cancer were independently observed in a study of more than 2,500 transplant patients (Vegso et al. 2007). Elevation of SIRs was also observed for malignancies such as nonmelanoma skin tumors and tumors of the lip, esophagus, larynx, and eye, where association with HPV has been suggested but not clearly established. In addition to the clearly and possibly virally linked tumors, there are also tumor types in which there is no suggestion of viral association. These include renal tumors, multiple myeloma, melanoma, and some leukemias. There is clear evidence of characteristic genetic changes in these tumors, specifically for renal cell carcinoma (Finley, Pantuck, and Belldegrun 2011), multiple myeloma (Palumbo and Anderson 2011), and malignant melanoma (Ko, Velez, and Tsao 2010). A similar mixture on viral-associated and genetic malignancies has been observed with pediatric tumor findings in patients treated with tumor necrosis factor–α (TNF-α) inhibitors (Diak et al. 2010). Serving as an internal control, the rates of some common tumors such as breast or prostate are not increased in immunocompromised patients (Grulich et al. 2007).
To summarize this section, the evidence suggests that immunosuppression from a variety of sources has the ability to increase the risk of certain types of malignancies. There is clearly a subset of the immunosuppresive-associated tumors that are associated with known oncogenic viruses such as EBV, HHV-8, and HPV. It is also clear that there are tumor types in which there is no known viral association and in which there is a common pathway of genetic alterations. This second class may be the result of the failure of primary tumor surveillance.
Immunologically Active Drugs
A complementary approach to the issue is to examine those immunologically active drugs (IAD) currently being marketed in the United States to see what is known about any association between intended pharmacology and cancer risk. A variety of sources was used in 2010 to compile a list of IAD. This group includes 67 small molecules and 34 therapeutic proteins. The entry criteria were that the drug was reasonably expected to affect the immune system as an intended effect. Known cytotoxic drugs such as antitumor compounds were not included. Approval dates ranged from 1950 to 2009. Summary information on the groups within this classification is shown in Table 1.
Summary statistics of immunologically active drugs groups.
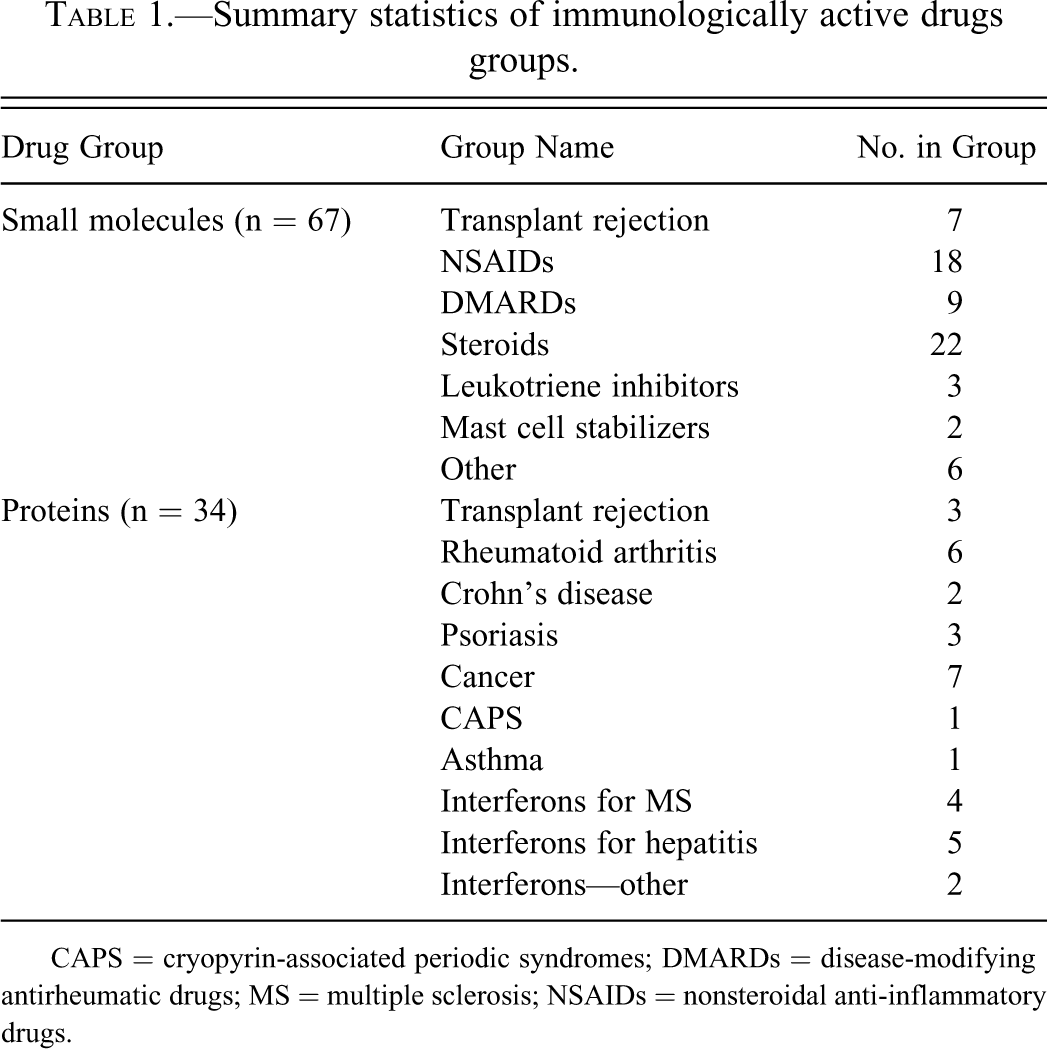
CAPS = cryopyrin-associated periodic syndromes; DMARDs = disease-modifying antirheumatic drugs; MS = multiple sclerosis; NSAIDs = nonsteroidal anti-inflammatory drugs.
For the next phase, we obtained information on the carcinogenicity evaluation (CE) as reported in the text of the approved drug labels as well as a recent compilation (Brambilla and Martelli 2009). For those studies that were not reported in labeling text, we used the current regulatory criteria to determine the acceptability of the study. A fully adequate (FA) CE is currently defined as a study of ≥18 months’ duration and ≥25-fold of intended clinical dose (ICH S1C(R2) 2008).
CE Testing in Small Molecules
A total of 67 drugs were identified, and of these, 42 had a reported CE study (63%) and 8 of 42 had at least one FA study (19%). This compares with the overall rate of FA studies of about 25% of CE studies cited in ICH S1C(R2). Note, however, that CE studies have not been reported for any of the 22 steroids in this data set.
The correlation of CE results with human clinical findings is the pivotal data for the evaluation of the value of nonclinical CE studies. There is sufficient evidence of clinical carcinogenicity for several small-molecule IADs. Among drugs used for organ transplantation, cyclosporine A, tacrolimus, mycophenolate mofetil, and rapamune have multiple studies showing an association. Among the small molecules used to treat rheumatoid arthritis, both methotrexate (Nurmohamed and Dijkmans 2005) and azathioprine are considered to have some potential for clinical carcinogenicity (Gutierrez-Dalmau and Campistol 2007). This information is summarized in Table 2.
Carcinogenicity evaluation (CE) studies for small-molecule immunologically active drugs now known to have human tumor risk.
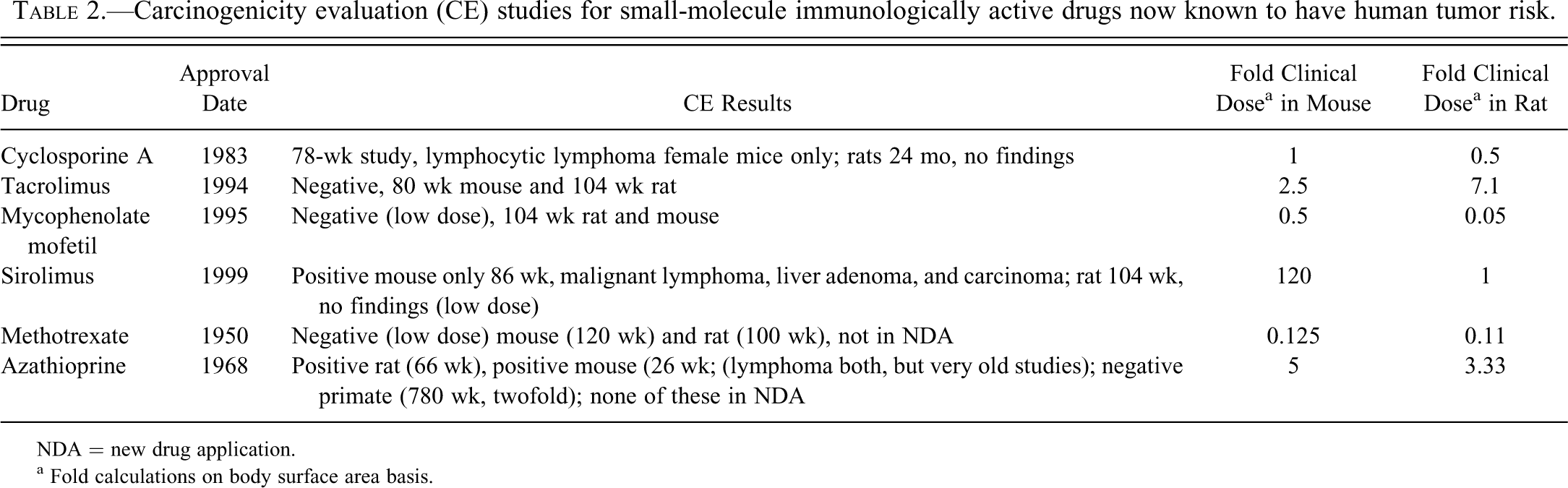
NDA = new drug application.
a Fold calculations on body surface area basis.
CE Testing for Therapeutic Proteins
For therapeutic protein IADs, there was 1 mouse CE study among 34 total approved drugs (2.9%), but it was not FA by the fold clinical dose criteria (threefold actual). Two other drugs had a study with some chance of informing carcinogenicity hazard. Among IAD protein drugs, the evidence of clinical carcinogenicity is clear only for muranomab-CD3 (Kauffman et al. 2006). The evidence for association between tumors with TNF-α inhibitors is conflicted. A study of postmarketing adverse event reports suggests an increased risk for pediatric patients (Diak et al. 2010). In contrast, a study of data from a Swedish registry showed no excess risk of any tumor type (Askling et al. 2009).
The limited results for classical CE testing are not as predictive as one might desire for IAD. However, when the types of clinical tumors are examined, it is clear that the classical CE method does not have any ability to detect a risk due to failure to control oncogenic viruses such as the rodent equivalents of EBV, HHV-8, or HPV. To keep small rodents alive at a useful rate for a 2-year study, the animal suppliers have gone to great lengths to eliminate pathogens from their breeding colonies. The end result is healthier rodents but the inability to report on the state of antiviral immunity.
Novel Nonclinical Methods Development
The previous discussions have established that modulation of the immune system is clearly associated with increased risk of cancer. This risk appears to involve either the failure to control normally repressed oncogenic viruses or the failure of primary tumor surveillance. The existing CE methods do not have the capability for detecting failure of antiviral immunity. They may in theory have some ability to detect failure of tumor surveillance, but experimental support for that hypothesis is currently lacking. The regulatory need exists to evaluate the risk of immunosuppression-associated carcinogenicity for investigational compounds. Therefore, novel methods must be developed to meet this need.
The novel method should be designed to specifically evaluate known mechanisms of carcinogenicity. For the case of IAD, this means either modulation of antiviral immunity or inhibition of primary tumor surveillance. The second mechanism is not easily evaluated, so attention is focused on possible methods to evaluate modulation of antiviral immunity. An initial action is to identify potential nonclinical systems and to determine which system has the potential to be developed into a method suitable for regulatory use.
A desirable viral model system should have several characteristics. First, the viruses in nonclinical species should be highly related to a known oncogenic human virus. Second, there should be viruses in as many nonclinical species as possible. Third, it would be better if there was evidence of virus-associated tumors. A summary of the characteristics of the candidates is shown in Table 3. From this listing, it can be seen that the gamma-herpesviruses provide the most complete known set of related viruses. A more detailed evaluation of the gamma-herpesviruses is shown in Table 4. This shows that these three viruses fit most of the desired characteristics of a nonclinical model. There is evidence of immunosuppression-associated tumors in both the murine MHV-68 model (Sunil-Chandra et al. 1994) and in the cynomolgus monkey with LCV (Schmidtko et al. 2002).
Comparison among clinical and nonclinical oncogenic viruses.

Comparison among human and nonhuman γ-herpesviruses.
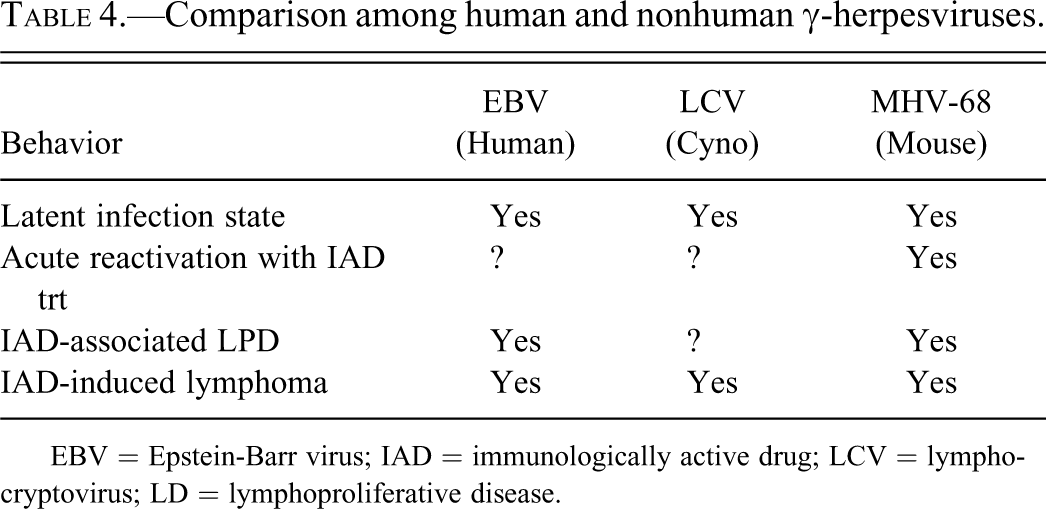
EBV = Epstein-Barr virus; IAD = immunologically active drug; LCV = lymphocryptovirus; LD = lymphoproliferative disease.
The MHV-68 virus has a complex life cycle within the mouse. A study using an MHV-68 construct with luciferase under the control of the highly active M3 promoter shows that areas of infection appear in at least five different anatomical locations among three major waves of infection (Hwang et al. 2008). An additional experiment studied with mice that had fully suppressed the original infection (day +90). The results showed that a single dose of the ISD cyclosporine caused a transient reactivation of virus proliferation. This was strongly positive at days +5 and +8 after treatment but was fully suppressed again by day +11 (Hwang et al. 2008). This result suggests that it might be possible to devise an assay system to detect the potential for unexpected suppression of viral immunity.
Members of the herpesvirus group have been identified in a very wide variety of vertebrate hosts (Davison 2002). In the herpesviruses with primate hosts, EBV is currently classified in Clade B of the gamma-1 herpesviruses (Ehlers et al. 2010). The equivalent virus (LCV-1) in the cynomolgus monkey (Macaca fasicularis) is also classified in Clade B. This virus appears to be highly prevalent in both wild (Ishida and Varavudhi 1992) and in captive-bred populations (Fujimoto and Honjo 1991). The value of LCV-1 as a model of EBV infection is illustrated by data from two studies. A report on compiled necropsy data from SIV-infected cynomolgus monkeys shows an incidence of lymphoma in 8 of 26 (31%; Habis et al. 1999). The incidence in a much larger population of rhesus was about 4%. Selected samples were examined for the presence of LCV-1 sequences, and 2 of 8 samples showed clear evidence of the presence of LCV-1 in lymphoma tissue (Habis et al. 1999). A second study shows that lymphoma was observed in 9 of 160 (5.6%) of cynomolgus monkeys used in a renal transplantation program (Schmidtko et al. 2002). Hybridization for EBV-encoded RNA was positive in all nine cases reported. These studies demonstrate that the cynomolgus monkey has a herpesvirus closely related to EBV and that immunosuppression by infectious or pharmacological methods results in an increased risk of herpesvirus-positive lymphoma. Therefore, this model system has clear potential for use in detecting unexpected suppression of antiviral immunity. This would be of clear value for the evaluation of ISD-associated carcinogenicity risk for therapeutic proteins that may be inactive in rodent systems.
An additional potential model system is found in mice with humanized immune systems. There are several variants of this model, but in general, mice with genetic deletions in critical immune system genes are implanted with human fetal liver, thymus, and CD34+ leukocytic stem cells (Melkus et al. 2006). These mice are able to mount some immune responses following EBV infection. Additional studies with a similar model system show that these mice have approximately a 50% rate of lymphoma within 6 to 12 weeks following EBV infection (Yajima et al. 2008; Ma et al. 2011). There is evidence that this high rate of lymphoma is related to the original dose of EBV used to infect the mice. Mice infected with doses of 102 TD50 or higher of EBV went on to develop lymphoproliferative disease (LPD), whereas mice infected with several lower doses were able to control the initial infection and showed persistent infection in the absence of LPD or lymphoma (Yajima et al. 2008). These results suggest that these mice with a humanized immune system have the potential to provide a more direct assay of drug interference with human antiviral immunity. However, significant development work remains to be done to establish the value of this model.
In conclusion, the available experimental and clinical data clearly establish that suppression of the immune system results in an increased risk of certain types of tumors. A significant fraction of these tumors is associated with known oncogenic viruses such as EBV or HPVs. The existing nonclinical systems for evaluating risk of carcinogenicity for investigational drugs will not detect this class of risk because of the lack of oncogenic viruses in experimental rodents. Several model systems including the murine MHV-68 virus, cynomolgus LCV-1, and EBV in mice with a humanized immune system have the potential to detect this class of risk. In each case, significant research is needed to develop these models into an assay suitable for use in a regulatory environment.
Footnotes
Abbreviations
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article. The authors received no financial support for the research and/or authorship of this article.
This report is not an official U.S. Food and Drug Administration guidance or policy statement. No official support or endorsement by the U.S. Food and Drug Administration is intended or should be inferred.